Tariq Mughal Vice-President Medical affairs, Foundation Medicine
Professor of Hematology-Oncology
Personalized Cancer Medicine
HCA-SCRI Healthcare Meeting London; 25 Feb 2016


‘Moon-shot’ Cancer Medicine - Obama State of the Union Address, Jan 2016

Cancer Core Europe: Sep 2015 Cambridge
Cambridge Cancer Centre, Cambridge Institute Gustave Roussy, Paris Karolinska Institute, Stockholm
Netherlands Cancer Institute, Amsterdam Vall d’Hebron Institute of Oncology, Barcelona German Cancer Research Center, Heidelberg


6
20
10
201
1
20
12
20
13
20
14
20
15
Largest
Aggregation
of Validated
Oncology
Genomic
Information
68,000
+ Tests
FoundationCORE™ Knowledgebase
Significant Value Creation from Molecular Information

Personalized Cancer Medicine: Some
Conceptual thoughts
1. A brief history of precision medicine
2. What really is a driver mutation?
3. How can be best identify driver mutations?
4. Some case histories
5. Concluding thoughts

Philadelphia Chromosome: t(9;22)(q34;q11)
1960 Peter Nowell David Hungerford 1973 Janet Rowley

28 May 2001
N
N
N
H
N
H
N N
N
O
N
(C30H35N7SO4)
Imatinib mesylate
(STI571; Glivec®)

Survival for Patients with CML by Treatment Era
Courtesy of Prof H Kantarjian; adapted, with permission, from Harrison’s Principles of Internal Medicine, 2014.

EVOLUTION OF GENOME DRIVEN THERAPIES FOR CANCER
• 1970’s ER Testing and Hormonal Therapy for Breast Cancer
• 1990’s Cytogenetics/FISH Testing and Therapy for Heme Malignancies
• 1998 HER2 Testing and Trastuzumab for Breast Cancer
• 2001 BCR-ABL Testing and Imatinib for CML
• 2003 EGFR Mutation Testing and Erlotinib for NSCLC
• 2007 KRAS Mutation Testing and Cetuximab/Panitumumab for CRC
• 2010 EML4-ALK Testing and Crizotinib in NSCLC
• 2011 BRAF Mutation Testing and Vemurafenib in Melanoma
• 2012 ROS1 and RET Fusion Testing for Crizotinib and RET inhibitors in NSLC
• 2013 HER2 mutations in and targeted therapy for NSCLC, Breast Cancer, and MPUC
NTRK1 Fusion Testing and Crizotinib in NSCLC
• 2014 Pembrolizumab, Nivolumab for Melanoma and NSCLC
Olaparib for BRCA-mutated Ovarian Cancer
• 2015 Alectinib for Crizotinib-resistant ALK-mutated tumors
Osimertinib for T790M EGFR
Microsatellite instability indicates immunotherapy responses
• 2016 Tumor mutation burden indicates immunotherapy responses

12
Targeted Therapies: Evolution into a Revolution
1998 to 2000 2000 to 2005 2000 to 2010 2010 to 2015 2015 to 2020
~150 targets in development
~700 compounds evaluated
Coming Soon
Extrapolated from BioCentury Online Intelligence Database

Personalized Cancer Medicine: Some
conceptual thoughts
1. A brief history of precision medicine
2. What really is a driver mutation?
3. How can be best identify driver mutations?
4. Some case histories
5. Concluding thoughts

What is a driver mutation?
Biological definition: a mutation that directly or indirectly confers a selective growth advantage to the cell in which it occurs Clinical definition: a mutation that has significant diagnostic, prognostic, or therapeutic implications in subsets of cancer patients and for specific therapies


©2015 Foundation Medicine, Inc. | Confidential 16
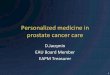
Personalized approach improves
cancer treatment outcomes
Genomics-matched targeted therapy = Best Outcome
Targeted therapy w/o mutation matching = Worst outcome
(Ref: Schwaederle et al., JCO 2015)
Response Rate to Therapy Progression Free Survival Overall Survival
P <0.001 P <0.001 P <0.001

Personalized Cancer Medicine: Some
conceptual thoughts
1. A brief history of precision medicine
2. What really is a driver mutation?
3. How can be best identify driver mutations?
4. Some case histories
5. Concluding thoughts

©2015 Foundation Medicine, Inc. 18
Test Detects Can Miss
IHC Protein expression Any alteration not known of ahead of time
FISH Copy number alterations, Rearrangements Indels, Substitutions
Hot Spot Panels Substitutions Indels, Copy number alterations, Rearrangements
Copy Number
Alterations
HER2 amplification
Trastuzumab
Insertions and
Deletions
EGFR Exon 19
Deletion- Erlotinib
Base
Substitutions
BRAF V600E
Vemurafenib
Rearrangements
ALK Fusion
Crizotinib
FOUR TYPES OF GENOMIC ALTERATIONS DRIVE TUMOR GROWTH
Limitations of traditional testing

NGS: Various Approaches • Whole Genome Sequencing (WGS)
– Determines the complete DNA sequence of an organism's genome at a single time
• Whole Exome Sequencing (WES)
– Selectively sequences only the coding areas of the genome
• Comprehensive Genomic Profiling
– Massively parallel sequencing of the entire coding region in a defined subset of genes of interest and detects all four classes of alterations
• Targeted Sequencing (Hot spot)
– Sequences only the hot spots of a subset of genes of interest

Founding Team Of Foundation Medicine Eric Lander, PhD
• Cancer genomics innovator and creator of OncoMap project
• Medical Oncology, Dana Farber Cancer Institute, Broad Institute
• NIH “New Innovator”
Levi Garraway, MD, PhD
• Recognized leader in cancer genomics, targeted therapeutics
• Founding director of Broad Institute Cancer Program
• Dana Farber, HHMI, NCI advisor
Todd Golub, MD
• Principal Investigator of The Cancer Genome Atlas program
• Clinical Pathology, Dana Farber Cancer Institute, Broad Institute
• Co-discoverer of EGFR mutations in lung cancer
Matthew Meyerson, MD, PhD
• Recognized driving force in genomics
• Founding Director of the Broad Institute
• MIT, Harvard Medical School
• Founder Millennium Pharmaceuticals
• Successful biotechnology entrepreneur
• Founder, CEO of CombinatoRx, $750M, public listing
• TR Innovator of the Year
• Boards of BIO, Forma Therapeutics, Science Museum
Alexis Borisy
2010

©2013 Foundation Medicine, Inc. | Confidential 21
Analytic Validation Demonstration of high accuracy and reproducibility required for clinical use
Controlled validation studies: Cell-line pools with known alterations:
- 2056 subs 227 indels
- 210 CNAs 32 fusions
Base Substitutions (MAF 5-100%)
Sensitivity: >99.9% PPV: >99.9%
Insertions/Deletions (1-40bp, MAF 10-100%)
Sensitivity: 98% PPV: >99%
Copy Number Alterations (>20% tumor content, zero or ≥8 copies)
Sensitivity: >95% PPV: >99%
Gene Fusions (>20% tumor content, select introns)
Sensitivity: >99% PPV: >99%
Concordance studies with existing platforms on clinical samples:
- 118 subs/indels: Sequenom, PCR
- 185 CNAs: FISH, IHC
- 43 fusions: break-apart FISH
Frampton et al, Nature Biotechnology 2013

CASE PRESENTATION
22 ©2015 Foundation Medicine, Inc. | Confidential

Drilon A, Clin Cancer Res, 2015
MSKCC vs FoundationOne Comparison: In 65% of patients, a targeted therapy was identified
Targeted agent on or off
clinical trial
Targeted therapy in NCCN guidelines
No genomic alteration identified
Genomic alterations
identified, but no targeted
therapy options available

Why FoundationONEHemeTM Test was
Developed
• Detects all clinically relevant classes of genomic alterations in hematologic and soft tissue tumors
• DNAseq of the entire coding region of 405 genes and select intronic regions in 31 genes known to be clinically & biologically relevant in cancer
• RNAseq of 265 genes recurrently rearranged in cancer
• Validated high accuracy achieved by high, uniform coverage: at median exon depth of 250x, >99.5% of exons covered >100X
• Requires only small amounts of fresh (peripheral blood/bone marrow aspirate) or FFPE clinical specimens (≥50ng of DNA, lesional tissue >20% of nucleated elements)
• Customized computational biology algorithms validated for high accuracy in clinical samples with high stromal contamination
He, et al, in press, Blood, 2016

©2015 Foundation Medicine, Inc. | Confidential 25
Combined DNA/RNA Sequencing Markedly Increases The Ability To Detect Fusion Genes
416 samples: Detected 56 distinct fusion/rearrangement events:
DNA- seq
Common isoforms: BCR-ABL1; PML-RARA;
MLL-PTD
RNA-seq 285 genes: Uncommon fusions/isoforms: BCR-ABL1; ETV6-ABL1
MYST3-CREBBP; P2RY8-CRLF2
PAX5-FLI1; ETV6-EVI1; CBFB-MYH11
NUP214-DEK; TCF3-PBX1
BOTH
405 genes: Extra-gene rearrangements: IGH-MYC; IGH-BCL2
IGH-BCL6
Lipson et al, Presented at American Society of Hematology Annual Meeting, December 2013.
He, et al, in press, Blood, 2016

Mutations detectable by first-generation vs NGS
Y253H
M343V
T315I
L248Q
M351V
Lower detection limit of Sanger Sequencing

Personalized Cancer Medicine: Some
conceptual thoughts
1. A brief history of precision medicine
2. What really is a driver mutation?
3. How can be best identify driver mutations?
4. Some case histories
5. Concluding thoughts

• 57 year old patient with triple negative inflammatory breast cancer
• ER/PR/HER2 negative
• Extensive prior chemotherapy with multiple regimens
• Widespread metastatic disease with extensive skin involvement
• Patient was started on HER-2 targeted therapies with chemotherapy:
• Lapatinib/Oral capecitabine 4/12-5/12->SD (difficulty swallowing)
• Lapatinib/Trastuzumab-Albumin bound paclitaxel 5/12-6/12 *
• Lapatinib/Trastuzumab-Vinorelbine 6/12-7/12- PR; she continues treatment off steroids
ERBB2 Mutated Inflammatory Breast Cancer
Cristofanilli M et al., SABCS, 2012/Ali SM et al., J
Clin Oncol. In press May 2012

Inflammatory Breast Cancer (ILC) With ERBB2 Mutation Response to anti-HER Targeted Therapy
5/15/12
8/14/12
Images provided by Dr. M Cristofanilli, Jefferson U, Philadelphia, PA

Response to Anti-HER2 Targeted Therapy
Pre-therapy: extensive active disease
Post-therapy: good response with lower/less activity
Cristofanilli M et al., SABCS, 2012/Ali SM et al., J Clin Oncol. In press May 2012

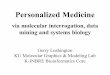
Cervix Squamous Cell Carcinoma with FBXW7 Mutation Responds to Everolimus
Before targeted therapy On Everolimus x 2 mo

Recurrent/Metastatic Uterine Carcinoma Found to Have an ALK Fusion and Responds to Crizotinib
A
Baseline
B
Follow-up

Personalized Cancer Medicine: Some
conceptual thoughts
1. A brief history of precision medicine
2. What really is a driver mutation?
3. How can be best identify driver mutations?
4. Some case histories
5. Concluding thoughts

Complexity of Cancer Genome
• Cancer evolves & adapts (in a Darwinian fashion) to both host defenses and to therapy - driven by clonal heterogeneity
• Clonal evolution contributes to resistance to therapy; treatment may hasten the evolutionary process
• Functionality: Lineage specificity of genomic abn: BRAF V600E no response to vemurafenib in colorectal cancer; HER2 amplification no benefit to trastuzumab in endometrial cancer
• Different areas of the genome may have different rates of mutation acquistion and indeed the order
Hyman et al, NEJM 2015

Concluding thoughts
• Hybrid-capture NGS technology is enabling us
to deliver evidence-based precision cancer medicine
• In the near future, comprehensive genomic profiling will incorporate predictive biomarkers for immunotherapy enabling even greater clinical application

Acknowledgements
Recommended