
Results: A total of 11043 TTECG were obtained (mean 84.3/patient). Ingroup A 20/64 (31.2%) had AF recurrences compared with 50/67 (74.6%)group B patients (p�0.001). The percentage of patients with both symp-tomatic and asymptomatic recurrence were not different between the twogroups (6/20 in group A, 11/53 in group B). Also the percentage of patientswith only asymptomatic AF recurrence was not different between the twogroups (6/20, 30%, in group A; 7/53, 13%, in group B) (p�0.1). Theoverall percentage of patients with asymptomatic AF recurrence was sig-nificantly higher in group A (12/20 patients, 60%) compared with group B(18/53, 33.9%)(p�0.04).Conclusions: Asymptomatic AF recurrence are more frequent in patientswho underwent RCA as compared with patients treated with AAD alone.Placebo effect, denervation and cavo-tricuspid isthmus ablation mightcontribute to this.
AB8-5
LINEAR ABLATION OF THE MITRAL ISTHMUS DURINGATRIAL FIBRILLATION ABLATION INCREASES THEINCIDENCE OF LEFT ATRIAL TACHYCARDIAJesse S. Sethi, MD, Bryan T. Piedad, MD, John R. Bullinga,MD, Douglas S. Holmes, MD, Neil E. Bernstein, MD andLarry A. Chinitz, MD. NYU Medical Center, New York, NY.
Background: Catheter ablation of the left atrial mitral isthmus (LAMI)during atrial fibrillation (AF) ablation has been shown to incrementallyreduce the incidence of AF recurrence. It is not clear if LAMI conductionblock is necessary to achieve these clinical benefits. We sought to evaluatethe efficacy of an anatomic approach to the deployment and completion ofthis linear ablation as opposed to the use of LAMI conduction block as anelectrophysiologic endpoint.Methods and Results: We studied 101 consecutive patients (age 53.3 �11.6 years, 82 males) with either paroxysmal (84 pts) or persistent (17 pts)AF who underwent left atrial circumferential ablation with an 8mm tipcatheter using a non-fluoroscopic, three-dimensional navigation system(NavX, Endocardial Solutions) followed by segmental ostial ablation toensure electrical isolation of the pulmonary veins (PVs). A linear LAMIablation from the left inferior PV to the lateral mitral annulus was deliveredin 47 (46.5%) of the patients. At a mean follow-up of 6.9 � 3.8 months,the incidence of AF recurrence was 23.4% in patients who received aLAMI ablation compared with 11.1% in patients who did not undergoLAMI ablation (p�0.12). The incidence of clinically significant left atrialtachycardia (LAT) within the first three post-procedure months was 17.0%in patients who received a LAMI ablation compared with 1.9% in patientswho did not (p�0.01). The locations of the LAT were the posterior mitralisthmus (n�4, 4 of 4 pts had received LAMI ablation) and the posterior leftatrial roof (n�5, 4 of 5 pts had received LAMI ablation). There was nosignificant correlation between male sex, persistent AF, hypertension, di-abetes, LA size � 4cm or ejection fraction � 55% and the incidence ofLAT recurrence.Conclusions: In patients undergoing pulmonary vein isolation, the additionof an anatomically guided LAMI ablation does not reduce AF recurrenceand is associated with a significantly higher incidence of LAT.
AB8-6
COMPLETE MITRAL ISTHMIC BLOCK IS NOT REQUIRED TOPREVENT ATRIAL TACHYCARDIA AFTER CIRCUMFERENTIALPULMONARY VEIN ABLATIONCarlo Pappone, MD, PhD, Giuseppe Augello, MD, PatrizioMazzone, Takeshi Tomita, Gabriele Vicedomini and VincenzoSantinelli, MD. San Raffaele University Hospital, Milan,Italy.
Background: Left atrial tachycardia (LA AT) is the most frequent com-plication after standard circumferential PV ablation (CPVA). As the ma-jority of these incisional tachycardias seem to be mitral isthmus dependent,an ablation line at this site is required. However, the amount of conduction
delay/block across this isthmus needed to prevent the occurrence of LA ATis not known.Methods: 643 consecutive patients underwent CPVA with an adjunctiveisthmic line. After ablation this line was considered complete if we ob-tained a minimum amount of 80 ms between widely spaced double poten-tials across the line while pacing from the coronary sinus. Activationmapping validation using CARTO was not routinely assessed. The occur-rence of AF and atrial tachycardia in the first 6 months after ablation wassystematically assessed in all patients by obtaining a minimum of 2 weeklytranstelephonic monitoring for 6 months.Results: Follow-up was completed by 619 patients. Atrial fibrillationrecurred in 12% of patients with paroxysmal AF and 21% of those withchronic arrhythmia. Atrial tachycardia occurs in 14% of patients, withspontaneous resolution at one month in 55%. Patients were categorized intotertiles according to the amount of conduction delay/block across theisthmic line (group 1, 80 to 120 ms, group 2 120 to 150 ms, group 3 �150ms; mena time for drawing isthmic line: 5.2 min, 8.3 min, 16.3 min). Alogistic multivariable regression analysis was performed to determine sep-arate predictors of atrial fibrillation and atria tachycardia. Among severaltested variables, only the amount of encircled area, LA size �45mm and noelicitation/abolition of vagal reflexes were associated with AF 6 monthsafter ablation (p�0.001 for all 3 variables). The only predictors of LA ATafter CPVA were an enlarged LA (�45mm) and an amount of isthmicblock � 120 ms. AT occurred in 3.9%, 4.5% and 13.3%.Conclusions: Complete isthmic block (with a minimum amount of 150 ms)is time consuming and not required for preventing LA AT; however, aminimum of 120 ms of conduction delay across the ablation line isrequired.
ABSTRACT SESSION 9: DEVICES III: Treatment of AtrialTachyarrhythmias with Implantable DevicesThursday, May 5, 200511:15 a.m.–12:45 p.m.
AB9-1
PREDICTORS OF ATRIAL FIBRILLATION PROGRESSION IN APACEMAKER POPULATION: ROLE OF ATRIAL FIBRILLATIONSUPPRESSION ALGORITHMS*Roger A. Freedman, MD, *Robert Graumann, *JosephAlonso, MD, *Anil Chhabra, MD, *Kent Volosin, MD,*Xiaozheng Zhang, MD and Investigators from the RARETrial. University of Utah, Salt Lake City, UT, St. JudeMedical, Sylmar, CA, Central Florida Heart Center, Ocala,FL, Willis Knighton, Shreveport, LA and PENN Cardiology,Cherry Hill, NJ.
Background: Atrial fibrillation (AF) is a progressive condition with naturalhistory typically showing increasing frequency of episodes. The presentstudy examines changes in AF frequency in a large cohort of patientsimplanted with a dual-chamber pacemaker with a programmable atrialfibrillation suppression algorithm (AFx).Methods: A total of 1319 patients were implanted, primarily for sinus nodedysfunction, with a dual-chamber pacemaker having programmable AFx.During follow-up, episodes of atrial fibrillation were defined as automaticmode switch episodes triggered by atrial rates �220 bpm lasting �20minutes. AFx was programmed on, at physician discretion, in 507 patients(38.4%). Patients were followed for a mean of 4.1 months (range, 3-6months). The independent predictive variables of AF progression wereassessed by multivariate analysis. Variables examined were gender, age,initial frequency of AF, hypertension, coronary artery disease (CAD), leftventricular ejection fraction (LVEF), NYHA class, and AFx turned on oroff.Results: Among all 1319 patients (age 75.9�9.9; LVEF 53.5�11.6;51,3% male; 27.0% with NYHA II-IV; 47.7% with hypertension and36.5% with CAD), the monthly frequency of AF was 3.6�17.9 at onemonth after implantation, 2.2�10.6 at 3 months, and 2.3�13.8 at 6months. The results of the multivariate analysis showed that independent
S16 Heart Rhythm, Vol 2, No 5, May Supplement 2005
predictors of increase in AF frequency were low initial frequency of AF(p�0.0008) and AFx turned off (p�0.0176). The interaction betweeninitial frequency of AF and AFx was not significant (p�0.1534).Conclusions: In this large pacemaker population, programming on AFxwas an independent determinant of less progression of atrial fibrillation inthe first 6 months after implantation.
AB9-2
ATRIAL ANTITACHYCARDIA PACING IS MOST EFFECTIVE ATNIGHTLana E. Boodhoo, MRCP, Andrew R. Mitchell, MD, SpyrosArvanitakis, MRCP, Guy W. Lloyd, MD, Nikhil Patel, MD,FRCP, Kayvan Kamalvand, MD, S. O’Nunain, MD and *NeilSulke, MD, FRCP. Eastbourne General Hospital, Eastbourne,United Kingdom, William Harvey Hospital, Ashford, UnitedKingdom and Royal Sussex Hospial, Brighton, UnitedKingdom.
Background: Atrial antitachycardia pacing (ATP) has been demonstratedto be successful in over 50% of AT/AF episodes in patients with parox-ysmal AF. The aim of this study was to assess whether there is a circadianvariation in the effectiveness of atrial ATP.Methods: Thirty patients, mean age 70�9 years, 55% male, withMedtronic AT500 pacemakers implanted for paroxysmal AT/AF werefollowed over 3 months. ATP efficacy was assessed by manual inspectionof stored atrial electrograms (EGMs).Results: Atrial ATP was delivered to 5,555 arrhythmias, of which 715were recorded and analysed. ATP efficacy peaked nocturnally between9PM and 3AM, and was least effective between 9AM and 3AM, (49%versus 24%, p�0.0003). There was no difference in the mean arrhythmiacycle lengths between these two periods (202 � 32 versus 201 � 29 ms,p�0.9).Conclusion: ATP efficacy is maximal at night, for reasons which areunclear. These findings may allow improved pacemaker and hybrid treat-ment of paroxysmal atrial fibrillation.
AB9-3
THE LEAF (LOW ENERGY IN ATRIAL FIBRILLATION) STUDYRESULTS: EVALUATION OF DEVICE BASED THERAPIES FORATRIAL TACHYARRHYTHMIA PREVENTION ANDTERMINATIONPhilippe Mabo, MD, PhD and The LEAF study group. LEAFInvestigator european centers, France.
The LEAF study was a prospective, randomized, single blind, crossover,multi-center trial designed to evaluate the impact on atrial tachyarrhythmia(AT) burden of prevention and antitachycardia pacing (ATP) featuresincorporated in a new DDDRT device.Method: 243 patients (52.7% male, 72�9 years) were implanted with theMedtronic AT500TM pacemaker in 44 european centers between Septem-ber 2000 and 2002. All patients had a conventional indication for dualchamber pacing (AVB�12.3%, SND�75.3%) and at least two episodes ofAT within the last 12 months. One month after implantation patients wererandomized for 2 periods of six months each, 1 therapy period (ATprevention and ATP “ON”) and 1 observation period (DDDR mode butprevention and ATP “OFF”). At each follow-up, device stored data was
saved and QoL questionnaire were completed. The primary endpoint wasto evaluate a difference in AT burden between therapy and observationperiods.Results: Complete data were obtained from 237 patients (54% were on AAdrugs: 40% on amiodarone). AT burden decreased from 2.36 hrs/dayduring the observation period to 2.14 hrs/day during the therapy period.The mean reduction was 0.32 � 20 hrs/day (p�0.25). The % ventricularpacing was high (�80%) during OFF and ON periods. Despite the inclu-sion criteria, 50% of the patients were free of AT during the study.Restrospectively selecting patients with at least one AT episode in the 1month run in period (86 patients) showed a trend toward reduction in ATburden (p � 0.05) in the ON period. Patient QoL and symptoms signifi-cantly improved in the 12 months post-implant period when compared onlywith pre-implant data (p�0.005).Conclusion: Similar to recently published trials, the LEAF study did notdemonstrate a significant effect of prevention and ATP therapies on ATburden. This may be because of methodological limitations e.g. high % Vpacing, short FU, loss of power due to the large % of patients free of AT.Retrospective selections of patients having episodes after device implan-tation showed a trend towards reduction in AT burden when ATP andprevention therapies were enabled.
AB9-4
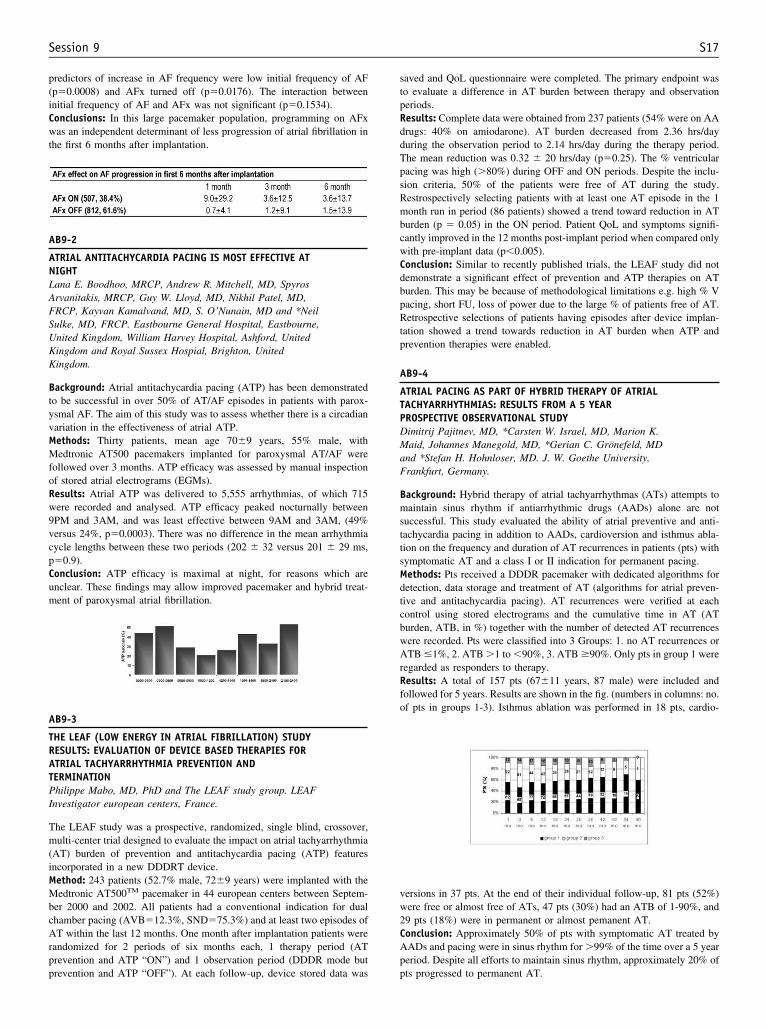
ATRIAL PACING AS PART OF HYBRID THERAPY OF ATRIALTACHYARRHYTHMIAS: RESULTS FROM A 5 YEARPROSPECTIVE OBSERVATIONAL STUDYDimitrij Pajitnev, MD, *Carsten W. Israel, MD, Marion K.Maid, Johannes Manegold, MD, *Gerian C. Gronefeld, MDand *Stefan H. Hohnloser, MD. J. W. Goethe University,Frankfurt, Germany.
Background: Hybrid therapy of atrial tachyarrhythmas (ATs) attempts tomaintain sinus rhythm if antiarrhythmic drugs (AADs) alone are notsuccessful. This study evaluated the ability of atrial preventive and anti-tachycardia pacing in addition to AADs, cardioversion and isthmus abla-tion on the frequency and duration of AT recurrences in patients (pts) withsymptomatic AT and a class I or II indication for permanent pacing.Methods: Pts received a DDDR pacemaker with dedicated algorithms fordetection, data storage and treatment of AT (algorithms for atrial preven-tive and antitachycardia pacing). AT recurrences were verified at eachcontrol using stored electrograms and the cumulative time in AT (ATburden, ATB, in %) together with the number of detected AT recurrenceswere recorded. Pts were classified into 3 Groups: 1. no AT recurrences orATB �1%, 2. ATB �1 to �90%, 3. ATB �90%. Only pts in group 1 wereregarded as responders to therapy.Results: A total of 157 pts (67�11 years, 87 male) were included andfollowed for 5 years. Results are shown in the fig. (numbers in columns: no.of pts in groups 1-3). Isthmus ablation was performed in 18 pts, cardio-
versions in 37 pts. At the end of their individual follow-up, 81 pts (52%)were free or almost free of ATs, 47 pts (30%) had an ATB of 1-90%, and29 pts (18%) were in permanent or almost pemanent AT.Conclusion: Approximately 50% of pts with symptomatic AT treated byAADs and pacing were in sinus rhythm for �99% of the time over a 5 yearperiod. Despite all efforts to maintain sinus rhythm, approximately 20% ofpts progressed to permanent AT.
S17Session 9
Recommended

















