Reducing Mental Health Disparities
King Davis, Ph.D.
What is the relationship between the mental health services system and help seeking
behavior patterns of people of color?
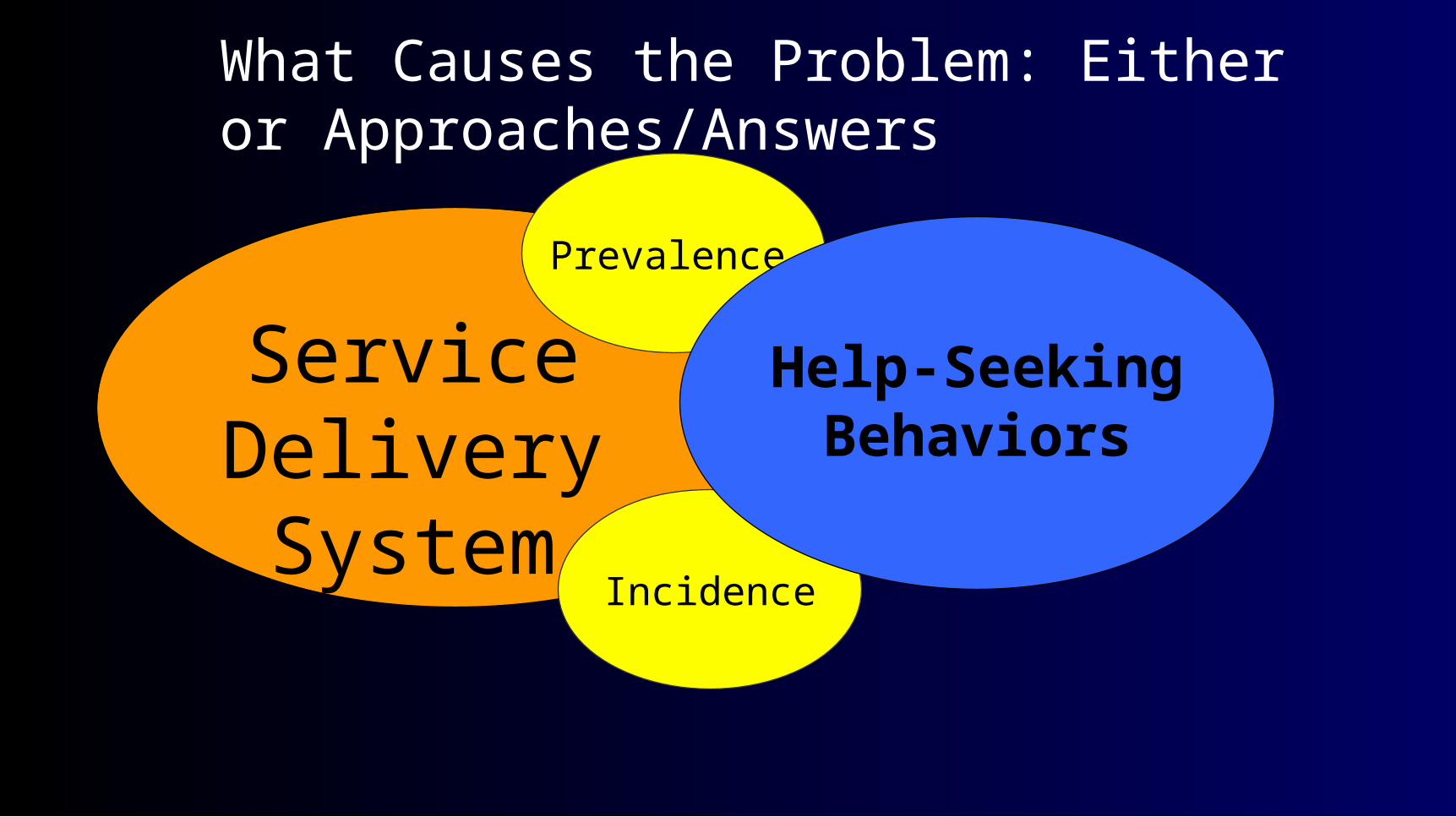
Service Delivery System
Incidence
Prevalence
Help-Seeking Behaviors
What Causes the Problem: Either or Approaches/Answers
What is Help – Seeking?• Help-seeking involves a number of pro-active steps
that take a person, family, or community from the point of recognizing a problem exists to using [entrusting] an external resource to solve, lessen, or cure the problem.
The Help Seeking Paradox
• Although there are reportedly minimal differences in rates, there are marked differences in help seeking by race, ethnicity, language, gender, residence, and other identifiable characteristics.
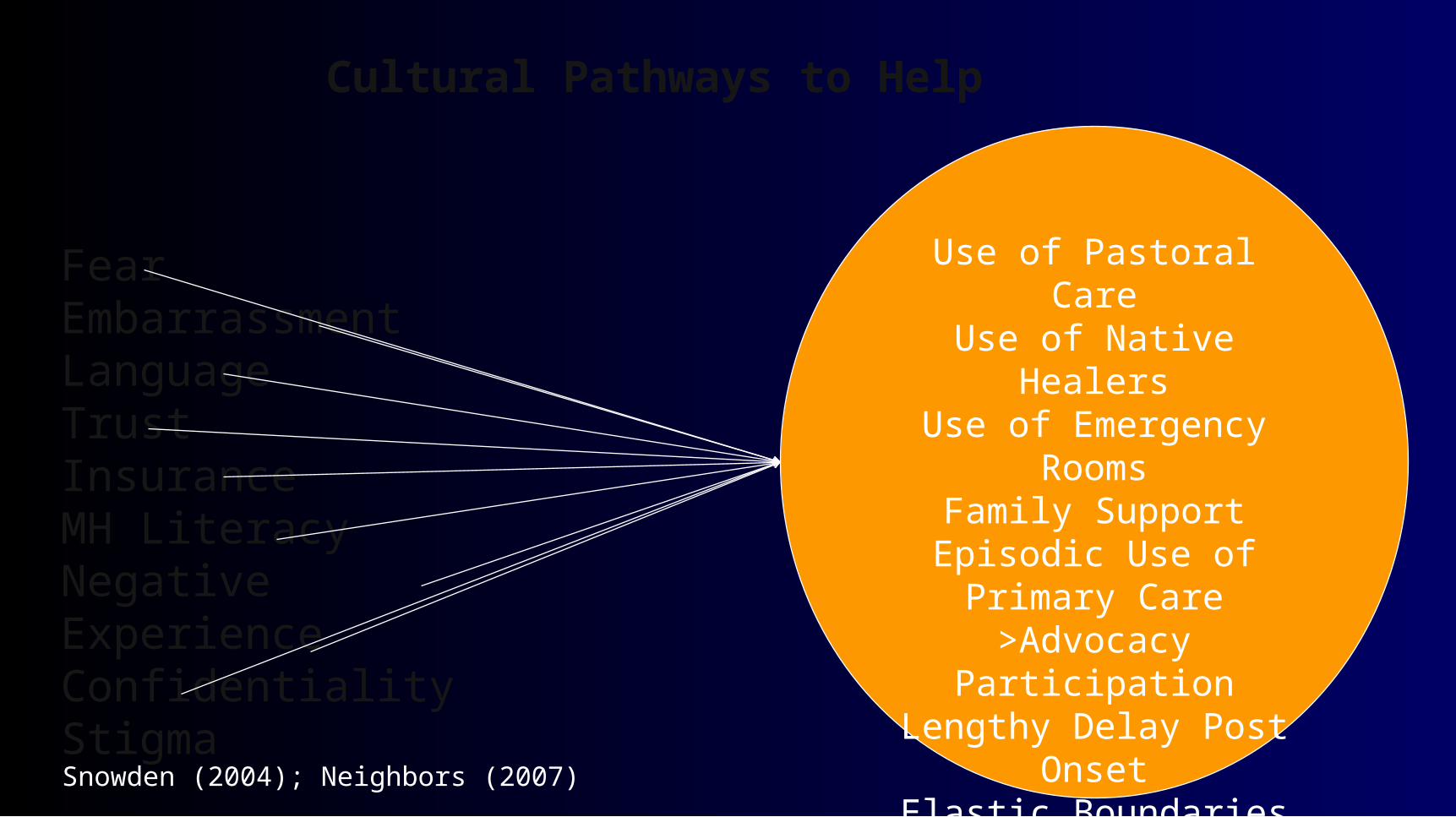
Use of Pastoral CareUse of Native Healers
Use of Emergency RoomsFamily Support
Episodic Use of Primary Care
>Advocacy ParticipationLengthy Delay Post Onset
Elastic Boundaries
Cultural Pathways to Help
FearEmbarrassmentLanguageTrustInsuranceMH LiteracyNegative ExperienceConfidentialityStigma
Snowden (2004); Neighbors (2007)
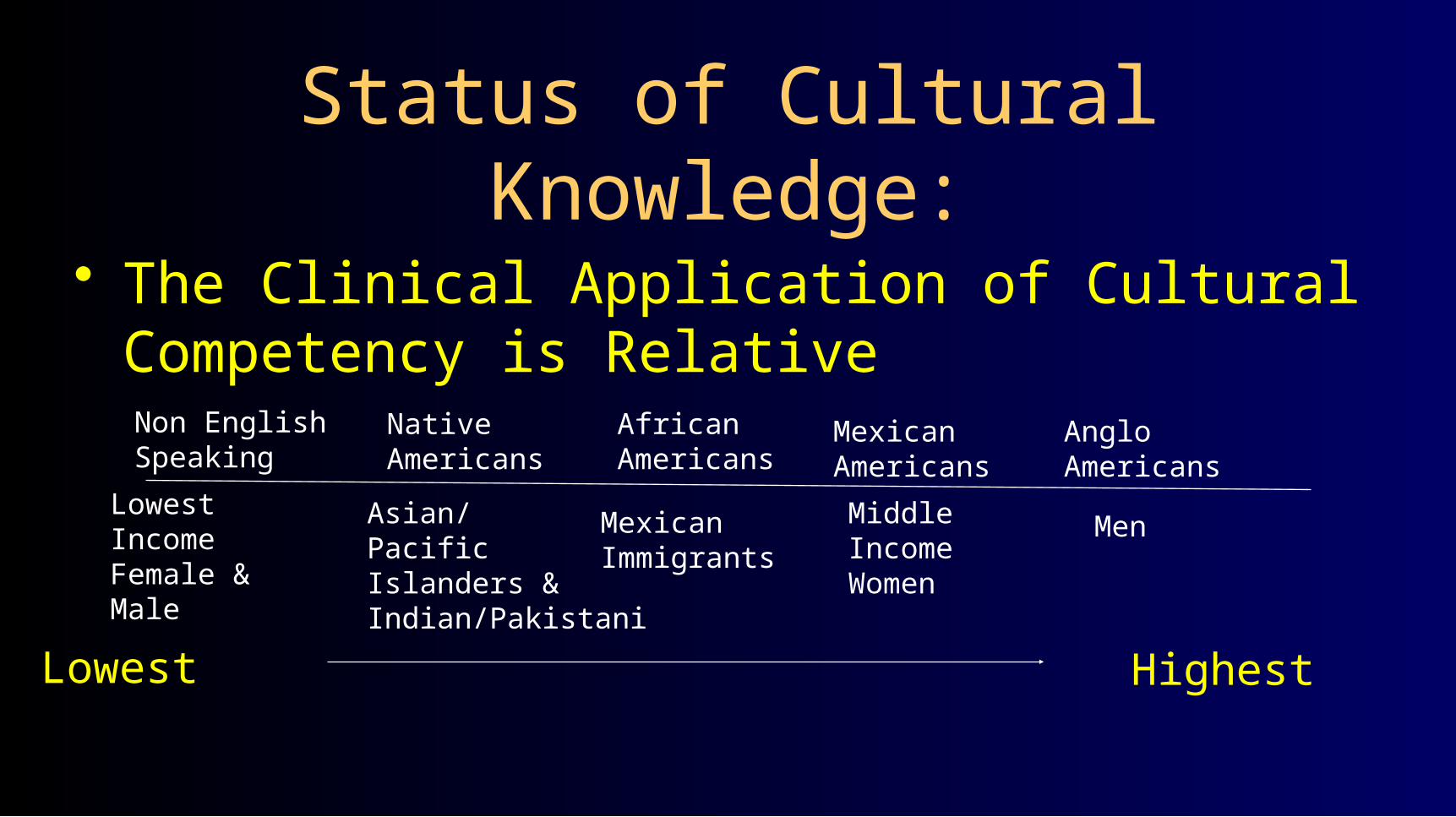
Status of Cultural Knowledge:
• The Clinical Application of Cultural Competency is Relative
Non EnglishSpeaking
Native Americans
Lowest IncomeFemale & Male
Asian/PacificIslanders &Indian/Pakistani
AfricanAmericans
MexicanImmigrants
MexicanAmericans
MiddleIncomeWomen
AngloAmericans
Men
Lowest Highest

Working Definition of Disparity
• Measurable, not assumed, differences between two or more objects, groups, people, or an absence of parity or equality between them. Unlike health disparities, mental health disparities are mainly in service patterns rather than rates of morbidity.
King Davis, 2009
Mental Health Disparity
Principally, a measurable difference in services [clinical choices and decisions], risk, help seeking, outcome, prevalence/incidence, and/or mortality by race, culture, ethnicity, language, gender, or any other identifiable characteristic.
Help-Seeking Behaviors
Elements in Disparities
Service System
Public Policies
AcademicTraining & EducationPrograms
Disparity
“…should be viewed as a train of events leading to a difference in:– Access to, utilization of, or quality of care– Health status, or– Health outcome
….that deserves scrutiny.”
Pearcy & Keppel 2009
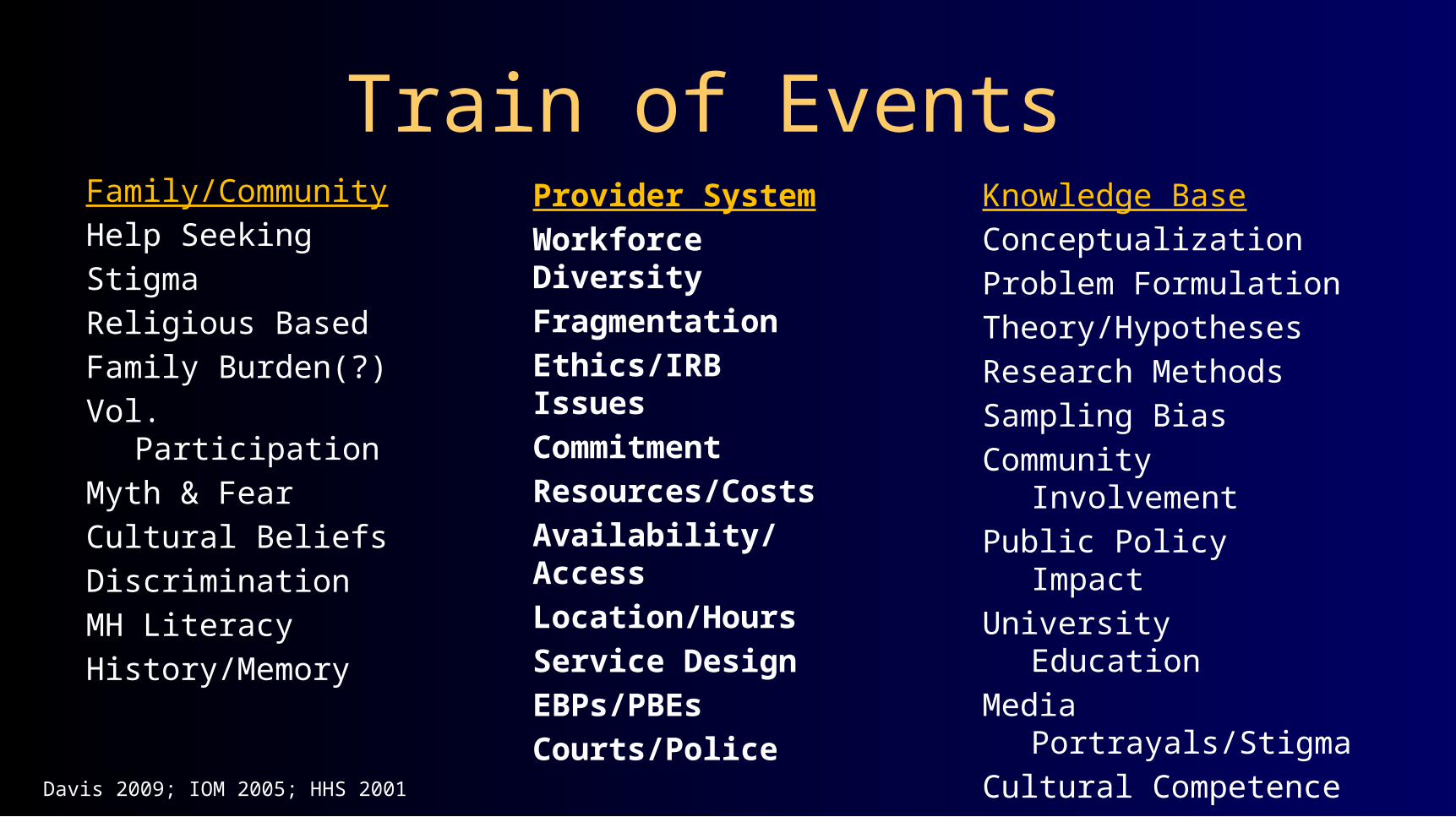
Train of Events Family/Community
Help Seeking
Stigma
Religious Based
Family Burden(?)
Vol. Participation
Myth & Fear
Cultural Beliefs
Discrimination
MH Literacy
History/Memory
Provider System
Workforce Diversity
Fragmentation
Ethics/IRB Issues
Commitment
Resources/Costs
Availability/Access
Location/Hours
Service Design
EBPs/PBEs
Courts/Police
Knowledge Base
Conceptualization
Problem Formulation
Theory/Hypotheses
Research Methods
Sampling Bias
Community Involvement
Public Policy Impact
University Education
Media Portrayals/Stigma
Cultural Competence
Comparative Outcomes
Davis 2009; IOM 2005; HHS 2001
FRAGMENTATION
• The U.S. health, mental health and substance abuse treatment systems have developed independent of each other and of primary care. They typically are operated separately, without regard for the reality that physical and behavioral health are linked if not the same.
• Training programs reflect the same fragmentation.
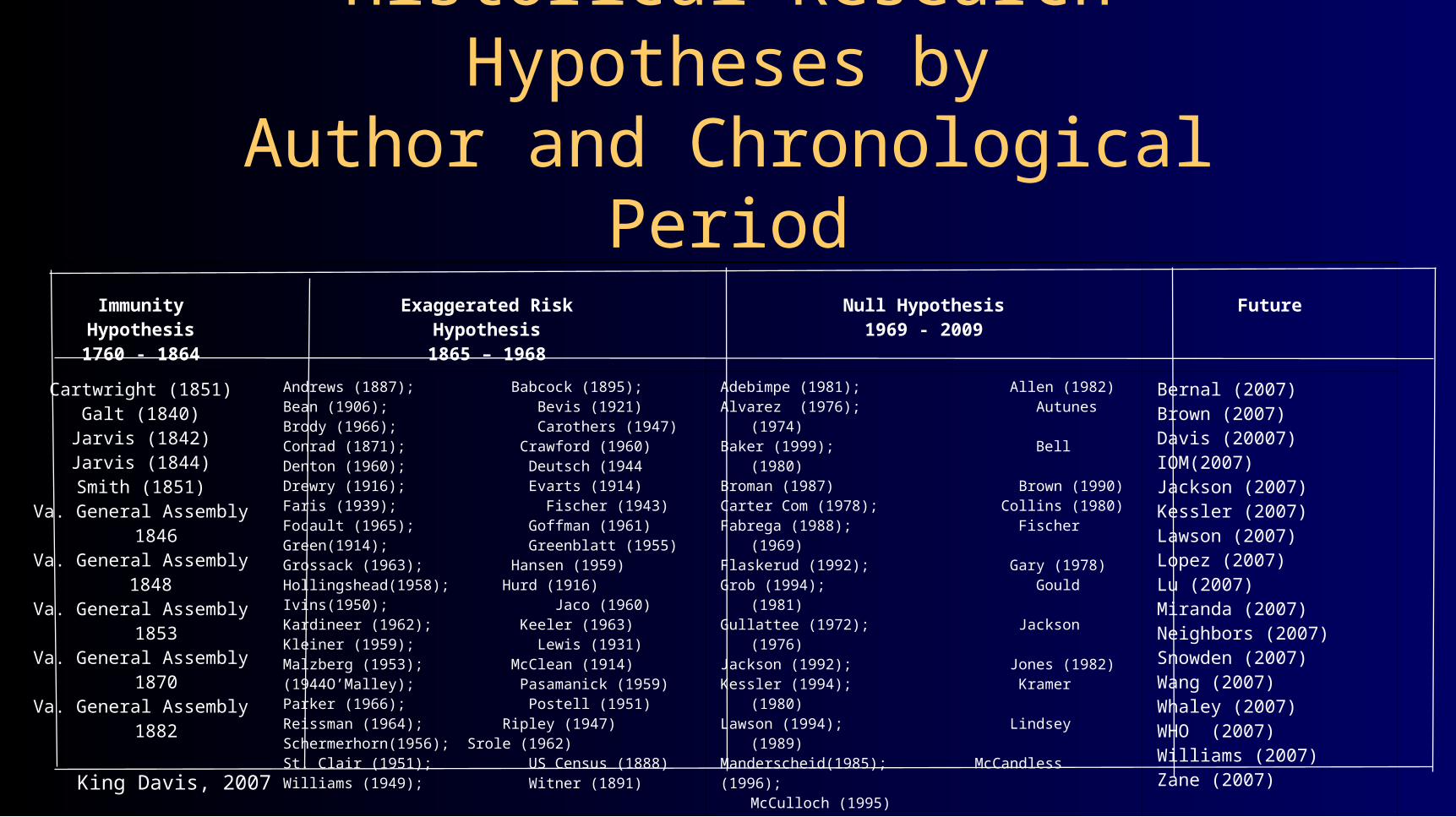
Historical Research Hypotheses byAuthor and Chronological Period
ImmunityHypothesis1760 - 1864
Exaggerated RiskHypothesis1865 – 1968
Null Hypothesis1969 - 2009
Future
Cartwright (1851)Galt (1840)
Jarvis (1842)Jarvis (1844)Smith (1851)
Va. General Assembly 1846Va. General Assembly 1848 Va. General Assembly 1853Va. General Assembly 1870Va. General Assembly 1882
Andrews (1887); Babcock (1895); Bean (1906); Bevis (1921) Brody (1966); Carothers (1947)Conrad (1871); Crawford (1960)Denton (1960); Deutsch (1944Drewry (1916); Evarts (1914)Faris (1939); Fischer (1943)Focault (1965); Goffman (1961)Green(1914); Greenblatt (1955)Grossack (1963); Hansen (1959)Hollingshead(1958); Hurd (1916)Ivins(1950); Jaco (1960)Kardineer (1962); Keeler (1963)Kleiner (1959); Lewis (1931)Malzberg (1953); McClean (1914)(1944O’Malley); Pasamanick (1959)Parker (1966); Postell (1951)Reissman (1964); Ripley (1947)Schermerhorn(1956); Srole (1962)St. Clair (1951); US Census (1888)Williams (1949); Witner (1891)
Adebimpe (1981); Allen (1982)Alvarez (1976); Autunes (1974)Baker (1999); Bell (1980)Broman (1987) Brown (1990)Carter Com (1978); Collins (1980)Fabrega (1988); Fischer (1969)Flaskerud (1992); Gary (1978)Grob (1994); Gould (1981)Gullattee (1972); Jackson (1976)Jackson (1992); Jones (1982)Kessler (1994); Kramer (1980)Lawson (1994); Lindsey (1989)Manderscheid(1985); McCandless (1996); McCulloch (1995)Milstein (1995); Mollica (1980)Neighbors (1987); Poussaint (1998)Rack (1982); Ramm (1989)Regier (1993); Robins (1991)Rothman(1970); Ruiz (1990)Simon (1973); Snowden (1990)Thomas (1972); Warheit (1998)Wexberg (1998); Williams (1986)Willie (1973)
Bernal (2007)Brown (2007)Davis (20007)IOM(2007)Jackson (2007)Kessler (2007)Lawson (2007)Lopez (2007)Lu (2007)Miranda (2007)Neighbors (2007)Snowden (2007)Wang (2007)Whaley (2007)WHO (2007)Williams (2007)Zane (2007)
King Davis, 2007
Examples of Disparities
• Admissions Involuntary Commitments• Length of Stay Access to Service • Recidivism RatesDiagnosis of SMI• Use of Police Quality of Care• Homelessness Use of Medication - EBPs• Mortality Rates Accuracy of Diagnosis
King Davis, 2009
Mental Health, Health, Mortality and Race
• Individuals with a diagnosis of severe mental illness die an average of 25-32 years earlier than individuals without mental illness.
• What are the implications for people of color with severe mental illness?
• What solutions can be offered to prevent or reduce the rate of deaths?
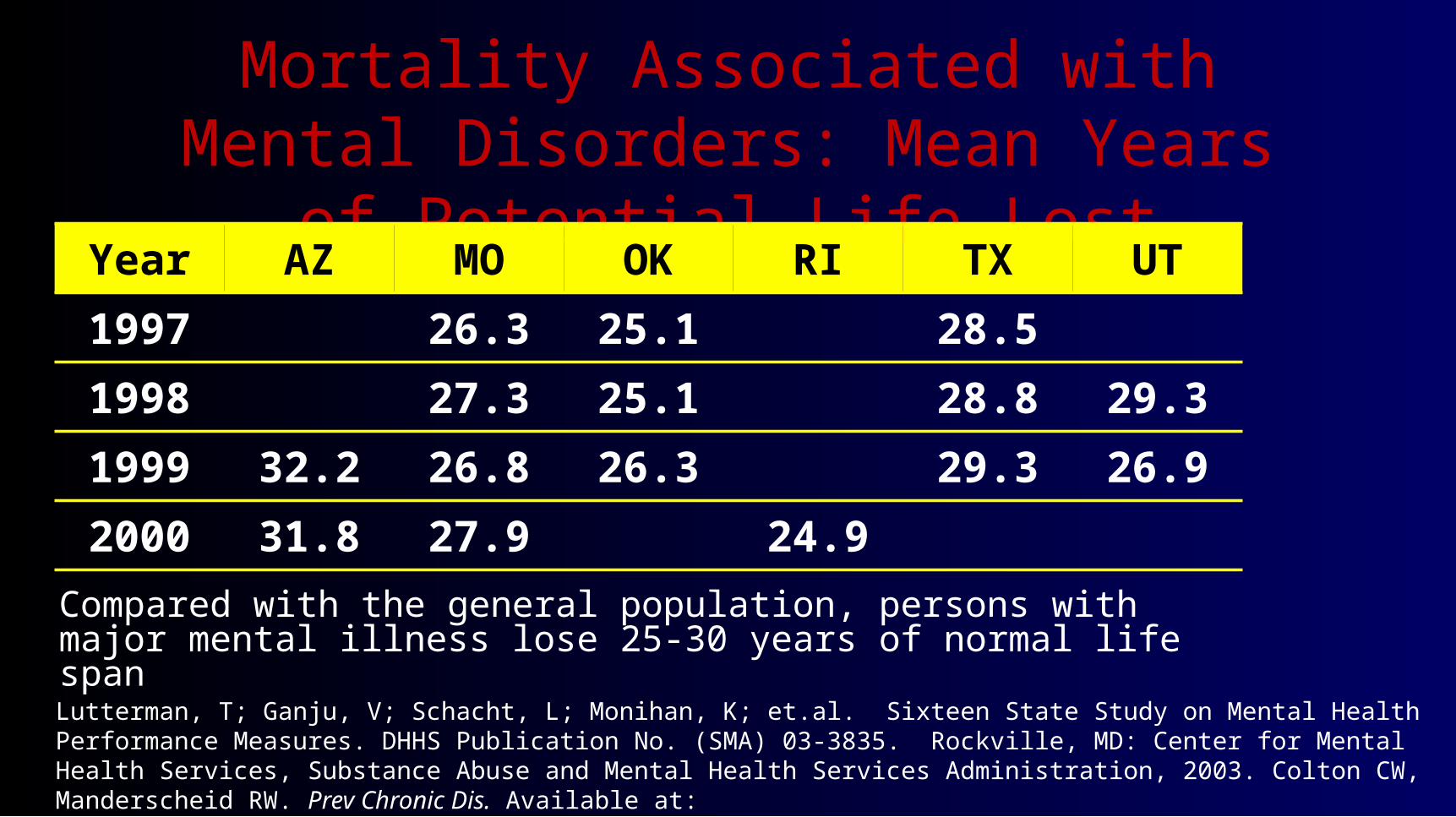
Mortality Associated with Mental Disorders: Mean Years of Potential Life Lost
Compared with the general population, persons with major mental illness lose 25-30 years of normal life span
Year AZ MO OK RI TX UT
1997 26.3 25.1 28.5
1998 27.3 25.1 28.8 29.3
1999 32.2 26.8 26.3 29.3 26.9
2000 31.8 27.9 24.9
Lutterman, T; Ganju, V; Schacht, L; Monihan, K; et.al. Sixteen State Study on Mental Health Performance Measures. DHHS Publication No. (SMA) 03-3835. Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, 2003. Colton CW, Manderscheid RW. Prev Chronic Dis. Available at: ttp://www.cdc.gov/pcd/issues/2006/apr/05_0180.htm.

Access and Quality of Care• SMI may be a health risk factor because of:
– Patient factors, e.g.: amotivation, fearfulness, homelessness, victimization/trauma, resources, advocacy, unemployment, incarceration, social instability, IV drug use, etc
– Provider factors: Comfort level and attitude of healthcare providers, coordination between mental health and general health care, stigma,
– System factors: Funding, fragmentationJoe Parks, MD 2009
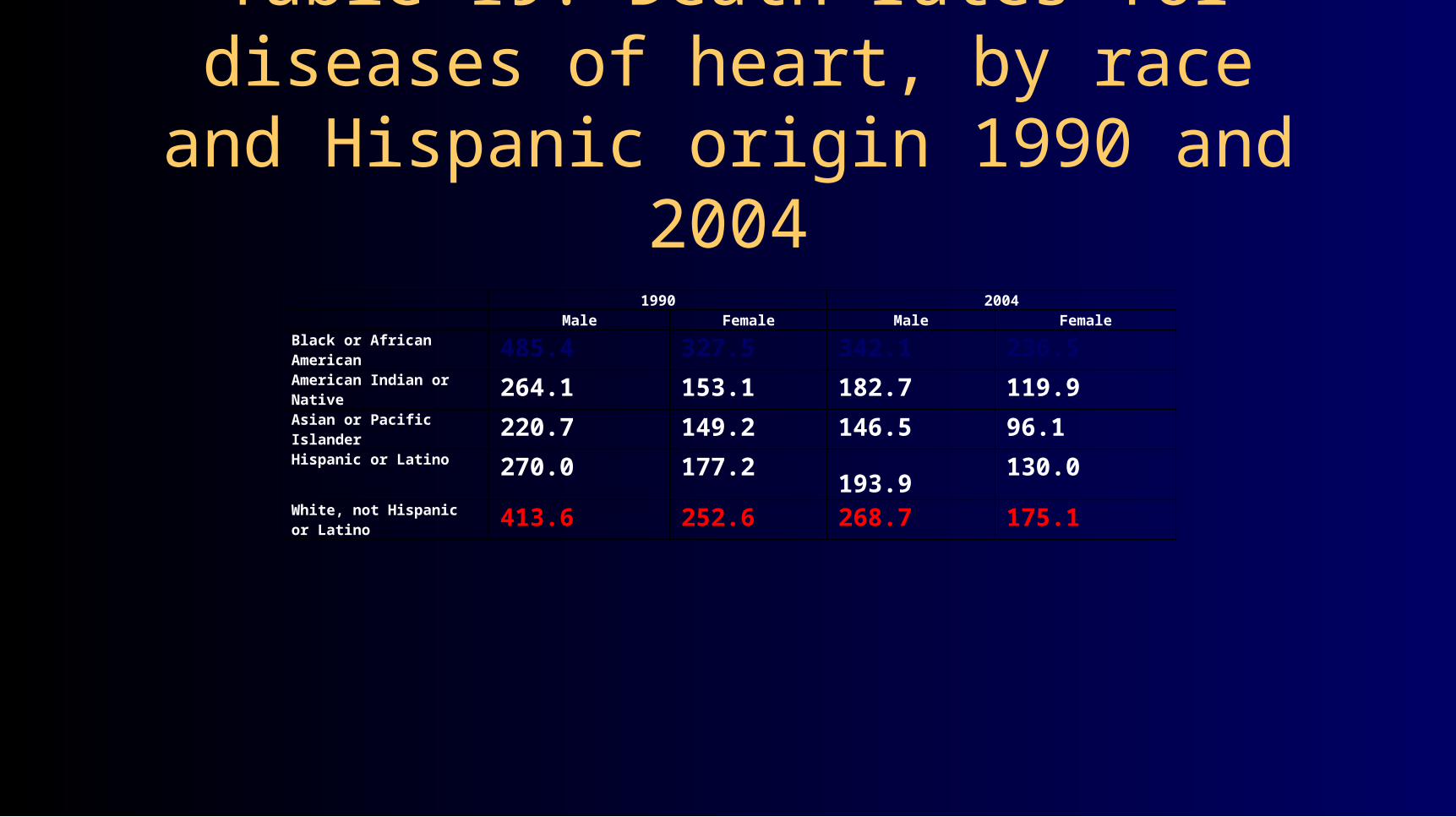
1990 2004Male Female Male Female
Black or African American 485.4 327.5 342.1 236.5American Indian or Native 264.1 153.1 182.7 119.9Asian or Pacific Islander 220.7 149.2 146.5 96.1Hispanic or Latino 270.0 177.2 193.9 130.0
White, not Hispanic or Latino 413.6 252.6 268.7 175.1
Table 19. Death rates for diseases of heart, by race and Hispanic origin 1990 and 2004
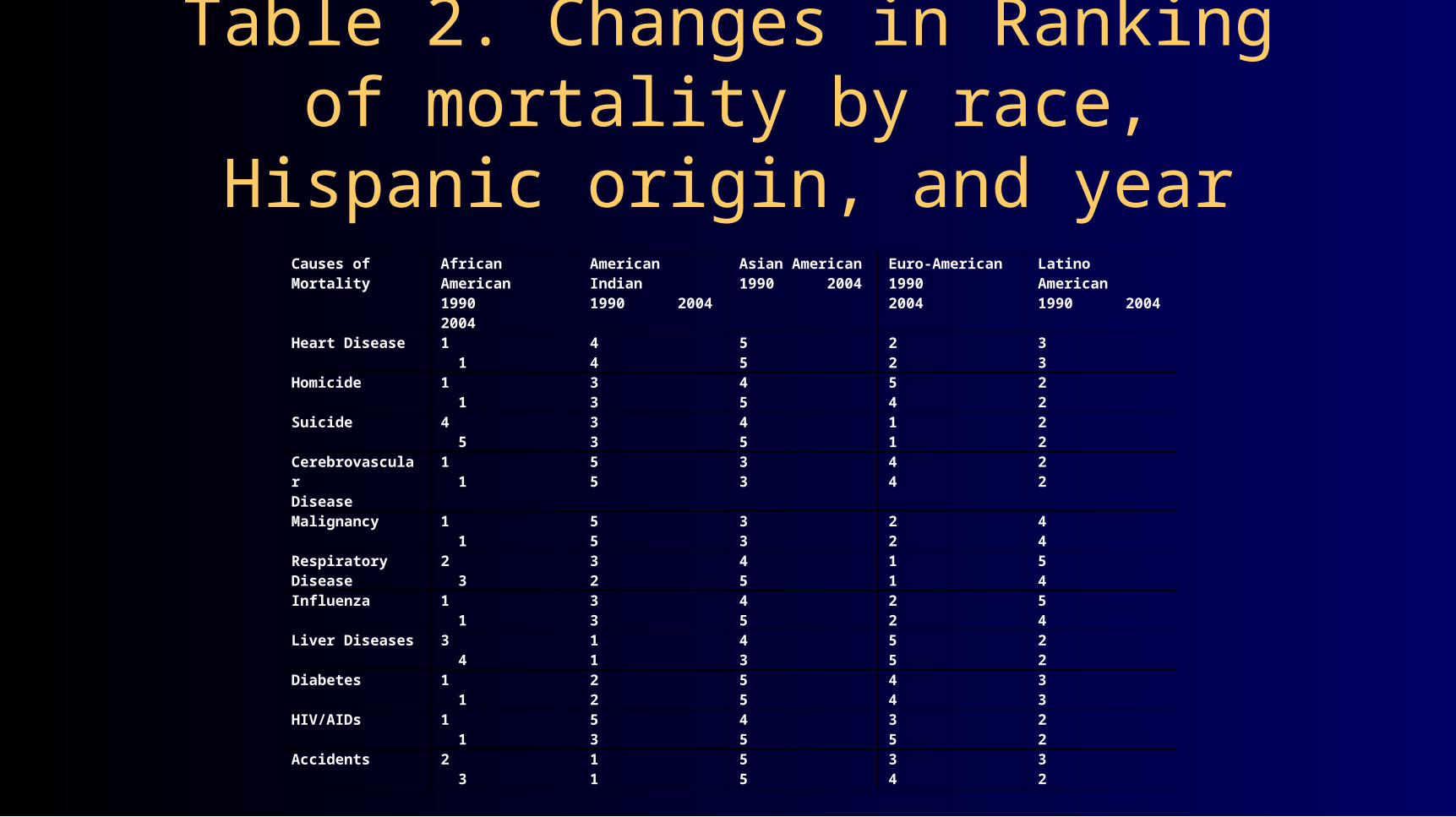
Causes of Mortality African American1990 2004
American Indian1990 2004
Asian American1990 2004
Euro-American1990 2004
Latino American1990 2004
Heart Disease 1 1 4 4 5 5 2 2 3 3Homicide 1 1 3 3 4 5 5 4 2 2Suicide 4 5 3 3 4 5 1 1 2 2CerebrovascularDisease
1 1 5 5 3 3 4 4 2 2
Malignancy 1 1 5 5 3 3 2 2 4 4Respiratory Disease 2 3 3 2 4 5 1 1 5 4
Influenza 1 1 3 3 4 5 2 2 5 4Liver Diseases 3 4 1 1 4 3 5 5 2 2Diabetes 1 1 2 2 5 5 4 4 3 3HIV/AIDs 1 1 5 3 4 5 3 5 2 2Accidents 2 3 1 1 5 5 3 4 3 2
Table 2. Changes in Ranking of mortality by race, Hispanic origin, and year

Neighbors, Baser & Martin (2007). unpublished data from the National Survey of American Life
Cumulative Percentages
# years after disorder onset 1 2 5 10 15 20 30
Major Depression African American 27.2 31.7 39.0 46.4 57.4 64.3 77.6
White American 39.5 44.4 51.1 58.2 64.7 70.3 78.0
Bipolar Disorder
African American 17.3 19.5 24.5 33.0 38.1 38.1 43.9
White American 40.5 44.3 49.8 58.2 70.5 71.3 79.4
Black-White Comparison of Cumulative Proportions of Cases making Treatment Contact by Selected Years
After Disorder Onset

CardiovascularDisease
Depression
Sickle Cell
Schizophrenia
PeriodontalDisease
Diabetes
HIV
Alcohol Abuse
Cancer Obesity
BipolarPersonalityDisorder Dementia
HomicidesDomestic Violence
Unemployment
Sub-Prime Loans
Low BirthWeightBabies
Low Income
AssetAccumulation
VotingPoliticalOffice
SentencingCriminalJustice
Cocaine Use/Sale
Housing &Homelessness
NutritionLiteracy
Maternal/Infant Deaths
MentalRetardation
Uninsured
GraduationRates
CrimeVictims
CapitalPunishment
King Davis, 2003
Why be Concerned: Multiple Costs• Excess Preventable Deaths• Untreated Illness & Lower Achievement• Excess Hospital Admissions & Readmissions• Misdiagnosis & Poor Application of EBPs• Community Suspicion and Mistrust• Staff Division and Conflict• Absence of Scientific Knowledge & Theory• Ethical Conflict: Professional & Personal• Increased Direct and Indirect Costs: Tremendous Waste• Loss of Input from Special Markets: Volunteers/Policy• Clinical Dropouts• Cultural Malpractice• Public Customers are Disproportionately Persons of Color!
King Davis, 2008

Path Dependence Analysis
Fragmentation
>Funding
Trauma
UsageRate
EmergencyUse
Beliefs InfoIncreased Admissions Stigma
Family SupportDelayed Help
Courts
Police/Sheriff
Fear
>Illness
FL. Statutes

Research Foci: Train of Events Family/Community
Help Seeking
Stigma
Religious Based
Family Burden(?)
Vol. Participation
Myth & Fear
Cultural Beliefs
Discrimination
MH Literacy
History/Memory
Provider System
Workforce Diversity
Fragmentation
Ethics/IRB Issues
Commitment
Resources/Costs
Availability/Access
Location/Hours
Service Design
EBPs/PBEs
Courts/Police
Knowledge Base
Conceptualization
Problem Formulation
Theory/Hypotheses
Research Methods
Sampling Bias
Community Involvement
Public Policy Impact
University Education
Media Portrayals/Stigma
Cultural Competence
Comparative Outcomes
Davis 2009; IOM 2005; HHS 2001
Recommended

















