Stiff Skin Syndrome: A Case Report
Cem Mat, M.D.,* Aylin Kalayciyan, M.D.,* Nurcan Arzuhal, M.D.,*
Cuyan Demirkesen, M.D.,� Murat Karacorlu, M.D.,� and Yalcın Tuzun, M.D.*
Departments of *Dermatology and �Pathology, Cerrahpasa Medical Faculty, University of Istanbul, and �IstanbulRetina Institute, Istanbul, Turkey
Abstract: Stiff skin syndrome (SSS) is a disease similar to sclerodermawith an unknown etiology. Stone-hard areas of skin are observed from birthor in early childhood. In this article we describe a 15-year-old girl with skinhardening and limitation of movement. We diagnosed the case as SSS, ofwhich we have not encountered a similar report in the Turkish literature.
Stiff skin syndrome (SSS) was first defined in 1971 byEsterly andMcKusick (1). It presents as stone-hard areasof skin that areobserved frombirthor in early childhood.Its etiology is unknown.
CASE REPORT
A 15-year-old girl was referred to us because of skinhardening and limitation of movement since infancy.Her family noticed that her leg and hip muscles weretighter than usual and sought medical attention. Sincethen, numerous studies including skin and subcutaneousbiopsies, whole-body bone radiographs, and elec-tromyography have been undertaken. She had severalprevious diagnoses, including Buschke scleredema,morphea, and dermatomyositis, and was treated withpenicillin-G, D-penicillamine, cyclosporine, and met-hotrexate, the shortest treatment duration being3 months. However, her skin stiffness has increased overtime.
On examination her skin was a normal color. Theright side of her facewas depressed and she had no radialfacial wrinkles. The range of motion in her limb jointswas limited, being more pronounced in the proximaljoints. Stiffness of the skin and subcutis was felt on pal-pation, mild in the hands and feet but more severeproximally.The greatest tightness of tissuewas felt on the
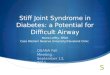
back, waistline, and gluteal region, with an unevenappearance of the skin overlying the femoral region. Allof the above findings weremore pronounced on the rightside of the body. Her posture was impaired, with an in-crease in thoracic kyphosis and lumbar lordosis, the leftshoulder being lower than the right, with mild flexioncontracture of the knee and elbow joints (Fig. 1). She hadmild hypertrichosis. The nails, hair, and teeth were nor-mal.
The history of the patient was unremarkable. Thechildhood development stages were in order and timelyand her mental status was normal.
Routine laboratory values were within the normalranges. The two-sided dorsolumbar vertebral radio-graphs revealed dorsal lordosis. No mucopolysaccha-rides were detected in the urinalysis. On ophthalmicexamination, no pathology was detected other thanaccommodative isotropia and hyperopia.
A biopsy specimen, taken from the right femoralregion, extending deep into the fascia, demonstratedhydropic degeneration of the basal keratinocytes, mildvascular proliferation in the upper dermis, and a milddeposition of mucopolysaccharides between the colla-gen bundles throughout the dermis, demonstratingmetachromasia with alcian blue stain (Fig. 2). Musclesand fascia showed no abnormalities. No amyloiddeposition was detected on Congo staining of the
Address correspondence to Aylin Kalayciyan, M.D., I_stanbulUniversitesi Cerrahpaa Tıp Fak, Dermatoloji AD, Kocamustaf-apasa, Istanbul, Turkey, or email: [email protected].
339
Pediatric Dermatology Vol. 20 No. 4 339–341, 2003

specimen, and no fibrotic changes were recorded in thefascia.
DISCUSSION
Stiff skin syndrome is a connective tissue disease similarto scleroderma, of unknown origin. The first patientwas described in 1968 with skin changes resemblingthose of scleroderma and with joint contractures (2), butthe disease was first well defined by Esterly andMcKusick in 1971 (1) in four patients as joint limitationand mild hypertrichosis, and termed SSS. Esterly andMcKusick thought of the condition as a localized formof mucopolysaccharidosis (1). The disease is present atbirth or develops early in infancy. In our patient theskin tightness was first noticed at the age of 1 year byher parents.
Two types of SSS have been defined. An autosomalrecessive type, also known as Parana syndrome, ischaracterized by diffuse hardening of skin with jointcontractures, hypertrichosis, hyperpigmentation, and avariety of systemic problems. This syndrome was des-cribed in eight patients in seven Brazilian families livingin a small area of southern Parana. By the age of 2 or3 months, the skin of the entire body becomes progres-sively thicker. All joints gradually become frozen andmovement of the chest and abdomen is severely restric-ted. Respiratory insufficiency may lead to death. Paranasyndrome is probably distinguishable from SSS by thesevere growth retardation, more malignant course, andprobable mode of inheritance (3).
In the autosomal dominant type, joint contracturesare also present, but other manifestations are less fre-quentlyobservedandaremilder (4).The skinfindings aremost commonly observed on the gluteal and femoralregions. The face, hands, and feet are usually spared (5).In our patient the stiffness was more pronounced at thewaistline and in the femoral and gluteal regions. Sclero-dactyly is not a prominent feature as in scleroderma, andin our patient the stiffness was clearly more prominent inthe proximal extremities.
Histopathologic examination shows noninflamma-tory thickening of the fascia, but the muscles and elasticfibers are not affected (5). In some cases, mucopolysac-charide deposition may be detected (4). Electron micro-scopic examination shows packed, abnormal collagenfibers (5). The histopathologic findings of our patientwere in accordance with those of previous reports. Thedifferential diagnosis includes morphea and sclerodermawith prominent, thick, deeply eosinophilic, closelypacked collagen bundles in the dermis. Another entity tobe considered is Schulman eosinophilic fasciitis, in whichthe fascia is markedly thickened and is permeated by a
Figure 1. Posture was impaired, with an increase in thoracickyphosis and lumbar lordosis, the left shoulder lower than theright, and a mild flexion contracture of the knee and elbowjoints.
Figure 2. Hydropic degeneration of the basal keratinocytes,mild vascular proliferation in the upper dermis, and milddeposition of mucopolysaccharides between the collagenbundles throughout the dermis. (Hematoxylin and eosin;magnification 100·.)
340 Pediatric Dermatology Vol. 20 No. 4 July/August 2003

chronic inflammatory infiltrate. The absence of pathol-ogy in collagen fibers, adnexae, and fascia in our patientrules out these conditions (6).
Stiff skin syndrome seems to be a diagnosis of exclu-sion, with a distinctive clinical presentation but nopathognomonic laboratory or histologic findings. Thestiffness being proximal rather than distal as in sclero-derma, the limitation of joint mobility, mild hypertri-chosis, and the appearance of the disease in early infancyare themain diagnostic elements. The absence of internalorgan involvement such as in dysphagia, renal, pul-monary, or cardiac disease, calcinosis cutis, Raynaudphenomenon, or sclerodactyly rules out these diseases inthe spectrumof systemic sclerosis (4). Our patient had noexposure to the chemical substances or drugs that havebeen implicated in the pathogenesis of pseudoscleroder-ma (7).
Evaluation of patients with SSS for possible muco-polysaccharidosis has been done previously and serumlevels of b-galactosidase, b-glucuronidase, b-hexosa-minidase, a-mannosidase, and a-fucosidase were foundto be within normal limits (2). Mucopolysacchariduriahas never been encountered (4,5). A similar evaluation ofourpatient revealednomucopolysacchariduria.With theclinical andevaluativedata, adiagnosis ofSSSwasmade.
No effective treatment has yet been found. Exercisesand rehabilitative therapy are important in maintainingthe patient’s quality of life (5).Our patientwas given a setof exercises and is being followed-up periodically, but ison no medications.
REFERENCES
1. Esterly NB, McKusick VA. Stiff skin syndrome. Pediatrics1971;47:360–369.
2. Kikuchi I, Inoue S, Hamada K, Ando H. Stiff skin syn-drome. Pediatr Dermatol 1985;3:48–53.
3. Cat I, Rodrigues-Magdalena NI, Parolin-Marinoni L,et al. Parana hard-skin syndrome: study of seven families.Lancet 1974;1:215–216.
4. Braun-Falco O, Plewig G, Wolff HH, Burgdorf WHC, eds.Diseases of connective tissue. In: Dermatology, 2nd ed.Berlin: Springer-Verlag, 2000:758.
5. DevaneyK,LevyML,OranjeAP.Fibromatoses, hyalinosesand stiff skin syndrome. In: Harper J, Oranje A, Prose N,eds. Textbook of pediatric dermatology. Oxford: BlackwellScientific, 2000:793–812.
6. LeverWJ, Schaumburg-LeverG.Connective tissue diseases.In: Histopathology of the skin. Philadelphia: JP Lippincott,1983:445–471.
7. Mitchell H, Bolster MB, LeRoy EC. Scleroderma andrelated conditions. Med Clin N Am 1997;81:129–149.
Mat et al: Stiff Skin Syndrome 341
Recommended