POSITIONAL ASPHYXIA
by Dr Faiz Ahmad
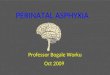
DEFINITION Any body positions of ones own body
that obstructs the restrained persons
airway or interferes with the
muscular or mechanical components
of respiration and person can not get
enough oxygen(hypoxia) - result in
positional asphyxia.
• Deprived of Oxygen.
• Excess carbon dioxide.
• Hypoxia .
• Loss of consciousness.
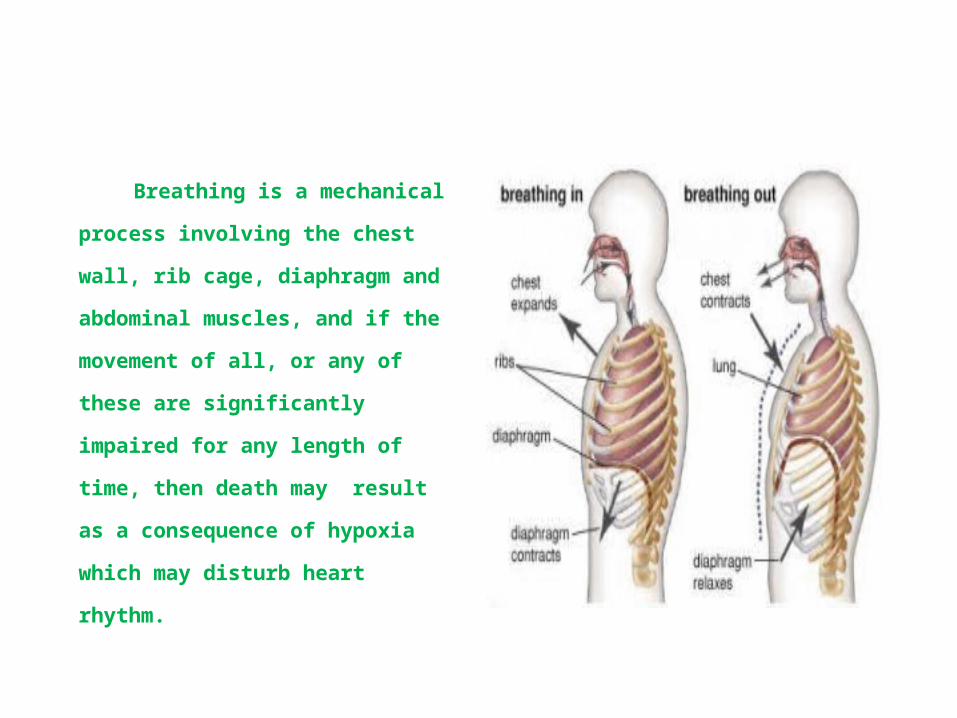
Breathing is a mechanical process
involving the chest wall, rib cage,
diaphragm and abdominal
muscles, and if the movement of
all, or any of these are
significantly impaired for any
length of time, then death may
result as a consequence of hypoxia
which may disturb heart rhythm.
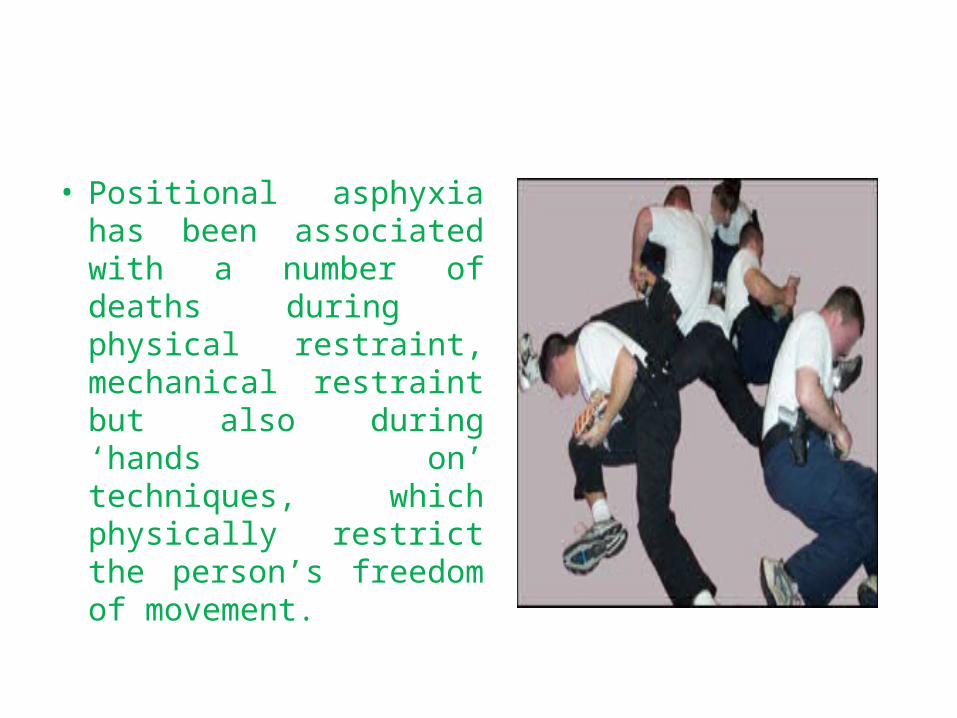
• Positional asphyxia has been associated with a number of deaths during physical restraint, mechanical restraint but also during ‘hands on’ techniques, which physically restrict the person’s freedom of movement.
What are Risk Factors?
• Position During Restraint (particularly face down
prone but also hyper flexion).• Prolonged struggle/agitated delirium syndrome• Drug or alcohol intoxication, in particular cocaine
and methamphetamine intoxication or cocaine-induced psychosis
• Mania• Obesity• Sedation/Accidents/Organic diseases/quadriplegia
• Respiratory Syndromes including Asthma and Bronchitis.
• Cardio Vascular Disorder including an enlarged heart
(hypertrophic cardiomyopathy) and other cardiovascular
disorders
• Prescribed Drugs.
A combination of factors may place individuals at Risk
of Positional Asphyxia.

Prolonged violent physical agitation
Stage 1 – Development of an incident –
The individual exhibits irrational,
violent, aggressive behaviour and
paranoia. The person may be
physically active and aroused.
Stage 2 – Intervention –
One or more interveners' are
tempted to sit or lean on the subject
to maintain control.
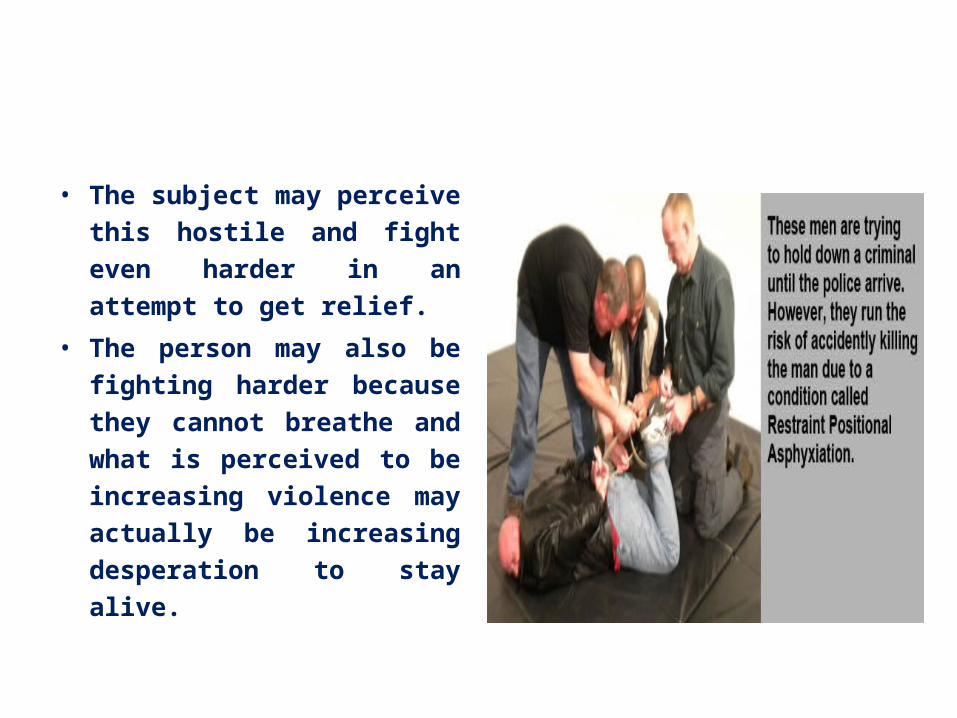
• The subject may perceive
this hostile and fight even
harder in an attempt to get
relief.
• The person may also be
fighting harder because they
cannot breathe and what is
perceived to be increasing
violence may actually be
increasing desperation to
stay alive.
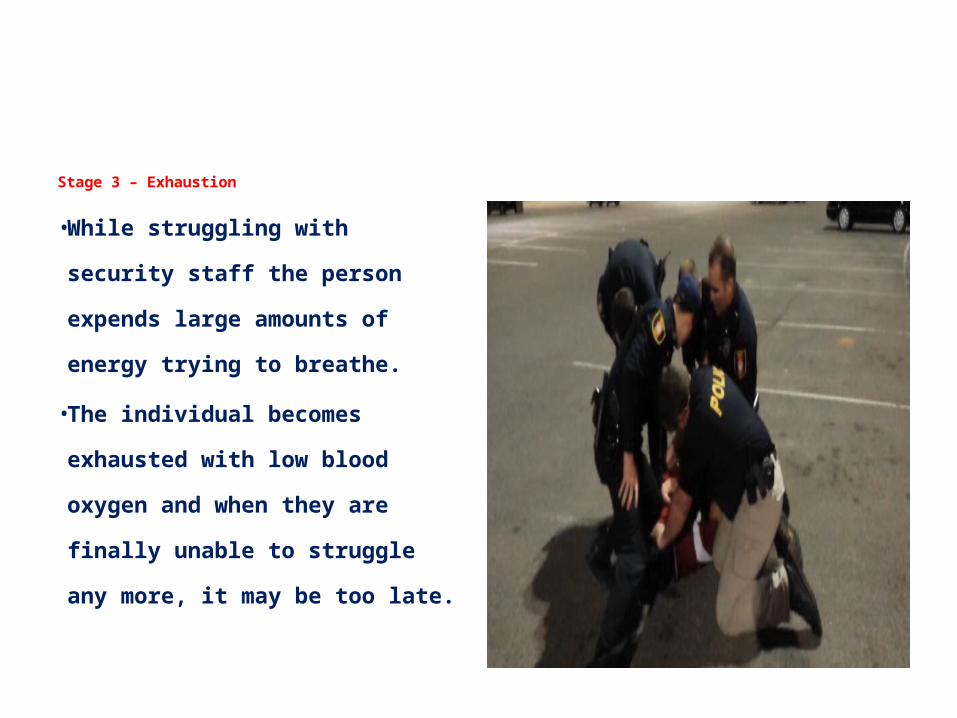
Stage 3 – Exhaustion
• While struggling with security
staff the person expends large
amounts of energy trying to
breathe.
• The individual becomes exhausted
with low blood oxygen and when
they are finally unable to struggle
any more, it may be too late.
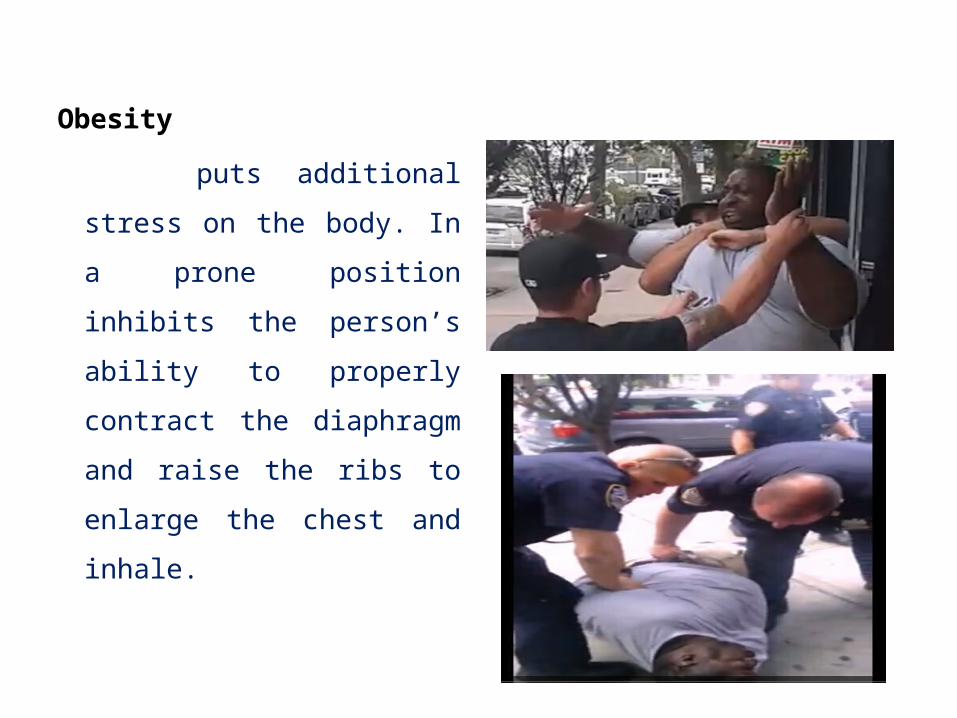
Obesity
puts additional stress on
the body. In a prone
position inhibits the
person’s ability to properly
contract the diaphragm and
raise the ribs to enlarge the
chest and inhale.
Psychosis
stimulant drugs (amphetamines,
speed, ‘ICE’, ecstasy) can create an
“excited delirium” in which the
person is paranoid, over excited and
potentially violent. The stimulation
of the heart can produce cardiac
rhythm disturbances which can be
fatal. In this situation any difficulty
breathing can result in sudden
deterioration in condition and
death.
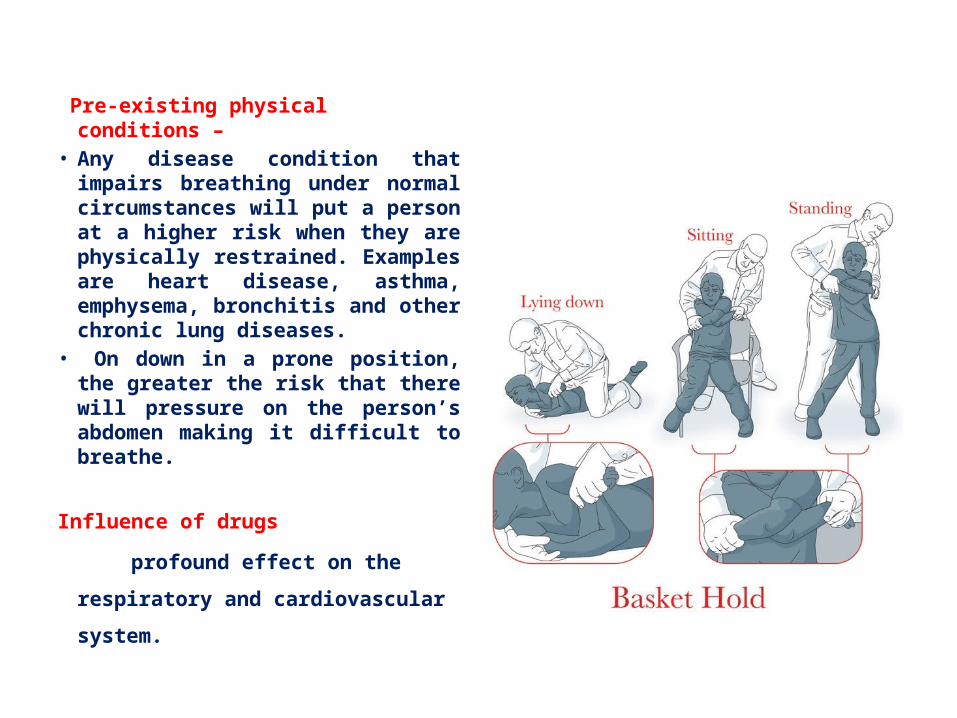
Pre-existing physical conditions – • Any disease condition that
impairs breathing under normal circumstances will put a person at a higher risk when they are physically restrained. Examples are heart disease, asthma, emphysema, bronchitis and other chronic lung diseases.
• On down in a prone position, the greater the risk that there will pressure on the person’s abdomen making it difficult to breathe.
Influence of drugs
profound effect on the respiratory
and cardiovascular system.
Excited Delirium Also known as
Agitated delirium
Cocaine induced psychosis
Acute exhaustive mania • It is characterised by purposeless, often violent activity coupled with
incoherent or often meaningless speech and hallucinations with paranoid delusions
o Bizarre or aggressive behaviour• Impaired thinking• Combativeness• Super-Human Strength• Disorientation • Hallucinations• Acute onset of paranoia• Shouting
Delirium Can Be Caused By
• Psychiatric illness
(combined with Drink and/or Drugs)
• Drug intoxication
(Cocaine is the best known cause of excited Delirium)
• Alcohol
Effects of Excite Delirium
• Hypothermia • High tolerance to pain • Quick to fatigue –
especially after a violent struggle
• Skin may be hot to touch • Abnormal Strength
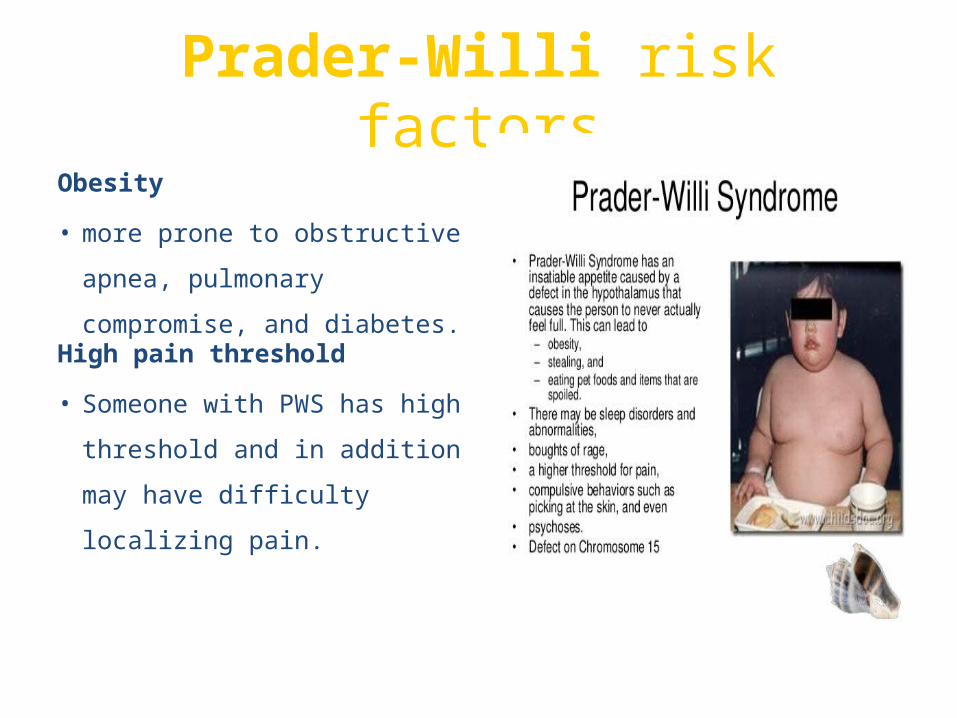
Prader-Willi risk factors
Obesity
• more prone to obstructive
apnea, pulmonary
compromise, and diabetes. High pain threshold
• Someone with PWS has
high threshold and in
addition may have difficulty
localizing pain.
Increased risk of respiratory difficulties• Hypotonic and weak chest muscles
Thick saliva• complicates airway management
Chronic stomach reflux and aspiration
Temperature instability
• Idiopathic hyper and hypothermia have been reported. Fever may be
present despite serious infection.
Bruise easilyAnatomic and physiologic differences
• such as : narrow airway, underdevelopment of the larynx, edema, hip
dysplasia, and scoliosis
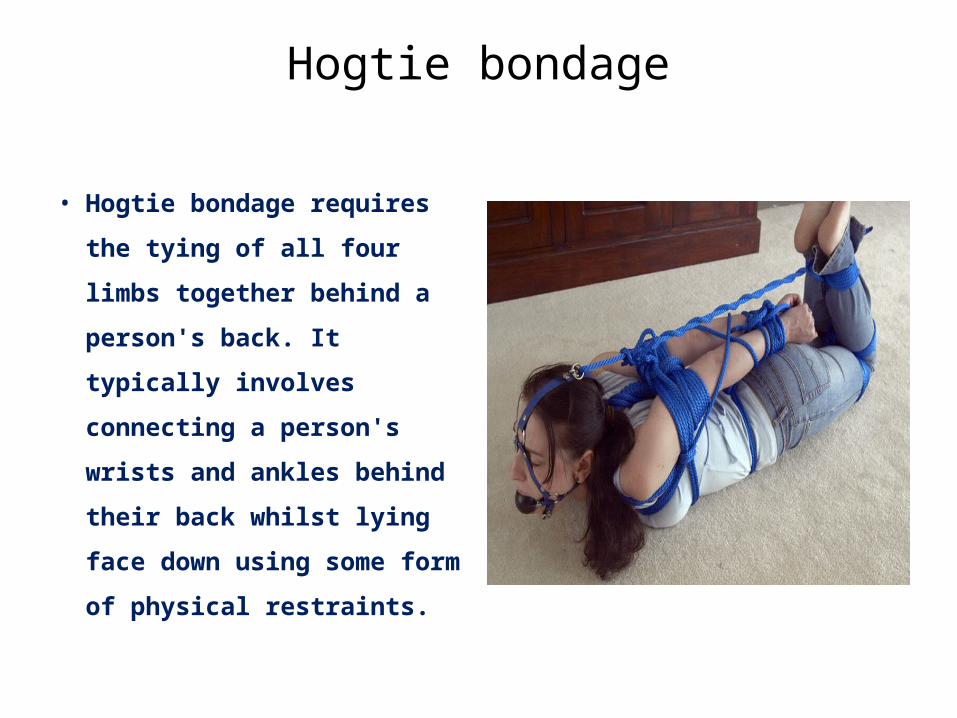
Hogtie bondage
• Hogtie bondage requires the
tying of all four limbs
together behind a person's
back. It typically involves
connecting a person's wrists
and ankles behind their back
whilst lying face down using
some form of physical
restraints.
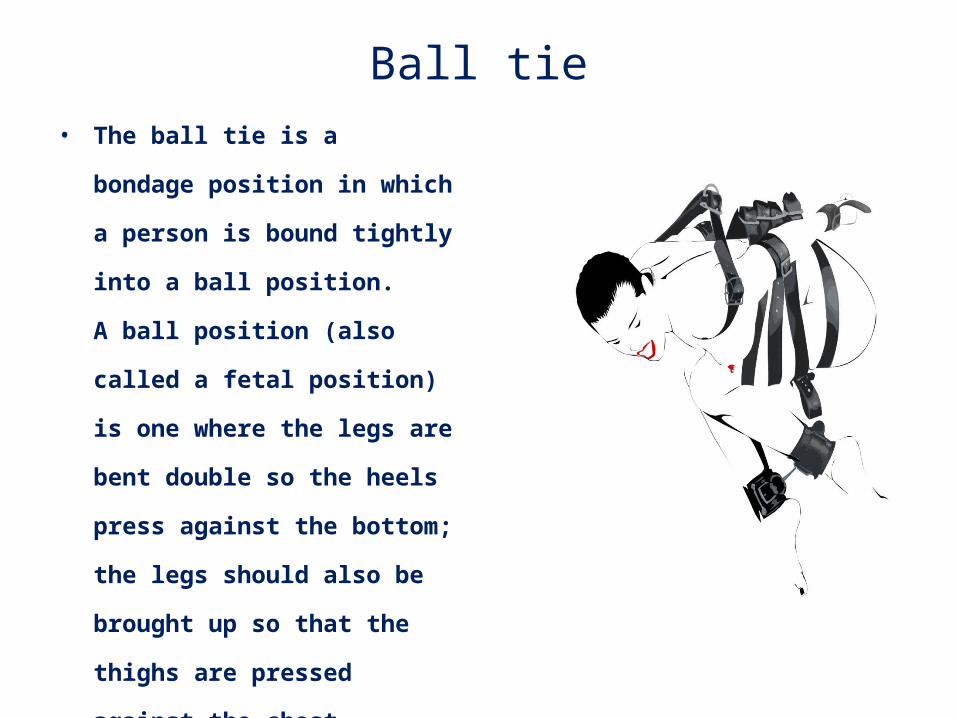
Ball tie• The ball tie is a bondage position in
which a person is bound tightly into
a ball position. A ball position (also
called a fetal position) is one where
the legs are bent double so the heels
press against the bottom; the legs
should also be brought up so that
the thighs are pressed against the
chest. Pressing the thighs against
the abdomen may restrict
breathing .
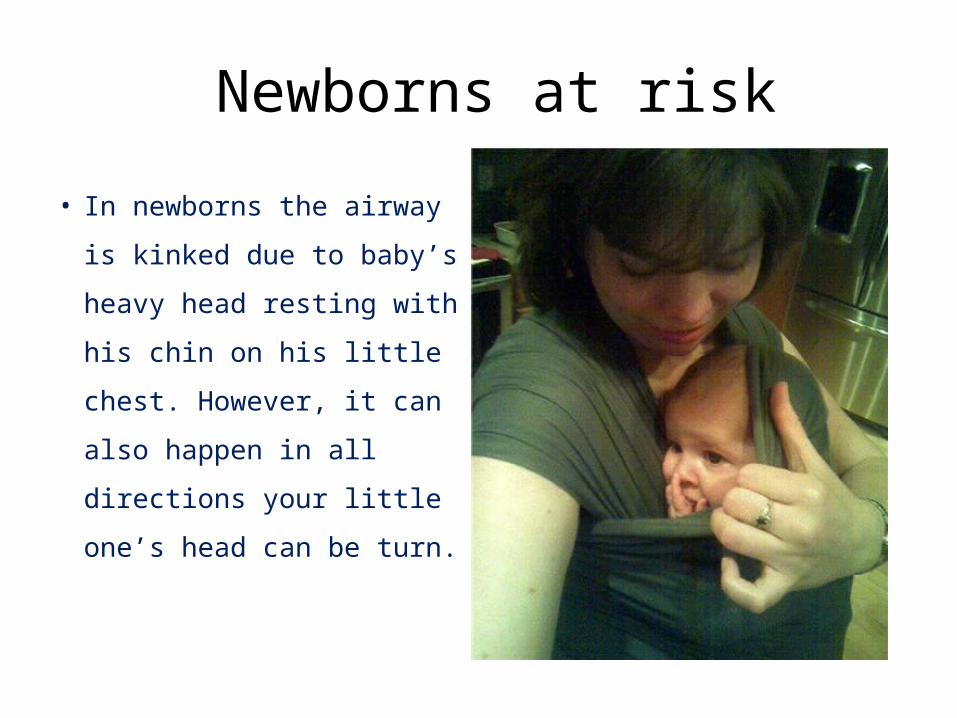
Newborns at risk
• In newborns the airway is
kinked due to baby’s heavy
head resting with his chin
on his little chest.
However, it can also
happen in all directions
your little one’s head can
be turn.
• Who is at risk?
Newborns from 0-4 month old are the greatest risk group.
Babies under 4 months old Newborns with low birth
weight Premature babies Babies with hypotonia
(low muscle tone) Babies placed in reclined
baby holding devices
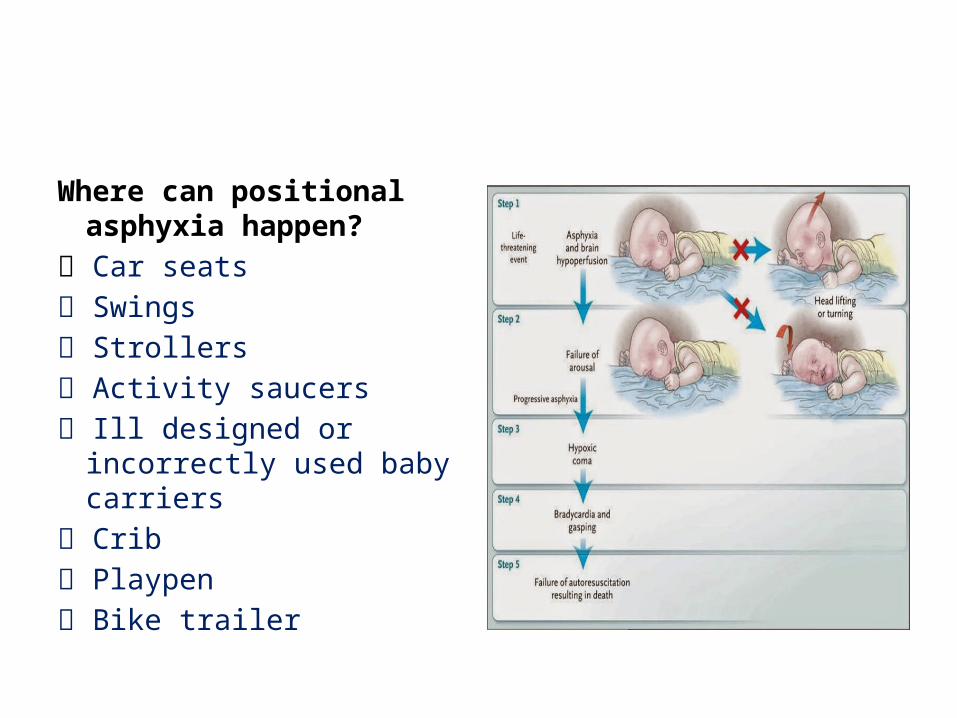
Where can positional asphyxia happen?
Car seats
Swings
Strollers
Activity saucers
Ill designed or incorrectly used baby carriers
Crib
Playpen
Bike trailer
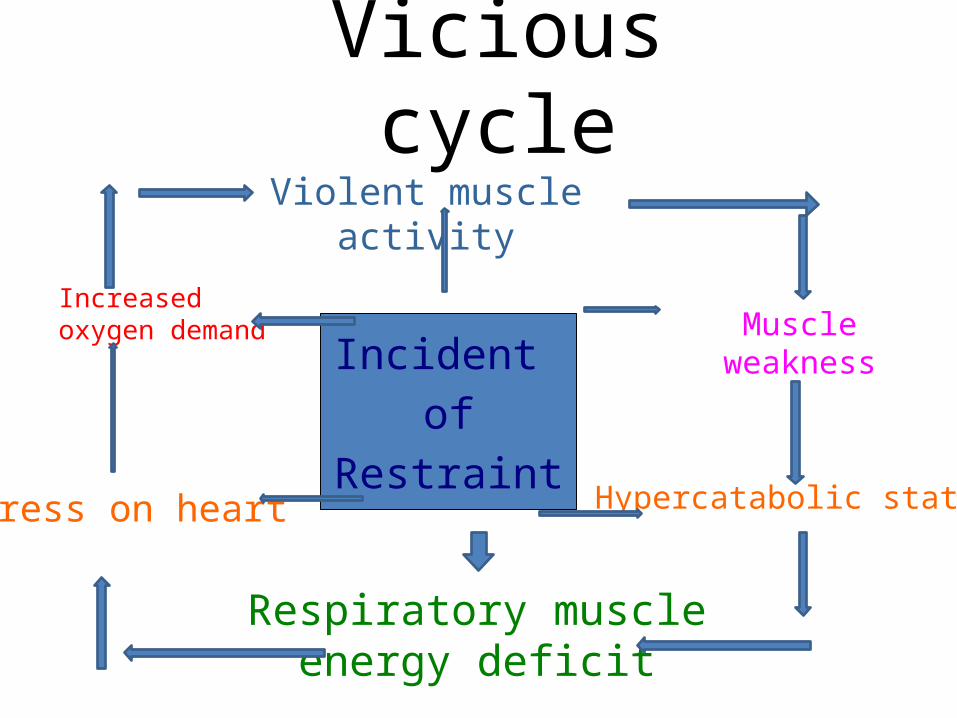
Incident
of
Restraint
Vicious cycleViolent muscle activity
Respiratory muscle energy deficit
Muscle weakness
Hypercatabolic state
Increased oxygen demand
Stress on heart
• Extreme physical energy expenditure generates excessive production of adrenalin and
noradrenalin. • A progressively increasing amount of these body
chemicals in the individuals system can occur creating a
• “hyper- catabolic state”.
• A hyper-catabolic state can weaken all the body's muscles especially the
• Respiratory muscles.
• The hyper-catabolic state also puts “stress” on the heart by increasing its workload
(requiring faster and stronger contractions). • Thus the heart needs more than normal
amounts of oxygen in order to keep it functioning.
• If an individual with severe respiratory muscle fatigue is restrained in a position that
impairs or prevents breathing it is easy to understand why asphyxia can occur so
quickly!
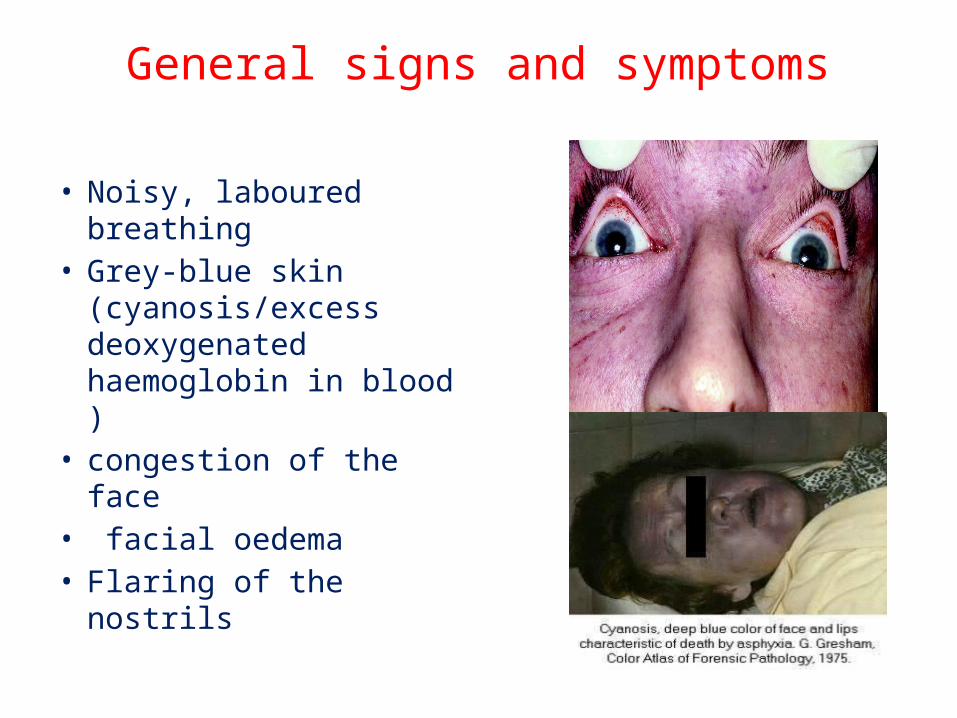
General signs and symptoms
• Noisy, laboured breathing
• Grey-blue skin (cyanosis/excess deoxygenated haemoglobin in blood )
• congestion of the face• facial oedema• Flaring of the nostrils
• Reversed movement of the chest while breathing; the chest wall will suck in as the casualty breathes in.
• Drawing in of the chest wall between the ribs and of the soft spaces above the collarbones and breastbone.
How to asphyxiate
• Compression to neck• Compression to chest/back/torso• Obstructed airways/vomiting• Chemical/environmental• Postural position
Distress signs
• Gurgling gasping sounds.
• Extremities cold to touch
• Face becomes flush or ashy
• Bleeding or bruising
• Seizures
• Unconsciousness
• Complaints of “I can’t breathe” or “I have chest pain”
• Limpness of the arms and legs
• A violent and loud individual suddenly changes to a passive, quiet, tranquil.
Safety points
Avoid putting direct weight or pressure on chest, stomach or back
Never put pressure on the neck or put the head in a position that compresses the neck
Never restrain on a soft surface (mattress) or place a pillow, towel under the head or
over the mouth.
Achieve a kneeling, sitting or standing position as soon as practical.
Monitor the individual’s vital signs.
Get medical assistance immediately if you have any concerns about the condition of
the individual under restraint.
Staff made aware of basic warning signs and of respiratory distress.
Must be able to recognise factors that contribute to Positional Asphyxia (medical
history, use of drugs, etc).
Vigilant monitoring of the person’s condition must be stressed.
Recent history i.e. past 24 hours – drug taking, alcohol use etc.
Medical history – establish any heart complaint, breathing problems etc.
thanks
Recommended