DR.RANVIR SAACHIN
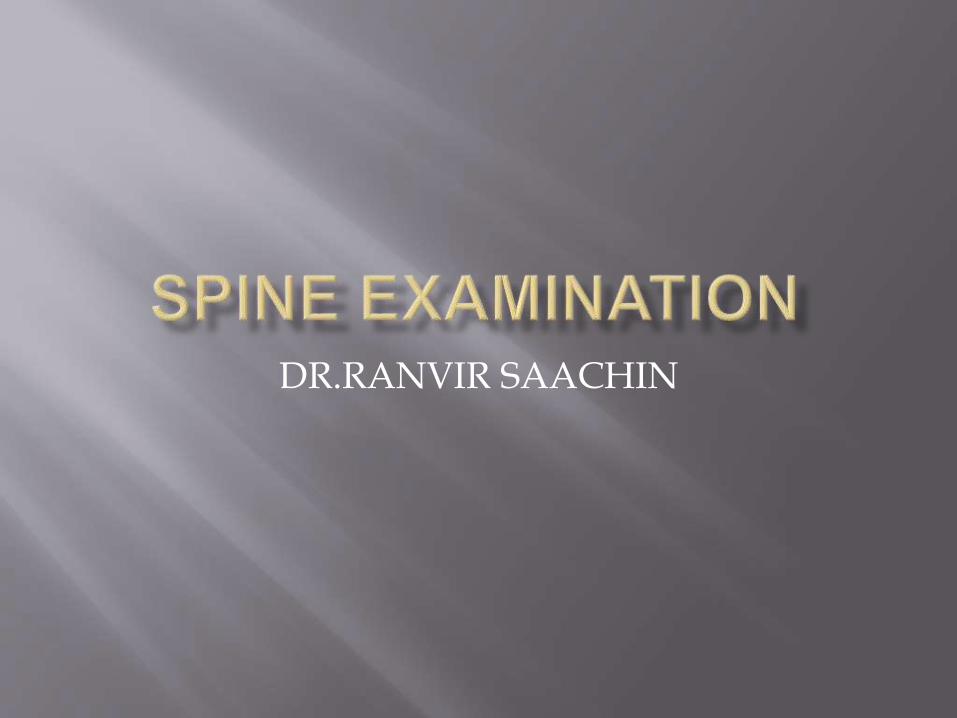
Basic Vertebral Structures
Cervical Thoracic Lumbar
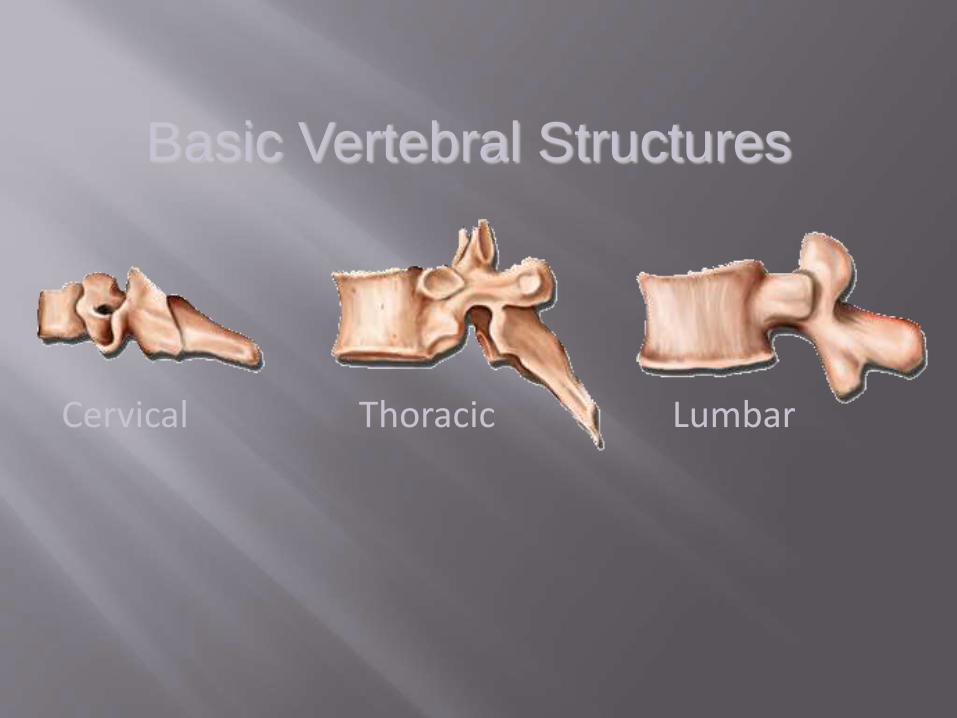
Cervical Lordosis 20°- 40°
Sacral Kyphosis
Lumbar Lordosis 30°- 50°
Thoracic Kyphosis 20°- 40°
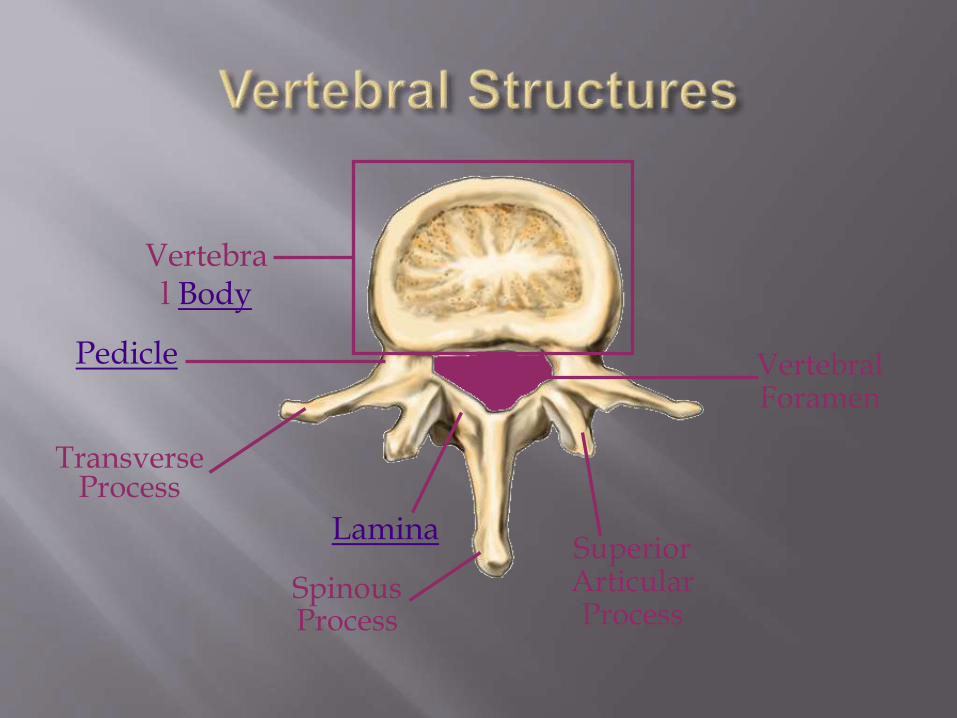
Vertebral Body
Pedicle
LaminaSuperior Articular Process
SpinousProcess
Transverse Process
Vertebral Foramen
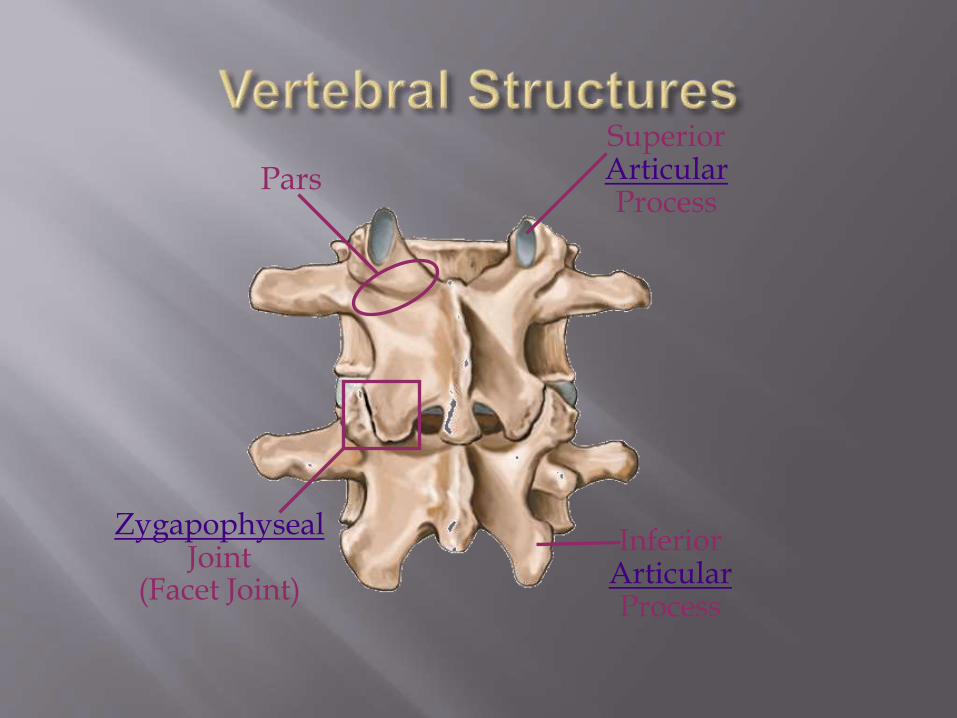
Superior ArticularProcess
Inferior ArticularProcess
ZygapophysealJoint
(Facet Joint)
Pars
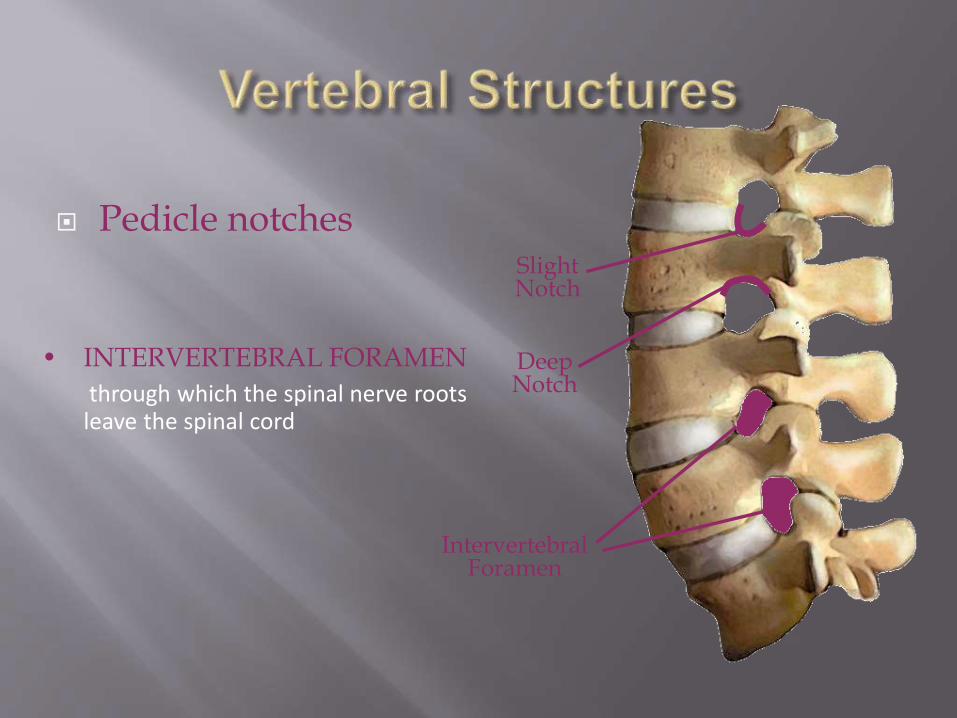
Pedicle notchesSlight Notch
Deep Notch
Intervertebral Foramen
• INTERVERTEBRAL FORAMEN
through which the spinal nerve roots leave the spinal cord

1. GAIT
NORMAL WALKING
WALKING ON TIP TOES – S1 WEAKNESS
WALKING ON HEELS - L5 WEAKNESS
(A) Look From Side
Normal spine
> cervical lordosis
> thoracic kyphosis
> lumbar lordosis
2.Increased kyphosis (posterior convexity of
the spine)
> senile kyphosis (with osteoporosis,
osteomalacia or pathological fracture)
> Scheuermann’s disease (osteochondritis
involving one or more of the vertebrae)
> ankylosing spondylitis
iii. Gibbus (angular kyphosis)
> fracture
> tuberculosis of the spine
> congenital abnormality
iv. Lumbar curvature
> flattening or reversal of lumbar lordosis :
- prolapsed intervertebral disc
- osteoarthritis of the spine
- infection of vertebral bodies
- ankylosing spondylitis
> increase in lumbar lordosis
- may be normal (esp. in women)
- spondylolisthesis
- secondary to increased thoracic curvature
or to flexion deformity of the hips
(b) Look from behind
i. listing of trunk (due to muscle spasm)
ii. Scoliosis (lateral curvature of spine)
- postural : scoliosis disappears with
forward flexion of the spine
- structural : scoliosis persists with forward
flexion of the spine and a rib hump
presents
iii. Shoulder tilt
iv. Pelvic tilt
v. Skin changes over the spine
- hair tuft (spina bifida)
- sinus
- colour changes or pigmentation (neurofibroma)
- scar
vi. Swelling
vii. Prominent crease of the trunk
viii. Wasting of glutei, hamstrings and calf muscles
along the spinous process, looking for
tenderness
paravertebral muscle spasm
sacro-iliac joint tenderness
step deformity (spondylolisthesis)
- Slide the fingers down the lumbar spine on to the
sacrum
- A palpable step at the lumbo-sacral junction
Thoracic and Lumbar spine
Flexion
- ask the patient to try to touch his toes
- watch the spine for smoothness of movement and any areas of restriction
- patients with advanced ankylosing spondylitishave a flat ankylosed spine and all the bending occur at the hips
Lumbar spine excursion test (Schober’s
method)
- Mark 2 points 10cm apart at the midline of
lumbar spine
- Anchor the top of the tape with a finger and ask
the patient to flex as far as he can
- Measure the increase in the distance between
the 2 points which indicate lumbar excursion
- Normal excursion = 5 cm or more
2. Extension
- ask the patient to arch his back
- assist him by steadying the pelvis and pulling
back on the shoulder
- normal : 30
3. Lateral flexion
- ask the patient to slide the hands down the side of each leg in turn
- record the point reached from the floor or
- measure the angle
- normal : 30-45°
4. Rotation
- patient seated to fix the pelvis or pelvis fixed
by examiner
- ask the patient to twist round to each side
- normal : 45°
UPPER LIMB
1. Tone
2. Power
3. Reflexs
4. Sensation
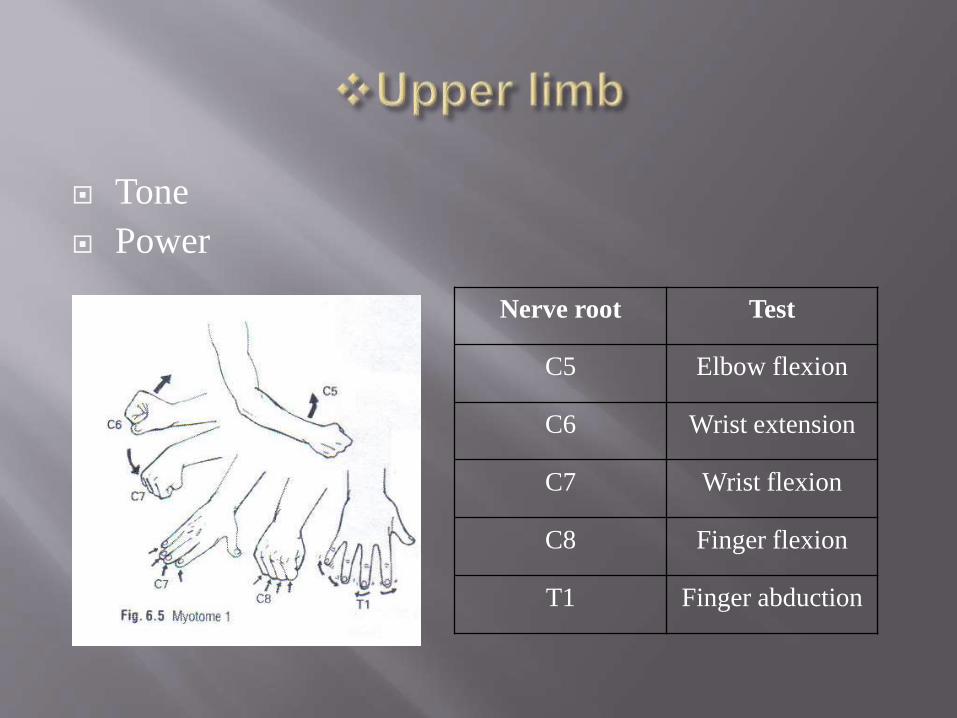
Tone
Power
Nerve root Test
C5 Elbow flexion
C6 Wrist extension
C7 Wrist flexion
C8 Finger flexion
T1 Finger abduction
1. Tone
Hypertonia - UMNL
Hypotonia - LMNL
2. Power
i. Shoulder
- abduction : C5,C6
- adduction : C6,C7,C8
ii. Elbow
- flexion : C5,C6
- extension : C7,C8
iii. Wrist
- flexion : C6,C7
- extension : C7,C8
iv. Fingers
- flexion : C7,C8
- extension : C7,C8
- abduction : C8,T1
- adduction : C8,T1
3. Reflex
- biceps jerk : C5,C6
- triceps jerk : C7,C8
- brachioradialis (supinator) jerk : C5,C6
4. Sensation
C5 – lateral arm
C6 – lateral forearm
- thumb & index finger
C7 – middle finger
C8 – ring&little finger
T1 – medial arm
LOWER LIMB
1. Tone
hypertonia : UMNL
normotonia
hypotonia : LMNL
Power i. Hip
- flexion : L2,L3
- extension : L5,S1,S2
- abduction : L4,L5,S1
- adduction : L2,L3,L4
ii. Knee
- flexion : L5,S1
- extension : L3,L4
iii. Ankle
- plantar flexion : S1,S2
- dorsiflexion : L4,L5
iv. Tarsal joint
- eversion : L5,S1
- inversion : L5,S1
3. Reflex
- knee jerk : L3,L4
- ankle jerk : S1,S2
- plantar reflex : L5,S1,S2
1. Straight leg raising test
- do on normal limb 1st
- raise the leg from the couch with the knee extended until the patient experiences pain (over the back & may radiate to the lower limb)
- Distribution of the pain indicating the involved nerve root
- Positive if the angle < 60°
- Cross sciatic tension : severe root irritation(pain on the affected side when raising the unaffected
leg)
2. Sciatic Stretch Test
- Following SLR test
- Drop the limb about 10° to relieve tension on
the irritated nerve root
- Dorsiflex the ankle to reproduce the same pain
3. Femoral Stretch Test
- For lumbar root sensitivity
- Patient should be prone
- Flex the patient’s knee and lift the hip into
extension
- Pain may be felt in front of the thigh and in the
back
Bowstring Test
Subject begins supine with legs extended Examiner performs a passive straight leg raise on the involved side If radiating pain is reported, the examiner then flexes the subjects knee until symptoms are reduced The examiner then applies pressure to the poplitealarea in attempt to reproduce the radicular pain
Pelvic rock test
Compress pelvis to midline- +ve if pain in SI joint
Gaenslens sign
Supine, patient draws both knees up to chest, then shift patient to side of couch so one buttock extends over edge. Allow unsupported leg to drop over edge while opposite leg remains drawn up to chest- +ve if pain in SI joint
Faber test(Flexion, abduction external rotation)
supine, place foot of involved side on opposite knee ( fig 4 position). To stress SI joint press down on knee with one hand & press down on opposite ASIS with the other hand
Examination of other joints
Rectal examination
THANK YOU
Recommended