Renal Failure Renal Failure andand
TreatmentTreatmentVicky Jefferson, RN, CNNVicky Jefferson, RN, CNN
Satellite DialysisSatellite Dialysis

Bones can break, muscles can Bones can break, muscles can atrophy, glands can loaf, even the atrophy, glands can loaf, even the brain can go to sleep without brain can go to sleep without immediate danger to survival. But immediate danger to survival. But -- should kidneys fail.... neither -- should kidneys fail.... neither bone, muscle, nor brain could carry bone, muscle, nor brain could carry on. on.
Homer Homer Smith, Ph.D.Smith, Ph.D.

Renal HemodynamicsRenal Hemodynamics
Renal circulation receives 20 - 25 % Renal circulation receives 20 - 25 % of cardiac output under of cardiac output under normal normal physiologic conditions.physiologic conditions.
The bodies blood volume circulates The bodies blood volume circulates through the kidney every 6 minutes through the kidney every 6 minutes (12 times/hour).(12 times/hour).

Functions of the KidneysFunctions of the Kidneys
Renin secretion Renin secretion and the regulation and the regulation of volume and of volume and composition of composition of extracellular fluid.extracellular fluid.
ExcretionExcretion Blood pressure Blood pressure
controlcontrol
Vitamin D Vitamin D activationactivation
Acid-base balance Acid-base balance regulation. regulation.
Erythropoietin Erythropoietin productionproduction
Urine formationUrine formation

ReninRenin
Renin is important in the regulation of Renin is important in the regulation of blood pressure. blood pressure.
It is released from the granular cells of It is released from the granular cells of the efferent arteriole in response to the efferent arteriole in response to decreased arteriole blood pressure, renal decreased arteriole blood pressure, renal ischemia, extracellular fluid depletion, ischemia, extracellular fluid depletion, increased norepinephrine, and increased increased norepinephrine, and increased urinary Naurinary Na++ concentration. concentration.

Blood Pressure Blood Pressure RegulationRegulation
4 mechanisms are involved4 mechanisms are involved Volume controlVolume control Aldosterone effectAldosterone effect Renin-angiotensin-aldosteroneRenin-angiotensin-aldosterone Renal prostaglandinRenal prostaglandin

ProstaglandinProstaglandin
Prostoglandins (PGs)-Prostoglandins (PGs)- synthesized synthesized by most body tissues. In the kidney, by most body tissues. In the kidney, PGs are synthesized in the medulla and PGs are synthesized in the medulla and have a vasodilating action and promote have a vasodilating action and promote NaNa++ excretion. PGs counteract the excretion. PGs counteract the vasoconstrictor effect of angiotensin vasoconstrictor effect of angiotensin and norepinephrine. Renal PGs and norepinephrine. Renal PGs systemically lower blood pressure by systemically lower blood pressure by decreasing systemic vascular decreasing systemic vascular resistance.resistance.

Vitamin DVitamin D
Acquired by the body through diet or Acquired by the body through diet or through synthesis by ultraviolet through synthesis by ultraviolet radiation on the cholesterol in the radiation on the cholesterol in the skin.skin.
The liver and the kidney make the The liver and the kidney make the vitamin active in the body. vitamin active in the body.

ErythropoietinErythropoietin
Erythropoietin is produced and released Erythropoietin is produced and released by the kidneys in response to decreased by the kidneys in response to decreased oxygen tension in the renal blood supply oxygen tension in the renal blood supply that is created by the loss of red blood that is created by the loss of red blood cells. cells.
Erythropoietin stimulates the production Erythropoietin stimulates the production of RBCs in the bone marrow. of RBCs in the bone marrow.
Erythropoietin deficiency leads to Erythropoietin deficiency leads to anemia in renal failure.anemia in renal failure.

RBC Synthesis & RBC Synthesis & MaturationMaturation
Kidney secrete Erythropoietin, it Kidney secrete Erythropoietin, it stimulates the bone marrow to stimulates the bone marrow to produce RBC’sproduce RBC’s
in oxygen delivery simulates releasein oxygen delivery simulates release in response the RBC count rises in 3 - 5 in response the RBC count rises in 3 - 5
daysdays speeds the maturation of RBC’sspeeds the maturation of RBC’s

Acid Base BalanceAcid Base Balance
Kidneys regulate acid-base balance Kidneys regulate acid-base balance by stabilizing body fluid volume & by stabilizing body fluid volume & flow rate to enhance the flow rate to enhance the reabsorption or excretion of reabsorption or excretion of bicarbonate & hydrogen ionsbicarbonate & hydrogen ions

Electrolyte RegulationElectrolyte Regulation
SodiumSodium PotassiumPotassium CalciumCalcium Need to Know:Need to Know: PhosphatePhosphate Normal ValuesNormal Values MagnesiumMagnesium FunctionsFunctions ChlorideChloride Factors affectFactors affect

Excretion of Metabolic Excretion of Metabolic WasteWaste
Over 200 waste products excretedOver 200 waste products excreted Only 2 are used for clinical Only 2 are used for clinical
assessmentassessment BUNBUN CreatinineCreatinine

Excretion of Metabolic Excretion of Metabolic WasteWaste
Over 200 waste products excretedOver 200 waste products excreted Only 2 are used for clinical Only 2 are used for clinical
assessmentassessment BUNBUN CreatinineCreatinine

BUNBUN
Normal 8 - 20 mg/dlNormal 8 - 20 mg/dl Nitrogenous waste product of Nitrogenous waste product of
protein metabolismprotein metabolism Unreliable in measurement of renal Unreliable in measurement of renal
functionfunction Relevance is assessed in conjunction Relevance is assessed in conjunction
with Creatininewith Creatinine

Factors Affecting BUNFactors Affecting BUN
Urine flowUrine flow low renal perfusionlow renal perfusion Volume depletionVolume depletion Metabolic rateMetabolic rate Protein metabolismProtein metabolism DrugsDrugs

CreatinineCreatinine
A waste product of muscle A waste product of muscle metabolismmetabolism
Normal value 0.6 - 1.2 mg/dlNormal value 0.6 - 1.2 mg/dl 2 times normal = 50% damage 2 times normal = 50% damage 8 times normal = 75% damage8 times normal = 75% damage 10 times normal = 90% damage10 times normal = 90% damage Exception - severe muscular disease Exception - severe muscular disease
can greatly can greatly Creatinine levels Creatinine levels

Diagnostic Tools for Diagnostic Tools for Assessing Renal FailureAssessing Renal Failure
Blood TestsBlood Tests BUN elevated (norm 10-20)BUN elevated (norm 10-20) Creatinine elevated (norm 0.6 - 1.2)Creatinine elevated (norm 0.6 - 1.2) K elevatedK elevated POPO4 4 elevatedelevated Ca decreasedCa decreased
UrinalysisUrinalysis Specific gravitySpecific gravity ProteinProtein Creatinine clearanceCreatinine clearance

Diagnostic ToolsDiagnostic Tools
BiopsyBiopsy UltrasoundUltrasound X-RaysX-Rays

Acute Renal Failure Acute Renal Failure (ARF)(ARF)
Sudden onset - hours to daysSudden onset - hours to days Often reversibleOften reversible Severe - 50% mortality rate overall; Severe - 50% mortality rate overall;
generally related to infectiongenerally related to infection. .
Characteristics of ARFCharacteristics of ARF
Homeostatic functions affected mostHomeostatic functions affected most Electrolyte imbalancesElectrolyte imbalances Volume regulationVolume regulation Blood pressure controlBlood pressure control
Endocrine functions affected leaseEndocrine functions affected lease Require time to evolveRequire time to evolve
Renal size is preservedRenal size is preserved Evidence of acute illness or insult Evidence of acute illness or insult
existsexists

Acute Renal Failure Acute Renal Failure (ARF)(ARF)
Sudden fall in glomerular filtration Sudden fall in glomerular filtration rate (GFR)rate (GFR) Retention of nitrogenous (BUN and Retention of nitrogenous (BUN and
creatinine) and other wastescreatinine) and other wastes Hours to daysHours to days
About 5% of all hospitalizationsAbout 5% of all hospitalizations About 20% of ICU admissionsAbout 20% of ICU admissions
Mortality 50 – 80%Mortality 50 – 80% Independent risk factor for death – 5x Independent risk factor for death – 5x
increase riskincrease risk

Chronic Renal FailureChronic Renal Failure
Slow progressive renal disorder Slow progressive renal disorder related to nephron loss, occurring related to nephron loss, occurring over months to yearsover months to years
Culminates in End Stage Renal Culminates in End Stage Renal DiseaseDisease

Characteristics of Characteristics of Chronic Renal FailureChronic Renal Failure
Cause & onset often unknownCause & onset often unknown Loss of function precedes lab Loss of function precedes lab
abnormalitiesabnormalities Lab abnormalities precede Lab abnormalities precede
symptomssymptoms Symptoms (usually) evolve in orderly Symptoms (usually) evolve in orderly
sequencesequence Renal size is usually decreasedRenal size is usually decreased

Causes of Chronic Renal Causes of Chronic Renal FailureFailure
DiabetesDiabetes HypertensionHypertension GlomerulonephritisGlomerulonephritis Cystic disordersCystic disorders Developmental - CongenitalDevelopmental - Congenital Infectious DiseaseInfectious Disease

Causes of Chronic Renal Causes of Chronic Renal Failure Failure
NeoplasmsNeoplasms Obstructive disordersObstructive disorders Autoimmune diseasesAutoimmune diseases
Lupus Lupus Hepatorenal failureHepatorenal failure SclerodermaScleroderma AmyloidosisAmyloidosis Drug toxicityDrug toxicity

Glomerular Filtration RateGlomerular Filtration RateGFRGFR
24 hour urine for creatinine 24 hour urine for creatinine clearanceclearance
Can estimate creatinine clearance Can estimate creatinine clearance by:by:
140 – {age x weight (kg)}140 – {age x weight (kg)}
72 x serum creatinine72 x serum creatinine

Stages of Chronic Renal Stages of Chronic Renal FailureFailure
Old SystemOld System Reduced Renal ReserveReduced Renal Reserve
Renal InsufficiencyRenal Insufficiency
End Stage Renal Disease (ESRD)End Stage Renal Disease (ESRD)

Stages of Chronic Renal Stages of Chronic Renal FailureFailure
NKF Classification SystemNKF Classification System
Stage 1: Stage 1: GFR > 90 ml/min despite GFR > 90 ml/min despite kidney kidney damagedamage

Stages of Chronic Renal Stages of Chronic Renal FailureFailure
NKF Classification SystemNKF Classification SystemStage 2:Stage 2: Mild reduction (GFR 60 – Mild reduction (GFR 60 –
89 89 ml/min)ml/min)
1. GFR of 60 may represent 1. GFR of 60 may represent 50% 50% loss in loss in function.function.
2. Parathyroid hormones 2. Parathyroid hormones starts to starts to increase. increase.
During Stage 1 - 2During Stage 1 - 2
No symptomsNo symptoms
Serum creatinine doublesSerum creatinine doubles
Up to 50% nephron lossUp to 50% nephron loss

Stages of Chronic Renal Stages of Chronic Renal FailureFailure
NKF Classification SystemNKF Classification SystemStage 3:Stage 3: Moderate reduction (GFR Moderate reduction (GFR
30 – 59 30 – 59 ml/min)ml/min)1. Calcium absorption 1. Calcium absorption
decreasesdecreases
2. Malnutrition onset2. Malnutrition onset
3. Anemia secondary to 3. Anemia secondary to Erythropoietin Erythropoietin deficiency deficiency
4. Left ventricular 4. Left ventricular hypertrophyhypertrophy
Stages of Chronic Renal Stages of Chronic Renal FailureFailure
NKF Classification SystemNKF Classification SystemStage 4:Stage 4: Sever reduction (GFR 15 – Sever reduction (GFR 15 –
29 29 ml/min)ml/min)
1. Serum triglycerides 1. Serum triglycerides increaseincrease
2. Hyperphosphatemia2. Hyperphosphatemia
3. Metabolic acidosis3. Metabolic acidosis
4. Hyperkalemia4. Hyperkalemia

During Stage 3 - 4During Stage 3 - 4
Signs and symptoms worsen if Signs and symptoms worsen if kidneys are stressedkidneys are stressed
Decreased ability to maintain Decreased ability to maintain homeostasishomeostasis

During stages 3 - 4During stages 3 - 4
75% nephron loss 75% nephron loss Decreased: glomerular filtration Decreased: glomerular filtration
rate, solute clearance, ability to rate, solute clearance, ability to concentrate urine and hormone concentrate urine and hormone secretionsecretion
Symptoms: elevated BUN & Symptoms: elevated BUN & Creatinine, mild azotemia, anemiaCreatinine, mild azotemia, anemia

Stages of Chronic Renal Stages of Chronic Renal FailureFailure
NKF Classification SystemNKF Classification System
Stage 5:Stage 5: Kidney failure (GFR < 15 Kidney failure (GFR < 15 ml/min)ml/min)
1. Azotemia1. Azotemia

During Stage 5During Stage 5
Residual function < 15% of normalResidual function < 15% of normal Excretory, regulatory and hormonal Excretory, regulatory and hormonal
functions severely impaired. functions severely impaired. metabolic acidosismetabolic acidosis Marked increase in: BUN, Marked increase in: BUN,
Creatinine, PhosphorousCreatinine, Phosphorous Marked decrease in: Hemoglobin, Marked decrease in: Hemoglobin,
Hematocrit, CalciumHematocrit, Calcium Fluid overloadFluid overload

During Stage 5During Stage 5
Uremic syndrome develops affecting Uremic syndrome develops affecting all body systemsall body systems can be diminished with early diagnosis can be diminished with early diagnosis
& treatment& treatment
Last stage of progressive CRFLast stage of progressive CRF Fatal if no treatmentFatal if no treatment

What happens when the What happens when the kidneys don’t function kidneys don’t function
correctly?correctly?

Manifestations of CRF -Manifestations of CRF -Nervous SystemNervous System
Mood swingsMood swings Impaired judgmentImpaired judgment Inability to concentrate and perform Inability to concentrate and perform
simple math functionssimple math functions Tremors, twitching, convulsionsTremors, twitching, convulsions Peripheral NeuropathyPeripheral Neuropathy
restless legsrestless legs foot dropfoot drop

Manifestations of CRFManifestations of CRFSkinSkin
Pale, grayish-bronze colorPale, grayish-bronze color Dry scalyDry scaly Severe itchingSevere itching Bruise easilyBruise easily Uremic frostUremic frost

Manifestations of CRFManifestations of CRFEyesEyes
Visual blurringVisual blurring Occasional blindnessOccasional blindness
Manifestations of CRF Manifestations of CRF Fluid - Electrolyte - pHFluid - Electrolyte - pH
Volume expansion and fluid overloadVolume expansion and fluid overload Metabolic AcidosisMetabolic Acidosis Electrolyte ImbalancesElectrolyte Imbalances
HyperkalemiaHyperkalemia

Manifestations of CRFManifestations of CRFGI TractGI Tract
Uremic fetorUremic fetor Anorexia, nausea, vomitingAnorexia, nausea, vomiting GI bleedingGI bleeding

Manifestations of CRF Manifestations of CRF HematologicHematologic
AnemiaAnemia Platelet dysfunctionPlatelet dysfunction

Manifestations of CRF Manifestations of CRF MusculoskeletalMusculoskeletal
Muscle crampsMuscle cramps Soft tissue calcificationsSoft tissue calcifications WeaknessWeakness Related to calcium phosphorous Related to calcium phosphorous
imbalancesimbalances
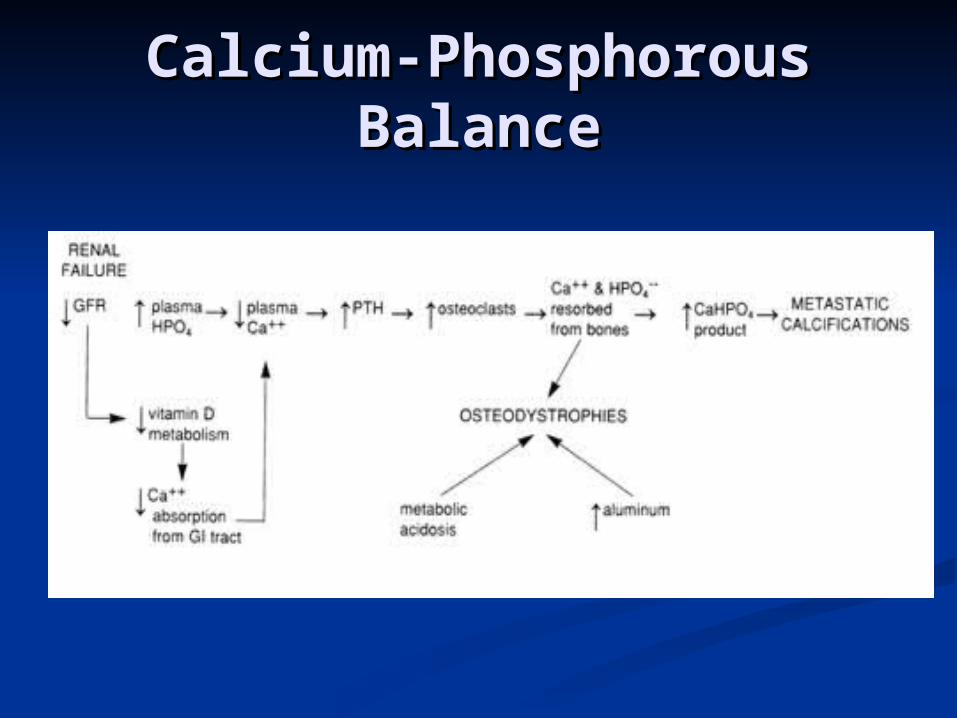
Calcium-Phosphorous Calcium-Phosphorous BalanceBalance
Manifestations of CRFManifestations of CRFHeart - LungsHeart - Lungs
HypertensionHypertension Congestive heart failureCongestive heart failure PericarditisPericarditis Pulmonary edemaPulmonary edema Pleural effusionsPleural effusions

Manifestations of CRF Manifestations of CRF Endocrine - MetabolicEndocrine - Metabolic
Erythropoietin production decreasedErythropoietin production decreased HypothyroidismHypothyroidism Insulin resistanceInsulin resistance Growth hormone decreasedGrowth hormone decreased Gonadal dysfunctionGonadal dysfunction Parathyroid hormone and Vitamin DParathyroid hormone and Vitamin D33
HyperlipidemiaHyperlipidemia

Treatment OptionsTreatment Options
HemodialysisHemodialysis Peritoneal DialysisPeritoneal Dialysis TransplantTransplant NothingNothing
HemodialysisHemodialysis
Removal of soluble substances Removal of soluble substances and and water from the blood by water from the blood by diffusion diffusion through a semi-through a semi-permeable membrane. permeable membrane.

HistoryHistory
Early animal experiments began Early animal experiments began 19131913
1st human dialysis 1940 by Dutch 1st human dialysis 1940 by Dutch physician Willem Kolff (2 of 17 physician Willem Kolff (2 of 17 patients survived)patients survived)
Considered experimental through Considered experimental through 1950’s, No intermittent blood 1950’s, No intermittent blood access; for acute renal failure only. access; for acute renal failure only.

History cont’dHistory cont’d
1960 Dr. Scribner developed 1960 Dr. Scribner developed Scribner ShuntScribner Shunt
1960’s Machines expensive, scarce, 1960’s Machines expensive, scarce, no funding.no funding.
““Death Panels” panels within Death Panels” panels within community decided who got to community decided who got to dialyze.dialyze.

Hemodialysis ProcessHemodialysis Process
Blood removed from patient into the Blood removed from patient into the extracorporeal circuit. extracorporeal circuit.
Diffusion and ultrafiltration take Diffusion and ultrafiltration take place in the dialyzer. place in the dialyzer.
Cleaned blood returned to patient. Cleaned blood returned to patient.

Extracorporeal CircuitExtracorporeal Circuit

How Hemodialysis How Hemodialysis WorksWorks
Vascular AccessVascular Access
Arterio-venous shunt (Scribner Arterio-venous shunt (Scribner External Shunt)External Shunt)
Arterio-venous (AV) FistulaArterio-venous (AV) Fistula PTFE GraftPTFE Graft Temporary cathetersTemporary catheters ““Permanent” cathetersPermanent” catheters

Scribner ShuntScribner Shunt
External- one end External- one end into artery, one into into artery, one into vein. vein.
AdvantagesAdvantages place at bedsideplace at bedside use immediatelyuse immediately
DisadvantagesDisadvantages infectioninfection skin erosionskin erosion accidental separation accidental separation limits use of limits use of
extremityextremity

Arterio-venous (AV) Arterio-venous (AV) FistulaFistula
Primary FistulaPrimary Fistula Patients own artery and vein surgically Patients own artery and vein surgically
anastomosed.anastomosed. AdvantagesAdvantages
patients own veinpatients own vein longevitylongevity low infection and thrombosis rateslow infection and thrombosis rates
DisadvantagesDisadvantages long time to mature, 1- 6 monthslong time to mature, 1- 6 months ““steal” syndromesteal” syndrome requires needle sticksrequires needle sticks

PTFE PTFE (Polytetraflourethylene) (Polytetraflourethylene)
GraftGraft Synthetic “vessel” anastomosed into an artery and Synthetic “vessel” anastomosed into an artery and
vein.vein. AdvantagesAdvantages
for people with inadequate vesselsfor people with inadequate vessels can be used in 7-14 dayscan be used in 7-14 days prominent vesselsprominent vessels
DisadvantagesDisadvantages clots easilyclots easily ““steal” syndrome more frequentsteal” syndrome more frequent requires needle sticksrequires needle sticks infection may necessitate removal of graftinfection may necessitate removal of graft

Temporary CathetersTemporary Catheters
Dual lumen catheter placed into a central Dual lumen catheter placed into a central vein-subclavian, jugular or femoral.vein-subclavian, jugular or femoral.
AdvantagesAdvantages immediate useimmediate use no needle sticksno needle sticks
DisadvantagesDisadvantages high incidence of infectionhigh incidence of infection subclavian vein stenosissubclavian vein stenosis poor flow-inadequate dialysispoor flow-inadequate dialysis clottingclotting

Cuffed Tunneled Cuffed Tunneled CathetersCatheters
Dual lumen catheter with Dacron Dual lumen catheter with Dacron cuff surgically tunneled into cuff surgically tunneled into subclavian, jugular or femoral subclavian, jugular or femoral vein.vein.
AdvantagesAdvantages immediate useimmediate use can be used for patients that can be used for patients that
can have no other permanent can have no other permanent accessaccess
no needle sticksno needle sticks DisadvantagesDisadvantages
high incidence of infectionhigh incidence of infection poor flows result in inadequate poor flows result in inadequate
dialysisdialysis clottingclotting

Care of Vascular AccessCare of Vascular Access
NONO BP’s, needle sticks to arm with BP’s, needle sticks to arm with vascular access. This includes finger vascular access. This includes finger sticks.sticks.
Place ID bands on other arm Place ID bands on other arm whenever possible.whenever possible.
Palpate thrill and listen for bruit.Palpate thrill and listen for bruit. Teach patient nothing constrictive, Teach patient nothing constrictive,
feel for thrill.feel for thrill.
Complications of Complications of HemodialysisHemodialysis
During dialysisDuring dialysis Fluid and electrolyte related Fluid and electrolyte related
hypotensionhypotension CardiovascularCardiovascular
arrythmiasarrythmias Associated with the extracorporeal circuitAssociated with the extracorporeal circuit
exsanguinationexsanguination NeurologicNeurologic
seizuresseizures otherother
feverfever

Complications of Complications of Hemodialysis cont’dHemodialysis cont’d
Between treatmentsBetween treatments Hypertension/HypotensionHypertension/Hypotension EdemaEdema Pulmonary edemaPulmonary edema HyperkalemiaHyperkalemia BleedingBleeding Clotting of accessClotting of access
Complications of Complications of Hemodialysis cont’dHemodialysis cont’d
Long termLong term MetabolicMetabolic
hyperparathyroidismhyperparathyroidism diabetic complicationsdiabetic complications
CardiovascularCardiovascular CHFCHF AV access failureAV access failure
RespiratoryRespiratory pulmonary edemapulmonary edema
NeuromuscularNeuromuscular neuropathyneuropathy

Complications of Complications of HemodialysisHemodialysis
cont’dcont’d Long term cont’dLong term cont’d
HematologicHematologic anemiaanemia
GIGI bleedingbleeding
dermatologicdermatologic calcium phosphorous depositscalcium phosphorous deposits
RheumatologicRheumatologic amyloid depositsamyloid deposits

Complications of Complications of Hemodialysis cont’dHemodialysis cont’d
Long term cont’dLong term cont’d GenitourinaryGenitourinary
infectioninfection sexual dysfunctionsexual dysfunction
PsychiatricPsychiatric depressiondepression
InfectionInfection bloodborne pathogensbloodborne pathogens

Dietary Restrictions on Dietary Restrictions on HemodialysisHemodialysis
Fluid restrictionsFluid restrictions Phosphorous restrictionsPhosphorous restrictions Potassium restrictionsPotassium restrictions Sodium restrictionsSodium restrictions Protein to maintain nitrogen balanceProtein to maintain nitrogen balance
too high - waste productstoo high - waste products too low - decreased albumin, increased too low - decreased albumin, increased
mortalitymortality Calories to maintain or reach ideal weightCalories to maintain or reach ideal weight
Peritoneal DialysisPeritoneal Dialysis
Removal of soluble substances and Removal of soluble substances and water from the blood by diffusion water from the blood by diffusion through a semi-permeable through a semi-permeable membrane that is intracorporeal membrane that is intracorporeal (inside the body).(inside the body).

Types of Peritoneal Types of Peritoneal DialysisDialysis
CAPD: CAPD: Continuous ambulatory peritoneal Continuous ambulatory peritoneal dialysisdialysis
CCPDCCPD: Continuous cycling peritoneal : Continuous cycling peritoneal dialysisdialysis
IPD: IPD: Intermittent peritoneal dialysisIntermittent peritoneal dialysis

CAPDCAPD
Catheter into peritoneal cavityCatheter into peritoneal cavity Exchanges 4 - 5 times per dayExchanges 4 - 5 times per day Treatment 24 hours; 7 days a weekTreatment 24 hours; 7 days a week Solution remains in peritoneal cavity Solution remains in peritoneal cavity
except during drain timeexcept during drain time Independent treatmentIndependent treatment


Phases of A Peritoneal Phases of A Peritoneal Dialysis ExchangeDialysis Exchange
Fill: fluid infused into peritoneal Fill: fluid infused into peritoneal cavitycavity
Dwell: time fluid remains in Dwell: time fluid remains in peritoneal cavityperitoneal cavity
Drain: time fluid drains from Drain: time fluid drains from peritoneal cavityperitoneal cavity

Complications of Complications of Peritoneal DialysisPeritoneal Dialysis
InfectionInfection peritonitisperitonitis tunnel infectionstunnel infections catheter exit site catheter exit site
HypervolemiaHypervolemia hypertensionhypertension pulmonary edemapulmonary edema
HypovolemiaHypovolemia hypotensionhypotension
HyperglycemiaHyperglycemia MalnutritionMalnutrition

Complications of Complications of Peritoneal Dialysis cont’dPeritoneal Dialysis cont’d ObesityObesity HypokalemiaHypokalemia HerniaHernia Cuff erosionCuff erosion

Advantages of CAPDAdvantages of CAPD
Independence for patientIndependence for patient No needle sticksNo needle sticks Better blood pressure controlBetter blood pressure control Some diabetics add insulin to solutionSome diabetics add insulin to solution Fewer dietary restrictionsFewer dietary restrictions
protein loses in dialysateprotein loses in dialysate generally need increased potassiumgenerally need increased potassium less fluid restrictionsless fluid restrictions

Peritoneal Catheter Exit Peritoneal Catheter Exit SiteSite


Medications Common to Medications Common to Dialysis PatientsDialysis Patients
Vitamins - water solubleVitamins - water soluble Phosphate binder - (Phoslo, Renagel, Phosphate binder - (Phoslo, Renagel,
Calcium, Aluminum hydroxide) Give Calcium, Aluminum hydroxide) Give with mealswith meals
Iron Supplements - don’t give with Iron Supplements - don’t give with phosphate binder or calciumphosphate binder or calcium
Antihypertensives - hold prior to Antihypertensives - hold prior to dialysisdialysis

Medications Common to Medications Common to Dialysis Patients cont’dDialysis Patients cont’d
ErythropoietinErythropoietin Calcium Supplements - Calcium Supplements - BetweenBetween
meals, meals, notnot with iron with iron Activated Vitamin DActivated Vitamin D3 3 - aids in - aids in
calcium absorptioncalcium absorption Antibiotics - hold dose prior to Antibiotics - hold dose prior to
dialysis if it dialyzes outdialysis if it dialyzes out

MedicationsMedications
Many drugs or their metabolites are Many drugs or their metabolites are excreted by the kidneyexcreted by the kidney
Dosages - many change when used Dosages - many change when used in renal failure patientsin renal failure patients
Dialyzability - many removed by Dialyzability - many removed by dialysis varies between HD and PDdialysis varies between HD and PD

Patient EducationPatient Education
Alleviate fearAlleviate fear Dialysis processDialysis process Fistula/catheter careFistula/catheter care Diet and fluid restrictionsDiet and fluid restrictions MedicationMedication Diabetic teachingDiabetic teaching

Case StudyCase Study
A 48 year old female with a history of A 48 year old female with a history of uncontrolled diabetes presents to uncontrolled diabetes presents to the ER. Her chief complaints are the ER. Her chief complaints are nausea, vomiting and fatigue.nausea, vomiting and fatigue.
Lab: Lab: BUN 100; Creatinine 10; H&H BUN 100; Creatinine 10; H&H 7.0/21.4; 7.0/21.4;
KK+ + 6.0, PO 6.0, PO4 4 5.5; Ca5.5; Ca++ ++ 7.57.5
What do you suspect? How would she What do you suspect? How would she possibly be treated?possibly be treated?

TransplantationTransplantation
TreatmentTreatment not not curecure

Kidney Awaiting Kidney Awaiting TransplantTransplant


Transplanted KidneyTransplanted Kidney

AdvantagesAdvantages
Restoration of “normal” renal Restoration of “normal” renal functionfunction
Freedom from dialysisFreedom from dialysis Return to “normal” lifeReturn to “normal” life

DisadvantagesDisadvantages
Life long medicationsLife long medications Multiple side effects from Multiple side effects from
medicationmedication Increased risk of tumorIncreased risk of tumor Increased risk of infectionIncreased risk of infection Major surgeryMajor surgery

Care of the RecipientCare of the Recipient
Major surgery with general Major surgery with general anesthesiaanesthesia
Assessment of renal functionAssessment of renal function Assessment of fluid and electrolyte Assessment of fluid and electrolyte
balancebalance Prevention of infectionPrevention of infection Prevention and management of Prevention and management of
rejectionrejection

FunctionFunction
ATN? (acute tubular necrosis) ATN? (acute tubular necrosis) 50% experience50% experience
Urine output >100 <500 cc/hrUrine output >100 <500 cc/hr BUN, creatinine, creatinine clearanceBUN, creatinine, creatinine clearance Fluid BalanceFluid Balance UltrasoundUltrasound Renal scansRenal scans Renal biopsyRenal biopsy

Fluid & Electrolyte Fluid & Electrolyte BalanceBalance
Accurate I & OAccurate I & O CRITICAL TO AVOID DEHYDRATIONCRITICAL TO AVOID DEHYDRATION Output normal - >100 <500 cc/hr, could Output normal - >100 <500 cc/hr, could
be 1-2 L/hrbe 1-2 L/hr Potential for volume overload/deficitPotential for volume overload/deficit
Daily weightsDaily weights Hyper/Hypokalemia potentialHyper/Hypokalemia potential HyponatremiaHyponatremia HyperglycemiaHyperglycemia

Prevention of InfectionPrevention of Infection
Major complication of Major complication of transplantation due to transplantation due to immunosuppressionimmunosuppression
HANDWASHINGHANDWASHING Crowds, KidsCrowds, Kids Patient EducationPatient Education

RejectionRejection
Hyperacute - preformed antibodies Hyperacute - preformed antibodies to donor antigento donor antigen function ceases within 24 hoursfunction ceases within 24 hours Rx = removalRx = removal
Accelerated - same as hyperacute Accelerated - same as hyperacute but slower, 1st week to monthbut slower, 1st week to month Rx = removalRx = removal

Rejection cont’dRejection cont’d
Acute - generally after 1st 10 days to Acute - generally after 1st 10 days to end of 2nd monthend of 2nd month 50% experience50% experience must differentiate between rejection must differentiate between rejection
and cyclosporine toxicityand cyclosporine toxicity Rx = steroids, monoclonal (OKTRx = steroids, monoclonal (OKT33), or ), or
polyclonal (HTG) antibodiespolyclonal (HTG) antibodies

Rejection cont’dRejection cont’d
Chronic - gradual process of graft Chronic - gradual process of graft dysfunctiondysfunction Repeated rejection episodes that have Repeated rejection episodes that have
not been completely resolved with not been completely resolved with treatmenttreatment
Rx = return to dialysis or re-Rx = return to dialysis or re-transplantationtransplantation
Immunosuppressant Immunosuppressant DrugsDrugs
PrednisonePrednisone Prevents infiltration of T lymphocytesPrevents infiltration of T lymphocytes
Side effectsSide effects cushnoid changescushnoid changes Avascular NecrosisAvascular Necrosis GI disturbancesGI disturbances DiabetesDiabetes infectioninfection risk of tumorrisk of tumor

Immunosuppressant Immunosuppressant Drugs cont’dDrugs cont’d
Azathioprine (Imuran)Azathioprine (Imuran) Prevents rapid growing lymphocytesPrevents rapid growing lymphocytes
Side EffectsSide Effects bone marrow toxicitybone marrow toxicity hepatotoxicityhepatotoxicity hair losshair loss infectioninfection risk of tumorrisk of tumor

Immunosuppressant Immunosuppressant Drugs cont’dDrugs cont’d
CyclosporinCyclosporin Interferes with production of Interferes with production of
interleukin 2 which is necessary for interleukin 2 which is necessary for growth and activation of T lymphocytes.growth and activation of T lymphocytes.
• Side EffectsSide Effects– NephrotoxicityNephrotoxicity– HTNHTN– HepatotoxicityHepatotoxicity– Gingival hyperplasiaGingival hyperplasia– InfectionInfection

Immunosuppressant Immunosuppressant Drugs cont’dDrugs cont’d
Cytoxan - in place of Imuran less Cytoxan - in place of Imuran less toxictoxic
FK506 - 100 x more potent than FK506 - 100 x more potent than CyclosporinCyclosporin
PrografPrograf CellceptCellcept

Immunosuppressant Immunosuppressant Drugs cont’dDrugs cont’d
OKTOKT33 - monoclonal antibody used to treat rejection - monoclonal antibody used to treat rejection or induce immunosuppressionor induce immunosuppression decreases CDdecreases CD3 3 cells within 1 hour cells within 1 hour
Side effectsSide effects anaphylaxisanaphylaxis fever/chillsfever/chills pulmonary edemapulmonary edema risk of infectionrisk of infection tumorstumors
1st dose reaction expected & wanted, pre-treat 1st dose reaction expected & wanted, pre-treat with Benadryl, Tylenol, Solumedrolwith Benadryl, Tylenol, Solumedrol

Immunosuppressant Immunosuppressant Drugs cont’dDrugs cont’d
Atgam - polyclonal antibody used to treat Atgam - polyclonal antibody used to treat rejection or induce immunosuppressionrejection or induce immunosuppression decreased number of T lymphocytesdecreased number of T lymphocytes
Side effectsSide effects anaphylaxisanaphylaxis fever chillsfever chills leukopenialeukopenia thrombocytopeniathrombocytopenia risk of infectionrisk of infection tumortumor

Patient EducationPatient Education
Signs of infectionSigns of infection Prevention of infectionPrevention of infection Signs of rejectionSigns of rejection
decreased urine outputdecreased urine output increased weight gainincreased weight gain tenderness over kidneytenderness over kidney fever > 100 degrees Ffever > 100 degrees F
MedicationsMedications time, dose, side effectstime, dose, side effects
Recommended