State Innovation Model (SIM) Grant Payer’s Working Session
May 27, 2015Beth A. Bortz | President & CEO

Provides financial and technical support for the development and testing of state-led, multi-payer health care payment and service delivery models.
States could seek a model design (up to $3M) or model testing (up to $100M) grant. Preference was given to states that had expanded Medicaid.
Virginia received a $2.6M Design Grant.
About SIM

LG’s Roundtable and Core Sets of Population Health and Quality Metrics
Accountable Care Communities
Delivery System Reform Incentive Payment (DSRIP) Program
In all, we are looking to focus Virginia’s measurement efforts and substantively move the needle on performance. Health plans are already working to do this with pay for performance. We need to work together.
Update on Key Components of SIM for Virginia’s Health Plans

The Lieutenant Governor’s Quality, Payment Reform, and HIT Roundtable (QPHR) is asked to pursue the following objectives in support of VHIP 2015:
Develop an aligned set of quality measures that reflect needed improvements in care coordination and population health;
Recommend an aligned set of payment reforms to better incentivize clinicians for reaching selected quality measure targets; and
Develop a Health Information Technology plan that ensures the data collection systems are in place to implement the aligned measurement and payment functions.
Additionally, VDH is preparing a core set of population health measures for Virginia’s Plan for Well-Being. We will work to align these two sets of measures.
LG’s Roundtable: Purpose

Agreed Upon Framework for Quality, Payment Reform, and HIT in Virginia
• Population Health and Well-Being Focus. Improvements in quality would inform and advance Virginia’s efforts to continuously measure and improve population health and well-being within communities and across the state.
• Aligned Quality Measures. All Virginia health organizations would have a core, non-duplicative set of quality measures that are used by all payers to judge provider quality of care as part of payer-specific financial incentive programs.
• Aligned Payment Models. All public and private payers would base payment
incentives on the same quality measures for populations with similar health needs (e.g. chronic conditions), although detailed payment models may vary across payers.
• Aligned HIT Capacity. All Virginia health organizations would have the
health information capacity necessary to optimize care within and across health care settings, including electronic health record systems and health information exchange capabilities.
LG’s Roundtable: Framework

Framework Continued:
• Rapid Feedback. All Virginia health organizations would have access to measures and reporting tools that enable them to rapidly identify and take action on opportunities to improve the quality and value of health services and supports.
• Consumer and Policymaker Empowerment. All Virginia consumers and policymakers would be equipped with valid and understandable information to inform their choices about individual care and system level changes based on evidence of quality and value.
• Summative Evaluation. The program would be able to rigorously and credibly estimate the summative impact of VHIP 2015 on Virginia health and health care.
LG’s Roundtable: Framework

PROPOSED Transformational Goals:
By 2020, we will achieve a measurable improvement in the health of Virginians and the value of health care they receive. We will set concrete, ambitious goals related to the following drivers of high-value care:
Improvement in targeted population health goals; Improved patient experience and patient engagement; Improved prevention and management of chronic and high-risk conditions; Improved access to coordinated care; Reductions in health care spending associated with unnecessary or
preventable utilization; An improved health care marketplace in which providers are rewarded for
high-value care; Increases in the number of patients that are informed and empowered
consumers of health care.
LG’s Roundtable: Transformational Goals and
High Level Indicators

Candidates for High Level Indicators:
• Measures of targeted population health improvement goals (Relates to Goal 1)
• Percent of Virginians reporting a positive health care experience (Relates to Goal 2).
• Percent of Virginians indicating positive engagement in their health care management (Relates to Goal 2)
• Percent of Virginians with access to primary or preventive outpatient care. (Relates to Goals 3 and 4).
• Population rate of Emergency Department visits related to target chronic and high-risk conditions. (Relates to Goals 3, 4, and 5).
• Population rate of inpatient admissions and re-admissions related to target chronic and high-risk conditions. (Relates to Goals 3, 4, and 5).
LG’s Roundtable: Transformational Goals and
High Level Indicators

Candidates for High Level Indicators (Continued):
• Percent of Virginians with advance directives. (Relates to Goals, 2, 5, 7).
• Percent of Virginians whose provider operates under a value-based contract. (Relates to Goal 6).
• Percent of providers indicating that payment systems create positive incentives for delivering high value care. (Relates to Goal 6).
• Percent of Virginians utilizing health care quality and cost data to inform health decisions (Relates to Goal 7)
• Total annual per capita spending on health care for Virginians. (Relates to Goals 1-7).
LG’s Roundtable: Transformational Goals and
High Level Indicators

For our work, we are proposing:
Value =
(Access to Care + Quality of Care + Patient Experience of Care + Health Outcomes)
Per Capita Health Care Spending
Using this conceptual definition, value is increased by improving access, care quality, patient experience, and/or health outcomes relative to per capita health care spending. The Virginia SIM will place special emphasis on efforts that target all five elements of the value equation (access, quality, experience, outcomes, and cost).
LG’s Roundtable: Proposed Definition of Value

SIM Staff are seeking input on these transformational goals and high level indicators. Specifically, we need for you to let us know:
• Are there other Transformational Goals that you believe we should consider? Please specify.
• Which of the High Level Indicators do you have concerns with, and why?
• Are there other High Level Indicators you believe we should consider? Please specify.
LG’s Roundtable: Seeking Input

• The SIM staff will compile input on the proposed transformational goals and high level indicators and bring a revised set to the June 15th Roundtable meeting. At that meeting, the expectation will be to review, refine and endorse the transformational goals and high level indicators.
• At that meeting, we will also discuss identifying Key Improvement Areas as an additional filter for the final selection of core measures. Key Improvement Areas might include diabetes, cardiovascular disease, cancer, etc.
• The SIM staff will then use the endorsed Goals, Indicators, and Key Improvement Areas (if applicable) as a filter for beginning to identify a core set of measures.
• At the July 27th meeting, Roundtable members would review, refine, and endorse Key Improvement Areas and begin a discussion of proposed core measures.
• At the August 17th meeting, Roundtable members would review, refine, and endorse a set of core measures that could be prioritized by DMAS, the state employee health benefits plan, and willing health plans and employers.
LG’s Roundtable: Next Steps

Public and private stakeholders work collaboratively to advance the Triple Aim for their region’s population.
• The creation of Accountable Care Communities (ACCs) in Virginia is the core strategy of Virginia’s State Innovation Model Design Award.
• Successful ACC development requires multiple public and private stakeholders to commit to working collaboratively to advance the Triple Aim in their regions and to share the responsibility for the health of the community.
• The success of regional ACC development depends on the creation of non-traditional partnerships.

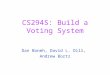
Proposed ACC Regions
Southwest
Central
Northwest
Northern
Eastern

PROCESS
APRIL
Select 5 regions to serve as pilot Accountable Care Communities
MAY
Introductory regional ACC meetings Who is the Coalition of the Willing? Beginning to look at regional population health data
JUNE - AUG
Ongoing updates via the VHIN: Population Health Improvement Plan SIM pilot development
SEPT
Regional ACC Meeting: DSRIP update SIM pilots update Funding opportunities
OCT
Solicit feedback from each region on emerging partnerships, potential ACC governance structures, and potential target areas.
NOV
Final ACC Meeting Regions present updates Discussion of priorities Next steps for 2016 – Regional Transformation Plans

DSRIP: Delivery System Reform Incentive Payment
Program
What is a DSRIP Waiver? Provides federal Medicaid funds to invest in transformation of the delivery system
for Medicaid and uninsured populations
State must have a clear and compelling vision for a transformed delivery system after the 5 years of DSRIP funding
State identifies new care delivery and payment innovations intended to transform the delivery system
Providers join together in integrated delivery systems to undertake transformation activities
State funds providers based on achieving specified milestones/metrics

17
Approved and Pending DSRIPs
WA
Approved Pending

18
State Amount of DSRIP
Duration Participating Providers
Texas $11.4 billion 5 years 300+ public and private hospitals, 38 local mental health authorities, public health departments, law enforcement agencies
New York $6.4 billion 5 years Public and private hospitals, FQHCs, primary care practices, mental health authorities, nursing homes, home health agencies
California $3.3 billion 5 years 21 public hospitals
Massachusetts $1.1 billion 5 years* 7 safety-net hospitals (1 public, 5 non-profit, 1 for-profit)
New Jersey $611 million 5 years Any hospital in state (can opt out)
Kansas $100 million 5 years State university hospital and children’s hospital
New Mexico $29 million 5 years 29 hospitals (public and sole community providers)
DSRIPs Approved in Other States
*Note: Massachusetts initially received $628 million over 3 years and recently had an extension improved for 2 additional years with hospitals receiving up to $230 million per year.

DSRIPs are increasingly focused on supporting state policy goals
19
CA: Hospital-specific quality improvement
projects
TX: Region-wide transformation plans anchored by hospitals
and local mental health authorities
MA: Payment reform to prepare for statewide
transition to alternative payment
methodologies
NJ: Healthy NJ chronic disease reduction
effort
NY: Specific goal to reduce preventable
hospitalizations by 25% statewide over 5 years

• Vision: States must have a vision for how DSRIP funds will support transformation of the delivery system for Medicaid and uninsured populations that aligns with state policy goals
• Overarching goal: States must have a goal they will achieve with DSRIP (such as New York’s goal is to decrease preventable hospitalizations by 25%) and the data to support why this goal is important for their state
• Focus on behavioral health: CMS is encouraging states to include mental health and substance abuse treatment innovations in their DSRIP project menus
• Measurement of outcomes: States are expected to build the infrastructure to collect and analyze data to measure the impact of DSRIP on regional outcomes and expenditures (DSRIP can pay for this data infrastructure and data analytics)
• Sustainability: CMS expects the program to become self-supporting over time and eliminate the need for continued federal subsidy
20
Emerging DSRIP Trends from CMS

New Opportunity: Heart of Virginia Healthcare
$11 M grant from AHRQ to Virginia to advance primary care transformation over the next 3 years. (Virginia is one of 7 grantees)
Key Partners: Virginia Commonwealth University, Virginia Center for Health Innovation, Virginia Association of Family Physicians, American College of Physicians, VA Chapter, Virginia Community Healthcare Association, Virginia Health Quality Center, Community Health Solutions, George Mason University
Core Activities: develop a package of capacity building supports to help primary care providers transform their practices for population health management based on principles of the Chronic Care Model, PCMH, health information exchange, and clinical-community partnership.
Focus is on disseminating six cardiovascular PCOR findings (ABCS) to small to mid-size (10 or fewer physicians, NPs, and Pas) practices. Highly beneficial to ensure we know how all health plans are measuring performance in these areas and work to eliminate an unnecessary conflicts.
We will offer extensive practice coaching through a statewide learning collaborative and 10 practice coaches.

What does all this mean for Virginia’s Health Plans?
• Collaboration on the identification, adoption, and promotion of shared quality improvement measures seems essential.
• VCHI wants to align its recommendations and activities with measures already incentivized by health plans where possible.
• To do this, we need to know what you measure. We need your engagement in these planning discussions.
Recommended