REDESIGNING HEALTHCARE PAYMENT AND DELIVERY FOR
HIGHER QUALITY, LOWER COSTCARE OF PATIENTS WITH DIABETES
Harold D. MillerPresident and CEO
Center for Healthcare Quality and Payment Reform
www.CHQPR.org
2© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
The Problem of Diabetes
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Bad Outcomes &High Spending
3© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
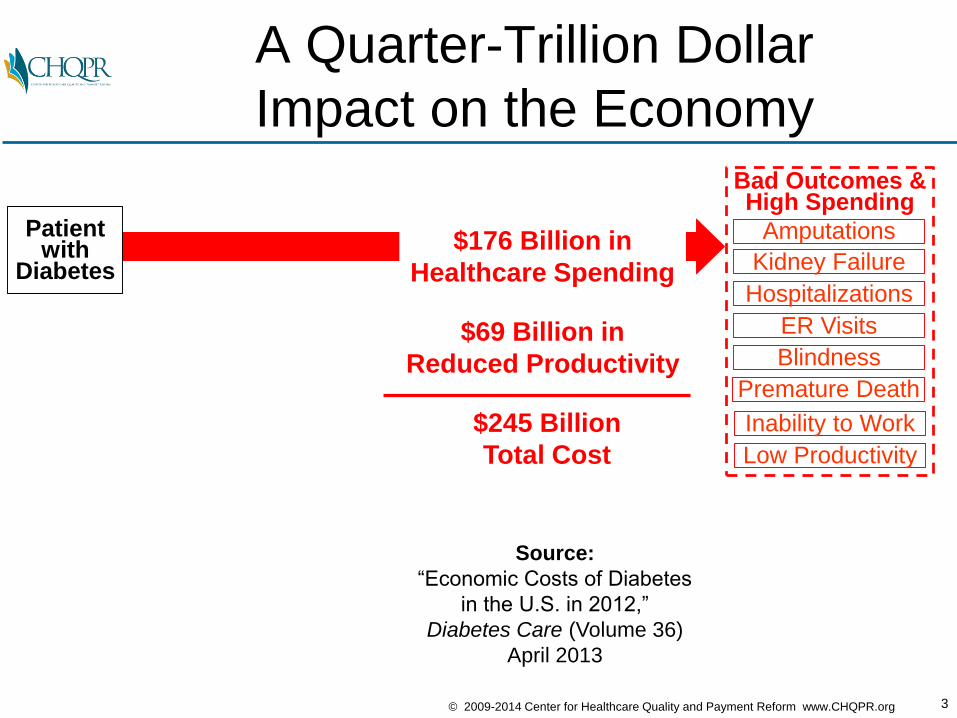
A Quarter-Trillion Dollar
Impact on the Economy
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Bad Outcomes &High Spending
$176 Billion in
Healthcare Spending
$69 Billion in
Reduced Productivity
$245 Billion
Total Cost
Source:
“Economic Costs of Diabetes
in the U.S. in 2012,”
Diabetes Care (Volume 36)
April 2013
4© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
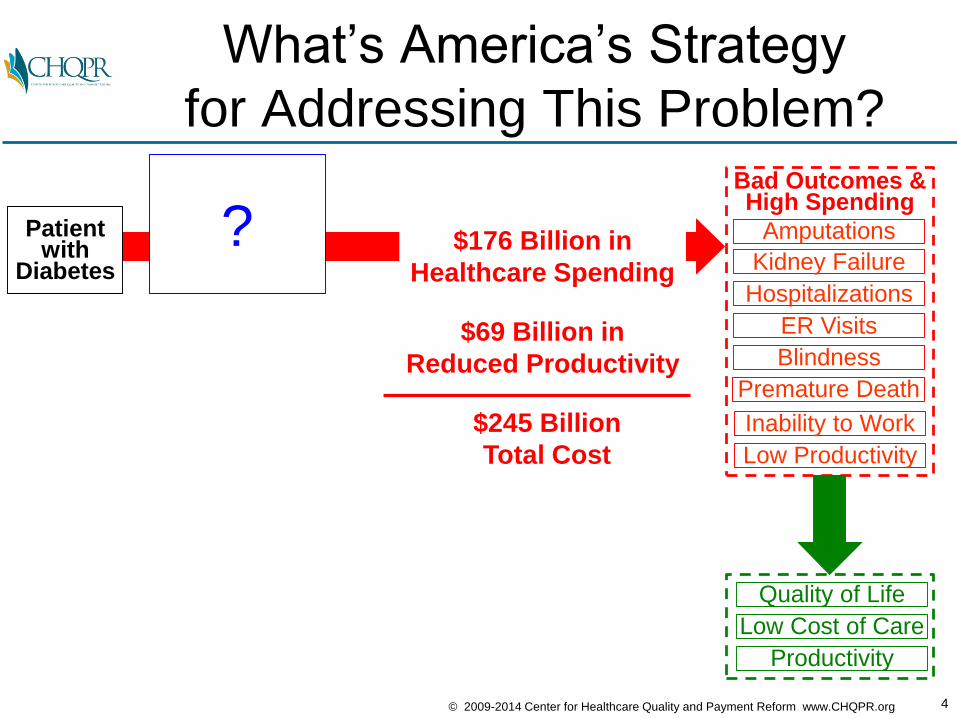
What’s America’s Strategy
for Addressing This Problem?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
Bad Outcomes &High Spending
$176 Billion in
Healthcare Spending
$69 Billion in
Reduced Productivity
$245 Billion
Total Cost
?
5© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
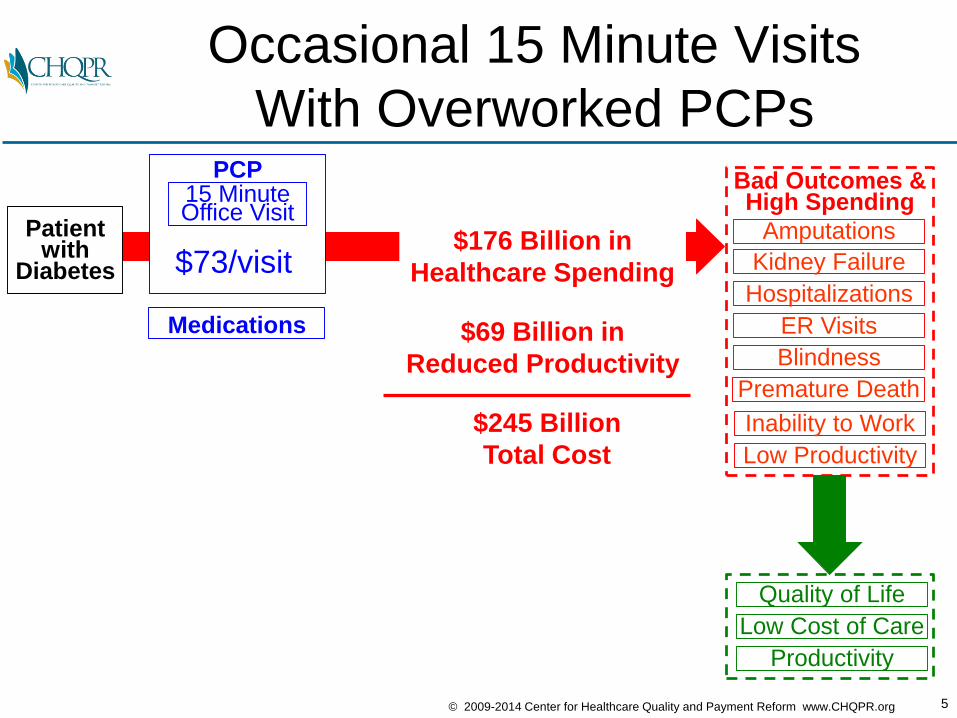
Occasional 15 Minute Visits
With Overworked PCPs
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
Bad Outcomes &High Spending
$176 Billion in
Healthcare Spending
$69 Billion in
Reduced Productivity
$245 Billion
Total Cost
PCP15 MinuteOffice Visit
$73/visit
Medications
6© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
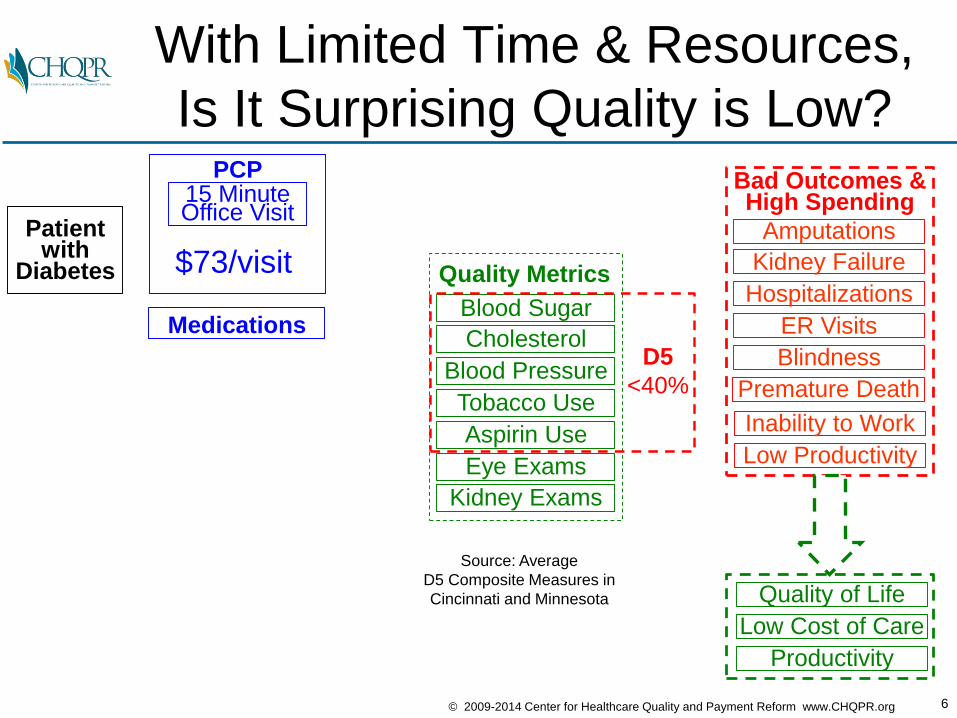
With Limited Time & Resources,
Is It Surprising Quality is Low?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
Bad Outcomes &High Spending
PCP15 MinuteOffice Visit
$73/visit
MedicationsBlood Sugar
Cholesterol
Blood Pressure
Tobacco Use
Aspirin Use
Eye Exams
Kidney Exams
Quality Metrics
D5
<40%
Source: Average
D5 Composite Measures in
Cincinnati and Minnesota
7© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
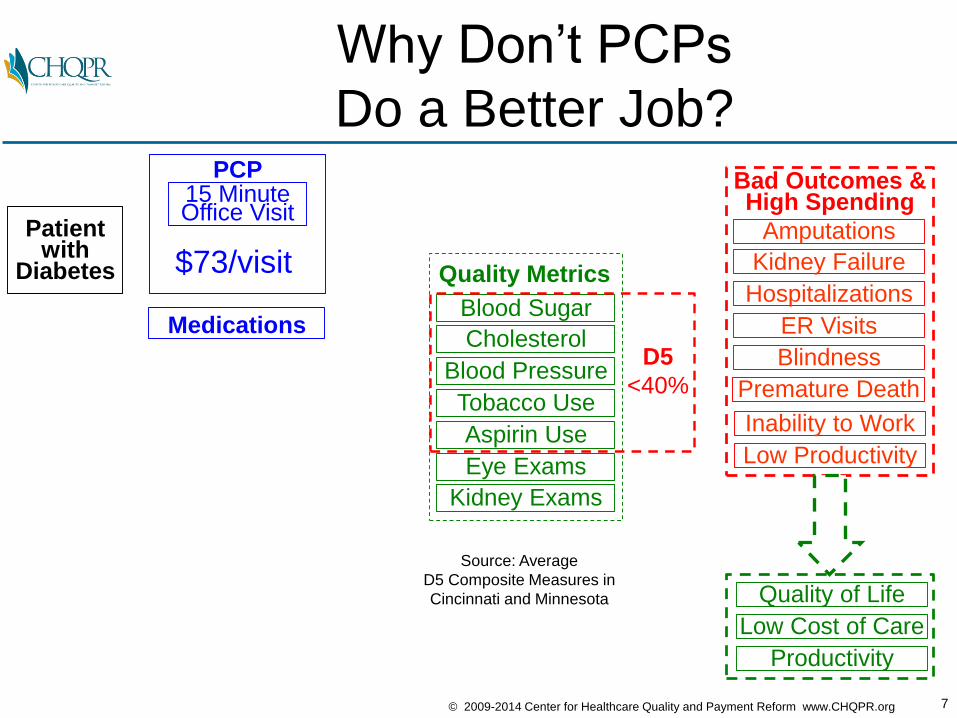
Why Don’t PCPs
Do a Better Job?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
Bad Outcomes &High Spending
PCP15 MinuteOffice Visit
$73/visit
MedicationsBlood Sugar
Cholesterol
Blood Pressure
Tobacco Use
Aspirin Use
Eye Exams
Kidney Exams
Quality Metrics
D5
<40%
Source: Average
D5 Composite Measures in
Cincinnati and Minnesota
8© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
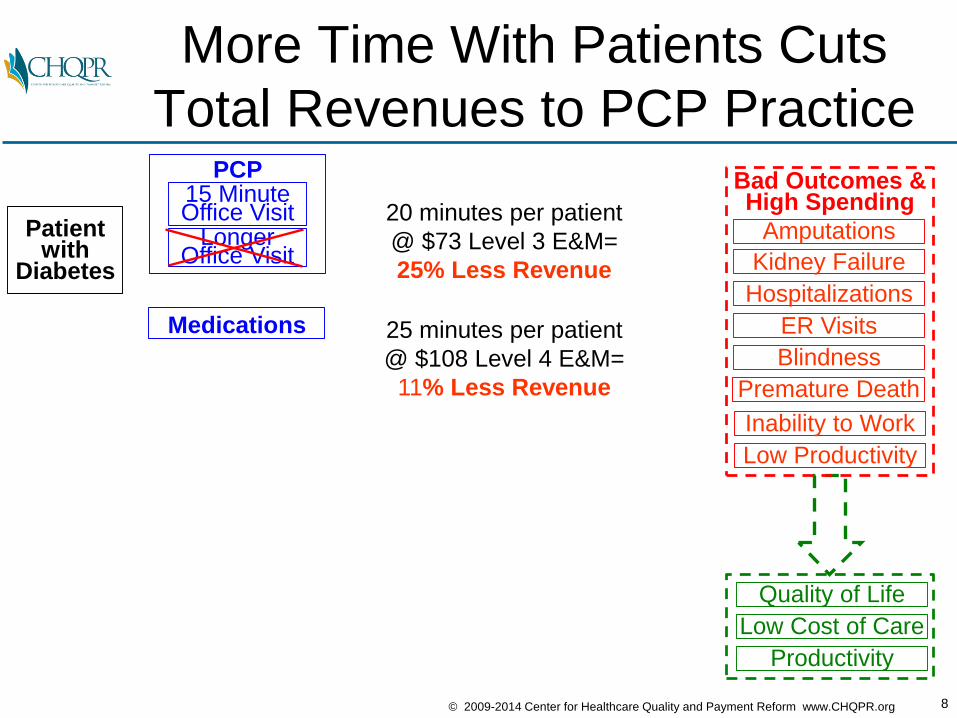
More Time With Patients Cuts
Total Revenues to PCP Practice
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Medications
20 minutes per patient
@ $73 Level 3 E&M=
25% Less Revenue
25 minutes per patient
@ $108 Level 4 E&M=
11% Less Revenue
Bad Outcomes &High Spending
9© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
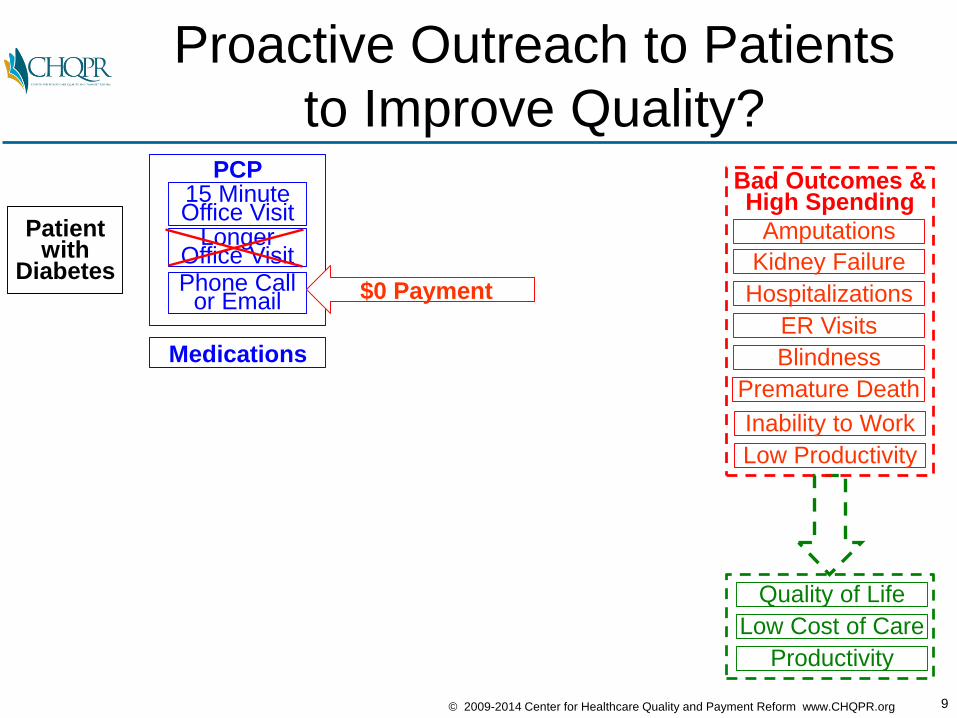
Proactive Outreach to Patients
to Improve Quality?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice VisitPhone Call
or Email
Medications
$0 Payment
Bad Outcomes &High Spending
10© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
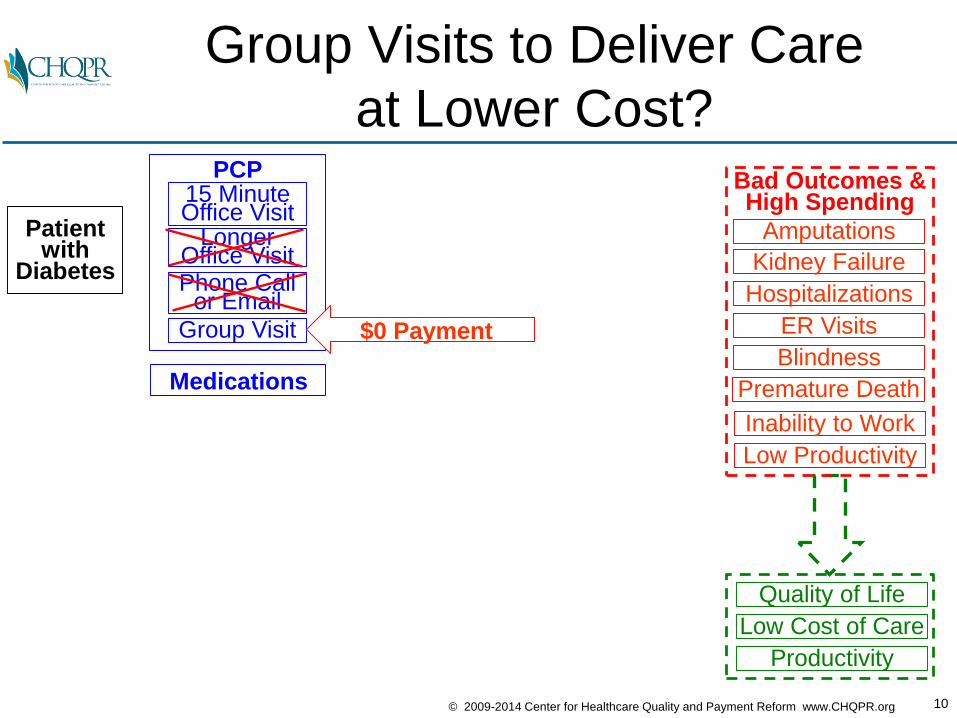
Group Visits to Deliver Care
at Lower Cost?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice VisitPhone Call
or Email
Group Visit
Medications
$0 Payment
Bad Outcomes &High Spending
11© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
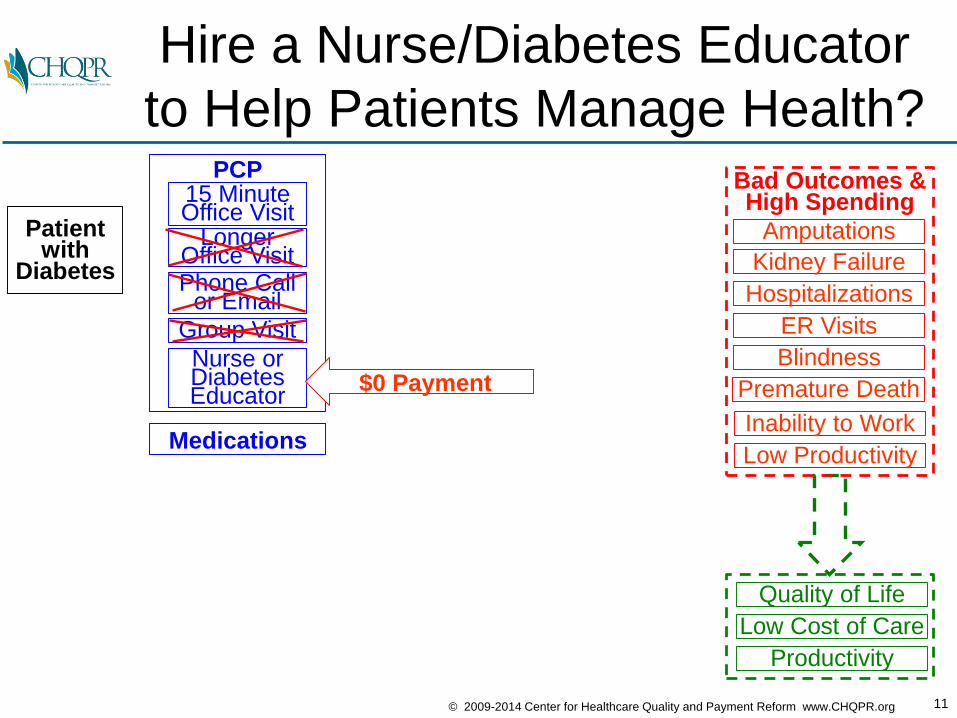
Hire a Nurse/Diabetes Educator
to Help Patients Manage Health?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Medications
$0 Payment
Bad Outcomes &High Spending
12© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
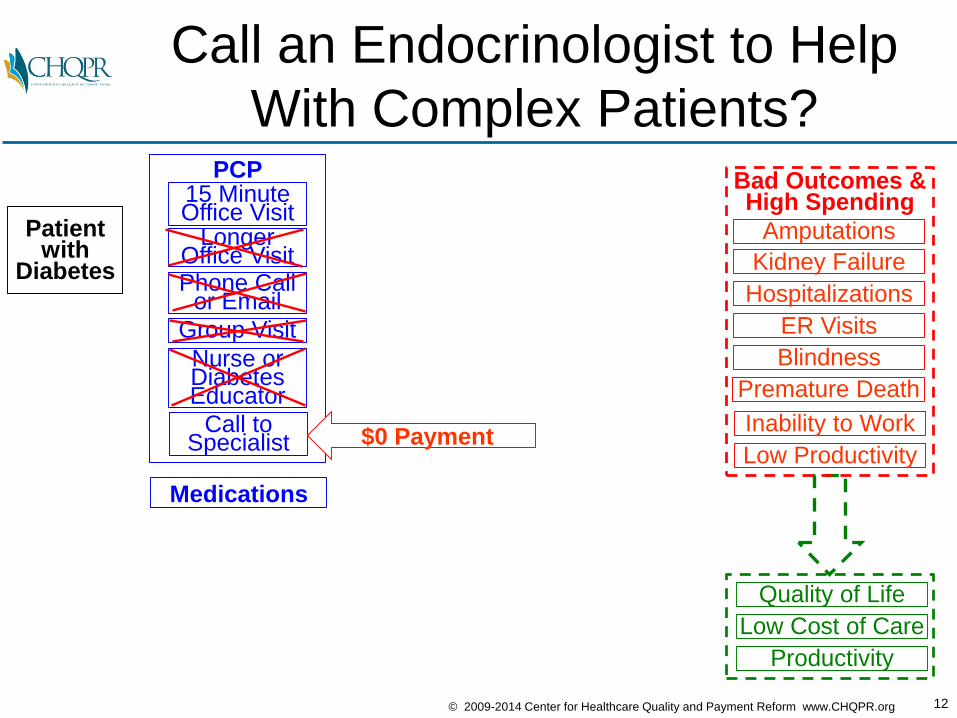
Call an Endocrinologist to Help
With Complex Patients?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Medications
$0 Payment
Bad Outcomes &High Spending
13© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
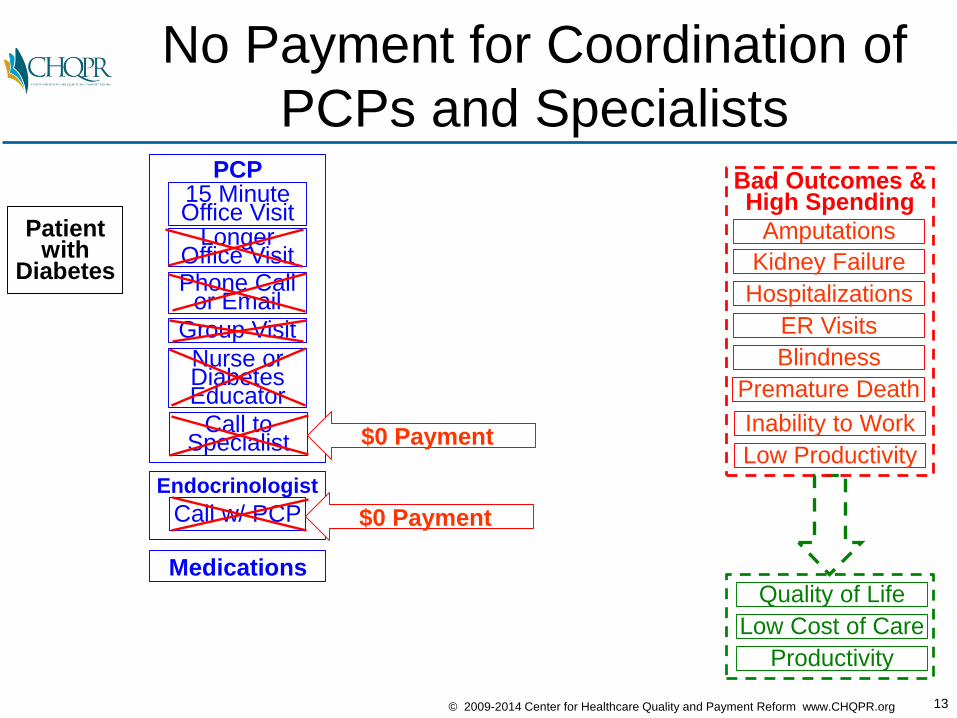
No Payment for Coordination of
PCPs and Specialists
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Endocrinologist
Call w/ PCP
Medications
$0 Payment
$0 Payment
Bad Outcomes &High Spending
14© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
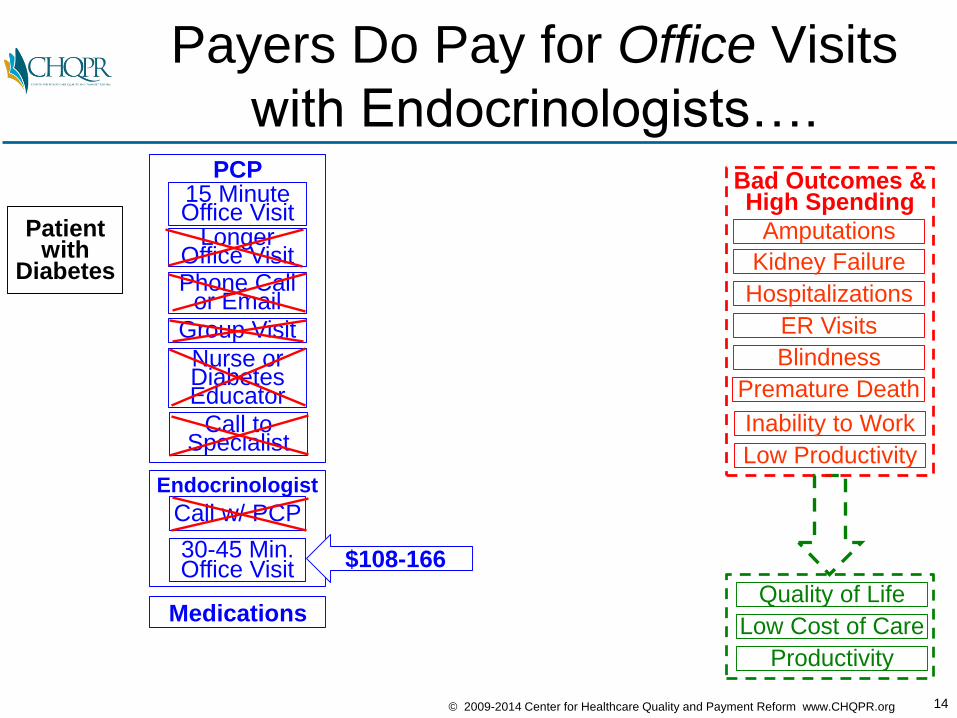
Payers Do Pay for Office Visits
with Endocrinologists….
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit $108-166
Bad Outcomes &High Spending
Medications
15© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
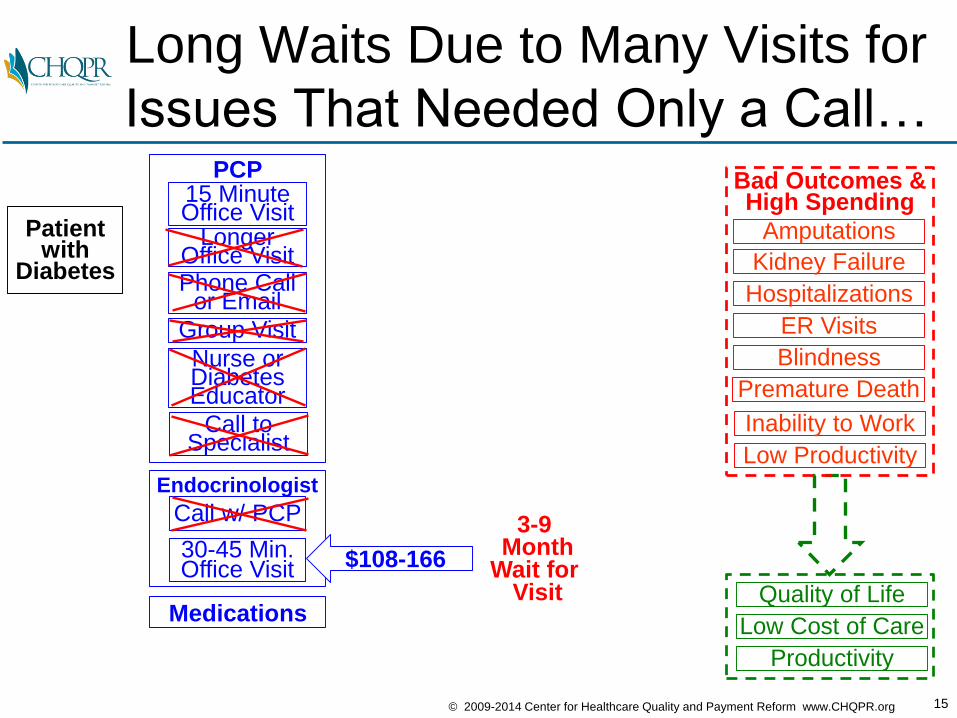
Long Waits Due to Many Visits for
Issues That Needed Only a Call…
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Bad Outcomes &High Spending
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit $108-166
Medications
3-9 Month
Wait for Visit
16© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
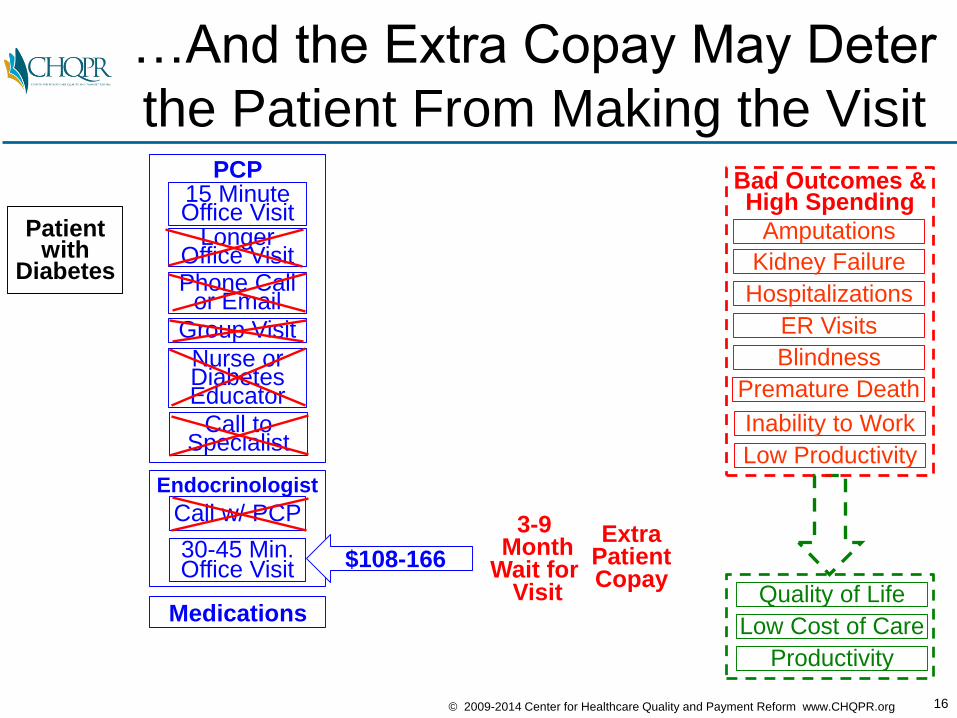
…And the Extra Copay May Deter
the Patient From Making the Visit
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
3-9 Month
Wait for Visit
ExtraPatientCopay
Bad Outcomes &High Spending
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit $108-166
Medications
17© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
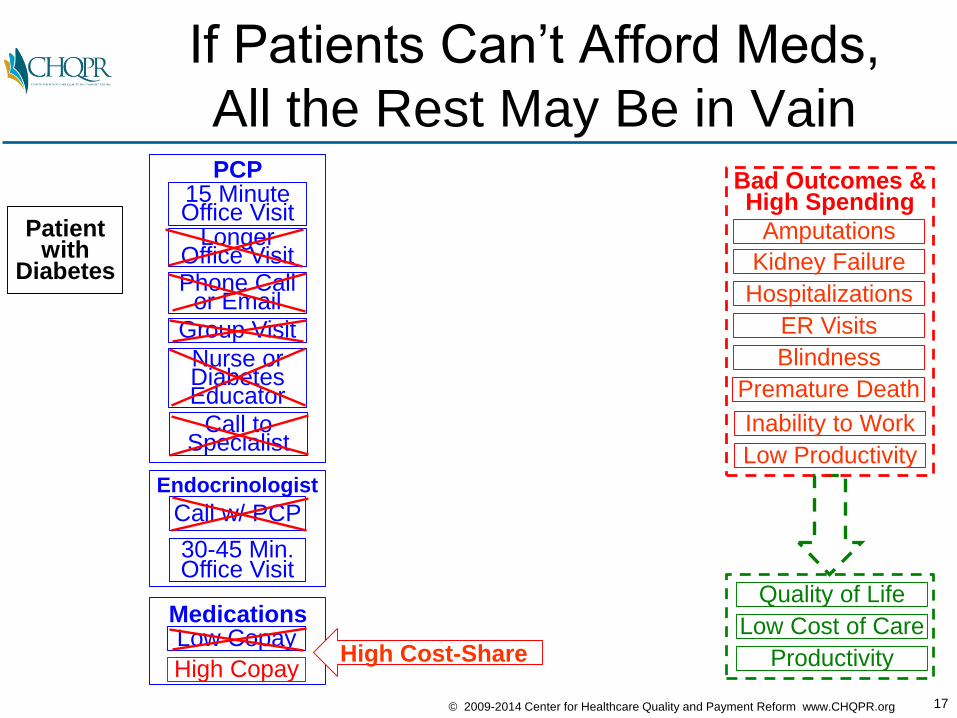
If Patients Can’t Afford Meds,
All the Rest May Be in Vain
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
MedicationsLow Copay
High CopayHigh Cost-Share
Bad Outcomes &High Spending
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
18© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
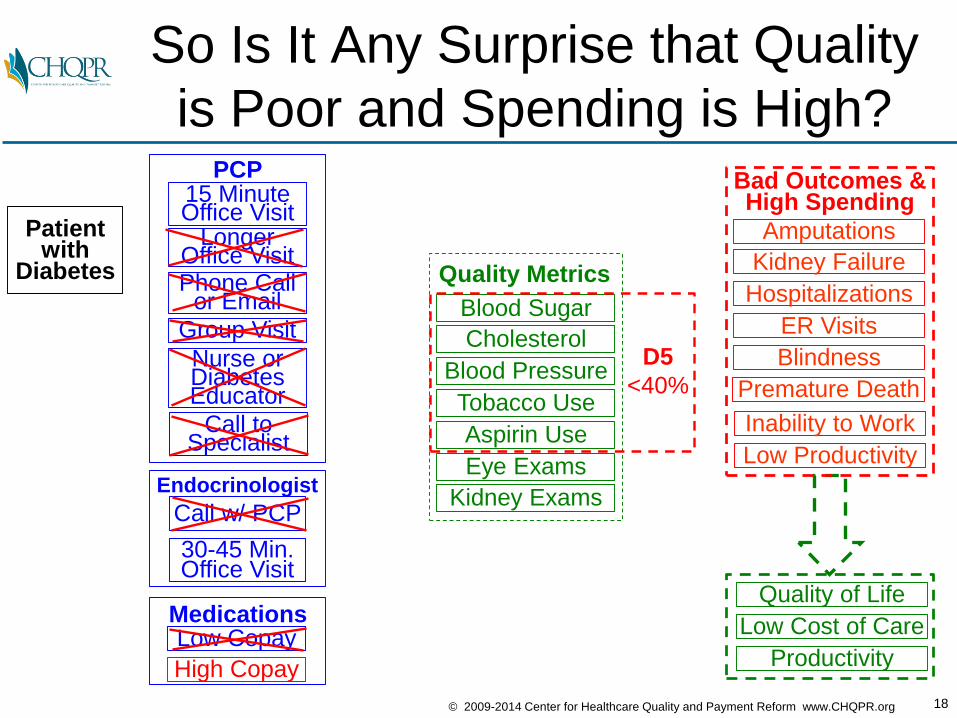
So Is It Any Surprise that Quality
is Poor and Spending is High?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Blood Sugar
Cholesterol
Blood Pressure
Tobacco Use
Aspirin Use
Eye Exams
Kidney Exams
Quality Metrics
D5
<40%
Bad Outcomes &High Spending
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
19© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
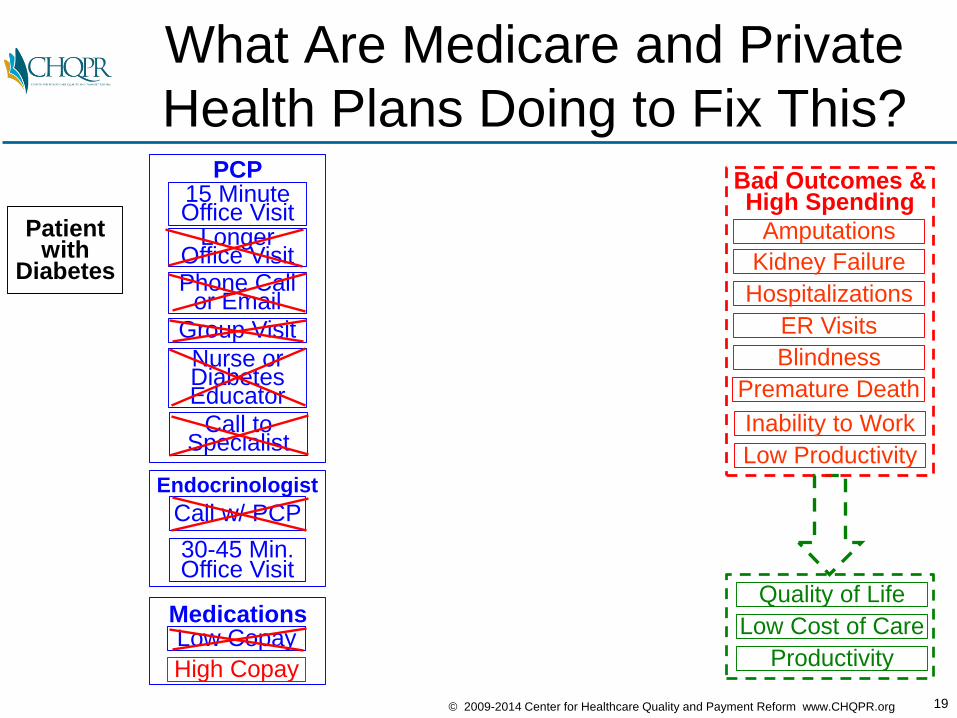
What Are Medicare and Private
Health Plans Doing to Fix This?
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Bad Outcomes &High Spending
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
20© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
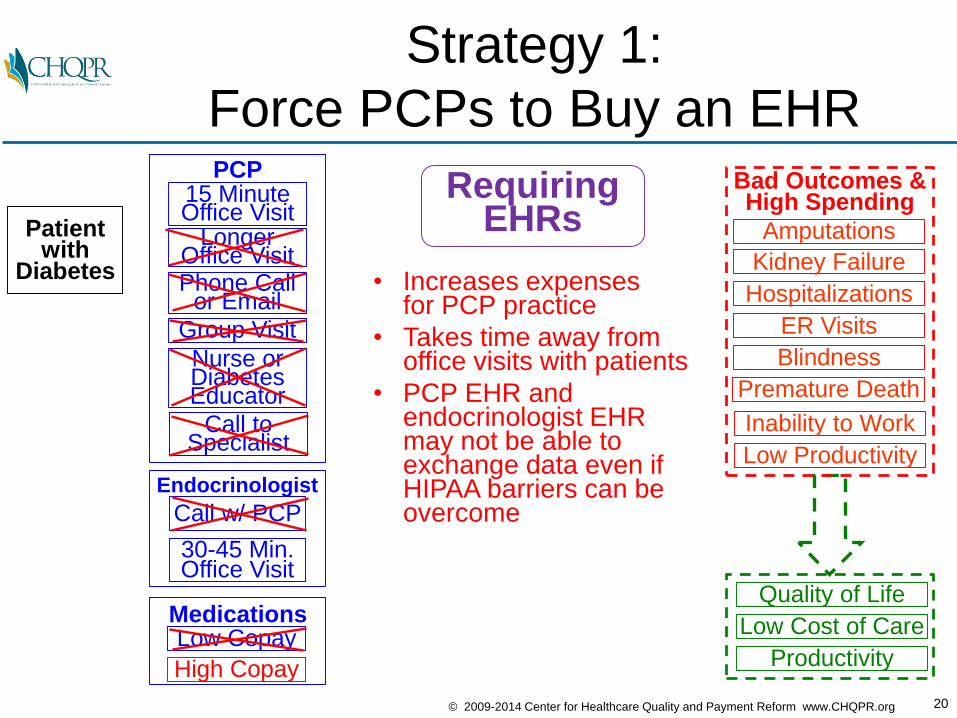
Strategy 1:
Force PCPs to Buy an EHR
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
RequiringEHRs
• Increases expensesfor PCP practice
• Takes time away fromoffice visits with patients
• PCP EHR and endocrinologist EHR may not be able to exchange data even ifHIPAA barriers can beovercome
Bad Outcomes &High Spending
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
21© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
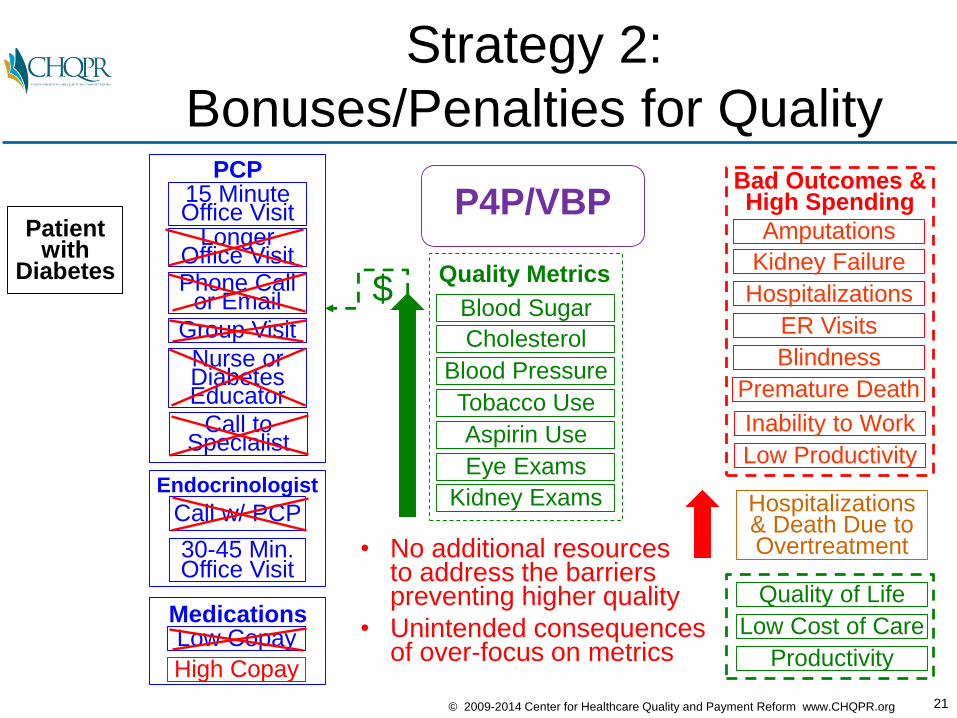
Strategy 2:
Bonuses/Penalties for Quality
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
P4P/VBP
Blood Sugar
Cholesterol
Blood Pressure
Tobacco Use
Aspirin Use
Eye Exams
Kidney Exams
Quality Metrics
• No additional resourcesto address the barrierspreventing higher quality
• Unintended consequencesof over-focus on metrics
Hospitalizations& Death Due to Overtreatment
Bad Outcomes &High Spending
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
$
22© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
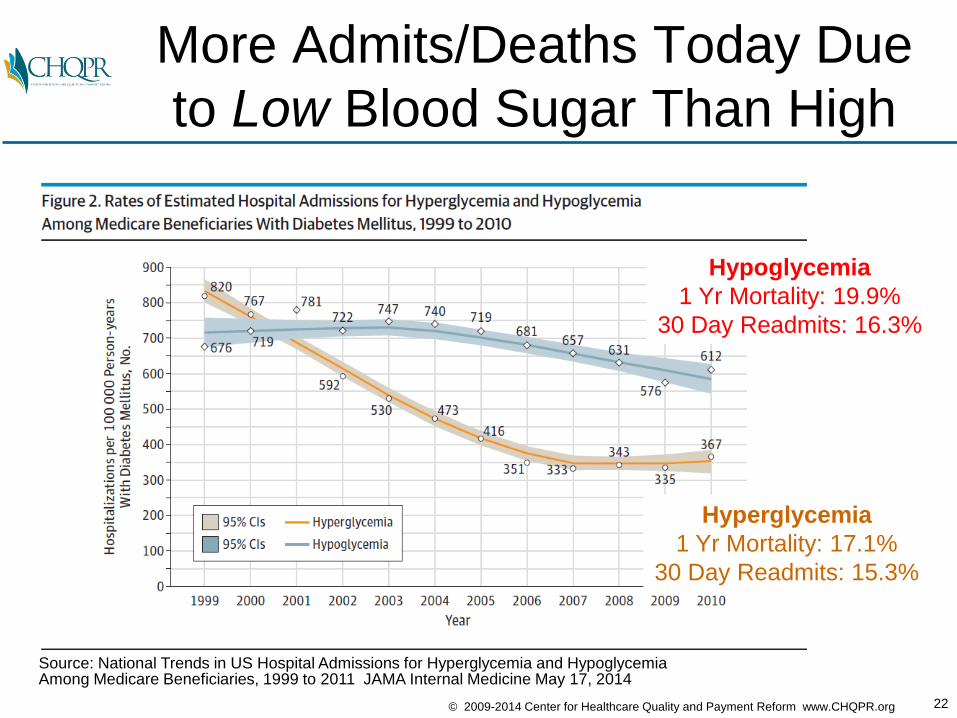
More Admits/Deaths Today Due
to Low Blood Sugar Than High
Hypoglycemia
1 Yr Mortality: 19.9%
30 Day Readmits: 16.3%
Hyperglycemia
1 Yr Mortality: 17.1%
30 Day Readmits: 15.3%
Source: National Trends in US Hospital Admissions for Hyperglycemia and HypoglycemiaAmong Medicare Beneficiaries, 1999 to 2011 JAMA Internal Medicine May 17, 2014
23© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
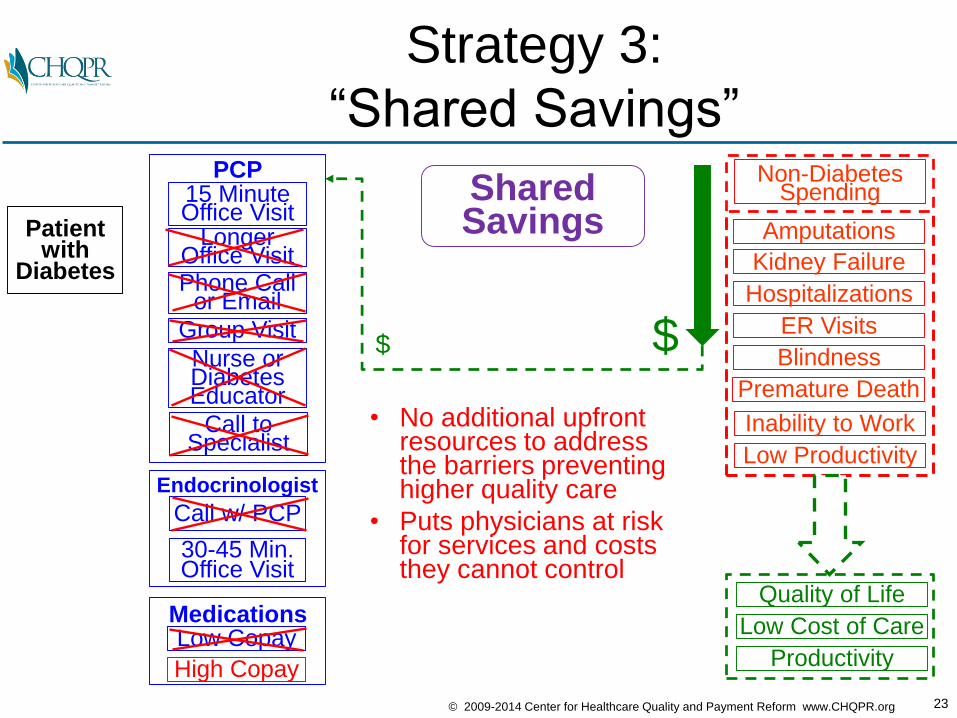
Strategy 3:
“Shared Savings”
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Non-DiabetesSpendingShared
Savings
• No additional upfrontresources to address the barriers preventing higher quality care
• Puts physicians at riskfor services and costs they cannot control
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
$ $
24© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
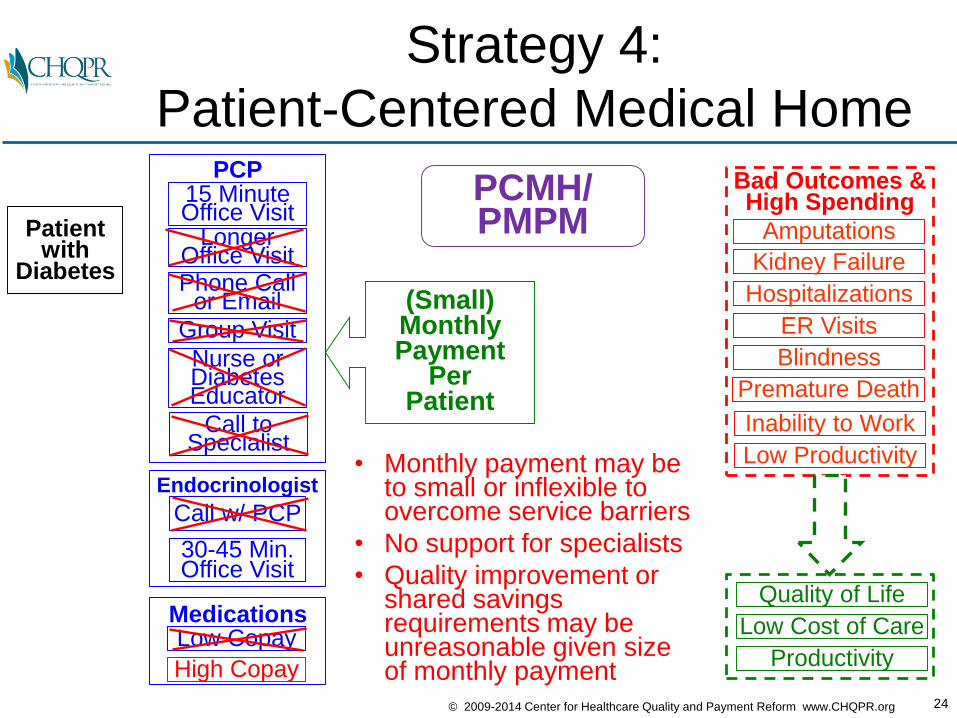
Strategy 4:
Patient-Centered Medical Home
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
PCMH/PMPM
• Monthly payment may beto small or inflexible toovercome service barriers
• No support for specialists
• Quality improvement orshared savings requirements may beunreasonable given sizeof monthly payment
Bad Outcomes &High Spending
(Small)MonthlyPayment
PerPatient
MedicationsLow Copay
High Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
25© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
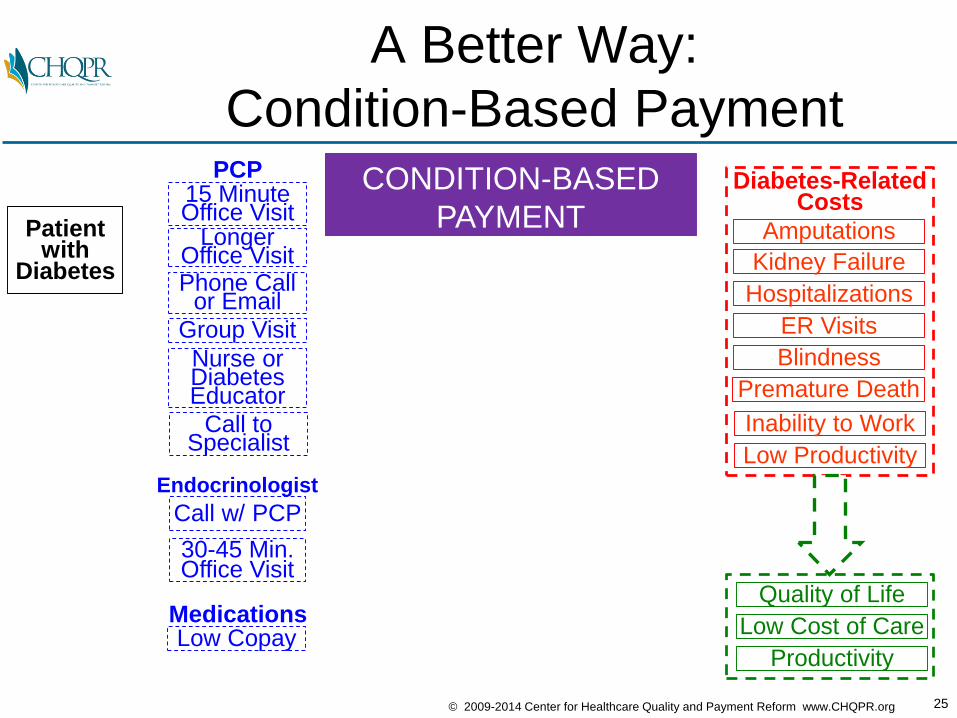
A Better Way:
Condition-Based Payment
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Diabetes-RelatedCosts
MedicationsLow Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
Quality of Life
Low Cost of Care
Productivity
CONDITION-BASED
PAYMENT
26© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
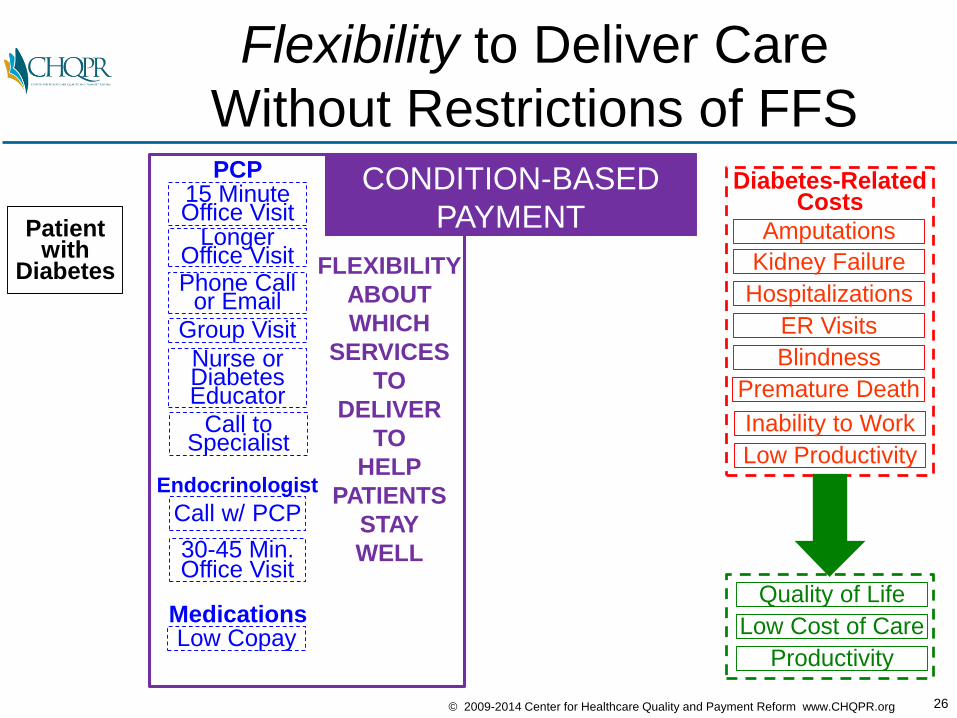
Flexibility to Deliver Care
Without Restrictions of FFS
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Diabetes-RelatedCosts
MedicationsLow Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
Quality of Life
Low Cost of Care
Productivity
FLEXIBILITY
ABOUT
WHICH
SERVICES
TO
DELIVER
TO
HELP
PATIENTS
STAY
WELL
CONDITION-BASED
PAYMENT
27© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
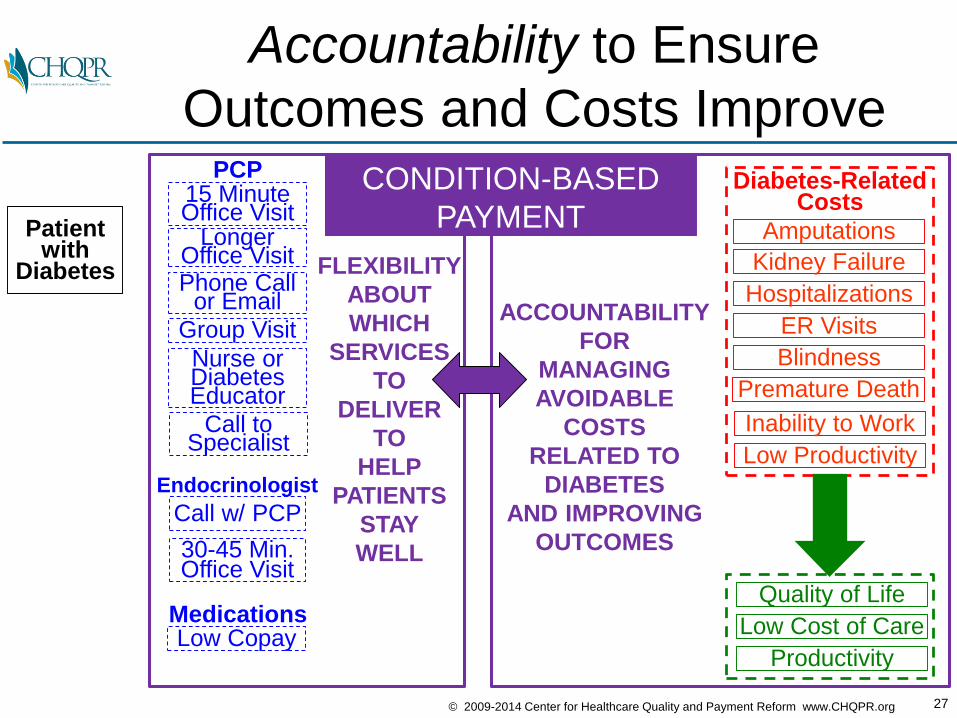
Accountability to Ensure
Outcomes and Costs Improve
Patient with
Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
15 MinuteOffice Visit
PCP
LongerOffice Visit
Nurse orDiabetesEducator
Phone Callor Email
Group Visit
Call toSpecialist
Diabetes-RelatedCosts
MedicationsLow Copay
Endocrinologist
Call w/ PCP
30-45 Min.Office Visit
Quality of Life
Low Cost of Care
Productivity
FLEXIBILITY
ABOUT
WHICH
SERVICES
TO
DELIVER
TO
HELP
PATIENTS
STAY
WELL
ACCOUNTABILITY
FOR
MANAGING
AVOIDABLE
COSTS
RELATED TO
DIABETES
AND IMPROVING
OUTCOMES
CONDITION-BASED
PAYMENT
28© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
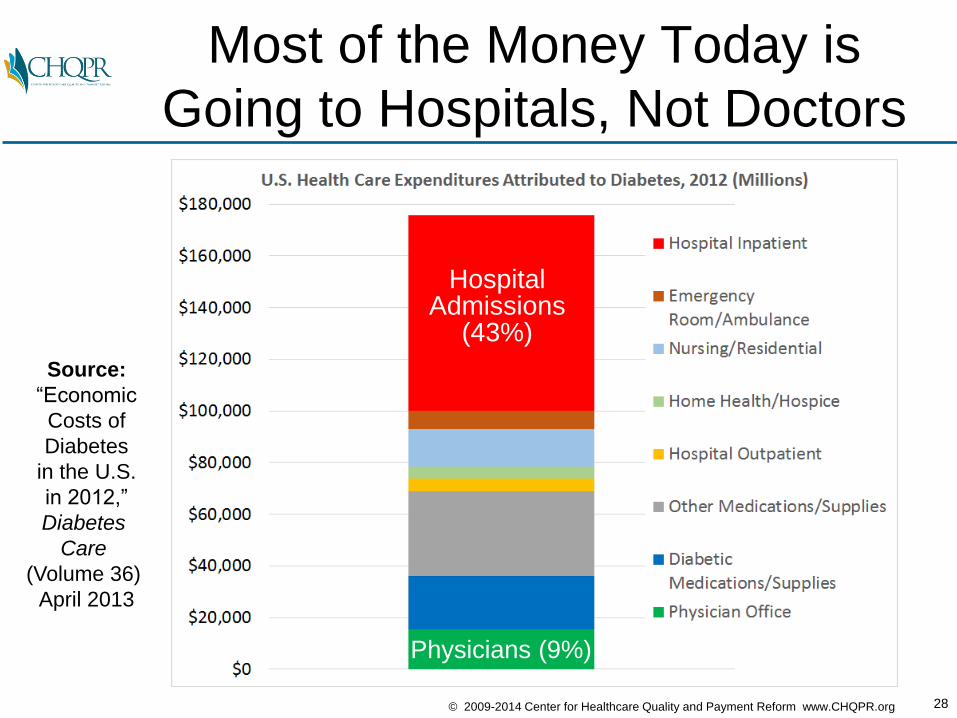
Most of the Money Today is
Going to Hospitals, Not Doctors
Source:
“Economic
Costs of
Diabetes
in the U.S.
in 2012,”
Diabetes
Care
(Volume 36)
April 2013
HospitalAdmissions
(43%)
Physicians (9%)
29© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
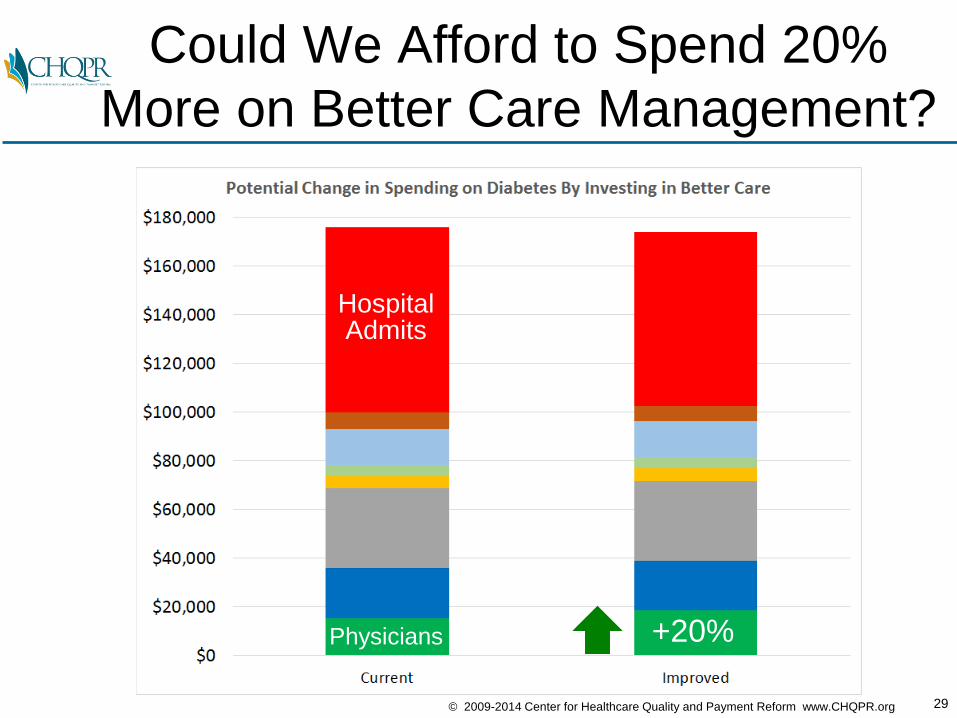
Could We Afford to Spend 20%
More on Better Care Management?
HospitalAdmits
Physicians +20%
30© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
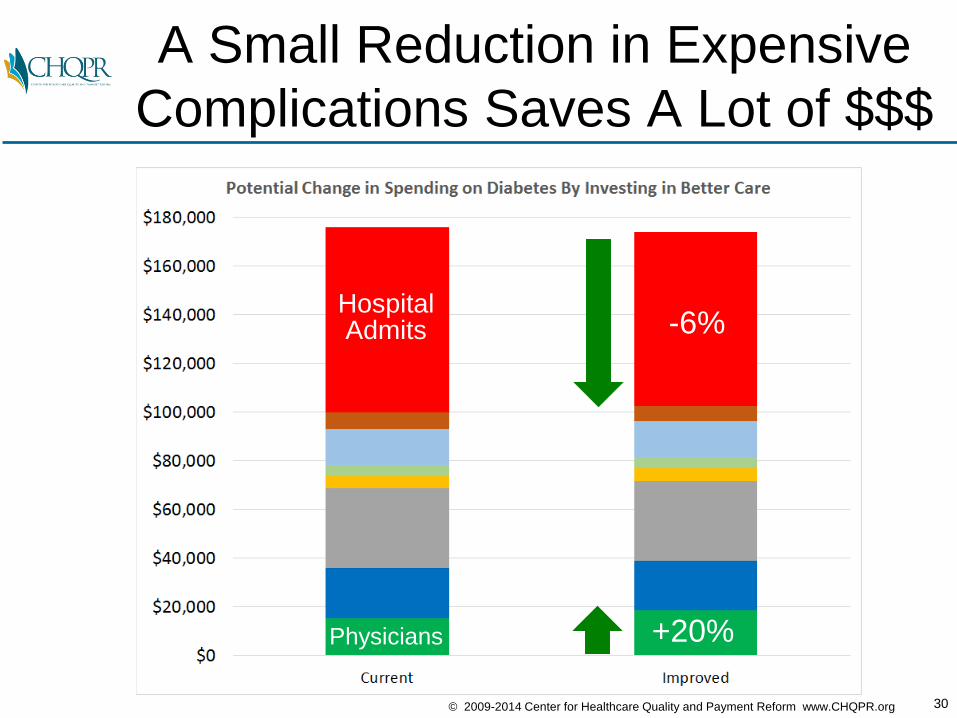
A Small Reduction in Expensive
Complications Saves A Lot of $$$
HospitalAdmits
Physicians +20%
-6%
31© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
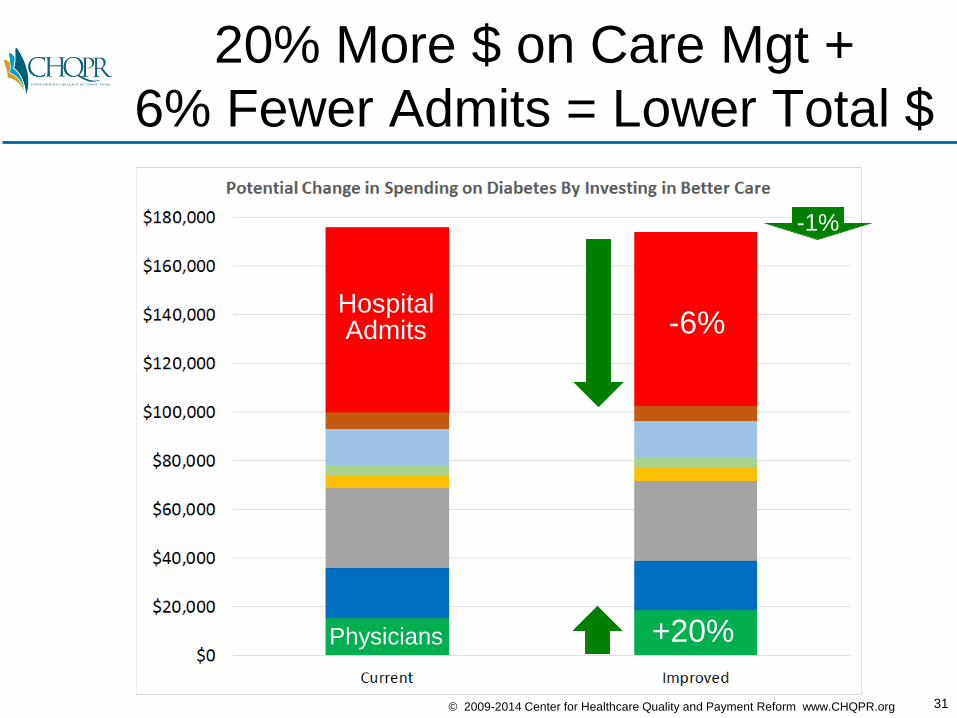
20% More $ on Care Mgt +
6% Fewer Admits = Lower Total $
HospitalAdmits
Physicians +20%
-6%
-1%
32© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
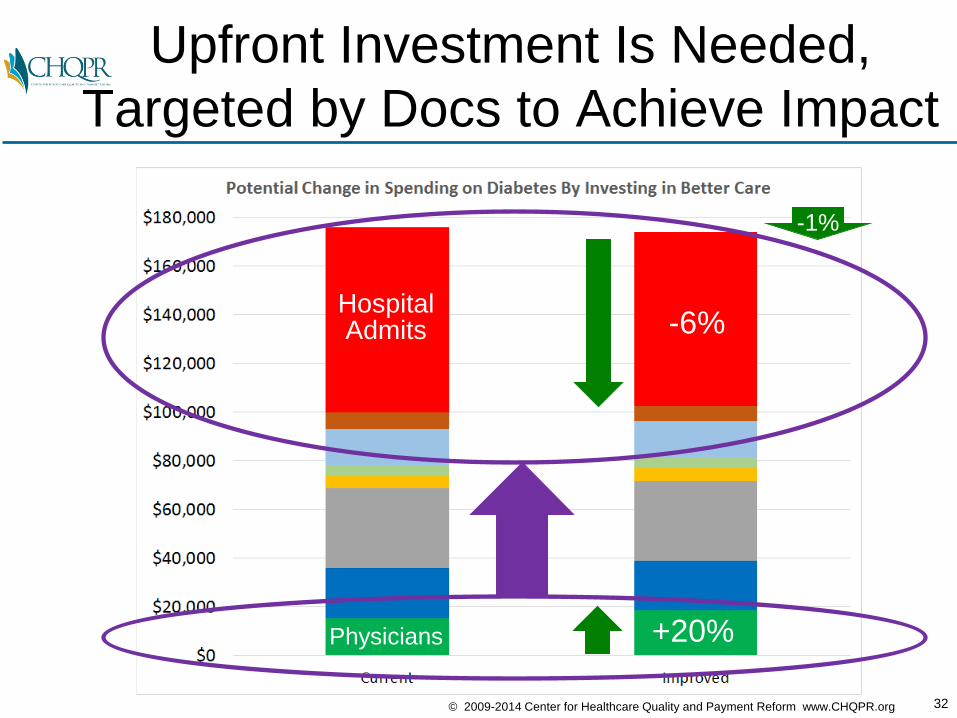
Upfront Investment Is Needed,
Targeted by Docs to Achieve Impact
HospitalAdmits
Physicians +20%
-6%
-1%
33© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
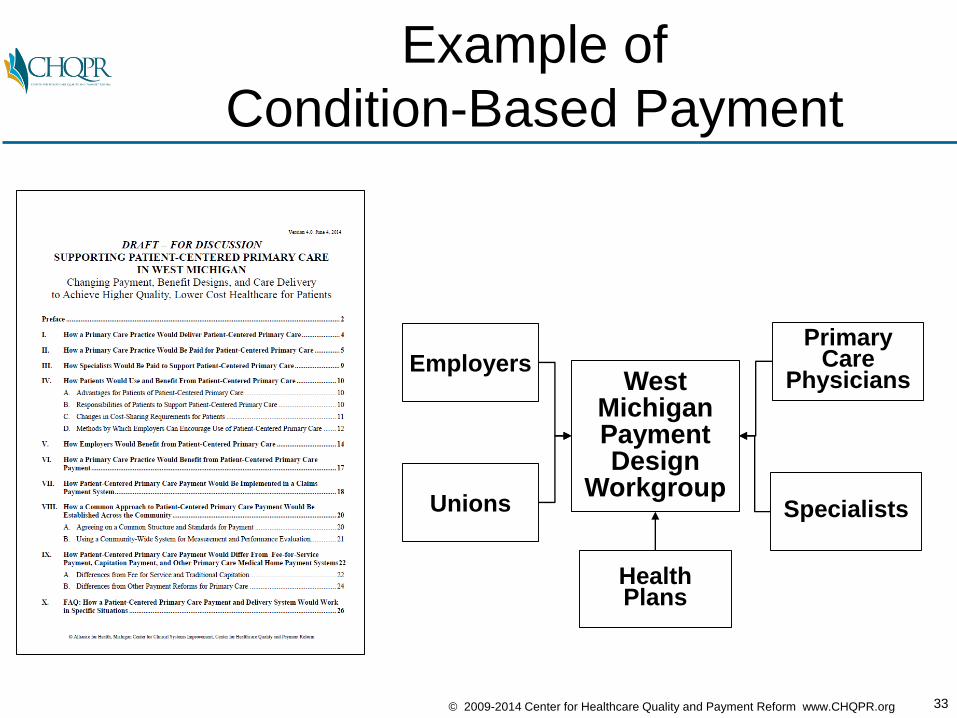
Example of
Condition-Based Payment
EmployersWest
MichiganPaymentDesign
Workgroup
PrimaryCare
Physicians
SpecialistsUnions
HealthPlans
34© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
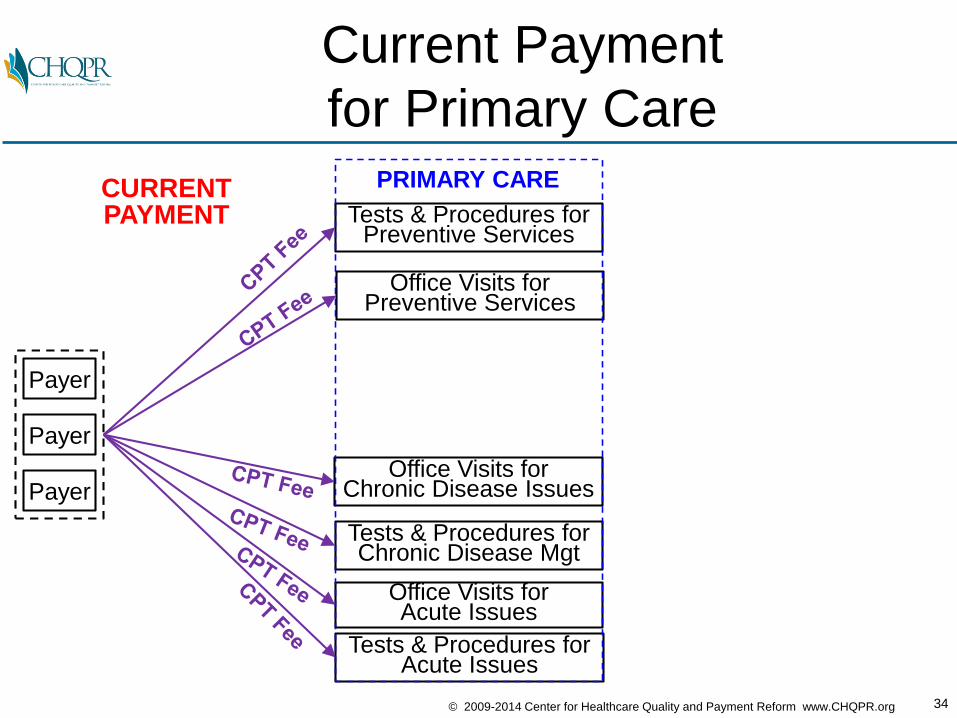
Current Payment
for Primary Care
Payer
Payer
Payer
Office Visits forPreventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
CURRENTPAYMENT
PRIMARY CARE
35© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
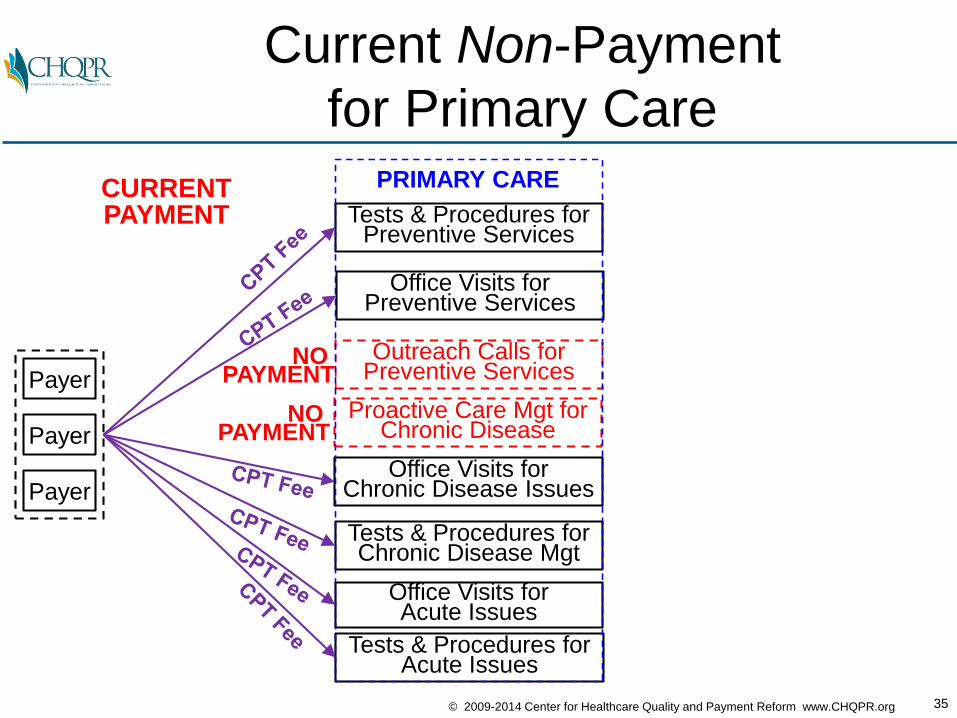
Current Non-Payment
for Primary Care
Payer
Payer
Payer
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Proactive Care Mgt for Chronic Disease
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
CURRENTPAYMENT
NO PAYMENT
NO PAYMENT
PRIMARY CARE
36© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
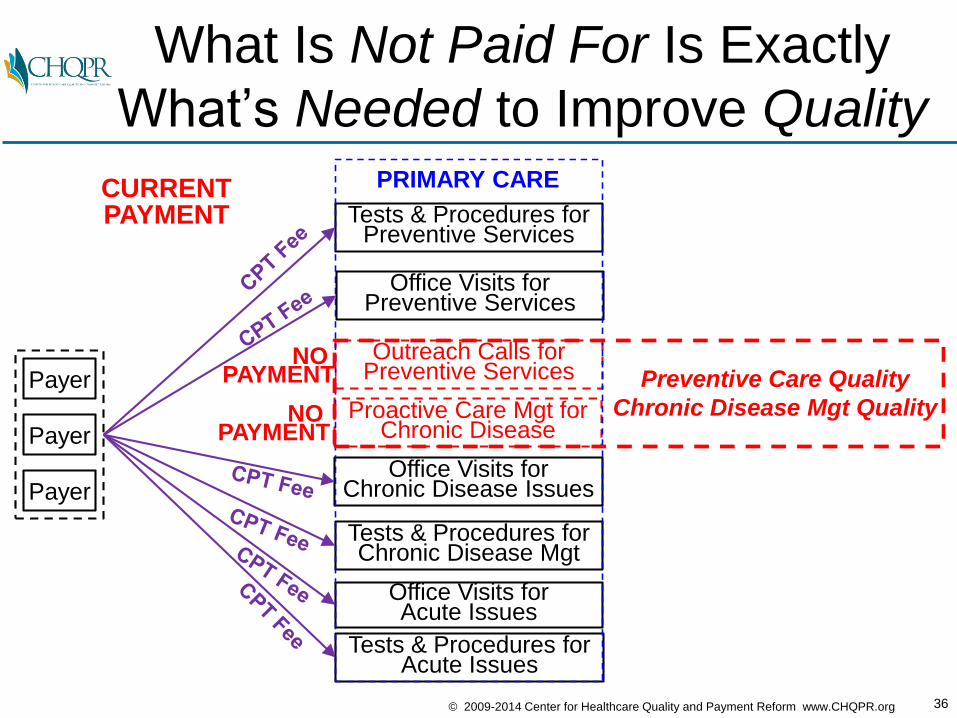
What Is Not Paid For Is Exactly
What’s Needed to Improve Quality
Payer
Payer
Payer
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Proactive Care Mgt for Chronic Disease
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
CURRENTPAYMENT
NO PAYMENT
NO PAYMENT
PRIMARY CARE
Preventive Care Quality
Chronic Disease Mgt Quality
37© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
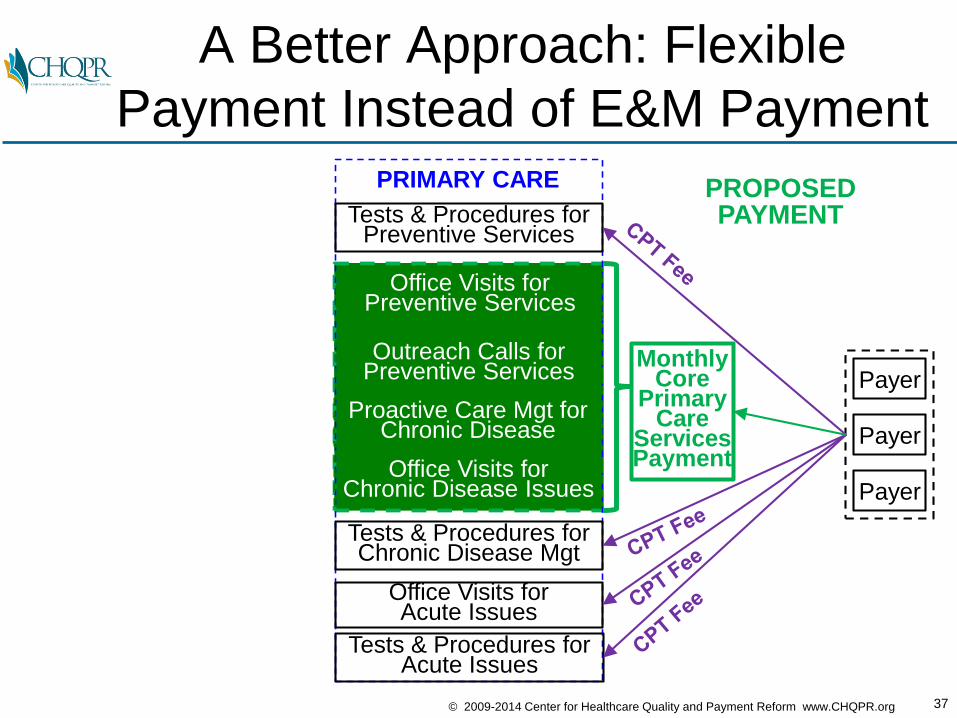
A Better Approach: Flexible
Payment Instead of E&M Payment
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PROPOSEDPAYMENT
Payer
Payer
Payer
MonthlyCore
Primary Care
Services Payment
PRIMARY CARE
Proactive Care Mgt for Chronic Disease
38© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
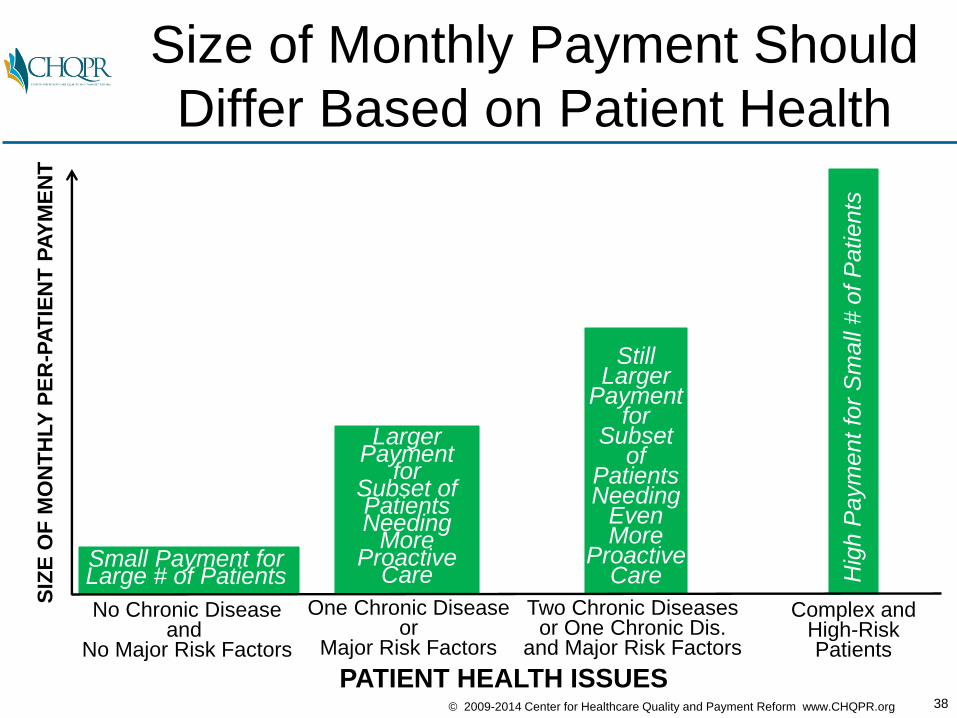
Size of Monthly Payment Should
Differ Based on Patient Health
No Chronic Diseaseand
No Major Risk Factors
PATIENT HEALTH ISSUES
SIZ
E O
F M
ON
TH
LY
PE
R-P
AT
IEN
T P
AY
ME
NT
One Chronic Diseaseor
Major Risk Factors
Two Chronic Diseasesor One Chronic Dis.
and Major Risk Factors
Complex andHigh-RiskPatients
Small Payment forLarge # of Patients H
igh P
aym
ent
for
Sm
all
# o
f P
atients
LargerPayment
forSubset ofPatientsNeeding
MoreProactive
Care
StillLarger
Payment for
Subset of
PatientsNeeding
EvenMore
ProactiveCare
39© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
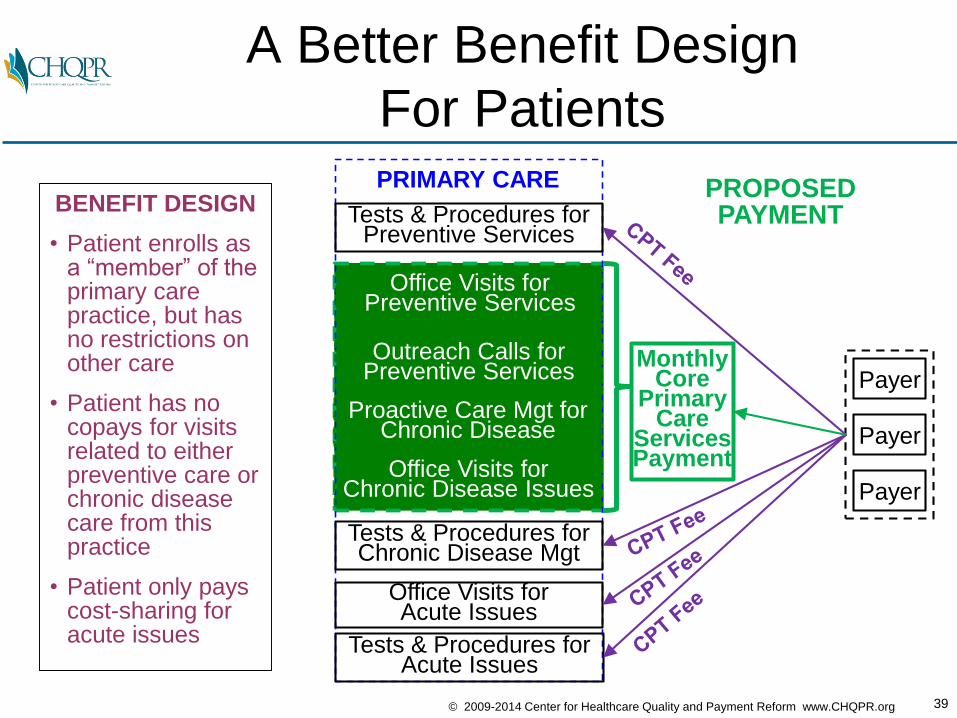
A Better Benefit Design
For Patients
BENEFIT DESIGN
• Patient enrolls as a “member” of the primary care practice, but has no restrictions on other care
• Patient has no copays for visits related to either preventive care or chronic disease care from this practice
• Patient only pays cost-sharing for acute issues
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PROPOSEDPAYMENT
Payer
Payer
Payer
MonthlyCore
Primary Care
Services Payment
PRIMARY CARE
Proactive Care Mgt for Chronic Disease
40© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
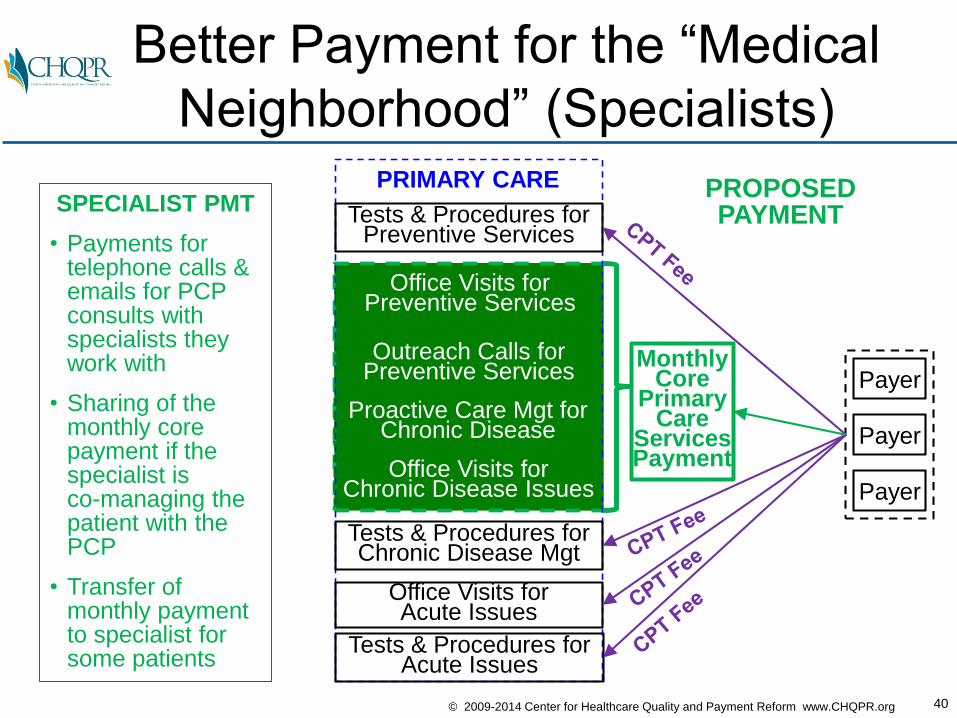
Better Payment for the “Medical
Neighborhood” (Specialists)
SPECIALIST PMT
• Payments for telephone calls & emails for PCP consults with specialists they work with
• Sharing of the monthly core payment if the specialist is co-managing the patient with thePCP
• Transfer of monthly payment to specialist for some patients
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PROPOSEDPAYMENT
Payer
Payer
Payer
MonthlyCore
Primary Care
Services Payment
PRIMARY CARE
Proactive Care Mgt for Chronic Disease
41© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
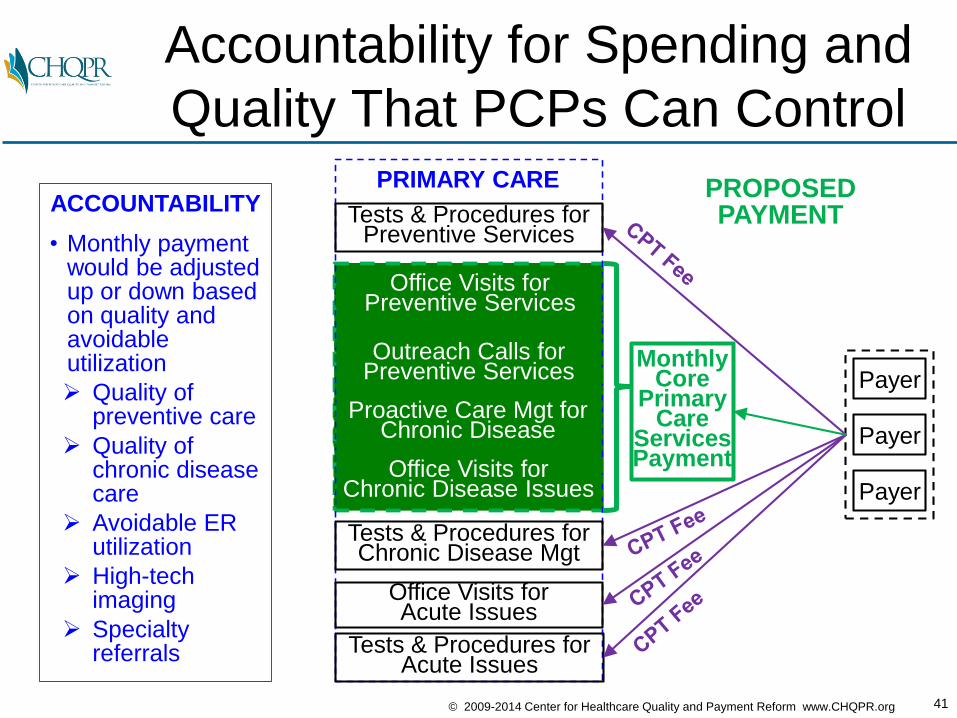
Accountability for Spending and
Quality That PCPs Can Control
ACCOUNTABILITY
• Monthly payment would be adjusted up or down based on quality and avoidable utilization
Quality of preventive care
Quality of chronic disease care
Avoidable ER utilization
High-tech imaging
Specialty referrals
Office Visits forPreventive Services
Outreach Calls for Preventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PROPOSEDPAYMENT
Payer
Payer
Payer
MonthlyCore
Primary Care
Services Payment
PRIMARY CARE
Proactive Care Mgt for Chronic Disease
42© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
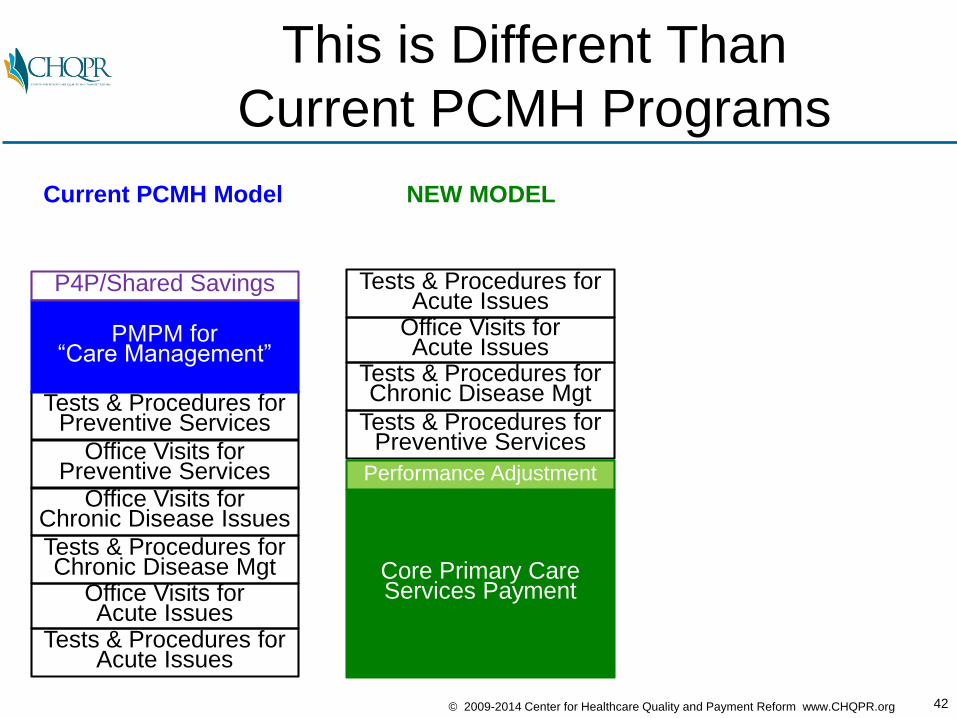
This is Different Than
Current PCMH Programs
Office Visits forPreventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PMPM for“Care Management”
Current PCMH Model
P4P/Shared Savings
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
Core Primary CareServices Payment
Performance Adjustment
NEW MODEL
43© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
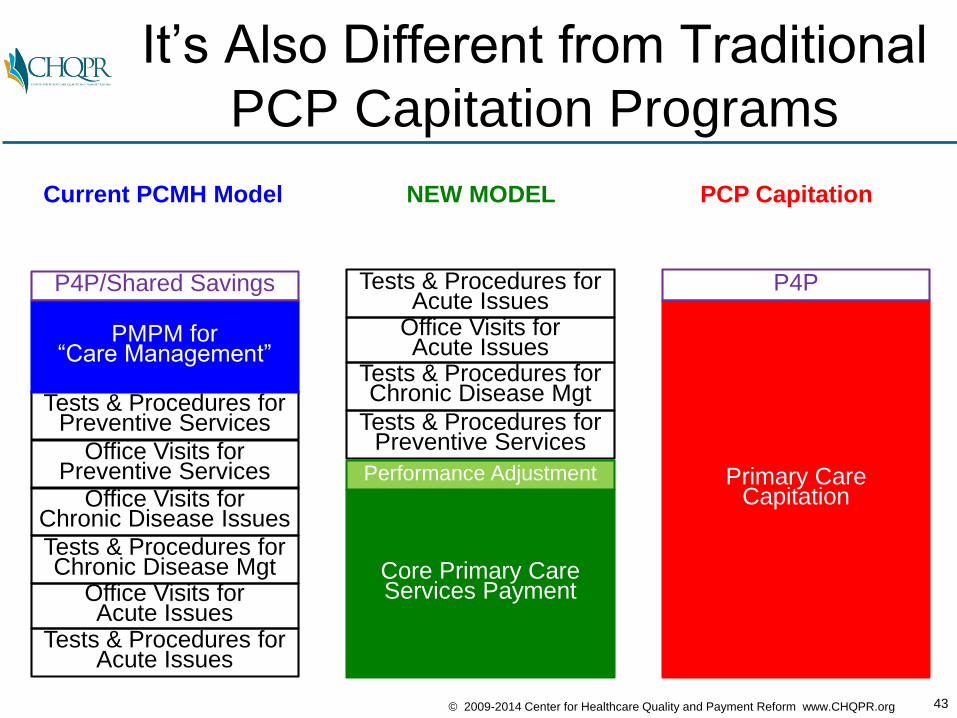
It’s Also Different from Traditional
PCP Capitation Programs
Office Visits forPreventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PMPM for“Care Management”
Primary CareCapitation
Current PCMH Model
P4P/Shared Savings P4P
PCP CapitationNEW MODEL
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
Core Primary CareServices Payment
Performance Adjustment
44© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
P4P
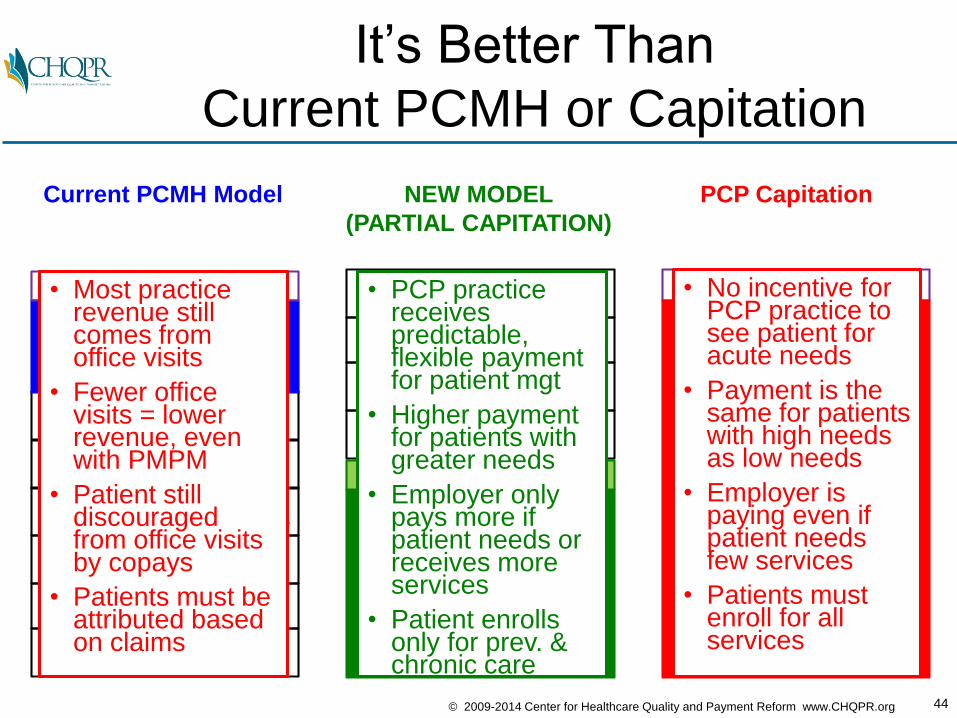
It’s Better Than
Current PCMH or Capitation
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
Office Visits forPreventive Services
Office Visits for Chronic Disease Issues
Tests & Procedures forPreventive Services
Tests & Procedures forChronic Disease Mgt
Tests & Procedures forAcute Issues
Office Visits forAcute Issues
PMPM for“Care Management”
Core Primary CareServices Payment
Primary CareCapitation
Current PCMH Model
P4P/Shared Savings
Performance Adjustment
PCP Capitation
• Most practice revenue still comes from office visits
• Fewer office visits = lower revenue, even with PMPM
• Patient still discouraged from office visits by copays
• Patients must beattributed based on claims
• No incentive for PCP practice to see patient for acute needs
• Payment is the same for patients with high needs as low needs
• Employer is paying even if patient needs few services
• Patients must enroll for all services
• PCP practice receives predictable, flexible payment for patient mgt
• Higher payment for patients withgreater needs
• Employer only pays more if patient needs or receives more services
• Patient enrollsonly for prev. & chronic care
NEW MODEL
(PARTIAL CAPITATION)
45© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
How Does This All Fit Into ACOs?
Diabetes
Heart
Disease
Back Pain
PATIENTS
Pregnancy
46© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
Each Patient Should Choose &
Use a Primary Care Practice…
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
Diabetes
Heart
Disease
47© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
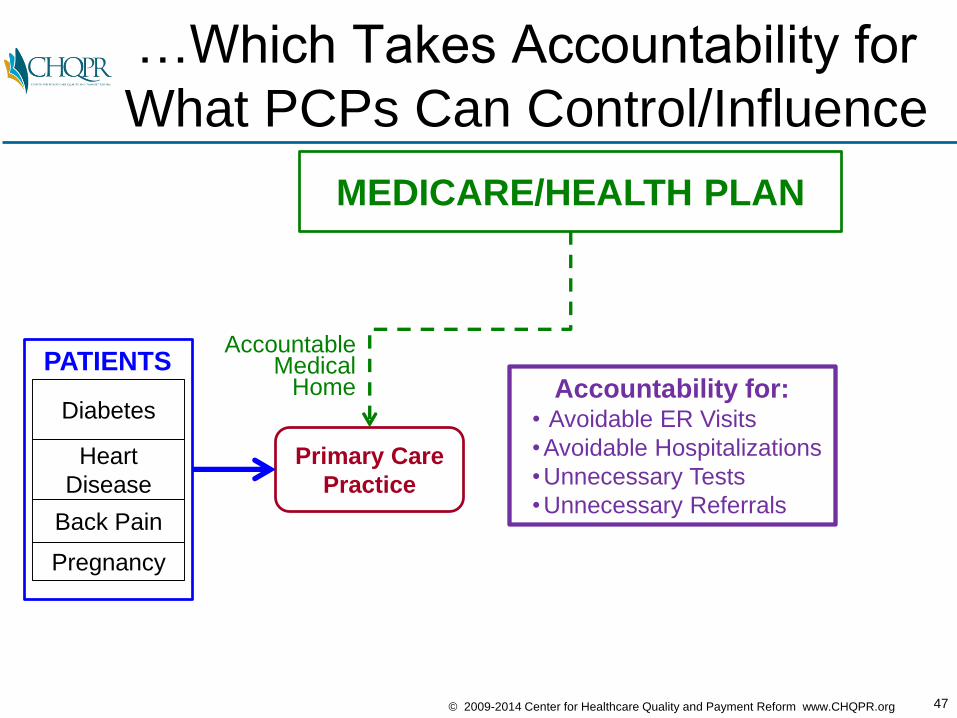
MEDICARE/HEALTH PLAN
…Which Takes Accountability for
What PCPs Can Control/Influence
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
AccountableMedical
Home Accountability for:• Avoidable ER Visits
•Avoidable Hospitalizations
•Unnecessary Tests
•Unnecessary Referrals
Diabetes
Heart
Disease
48© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
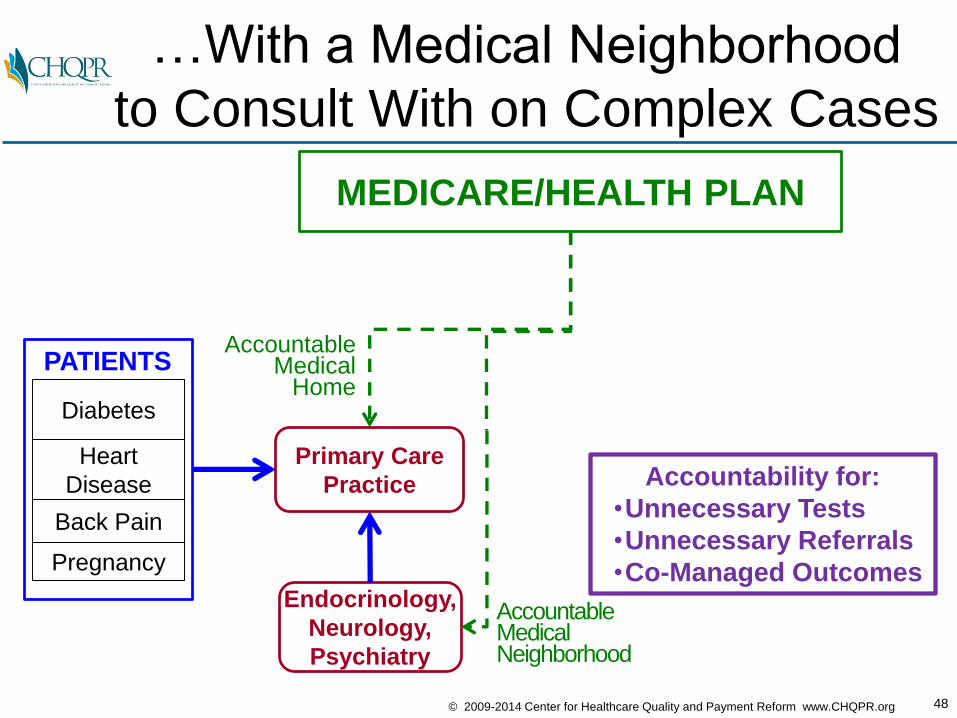
MEDICARE/HEALTH PLAN
…With a Medical Neighborhood
to Consult With on Complex Cases
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
AccountableMedical
Home
Endocrinology,
Neurology,
Psychiatry
AccountableMedicalNeighborhood
Accountability for:
•Unnecessary Tests
•Unnecessary Referrals
•Co-Managed Outcomes
Diabetes
Heart
Disease
49© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
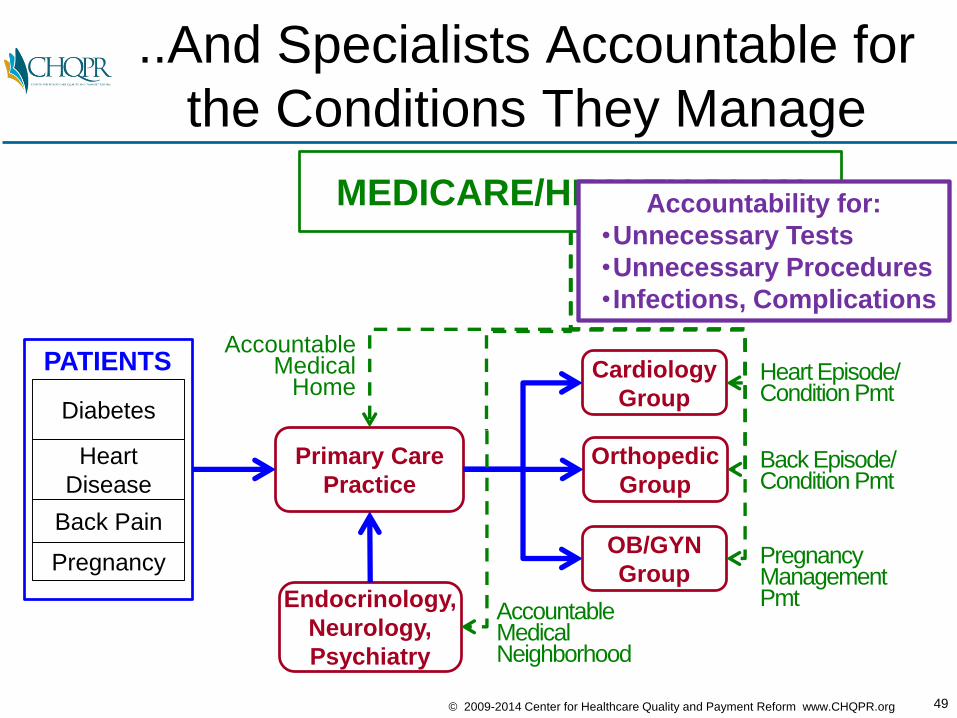
MEDICARE/HEALTH PLAN
..And Specialists Accountable for
the Conditions They Manage
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
Orthopedic
Group
OB/GYN
Group
Cardiology
GroupHeart Episode/Condition Pmt
Back Episode/Condition Pmt
PregnancyManagement Pmt
AccountableMedical
Home
Endocrinology,
Neurology,
Psychiatry
AccountableMedicalNeighborhood
Accountability for:
•Unnecessary Tests
•Unnecessary Procedures
•Infections, Complications
Diabetes
Heart
Disease
50© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
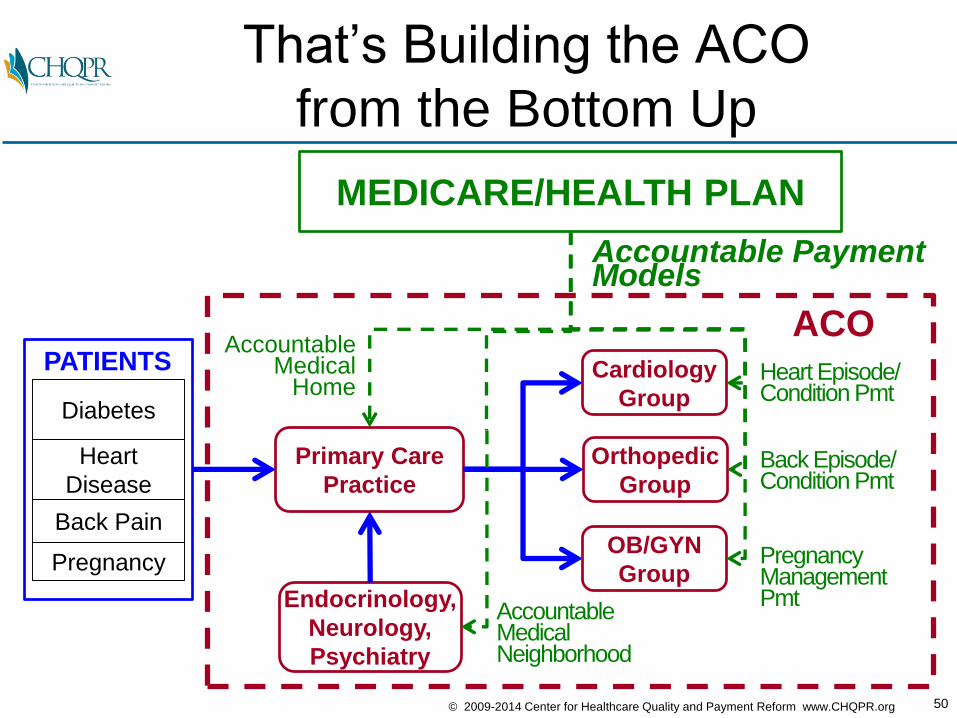
MEDICARE/HEALTH PLAN
That’s Building the ACO
from the Bottom Up
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
Orthopedic
Group
OB/GYN
Group
Cardiology
GroupHeart Episode/Condition Pmt
Back Episode/Condition Pmt
PregnancyManagement Pmt
AccountableMedical
Home
Endocrinology,
Neurology,
Psychiatry
AccountableMedicalNeighborhood
ACO
Accountable PaymentModels
Diabetes
Heart
Disease
51© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
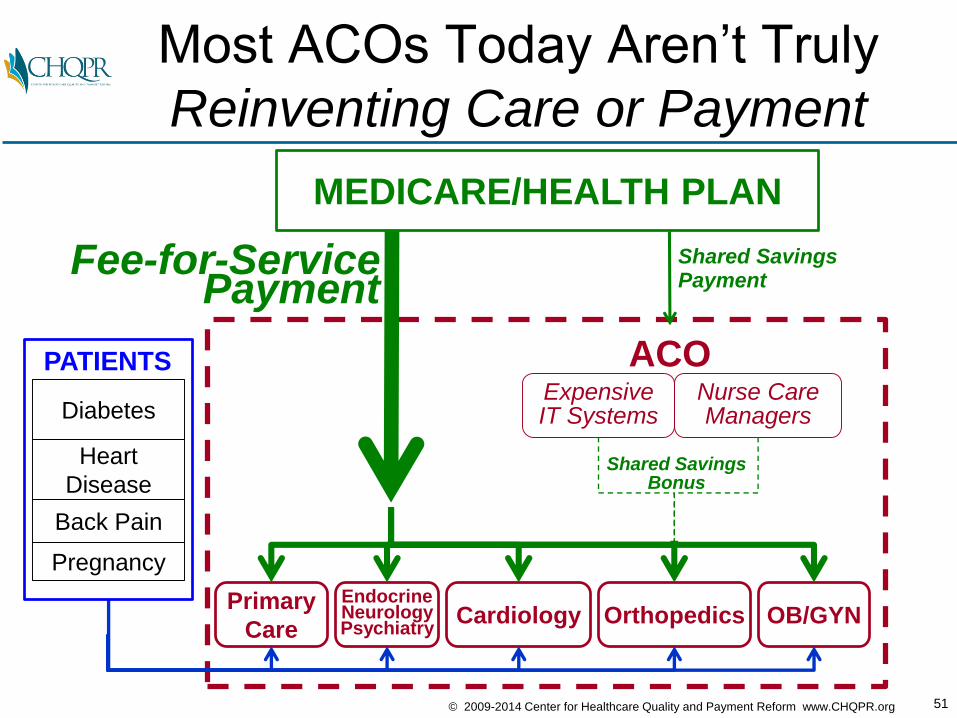
MEDICARE/HEALTH PLAN
Shared SavingsPayment
Primary
Care
ACO
Orthopedics OB/GYNCardiology
Most ACOs Today Aren’t Truly
Reinventing Care or Payment
Fee-for-ServicePayment
Expensive IT Systems
EndocrineNeurologyPsychiatry
Nurse Care Managers
Back Pain
PATIENTS
Pregnancy
Shared SavingsBonus
Diabetes
Heart
Disease
52© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
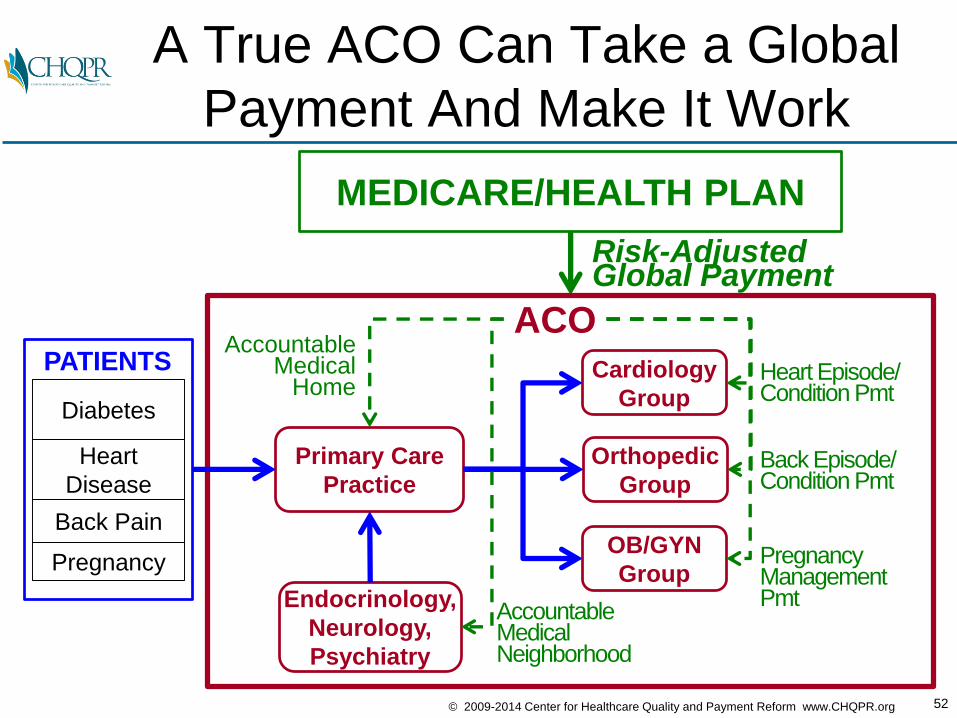
MEDICARE/HEALTH PLAN
A True ACO Can Take a Global
Payment And Make It Work
Back Pain
PATIENTS
Pregnancy
Primary Care
Practice
ACO
Orthopedic
Group
OB/GYN
Group
Cardiology
GroupHeart Episode/Condition Pmt
Back Episode/Condition Pmt
PregnancyManagement Pmt
AccountableMedical
Home
Endocrinology,
Neurology,
Psychiatry
Risk-AdjustedGlobal Payment
AccountableMedicalNeighborhood
Diabetes
Heart
Disease
53© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
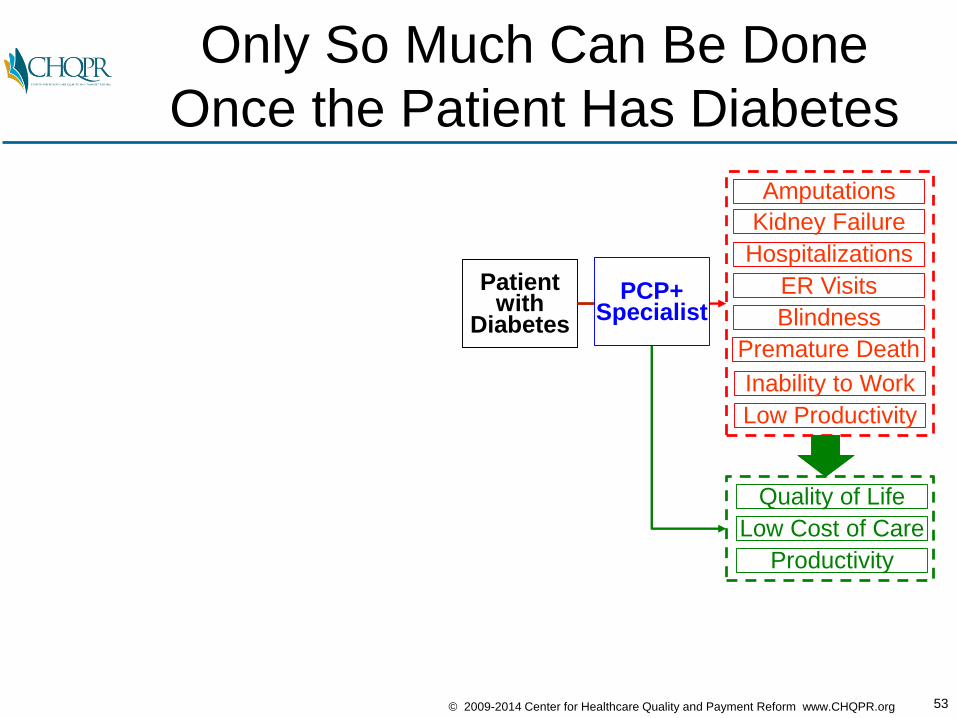
Only So Much Can Be Done
Once the Patient Has Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
Patient with
Diabetes
PCP+Specialist
54© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
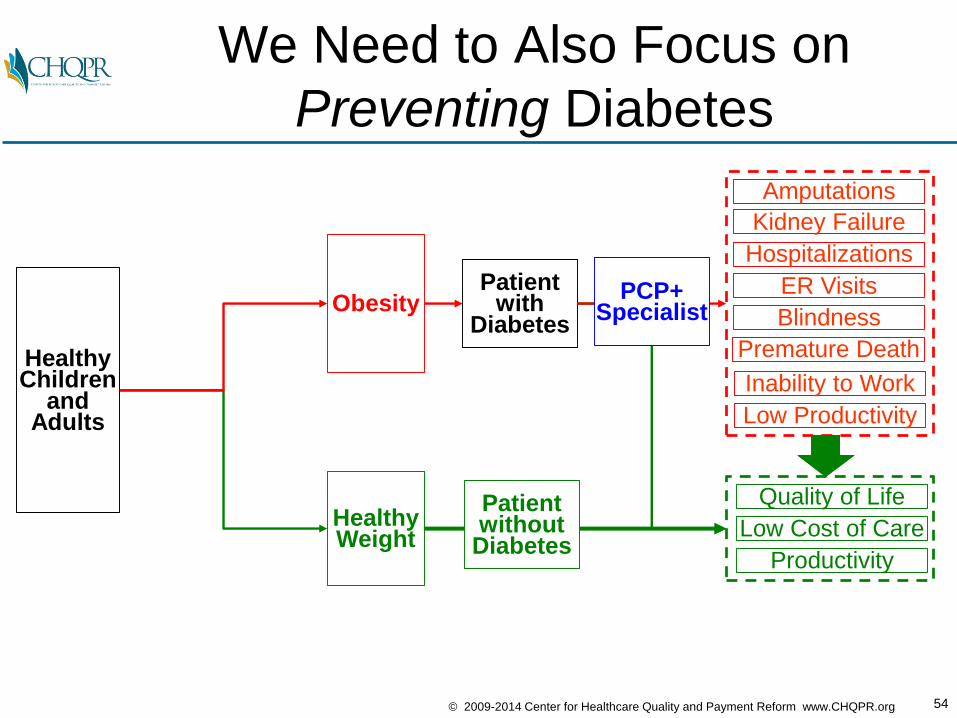
We Need to Also Focus on
Preventing Diabetes
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
HealthyChildren
andAdults
Obesity
HealthyWeight
Patient with
Diabetes
PCP+Specialist
Patient without
Diabetes
55© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
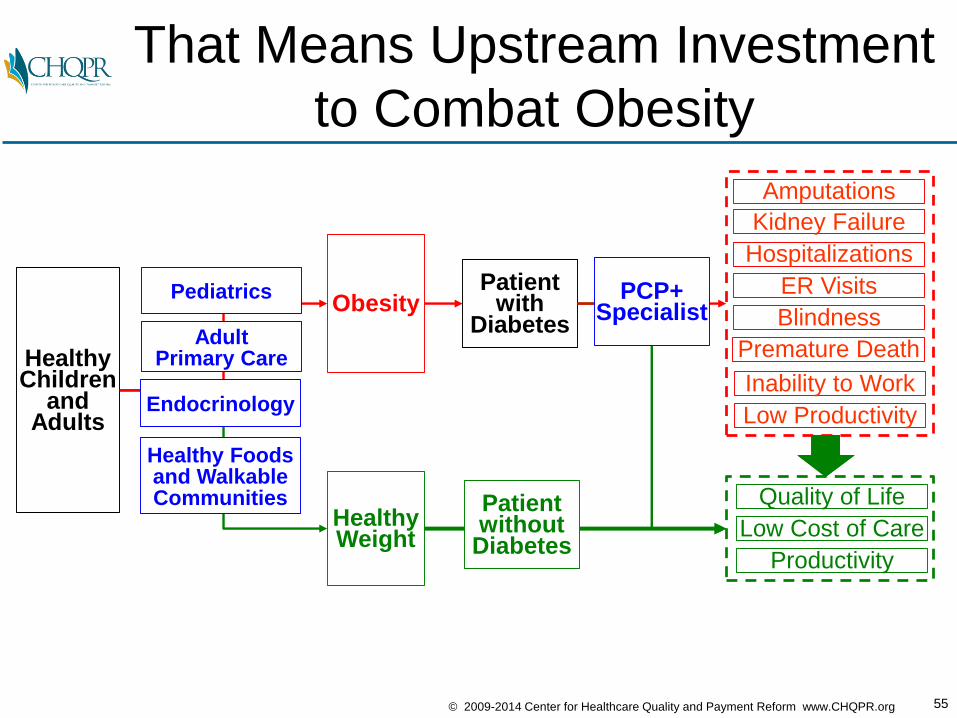
That Means Upstream Investment
to Combat Obesity
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
HealthyChildren
andAdults
Obesity
HealthyWeight
Patient with
Diabetes
PCP+Specialist
Pediatrics
AdultPrimary Care
Endocrinology
Patient without
Diabetes
Healthy Foodsand WalkableCommunities
56© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
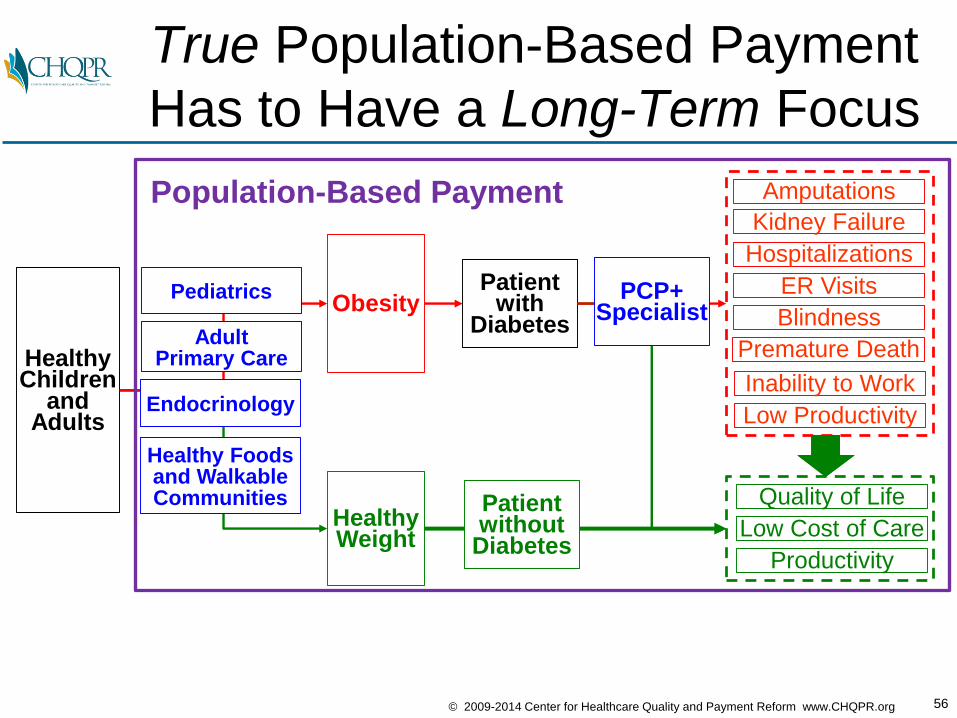
True Population-Based Payment
Has to Have a Long-Term Focus
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
HealthyChildren
andAdults
Obesity
HealthyWeight
Patient with
Diabetes
PCP+Specialist
Population-Based Payment
Patient without
Diabetes
Pediatrics
AdultPrimary Care
Endocrinology
Healthy Foodsand WalkableCommunities
57© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
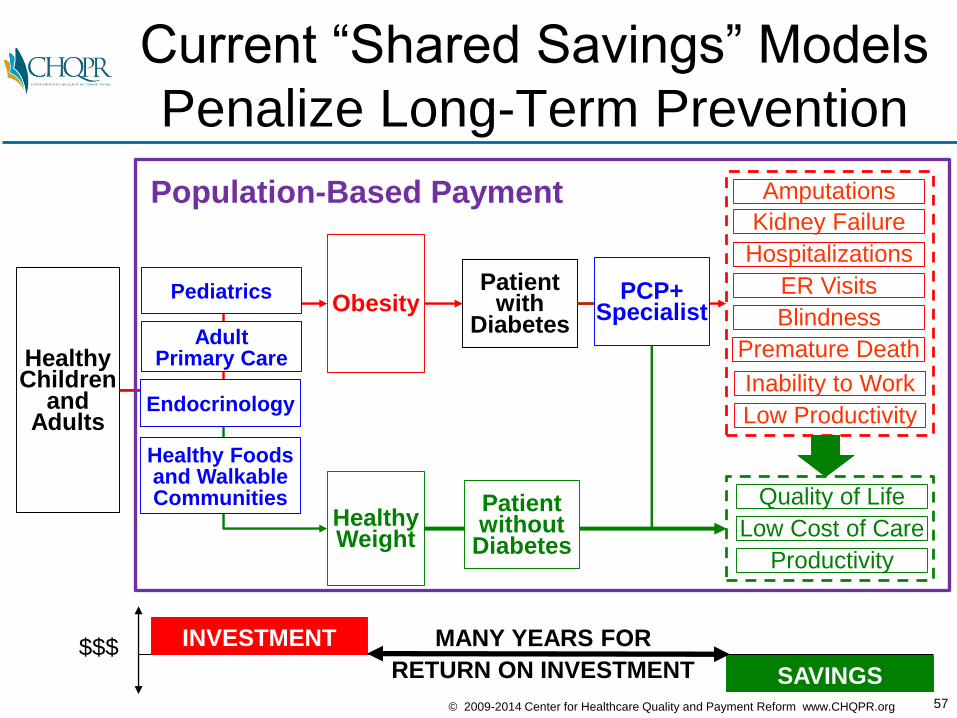
MANY YEARS FOR
RETURN ON INVESTMENT
Current “Shared Savings” Models
Penalize Long-Term Prevention
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
HealthyChildren
andAdults
Obesity
HealthyWeight
Patient with
Diabetes
PCP+Specialist
Population-Based Payment
$$$ INVESTMENT
SAVINGS
Patient without
Diabetes
Pediatrics
AdultPrimary Care
Endocrinology
Healthy Foodsand WalkableCommunities
58© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
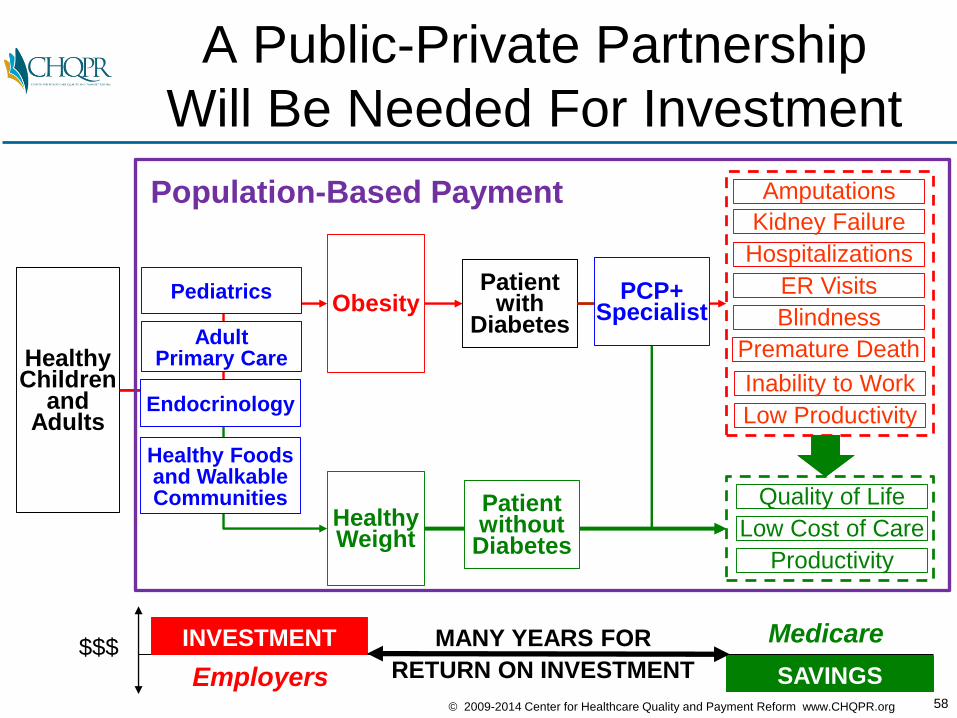
MANY YEARS FOR
RETURN ON INVESTMENT
A Public-Private Partnership
Will Be Needed For Investment
Premature Death
Amputations
Blindness
Kidney Failure
Hospitalizations
ER Visits
Inability to Work
Low Productivity
Quality of Life
Low Cost of Care
Productivity
HealthyChildren
andAdults
Obesity
HealthyWeight
Patient with
Diabetes
PCP+Specialist
Population-Based Payment
$$$ INVESTMENT
SAVINGSEmployers
Medicare
Patient without
Diabetes
Pediatrics
AdultPrimary Care
Endocrinology
Healthy Foodsand WalkableCommunities
59© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
In Summary
• Most current “reforms” (pay for performance, value-based purchasing, and shared savings) don’t solve the real problems with care delivery and may make things worse
• True payment reform can be a win-win-win:– Better care for patients
– Lower spending for payers
– Financially viable PCP and endocrinology practices that attract new physicians
• Condition-based payment for diabetes can be an important building block for successful ACOs
• Medicare and commercial health plans need to implement new payment models designed by physicians
• Multi-year contracts and public-private partnerships will be needed to adequately invest in prevention for long-term savings and better outcomes
60© 2009-2014 Center for Healthcare Quality and Payment Reform www.CHQPR.org
Learn More About Win-Win-Win
Payment and Delivery Reform
Center for Healthcare Quality and Payment Reform
www.PaymentReform.org
For More Information:
Harold D. MillerPresident and CEO
Center for Healthcare Quality and Payment Reform
(412) 803-3650
www.CHQPR.org
www.PaymentReform.org
Recommended

















