PEN-BASED COMPUTERS
IN EMS

PEN-BASED COMPUTERS IN EMS
PRESENTED BY:
• Moises Alajado• Gerone Hamilton• Mike Junker• Chuck Schwartz• Mike Tschida

SPECIAL THANKS
• Mike Vukovich, President/Owner, Open, Inc.
• Captain Rick Fretchel, SPFD
• Captain Greg Erickson, SPFD
• Dave Page, Instructor, IHCC

INTRODUCTION
• Mike Junker: Introduction & History/Future of Pen Based Computers.
• Mike Tschida & Moises Alajado: What are Pen-Based Computers and what are its advantages.
• Gerone Hamilton & Chuck Schwartz: Features and Sample Reports.

HISTORY
December 1994
Issue of “Fire Chief” Magazine has an article on pen-based computers.Used for:
• maintenance of hydrants• conduct fire inspections• inspect apparatus• complete run reports

St. Paul Fire History
• St. Paul Fire Department First Started To Research PBCs In April 1995
• In 1997 SPFD signed a contract with Open, Inc. to take full responsibility to bring SPFD into the new millenium fully operational and paperless using PBCs.
• Over the past 4 years there have been a lot of changes, ups and downs, and the transition has not been an easy one, however, by 1-1-2000 it appears PBCs will be fully operational!

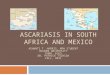
These medics are focusing on what they do best . . . providing effective patient care.
The medic on the left is also collecting, managing, and communicating critical emergency medical information electronically.
How ?

SafetyPAD™
Information you need
. . . Anytime
. . . Anywhere
a product of OPEN incorporated

‘Musts’ to Success
• Real-time usability• As fast or faster than paper
(min man. Entry)• Easy-to-use, intuitive• Highly customizable• More than data collection• Expandable architecture

a problem . . .
• Improve productivity and efficiency?
• Increase profitability?
• Reduce time and resource requirements?
• Cut costs?
• Enhance patient care?
• Optimize information collection and management?
• Generate accurate, comprehensive, and omission-free reports?
• Decrease liability exposure?
• Eliminate paper and duplicate data entry?
How can you . . .

a solution . . .Linking it all together
• Information
• People
• Communications
PeoplePeople Hospital
Operations
QA / QI
Dispatch
Billing
Medic
Administration
State / Local
Educators
SafetyPADSafetyPADmobilemobile Collect
Hands-free
Portable
Pen / Wearable
Paperless Voice-enabled
Real-time
SafetyPADSafetyPADbasebase
Manage
Share
Analyze
Distribute
Automate
Communicate
ThingsThings
GPS / Mapping
Camera/Video
Multimedia
Medical Devices
Modem PC card
Peripherals
Printer / FAX
Inter/Intranet
Wireless
Dial-in
Cable / Dock
CDPD Cellular
LAN/WAN
Infrared
Private / Public
Radio
LinkLink

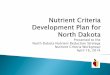
SafetyPAD architecture. . .
Wireless (IrDA, CDPD)
Wireline (Intra/Internet)
Enterprise Database
Billing State / Local
QA/QI Education
CAD Medical Ctl.
ER Specialists
Enterprise Database
Billing State / Local
QA/QI Education
CAD Medical Control
ER Specialists
GPS Map AVL
Other SafetyPADs
Medical and Digital Devices
Printer FAX

What is SafetyPADmobile . . .
• Real-time usable field data collection and information management
• Collect, reference, and communicate EMS information
• Mobile pen-based and wearable computer technology
• More than data collection

What is SafetyPADbase . . .
• Enterprise-wide information management system
• Mobile manager• Collect, analyze, communicate . . . • Distribute and link information between
a variety of information systems• Multi-tiered architecture• Open standards

a benefit to everyone . . .
• Medics and Responders• Patients• Operations /
Administration• QA / QI• Billing• Medical Direction• Hospitals and ER Staff• Dispatch• Educators• State and Area Agencies• Legal Agents
• Optimize documentation
• Improved care• Link info systems• Enhance quality• Higher collection rates• Improve effectiveness• Legible, timely reports• Status and tracking• Modify education• Paperless submissions• Comprehensive doc.

key benefits . . .
Eliminate paper. Reduce time and resource
requirements. End duplicate data re-entry. Optimize information management. Dramatically reduce the inefficiencies
of managing information with paper.
• Significantly cut costs and increase efficiency . . .
Improve billing collection rates. Assure that reimbursement-critical
information is collected. Shorten billing cycles. Minimize delays.
• Increase profitability . . .
Easily enter, reference, analyze, manage, and distribute call and patient information with one comprehensive, enterprise-wide solution.
• Enhance productivity . . .
• Improve quality and decrease liability exposure . . .
Generate complete, accurate, legible, and omission-free reports.• Optimize QA and QI . . .
unlimited data analysis capabilities. assess effectiveness and efficiency. track clinical outcomes. identify trends.

a few other benefits . . .
• Optimize performance and information accessibility . .
• Flexible, powerful customization capabilities . . .
• Optimize protocol compliance and accelerate data entry and referencing . . .
• Improve overall patient care . . .
• Minimize training requirements . . .
• Advanced, expandable, upgradeable technologies. . .
• and many more . . .

“GOING FORWARD TO THE FUTURE”
• With technology changing by the day the future looks promising for PBCS.– Fax from Medics to the hospital– Infra-red cameras to provide picture from scene to hospital– Sharing EKG from LifePack to hospital personnel
– Instructional videos (chest decompression) – Voice recognition – Access to the CAD System

SafetyPADa revolutionary solution. . .an invaluable tool . . .

02:03 “MEDIC 4 - 2943 W. 7TH .. CHEST PAIN”Accurate and timely information is wirelessly delivered within seconds between SafetyPADmobile and other common systems, such as dispatch, using public or private radio services.

02:05 “AVL / GPS / MAPPING”Integrated GPS and mapping instantly lets you and others know where you are and where you need to go!

02:04 “MEDIC 4 - IN ROUTE”Frequent destination and past patient records are maintained for immediate retrieval. SafetyPADmobile becomes your agency’s intelligent MDT through convenient one-touch or voice-enabled status commands.

02:08 “MEDIC 4 - AT SCENE”SafetyPADmobile utilizes advanced Pentium-class pen-based and wearable computers to take advantage of their natural entry mechanisms, maximized mobility, and convenience. Information is collected in the field and wirelessly ’beamed’ between two or more responders, eliminating redundancy and speeding entry. Archived data, such as the patient’s past history and demographics, is accessed from local or remote databases or smartcards. A multilingual translator minimizes a language barrier between medics and the patient.

02:09 “FOCUS ON PATIENT”Call and patient information is rapidly collected using an extremely advanced, yet easy-to-use pen and voice enhanced interface. Auto-complete speeds entry. ‘Active Guidelines’ feature helps guide responders through their agency’s protocol to optimize assessing, treating, and documenting while minimizing mistakes and eliminating omissions. Voice-enabled technology allow responders to gather and reference information hands-free while physically caring for patients.

02:17 “MEDIC 4 - DEPARTED SCENE”Protocols, medication contraindications, and instructional videos are instantly reviewed within an embedded browser. Images taken from a digital camera and ECG data collected from an attached interpretive cardiac monitor, along with patient and clinical data are gathered, reviewed, and communicated wirelessly to medical control and a cardiologist to make telemedicine a reality. A preliminary report is instantly delivered to the receiving ER prior to arrival. Final interventions and vitals are documented and time-stamped just by stating them.

02:26 “MEDIC 4 - AT DESTINATION”All signatures are collected electronically. The report is spell checked, then reviewed in a call summary screen with narratives automatically generated from collected data. A legible, accurate and complete report is insured by electronically checking it against a set of agency-defined rules. The final run report is saved, then beamed to an infrared-enabled printer in a matter of seconds.

02:29 “MEDIC 4 - IN SERVICE . . .”

“THROUGHOUT THE DAY”Information is instantly shared between SafetyPADmobile and SafetyPADbase through wired and wireless connections. Call and patient data is immediately distributed to those who need it . . . billing, dispatch, QA/QI, operations, state/local . . . the way they need it . . . ODBC, ASCII, HTML, ActiveX, HL7. A direct interface to billing speeds up processing, and no paper means no additional data entry or transcription errors. QA/QI analyzes standardized data to spot trends and improve performance, while e-mailing results to educators and staff. Inventory is continually tracked when interventions are given throughout the day. SafetyPADbase electronically updates all mobile units with data field revisions, electronic surveys and studies, lookup tables, ‘Active Guidelines’, help documents, system files, e-mail, and more!

added features

15:14:11 VITALS 148/100 94 R 20 88% RA SIT 15:15:30 PROCEDURE 100% NON-REBREATHER; 10L/min, Kippels 15:17:22 PROCEDURE C-COLLAR 15:18:00 Pt STATUS DIZZINESS 15:18:30 VITALS 142/92 88 R 17 95% w/O2 SIT 15:19:30 PROCEDURE BACKBOARD & STRECHER 15:21:15 PROCEDURE CARDIAC MONITOR 15:21:15 ECG SINUS RHYTHM, w/ PVC’s; 3/min 15:22:13 PROCEDURE NORMAL SALINE; Successful, x1, IV, TKO, 18G, (R) AC, 500ml, Kippels 15:23:30 VITALS 134/86 84 R 16 99% w/O2 LAY; pt status improved 15:24:15 BLOOD SUGAR 112 15:25:00 SKIN NORMAL TEMP., NORMAL COLOR, NORMAL MOISTURE 15:28:00 VITALS 132/88 74 R 16 99% w/O2 LAY 15:30:15 Pt STATUS PT STATED “I FEEL MUCH BETTER”
INITIAL LOC: ALERT X 2 (Person, Place); AIRWAY: PATENT; BREATHING: EQUAL BILATERAL, EQUAL EXPANSION, CLEAR LUNG SOUNDS (R) (L); CIRCUL: PULSE PRESENT, RADIAL, STRONG, REG.; EYES: PERRL; SKIN: NORMAL TEMP, PALE COLOR, MOIST MOISTURE GCS: 15; 4-Eyes – Spontaneous, 5-Verbal – Oriented, 6-Motor – Obeys Cmnd, CMS: x4 PHYSICAL TENDERNESS (L) WRIST; Pt stated that his right hand was contorted as a result of airbag deployment. ABDOMEN – NO SIGNS OF TRAUMA; NORMAL RANGE OF MOTION; NO LOSS OF SENSATION; NO SIGNS OF JVD; NO OTHER VISIBLE SIGNS OF TRAUMA; IMPRESSION (L) WRIST FRACTURE; RULE OUT (L) WRIST SPRAIN; ULCER; RULE OUT PANCREATITIS;
ALLERGIES SULFA DRUGS; IBUPROFEN; RED MEAT; PEANUTS; IODINE; MEDS ANTIBIOTICS; DIABETIC MEDS; ZANTAC; PREEXIST CARDIAC BYPASS: within past 2 years; PANCREATITIS; DIABETIC; ULCERS;
CAUSE MOTOR VEHICLE ACCIDENT: pt was driver, pt in sitting position upon arrival, onset – < 10 min. ago, driver/pass. airbags deployed, driver/pass. seatbelts worn, impact speed < 30 mph, rear impact, < 20” vehicle deformity, < 12” intrusion into pt compartment COMPLAINT ABDOMEN PAIN: onset – immediately after cause, duration – still present, quality – dull, severity – 6 of 10, last meal < 3 hours ago SYMPTOMS TENSE; WEAK ALL OVER; DISORIENTED; DENIES LOSS OF CONSCIOUSNESS; DENIES SUBSTANCE USE; DENIES NAUSEA NOTE: Patient states that he feels extremely tense as a result of MVA.
C A L L P A T I E N T D A T E S / T I M E S
H x P R E S E N T
H x P A S T
F I N D I N G S
C A R E E V E N T S
R E S U L T A U T H O R I Z A T I O N
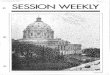
100 East 11th Street St. Paul, MN 55101 Phone # (651) 228-6260
Saint Paul Fire EMS Report
Run # Call Type Scene City State Agency Crew
20408 Motor Vehicle Accident Dale St & University Ave St. Paul MN MEDIC #9, Ph# 774-7630 Fretschel, Kippels, Zangs, Jones
ANDERSON, SVEN M 03/22/48 50 210 WHITE 2134 University Ave St. Paul, MN 55103 (651) 227-3459 Frascone Regions Hospital
Notified Departed At Scene At Patient Departed Scene At Destination In Service At Quarters
15:08:32 11/15/98 15:09:26 15:13:08 15:13:30 15:20:15 15:31:48 15:33:00 15:38:15
Subject Description / Details
Subject Description / Details
Subject Description / Details
Time Subject Description / Details BP P R SaO2 Pos
Disposition Trans. Reason Destination Dest. Reason Status MRCC #, Name
EVALUATED, TREATED, TRANSPORTED SINGLE PATIENT PT REQ. IMMOBILIZATION, O2 HOSPITAL, REGIONS HOSPITAL PATIENT CHOICE EMERGENCY, LIGHTS/SIRENS 119, JOHNSON
Medic . . . FRETSCHEL Received by . . . FOX, (RN)
Page 1 of 2 Next Page MVA images, ECG report
Patient ANDERSON, SVEN
Compaint(s) ABDOMEN PAIN
Patient Name Sex DOB Age Wt. Race Address City, State, Zip Phone # Physician Pref. Hospital

15:14:11 VITALS 148/100 94 R 20 88% RA SIT 15:15:30 PROCEDURE 100% NON-REBREATHER; 10L/min, Kippels 15:17:22 PROCEDURE C-COLLAR 15:18:00 Pt STATUS DIZZINESS 15:18:30 VITALS 142/92 88 R 17 95% w/O2 SIT 15:19:30 PROCEDURE BACKBOARD & STRECHER 15:21:15 PROCEDURE CARDIAC MONITOR 15:21:15 ECG SINUS RHYTHM, w/ PVC’s; 3/min 15:22:13 PROCEDURE NORMAL SALINE; Successful, x1, IV, TKO, 18G, (R) AC, 500ml, Kippels 15:23:30 VITALS 134/86 84 R 16 99% w/O2 LAY; pt status improved 15:24:15 BLOOD SUGAR 112 15:25:00 SKIN NORMAL TEMP., NORMAL COLOR, NORMAL MOISTURE 15:28:00 VITALS 132/88 74 R 16 99% w/O2 LAY 15:30:15 Pt STATUS PT STATED “I FEEL MUCH BETTER”
INITIAL LOC: ALERT X 2 (Person, Place); AIRWAY: PATENT; BREATHING: EQUAL BILATERAL, EQUAL EXPANSION, CLEAR LUNG SOUNDS (R) (L); CIRCUL: PULSE PRESENT, RADIAL, STRONG, REG.; EYES: PERRL; SKIN: NORMAL TEMP, PALE COLOR, MOIST MOISTURE GCS: 15; 4-Eyes – Spontaneous, 5-Verbal – Oriented, 6-Motor – Obeys Cmnd, CMS: x4 PHYSICAL TENDERNESS (L) WRIST; Pt stated that his right hand was contorted as a result of airbag deployment. ABDOMEN – NO SIGNS OF TRAUMA; NORMAL RANGE OF MOTION; NO LOSS OF SENSATION; NO SIGNS OF JVD; NO OTHER VISIBLE SIGNS OF TRAUMA; IMPRESSION (L) WRIST FRACTURE; RULE OUT (L) WRIST SPRAIN; ULCER; RULE OUT PANCREATITIS;
ALLERGIES SULFA DRUGS; IBUPROFEN; RED MEAT; PEANUTS; IODINE; MEDS ANTIBIOTICS; DIABETIC MEDS; ZANTAC; PREEXIST CARDIAC BYPASS: within past 2 years; PANCREATITIS; DIABETIC; ULCERS;
CAUSE MOTOR VEHICLE ACCIDENT: pt was driver, pt in sitting position upon arrival, onset – < 10 min. ago, driver/pass. airbags deployed, driver/pass. seatbelts worn, impact speed < 30 mph, rear impact, < 20” vehicle deformity, < 12” intrusion into pt compartment COMPLAINT ABDOMEN PAIN: onset – immediately after cause, duration – still present, quality – dull, severity – 6 of 10, last meal < 3 hours ago SYMPTOMS TENSE; WEAK ALL OVER; DISORIENTED; DENIES LOSS OF CONSCIOUSNESS; DENIES SUBSTANCE USE; DENIES NAUSEA NOTE: Patient states that he feels extremely tense as a result of MVA.
C A L L P A T I E N T D A T E S / T I M E S
H x P R E S E N T
H x P A S T
F I N D I N G S
C A R E E V E N T S
R E S U L T A U T H O R I Z A T I O N
100 East 11th Street St. Paul, MN 55101 Phone # (651) 228-6260
Saint Paul Fire EMS Report
Run # Call Type Scene City State Agency Crew
20408 Motor Vehicle Accident Dale St & University Ave St. Paul MN MEDIC #9, Ph# 774-7630 Fretschel, Kippels, Zangs, Jones
ANDERSON, SVEN M 03/22/48 50 210 WHITE 2134 University Ave St. Paul, MN 55103 (651) 227-3459 Frascone Regions Hospital
Notified Departed At Scene At Patient Departed Scene At Destination In Service At Quarters
15:08:32 11/15/98 15:09:26 15:13:08 15:13:30 15:20:15 15:31:48 15:33:00 15:38:15
Subject Description / Details
Subject Description / Details
Subject Description / Details
Time Subject Description / Details BP P R SaO2 Pos
Disposition Trans. Reason Destination Dest. Reason Status MRCC #, Name
EVALUATED, TREATED, TRANSPORTED SINGLE PATIENT PT REQ. IMMOBILIZATION, O2 HOSPITAL, REGIONS HOSPITAL PATIENT CHOICE EMERGENCY, LIGHTS/SIRENS 119, JOHNSON
Medic . . . FRETSCHEL Received by . . . FOX, (RN)
Page 1 of 2 Next Page MVA images, ECG report
Patient ANDERSON, SVEN
Compaint(s) ABDOMEN PAIN
Patient Name Sex DOB Age Wt. Race Address City, State, Zip Phone # Physician Pref. Hospital

Resources and references
• Mike Vukovich, Open, Inc• Captain Rick Fretchel, Technical
Support• Captain Greg Erickson, Mentor• December 1994 issue of “Fire Chief”
Magazine• December 1999 issue of “JEMS”• By e-mail: [email protected]
Recommended