AA
SL
DA
bst
ract
s
Hepatic Encephalopathy Scoring Algorithm (HESA)
Su1689
Eight Questions of the Patient-Reported Sickness Impact Profile CanEffectively Screen for Minimal Hepatic EncephalopathyEiman H. Nabi, Leroy R. Thacker, Douglas M. Heuman, Arun J. Sanyal, Richard K.Sterling, R. Todd Stravitz, Velimir A. Luketic, Iliana Bouneva, Michael Fuchs, MohammadS. Siddiqui, Melanie B. White, Pamela Monteith, Nicole Noble, Jasmohan Bajaj
Background: Minimal hepatic encephalopathy (MHE), which impairs quality of life (QOL),is difficult to diagnose using curent cognitive tests by non-specialists. The detection ratescould potentially improve with easier, patient-administered methods that do not requirespecialized testing or equipment. Aim: to detect MHE using a validated QOL questionnaire,Sickness Impact Profile (SIP). Methods: 170 cirrhotics (55yrs, 13 yr education, MELD 9,50%HCV,11%alcohol) without prior overt HE were administered a standard cognitive battery(Number connection-A/B, Digit Symbol and Blocks) as the gold standard for MHE diagnosisalong with SIP. SIP consists of 136 questions across 12 QOL domains (body care andmovements, mobility, ambulation,emotional behavior, social interactions, alertness,commu-nication, work, sleep and rest, eating, home management and recreation/ pastime) thatrequires a yes/no answer over the past 24 hours. Proportion of patients that responded "yes"to each question was compared between MHE and no-MHE groups. Variables independent ofcognitive testing; demographics (age,education,gender,alcoholic etiology) and SIP questionsdifferentiating between groups were analyzed using logistic regression and ROC analysis forMHE diagnosis. Results: 93(55%) patients had MHE on standard tests. On SIP, a "yes"response was found in a higher proportion of MHE patients on 54 questions across all QOLdomains. On regression age,male gender and eight questions " I stay away from home onlyfor brief periods of time ", "I do not maintain balance ","I react slowly to things said or done ", "Ido not keep my attention on any activity for long ", "I act irritable or impatient with myself "," Iam not doing any of the shopping that I would usually do ", "I am not doing any of my usualphysical recreation or activities" and "I am eating much less than usual " differentiated betweenMHE/no-MHE groups. These questions spanned domains of alertness, eating, recreation/pastimes, emotional behaviour, body care, mobility and home management.The AUC onROC for MHE diagnosis was 0.90 with 81% sensitivity and 78% specificity with all 8statements, age and male gender. Conclusions: Eight patient-reported questions on SIP caneffectively screen for MHE in outpatient cirrhotic patients. MHE screening strategies thatdo not include specialized testing could increase detection rates and therapy.
Su1690
Long Term Outcomes in Patients Undergoing Orthotopic Liver Transplantation(OLT) for Portopulmonary Hypertension (POPH)Saira A. Khaderi, Rashid Khan, Zeenat Safdar, Benjamin J. Blow, Rise Stribling, John M.Vierling, John A. Goss, Norman Sussman
Background: POPH occurs in 2-12.5% of cirrhotic patients. Survival in the absence of (OLT)is reportedly 38% at 3 yrs and 28% at 5 yrs. Mild POPH poses little perioperative risk, butmoderate-to-severe POPH (PA mean pressure [PAM] .35 mmHg) is associated with a 50-80% perioperative mortality. Hence, uncontrolled POPH is a contraindication for OLT.Although UNOS allows MELD exception points, only 79 patients were transplanted forPOPH in the USA from 2007-2011. Single-center series have demonstrated the feasibilityand short-term efficacy of OLT after controlling POPH with vasodilators, but long-termoutcomes after OLT have not been reported. Aims: To determine graft and patient survivalsand effect of OLT on pulmonary hypertension (PHT) in patients transplanted for POPH inour center. Methods: Of 492 adult patients transplanted between January 2004 and January2011, seven were transplanted for POPH after reducing PAM to ,35 mm Hg using vasodila-tors. Results: The 7 patients (1.4% of transplanted adults) included 3 men and 4 women,ages 38 to 53 yrs at the time of OLT. The etiologies of cirrhosis were hepatitis C (n= 3),alcohol (n= 2), and cryptogenic (n= 2). All patients were transplanted with MELD exceptionpoints of 25-34 (calculated MELD scores of 6-14). Six patients required pre-OLT IV epopros-tenol (EPO), and 1 was managed with oral sildenafil. All patients received IV or inhaledEPO in the perioperative period, and all were weaned off EPO over a period of 3 days to8 months. None required long-term EPO. Both graft and patient survivals are 100% aftera median follow-up of 7.5 years (range, 1.7 to 8.3 years). One patient has recurrent cirrhosiscaused by HCV infection and has recently started sildenafil for recurrent POPH. Five patients(71.4%, including the 1 with cirrhosis) require oral vasodilator therapy for persistent orrecurrent PHT. Their New York Heart Association Functional Class is I-II. Only 2 of the 7patients (3.3 and 7.5 years post-OLT) do not have PHT. Conclusions: Patients with POPHresponsive to vasodilator therapy may have excellent long-term graft and patient survivals
S-998AASLD Abstracts
after OLT. Their functional class after OLT appears to be similar to that of patients transplantedfor other indications. Despite alleviation of portal hypertension by OLT, most patients havepersistent or recurrent PHT that can be controlled with oral vasodilators
Su1691
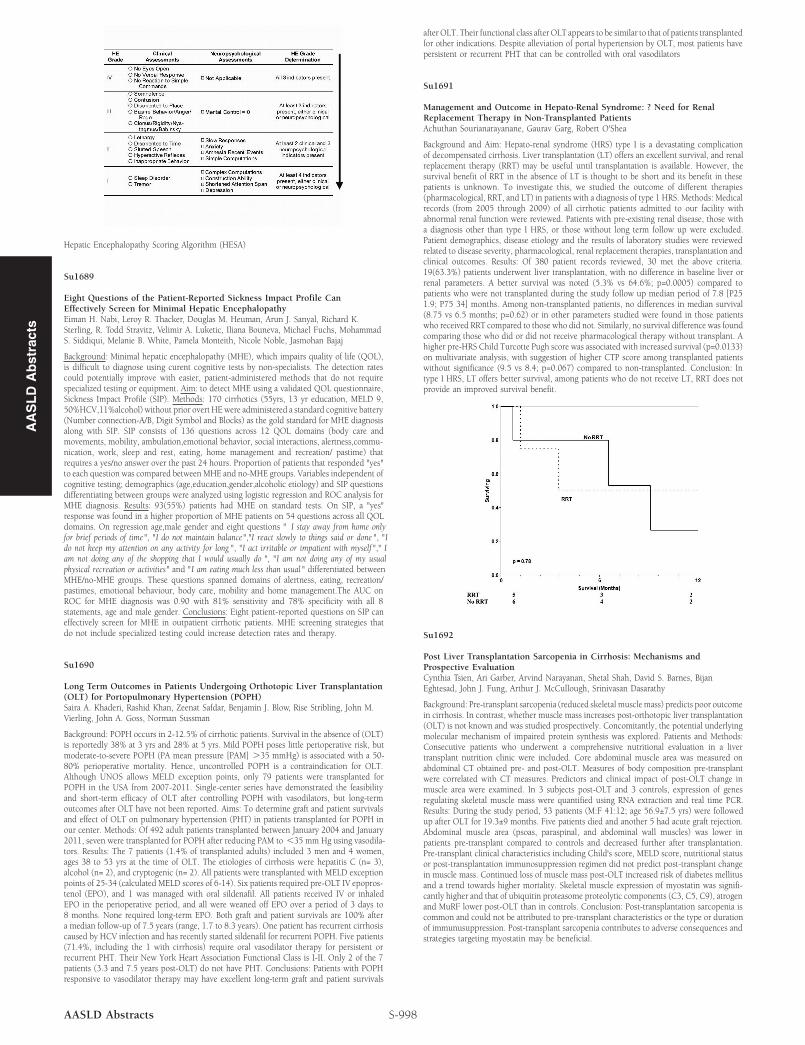
Management and Outcome in Hepato-Renal Syndrome: ? Need for RenalReplacement Therapy in Non-Transplanted PatientsAchuthan Sourianarayanane, Gaurav Garg, Robert O'Shea
Background and Aim: Hepato-renal syndrome (HRS) type I is a devastating complicationof decompensated cirrhosis. Liver transplantation (LT) offers an excellent survival, and renalreplacement therapy (RRT) may be useful until transplantation is available. However, thesurvival benefit of RRT in the absence of LT is thought to be short and its benefit in thesepatients is unknown. To investigate this, we studied the outcome of different therapies(pharmacological, RRT, and LT) in patients with a diagnosis of type 1 HRS. Methods: Medicalrecords (from 2005 through 2009) of all cirrhotic patients admitted to our facility withabnormal renal function were reviewed. Patients with pre-existing renal disease, those witha diagnosis other than type I HRS, or those without long term follow up were excluded.Patient demographics, disease etiology and the results of laboratory studies were reviewedrelated to disease severity, pharmacological, renal replacement therapies, transplantation andclinical outcomes. Results: Of 380 patient records reviewed, 30 met the above criteria.19(63.3%) patients underwent liver transplantation, with no difference in baseline liver orrenal parameters. A better survival was noted (5.3% vs 64.6%; p=0.0005) compared topatients who were not transplanted during the study follow up median period of 7.8 [P251.9; P75 34] months. Among non-transplanted patients, no differences in median survival(8.75 vs 6.5 months; p=0.62) or in other parameters studied were found in those patientswho received RRT compared to those who did not. Similarly, no survival difference was foundcomparing those who did or did not receive pharmacological therapy without transplant. Ahigher pre-HRS Child Turcotte Pugh score was associated with increased survival (p=0.0133)on multivariate analysis, with suggestion of higher CTP score among transplanted patientswithout significance (9.5 vs 8.4; p=0.067) compared to non-transplanted. Conclusion: Intype I HRS, LT offers better survival, among patients who do not receive LT, RRT does notprovide an improved survival benefit.
Su1692
Post Liver Transplantation Sarcopenia in Cirrhosis: Mechanisms andProspective EvaluationCynthia Tsien, Ari Garber, Arvind Narayanan, Shetal Shah, David S. Barnes, BijanEghtesad, John J. Fung, Arthur J. McCullough, Srinivasan Dasarathy
Background: Pre-transplant sarcopenia (reduced skeletal muscle mass) predicts poor outcomein cirrhosis. In contrast, whether muscle mass increases post-orthotopic liver transplantation(OLT) is not known and was studied prospectively. Concomitantly, the potential underlyingmolecular mechanism of impaired protein synthesis was explored. Patients and Methods:Consecutive patients who underwent a comprehensive nutritional evaluation in a livertransplant nutrition clinic were included. Core abdominal muscle area was measured onabdominal CT obtained pre- and post-OLT. Measures of body composition pre-transplantwere correlated with CT measures. Predictors and clinical impact of post-OLT change inmuscle area were examined. In 3 subjects post-OLT and 3 controls, expression of genesregulating skeletal muscle mass were quantified using RNA extraction and real time PCR.Results: During the study period, 53 patients (M:F 41:12; age 56.9±7.5 yrs) were followedup after OLT for 19.3±9 months. Five patients died and another 5 had acute graft rejection.Abdominal muscle area (psoas, paraspinal, and abdominal wall muscles) was lower inpatients pre-transplant compared to controls and decreased further after transplantation.Pre-transplant clinical characteristics including Child's score, MELD score, nutritional statusor post-transplantation immunosuppression regimen did not predict post-transplant changein muscle mass. Continued loss of muscle mass post-OLT increased risk of diabetes mellitusand a trend towards higher mortality. Skeletal muscle expression of myostatin was signifi-cantly higher and that of ubiquitin proteasome proteolytic components (C3, C5, C9), atrogenand MuRF lower post-OLT than in controls. Conclusion: Post-transplantation sarcopenia iscommon and could not be attributed to pre-transplant characteristics or the type or durationof immunusuppression. Post-transplant sarcopenia contributes to adverse consequences andstrategies targeting myostatin may be beneficial.
Recommended
![Hepatic Encephalopathy in Chronic Liver Disease: 2014 ... · ascites [7]. Overt hepatic encephalopathy is also reported in Overt hepatic encephalopathy is also reported in subjects](https://img.pdfslide.net/doc/110x75/5d489aa688c993047d8b91d5/hepatic-encephalopathy-in-chronic-liver-disease-2014-ascites-7-overt.jpg)
















