
Practice Variations Between Emergency Medicine and
Pediatric Physicians in the Treatment of URI’s
Nicole Colucci, DO, MAAP Nicole Colucci, DO, MAAP Resident, Emergency MedicineResident, Emergency Medicine
Resurrection Medical CenterResurrection Medical Center
Author and Co-investigators:Author and Co-investigators:
Mary Frances Kordick, MBA, PhD, RN, CNAA,BCMary Frances Kordick, MBA, PhD, RN, CNAA,BC
Shu Chan, MD, MS, FACEPShu Chan, MD, MS, FACEP
We are indebted to:We are indebted to:
All Survey Respondents All Survey Respondents
Study Team

INTRODUCTION/BACKGROUND
High prevalence of URI’s seen in the High prevalence of URI’s seen in the emergency departmentemergency department Most common cause of illness in Most common cause of illness in
childrenchildren Overuse of unnecessary antimicrobialsOveruse of unnecessary antimicrobials
Increasing antimicrobial resistance Increasing antimicrobial resistance patternspatterns
Sources: Ipp M, Carson S, Petric M, Parkin PC. Rapid painless diagnosis of viral respiratory infection. Arch Dis Child 2002; 86(5):372-373. Jacobs RF. Judicious use of antibiotics for common pediatric respiratoryinfections. Pediatr Infect Dis J 2000; 19(9):938-943.

STUDY OBJECTIVE
Examine practice variations between Examine practice variations between emergency medicine and pediatric emergency medicine and pediatric physicians focusing on:physicians focusing on: The diagnosis and management of The diagnosis and management of
children with respiratory signs/ children with respiratory signs/ symptomssymptoms
Specifically, URI’s Specifically, URI’s

CLINICAL RELEVANCE Reduce future resistance to Reduce future resistance to
antibiotics antibiotics Monetary impact Monetary impact Identify future areas for improving Identify future areas for improving
education to physicianseducation to physicians All previous studies evaluate All previous studies evaluate
pediatricianspediatricians
Sources:Jacobs RF. Judicious use of antibiotics for common pediatric respiratory infections. Pediatr Infect Dis J 2000; 19(9):938-943.Boccazzi A, Noviello S, Tonelli P, Coi P, Esposito S, Carnelli V. The decision-making process in antibacterial treatment of pediatric upper respiratory infections: A national prospective office-based observational study. Int J Infect Dis 2002; 6(2):103-107.

STUDY DESIGN Following acceptance by the IRB, a 22-item Following acceptance by the IRB, a 22-item
questionnaire questionnaire focusing on the diagnosis and focusing on the diagnosis and management of children(<15 years) with URI’s management of children(<15 years) with URI’s was e-mailed to all members was e-mailed to all members listed in listed in directories of SAEM and the AAP-subsection of directories of SAEM and the AAP-subsection of pediatric emergency medicinepediatric emergency medicine
A cover letter explaining the survey was sent A cover letter explaining the survey was sent with a hyperlink to the web-based survey sitewith a hyperlink to the web-based survey site (Formsite.com)(Formsite.com)
Repeat e-mails were sent at weeks 3-4 after Repeat e-mails were sent at weeks 3-4 after the initial mailingthe initial mailing

SURVEY QUESTIONS
Do you utilize the diagnosis of upper respiratory Do you utilize the diagnosis of upper respiratory infection (URI)?infection (URI)?
Is there an age in which URI is not an appropriate Is there an age in which URI is not an appropriate diagnosis?diagnosis? If you answered “yes” to the previous question, If you answered “yes” to the previous question,
choose your age criterion?choose your age criterion?
Do you document pulse oximetry in children with Do you document pulse oximetry in children with respiratory symptoms?respiratory symptoms?

SURVEY QUESTIONS Is there an age criterion in which you always Is there an age criterion in which you always
order a CXR to exclude evidence of order a CXR to exclude evidence of pneumonia or other pathology?pneumonia or other pathology?
Is there a season in which you order a CXR Is there a season in which you order a CXR
more frequently?more frequently?
Do you prescribe or recommend medications Do you prescribe or recommend medications when you diagnose URI?when you diagnose URI?
If you did not intend to provide a prescription If you did not intend to provide a prescription for medication and the parent requests an for medication and the parent requests an antibiotic, what describes your most frequent antibiotic, what describes your most frequent action?action?
DATA ANALYSIS
Data downloaded from Formsite.comData downloaded from Formsite.com
Descriptive and chi-square statistics were Descriptive and chi-square statistics were completed using the Statistical Package completed using the Statistical Package for Social Sciences for Windows Version for Social Sciences for Windows Version 11.511.5

RESULTS
3739 e-mails sent via two separate 3739 e-mails sent via two separate mailingsmailings Response Rate: 26.3%, N=728Response Rate: 26.3%, N=728 Population:Population:
EM physicians, 73.8% (n = 539)EM physicians, 73.8% (n = 539)Pediatric EM physicians, 24.0% (n = Pediatric EM physicians, 24.0% (n =
175)175)Remainder: non-physician practitioners Remainder: non-physician practitioners
and eliminated from the studyand eliminated from the study

DEMOGRAPHICS Similar for both groupsSimilar for both groups
Gender: Male-70.3%Gender: Male-70.3% Board eligibility/certification: 81-84%Board eligibility/certification: 81-84% Primary site of practice: Primary site of practice:
Urban/Academic Medical CentersUrban/Academic Medical Centers
Different between the groups of Different between the groups of physiciansphysicians Pediatric population of patients seenPediatric population of patients seen
EM-25%EM-25%PEM-75-100%PEM-75-100%

RESULTS EM physicians are more likely to confine EM physicians are more likely to confine
the diagnosis of URI to certain age groups the diagnosis of URI to certain age groups (EM-49.9% vs PEM-29.1%; P=0.000)(EM-49.9% vs PEM-29.1%; P=0.000) >8 years old>8 years old Both groups agree that URI is an Both groups agree that URI is an
inappropriate diagnosis in children < inappropriate diagnosis in children < 1 month old1 month old
PEM are less likely to use antibiotics, PEM are less likely to use antibiotics, decongestants or antihistamines for decongestants or antihistamines for treatment in pediatric URI’s treatment in pediatric URI’s (next slide)(next slide)
Saline drops, antipyreticsSaline drops, antipyretics
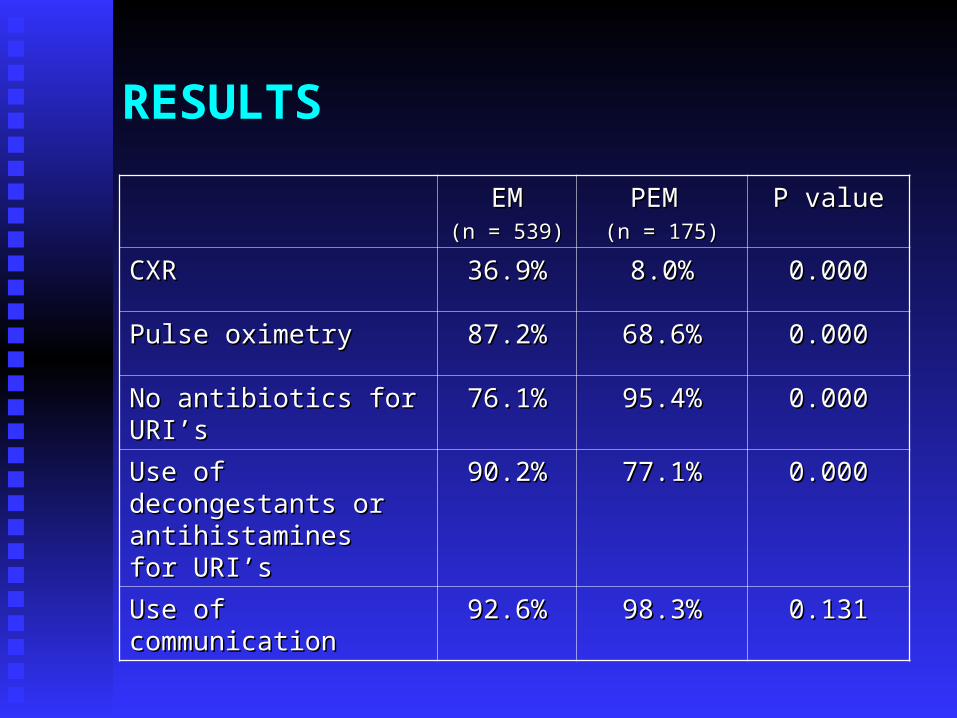
EMEM(n = 539)(n = 539)
PEM PEM (n = 175)(n = 175)
P valueP value
CXRCXR 36.9%36.9% 8.0%8.0% 0.0000.000
Pulse oximetryPulse oximetry 87.2%87.2% 68.6%68.6% 0.0000.000
No antibiotics for No antibiotics for URI’sURI’s
76.1%76.1% 95.4%95.4% 0.0000.000
Use of decongestants Use of decongestants or antihistamines for or antihistamines for URI’sURI’s
90.2%90.2% 77.1%77.1% 0.0000.000
Use of communicationUse of communication 92.6%92.6% 98.3%98.3% 0.1310.131
RESULTS

DISCUSSION Pulse oximetry should be the fifth vital Pulse oximetry should be the fifth vital
sign in children with respiratory sign in children with respiratory signs/symptomssigns/symptoms InexpensiveInexpensive Diagnose mild to moderate hypoxia Diagnose mild to moderate hypoxia
unsuspected by physical examunsuspected by physical exam CXR should be ordered on children with CXR should be ordered on children with
respiratory signs/symptoms:respiratory signs/symptoms: 0-3 months age, abnormal SaO2, 0-3 months age, abnormal SaO2,
occult fever work-upoccult fever work-up
Sources:Mower WR, Sachs C, Nicklin EL, Baraff LJ. Pulse oximetry as a fifth pediatric vital sign. Pediatrics 1997; 99(5):681-686. Baraff LJ. Management of fever without source in infants and children. Ann Emerg Med 2000; 36(6):602-614.

DISCUSSION Multiple sources agree that the most Multiple sources agree that the most
common cause of URI’s is viral and has no common cause of URI’s is viral and has no indication for antibioticsindication for antibiotics
Studies on the efficacy of the use of Studies on the efficacy of the use of antihistamines, cough suppressants and antihistamines, cough suppressants and mucolytics in the treatment of URI’s do not mucolytics in the treatment of URI’s do not change the course of the illnesschange the course of the illness
Sources: Morikawa M. Upper respiratory infection in acute pediatric care in internal conflict, Kosovo, 1999. J Trop Pediatr 2001; 47(6):379-382. Nambiar S, Schwartz RH, Sheridan MJ. Are pediatricians adhering to principles of judicious antibiotic use for upper respiratory tract infections? South Med J 2002; 95(10):1163-1167.
LIMITATIONS
Survey response rate of 26.3% with two Survey response rate of 26.3% with two mailingsmailings Allow for a third mailingAllow for a third mailing
Limited populationLimited population Utilize more databases(ACEP, SAEM, Utilize more databases(ACEP, SAEM,
AAP)AAP)
Unable to clearly define specific prescribing Unable to clearly define specific prescribing patterns of antibiotics/ decongestantspatterns of antibiotics/ decongestants More precise questionsMore precise questions
No specific definition for URINo specific definition for URI

CONCLUSIONS
Practice differences exist between Practice differences exist between emergency medicine and pediatric emergency medicine and pediatric emergency medicine physiciansemergency medicine physicians
Areas for additional education in both Areas for additional education in both groups of physiciansgroups of physicians Indications for diagnostic testsIndications for diagnostic tests Lack of indication for antibiotics in the Lack of indication for antibiotics in the
treatment of viral URI’streatment of viral URI’s Use of supportive care as treatment Use of supportive care as treatment
for URI’sfor URI’s Allowing the physician to offer non-Allowing the physician to offer non-
medication options to caregiversmedication options to caregivers
Recommended







![VARIATIONS GOLDBERG [ARIA et 30 variations] · Title: VARIATIONS GOLDBERG [ARIA et 30 variations] Author: Bach, Johann Sebastian - Arranger: Montreuille, Pierre - Publisher: Montreuille,](https://img.pdfslide.net/doc/110x75/610885d0028fe95f64358299/variations-goldberg-aria-et-30-variations-title-variations-goldberg-aria-et.jpg)









