Positioning and Early
Mobilisation in Acute Stroke
Claire Simcox Highly Specialist Physiotherapist
Stroke and Neurology

Objectives
• Discuss the importance of good positioning in acute
stroke
• Discuss shoulder care in acute stroke
• Review seating options for stroke patients
• Discuss the importance of early mobilisation
• Review aids and equipment to facilitate mobility of
stroke patients

Positioning Seating Mobilisation
Care and support of the affected upper limb

Hemiplegic shoulder pain (HSP)
• Around one quarter of patients develop HSP following
stroke, which is associated with poor recovery of arm
movement and function
• Multi-factorial cause
- subluxation, soft tissue damage, spasticity
• May result from trauma caused by incorrect moving and
handling

Upper limb after stroke

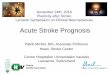
Subluxation

Reducing the risk of HSP
• Careful positioning with weight of limb supported
• Careful handling of the affected arm
• Avoid mechanical stress and excessive range of motion
(RCP 2016)

Positioning the upper limb
Always ensure the affected arm is well supported
Bexhill Arm Rest

Positioning the upper limb
Use pillows to support affected arm whilst seated (chair)

Positioning the upper limb
DO NOT allow the affected arm to hang / be unsupported
X X X

Handling the upper limb- rolling
X

Handling the upper limb- transfers
X X

Supporting the upper limb during
transfers & mobility
Slings should only be used
for transfers and walking
When in bed / chair sling
should be removed and arm
positioned appropriately

Positioning Seating Mobilisation
Care and support of the affected upper limb

Aims of Positioning
Avoid
- Skin damage
- Limb swelling
- Shoulder pain and
subluxation
- Contractures
- Aspiration and
respiratory complication
Promote:
- Comfort
- Maintenance of soft
tissue length
- Function
- Hydration and nutrition
(RCP 2016)

Supine
• Neutral head, neck and trunk alignment
• Upper limb supported
• Neutral hip/knee/ankle position
• Least recommended bed position
Advantages May enhance cerebral perfusion
Disadvantages
Risk of aspiration
Difficulty swallowing
Reduced social interaction

Side lying – weaker side
• Neutral head, neck, and trunk alignment • Upper limb alignment - scapular protraction, shoulder flexion and external rotation • Lower limb alignment
Advantages Able to use unaffected upper
limb
Disadvantages
Difficult to align affected side
Risk of shoulder injury

Side lying – stronger side
• Neutral head, neck, and trunk alignment • Upper limb supported • Lower limb alignment
Advantages Able to position affected side
Encourage use of affected side
Disadvantages
Unable to use unaffected upper
limb

Sitting upright
• Neutral head, neck and trunk
• Upper limb supported
• Neutral hip/knee/ankle position
Advantages Improved lung volumes and oxygenation
Reduced risk of aspiration
Optimal position to swallow safely
Patient able to eat, drink and socially interact more easily
Disadvantages
May reduce cerebral perfusion
May be tiring to maintain for prolonged periods

Adjuncts to Positioning

Positioning Seating Mobilisation
Care and support of the affected upper limb

Seating stroke patients
• Safe seating is considered an essential component of early
mobilisation and rehabilitation post-stroke
• Seating should enable a position that is erect, symmetrical and
aligned to support the natural anatomical structure of the body and
prevent the development of complications
• Different seating options are available dependent upon the patient’s
impairments

Seating options
Standard armchair
- Independent sitting balance or
minimal assistance to maintain sitting
balance
- Upper limb support may be required

Seating options
Wheelchair
- Provides more support than
regular armchair
- Can be used with alternative back
rests, lumbar rolls, lateral supports, arm
rest, cushions
- Enables patient transport

Lateral support and back rest
Bexhill arm rest

Seating options
Specialist wheelchair e.g. tilt in space
- Patients with limited head and trunk control
- Patients with limited physical endurance

Seating considerations
• Transfer method into and out of chair
• Physical ability to maintain seated position
- medical stability - head and trunk control
- physical endurance - pusher syndrome
• Cognitive and behavioural state
- confusion and disorientation - fluctuating attention
- impulsivity - reduced insight
• Team decision – Communication is vital!

Positioning Seating Mobilisation
Care and support of the affected upper limb

How Does Stroke Affect Mobility?
Stroke
Weakness
Balance
Vision
Inattention /
Neglect
Spasticity
Cognition
Sensory
Impairment
Pain
Nutrition
Plus many more……

Effects of immobilisation
Body system Effect
Musculoskeletal muscle weakness and wasting
reduced bone density
Respiratory reduced lung volumes
increased work of breathing
increased risk of lung collapse and pneumonia
Cardiovascular orthostatic intolerance
increased resting HR, decreased maximal cardiac output,
increased risk of DVT
Psychological reduced mood
increased risk of depression

Early mobilisation (24-48hrs)
• Early mobilisation aims to reduce the risks of bed
rest/inactivity and minimise post-stroke complications
• Early start of intensive stroke rehabilitation may be
associated with:
- greater and faster improvement of activities after stroke
- reduced length of hospital stay

Very early mobilisation
• AVERT study
• 2000 patients
• 92% mobilised with 24 hours (23% within 12 hours)
• Average of 6 times per day (therapists and nursing)
• No effect on immobility related complications
• No effect on walking recovery
• Greater disability at 3 month follow up

Benefits of early mobilisation
• Optimal time to commence mobilisation is not clear from the
literature
• Very early mobilisation i.e. within 24 hours post stroke is safe
and feasible
• However, the addition of very frequent mobilisation within 24
hours may not offer additional benefit and is not recommended
(AVERT, 2015)

Mobilising stroke patients
Mobilising a stroke patient requires individualised assessment of patient’s
impairments
- Cognition: alertness, confusion, safety awareness, neglect
- Communication: do they follow commands? can they express their needs?
- Vision: visual field loss e.g. hemianopia; diplopia
- Head and trunk control
- Lower limb function: extensor muscles to weight-bear, flexor muscles to
step
- Upper limb function: important for different types of equipment e.g. stick,
frame

Risk assessment for mobilising stroke
patients
T - Task
I - Individual
L - Load
E - Environment

Transfer and mobility methods
Hoist
Rota-stand
Pivot transfer
Step transfer
Walking frame
Walking stick
No aids
Dependent
Independent


•Used for patient’s with a foot drop
•Help to clear the foot from the
floor which helps with stepping
during mobility/ transfers when
worn inside a shoe
•Common pressure areas need to
be checked regularly (heel, along
edges of AFO) to prevent pressure
areas.
Ankle-Foot Orthoses (AFO)

Summary:
• Positioning requires a 24 hour approach by all members of the
MDT and is individual to each patient
• Specialist equipment is available to facilitate early seating /
mobilisation of acute stroke patients
• Mobilisation should begin within 24-48 hours of stroke – initially at
a low intensity
• Particular attention needs to be paid to the affected upper limb at
all times

References
1) WHO, World Health Assembly, 2005 2) UN Convention for the Rights of People with Disabilities, Article 26, 2008 3) Bernhardt J, Thuy MN, Collier JM, Legg LA. Very early versus delayed mobilisation after stroke. Cochrane
Database Systematic Review 2009; 1: CD006187 4) Stroke Unit Trialists’ Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database
Systematic Review 2007; 4: CD000197 5) Early Supported Discharge Trialists. Services for reducing duration of hospital care for acute stroke patients.
Cochrane Database Systematic Review 2005; 2: CD000443 6) Kwakkel G, van Peppen R, Wagenaar RC, Wood-Dauphinee S, Richards C, Ashburn A et al. Effects of
augmented exercise therapy time after stroke: a meta-analysis. Stroke 2004; 35: 2529–2539 7) French B, Thomas LH, Leathley MJ, Sutton CJ, McAdam J, Forster A et al. Repetitive task training for
improving functional ability after stroke. Cochrane Database Systematic Review 2007; 4: CD006073 8) van de Port IG, Wood-Dauphinee S, Lindeman E, Kwakkel G. Effects of exercise training programs on walking
competency after stroke: a systematic review. American Journal of Physical Medicine and Rehabilitation 2007; 86: 935–951
9) Kwakkel G, Wagenaar RC, Twisk JW, Lankhorst GJ, Koetsier JC. Intensity of leg and arm training after primary middle-cerebral-artery stroke: a randomised trial. Lancet 1999; 354: 191–196

References
10) AVERT Trial Collaboration Group. Efficacy and safety of very early mobilisation within 24 hours of stroke onset (AVERT): a randomised controlled trial. Lancet 2015; 386(9988): 46-55
11) Kwakkel G, Wagenaar RC, Koelman TW, Lankhorst GJ, Koetsier JC. Effects of intensity of rehabilitation after stroke. A research synthesis. Stroke 1997;28(8):1550 – 1556
12) Langhorne P, Wagenaar R, Partridge C. Physiotherapy after stroke: More is better? Physiotherapy Research International 1996;1(2):75 – 88
13) Indredavik B, Bakke F, Slordahl SA, Rokseth R, Haheim LL. Treatment in a combined acute and rehabilitation stroke unit: which aspects are most important? Stroke1999; 30(5): 917–923
14) Maulden SA, Gassaway J, Horn SD, Smout RJ, DeJong G. Timing of initiation of rehabilitation after stroke. Archives of Physical Medicine and Rehabilitation 2005; 86(12): S34–40
15) Truong AD, Fan E, Brower RG and Needham DM. Bench-to-bedside review: Mobilizing patients in the intensive are unit from pathophysiology to clinical trials. Critical Care Medicine 2009; 13(216): 1-8
16) Auriel E and Bornstein NM. Early mobilisation following stroke. European Neurological Review 2013; 8(2): 141-143
17) Bernhardt J, Dewey H, Thrift A, Collier J, Donnan G. A very early rehabilitation trial for stroke (AVERT): phase II safety and feasibility. Stroke 2008; 39(2):390–396
18) McGlinchey M, Walmsley N and Cluckie G. Positioning and pressure care. In: Bhalla A, Birns J, editors. Management of Post-Stroke Complications. Springer; 2015. p189-225

References
1) McGlinchey M, Walmsley N and Cluckie G. Positioning and pressure care. In: Bhalla A, Birns J, editors. Management of Post-Stroke Complications. Springer; 2015. p189-225
2) Ada L, Goddard E, McCully J, Stavrinos T, Bampton J. Thirty minutes of positioning reduces the development of shoulder external rotation contracture after stroke: a randomized controlled trial. Archives of Physical Medicine and Rehabilitation 2005; 86: 230–234
3) Dean CM, Mackey FH, Katrak P. Examination of shoulder positioning after stroke: a randomised controlled pilot trial. Australian Journal of Physiotherapy 2000; 46: 35–40
4) de Jong LD, Nieuwboer A, Aufdemkampe G. Contracture preventive positioning of the hemiplegic arm in subacute stroke patients: a pilot randomized controlled trial. Clinical Rehabilitation 2006; 20: 656–667
5) Gustafsson L, McKenna K. A programme of static positional stretches does not reduce hemiplegic shoulder pain or maintain shoulder range: a randomized controlled trial. Clinical Rehabilitation 2006; 20: 277–286
6) Horsley SA, Herbert RD, Ada L. Four weeks of daily stretch has little or no effect on wrist contracture after stroke: a randomised controlled trial. Australian Journal of Physiotherapy 2007; 53: 239–245
7) Turton AJ, Britton E A pilot randomized controlled trial of a daily muscle stretch regime to prevent contractures in the arm after stroke Clinical Rehabilitation 2005; 19: 600 -612
8) Chatterton HJ, Pomeroy V, Gratton J. Positioning for stroke patients: a survey of physiotherapists’ aims and practices. Disability and Rehabilitation 2001; 23(10): 413–421

References
9) Rowat AM. What do nurses and therapists think about the positioning of stroke patients? Journal of Advanced Nursing 2001; 34(6): 795–803
10) Mee LYS, Bee WH. A comparison study on nurses’ and therapists’ perception on the positioning of stroke patients in Singapore General Hospital. International Journal of Nursing Practice 2007; 13: 209–221
11) Schwarz S, Georgiadis D, Aschoff A, Schwab S. Effects of body position on intracranial pressure and cerebral perfusion in patients with large hemispheric stroke. Stroke 2002; 33: 497–501
12) Wojner-Alexandrov AW, Garami Z, Chernyshev OY and Alexandrov AV. Flat positioning improves blood flow velocity in acute ischaemic stroke. Neurology 2005; 64: 1354-1357
13) Tyson SF and Nightingale O. The effects of position on oxygen saturation in acute stroke: a systematic review. Clinical Rehabilitation 2004; 18: 863-871
14) Smith M. Management of hemiplegic shoulder pain following stroke. Nursing Standard 2012; 26(44): 35–44
15) Zeferino SI, Aycock DM. Post-stroke shoulder pain: inevitable or preventable? Rehabilitation Nursing 2010; 35(4): 147–51
16) Paci M, Nannetti L, Taiti P, Baccini M, Pasquini J, Rinaldi L. Shoulder subluxation after stroke: relationships with pain and motor recovery. Physiotherapy Research International 2007;12(2): 95–10

References
17) Ratnasabapathy Y, Broad J, Baskett J, Pledger M, Marshall J, Bonita R. Shoulder pain in people with a stroke: a population-based study. Clinical Rehabilitation 2003; 17(3): 304-311
18) Lindgren I, Jönsson A-C, Norrving B, Lindgren A. Shoulder pain after stroke: a prospective population-based study. Stroke 2007; 38: 343-348
19) Dromerick AW, Edwards DF, Kumar A. Hemiplegic shoulder pain syndrome: frequency and characteristics during inpatient stroke rehabilitation. Archives of Physical Medicine and Rehabilitation 2008; 89(8): 1589-1593
20) Gardner MJ , Ong BC, Liporace F, Koval KJ. Orthopedic issues after cerebrovascular accident. American Journal of Orthopaedics 2002; 31(10): 559-568
21) Huang Y-C, Liang P-J, Pong Y-P, Leong C-P, Tseng C-H. Physical findings and sonography of hemiplegic shoulder in patients after acute stroke during rehabilitation. Journal of Rehabilitation Medicine 2010: 42(1): 21-26
22) Lo S-F, Chen S-Y, Lin H-C, Jim Y-F, Meng N-H, Kao M-J. Arthrographic and clinical findings in patients with hemiplegic shoulder pain. Archives of Physical Medicine Rehabilitation 2003; 84(12): 1786-1791
Recommended