Superior Orbital Fissure Syndrome
Dr Rudraprasad Chakraborty1st Year PG Student
Department of Oral & Maxillofacial SurgeryRama Dental College Hospital And Research Centre
Kanpur, UP04/04/15
• Introduction
• The Syndromes
• The SOFS
• Related Anatomy
• Classification of SOFS
• Clinical Features
• Paathophysiology of C/F ( in White Board)
Inclusions

Introduction
Midface fractures on a high level in combination withorbital wall fractures can cause serious mechanical and neurogenic ophthalmologic complications
Based on the neurological deficits, different orbitalsyndromes can be distinguished
The Syndromes
• Partial or complete superior orbital fissure syndrome
• Retrobulbar hemorrhagic compression syndrome
• Orbital apex syndrome• Clivus syndrome
FrequencyThe frequency of orbital syndromes in complex midfacefractures is approximately 8% (Hardt and Sgier 1991).
Superior orbital fissure syndrome (SOFS) 2.2%Hemorrhagic-compression syndrome (HCS) 2.2%Nervus opticus syndrome (NOS) 1.9%Orbital apex syndrome (OAS) 1.6%Sinus cavernosus syndrome (SCS)
Superior Orbital Fissure Syndrome (SOFS)
A group of Neurological Deficits expressed by the altered functions of Nerves passing through the Superior Orbital Fissure due to dislocated bony fragments or comminuted fractures in the region of the superior orbital fissure or of the lesser wing of the sphenoid cause direct nerve lesions.
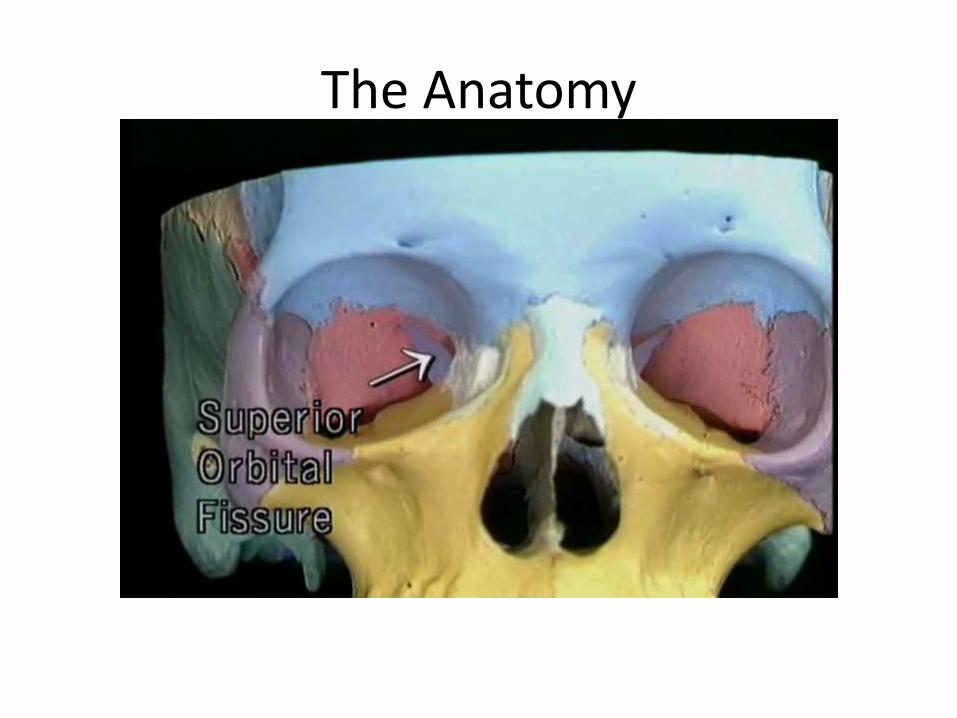
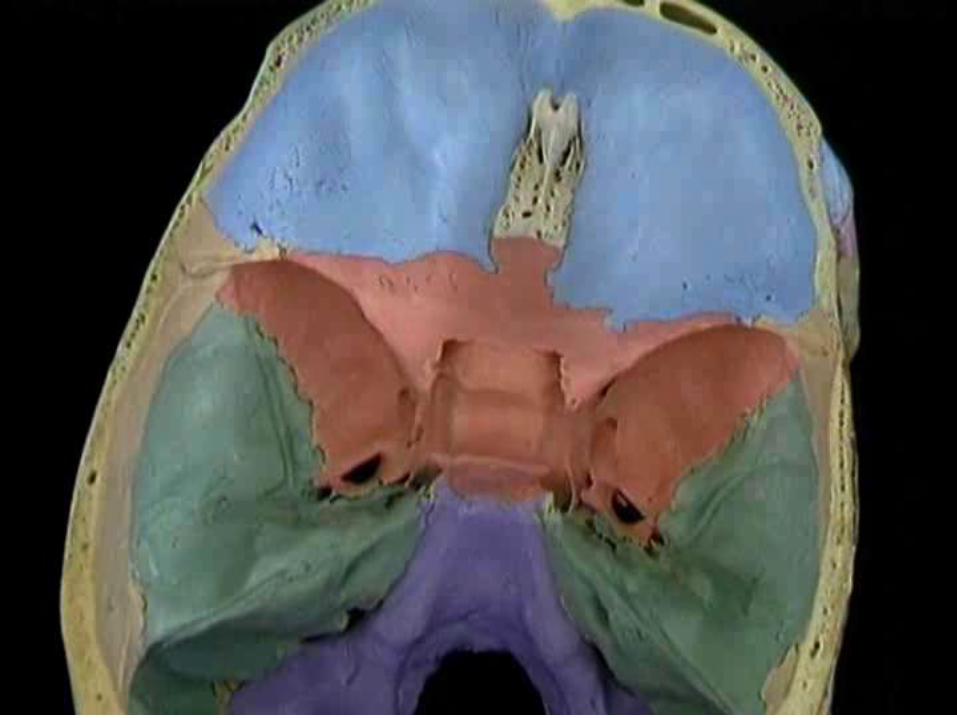
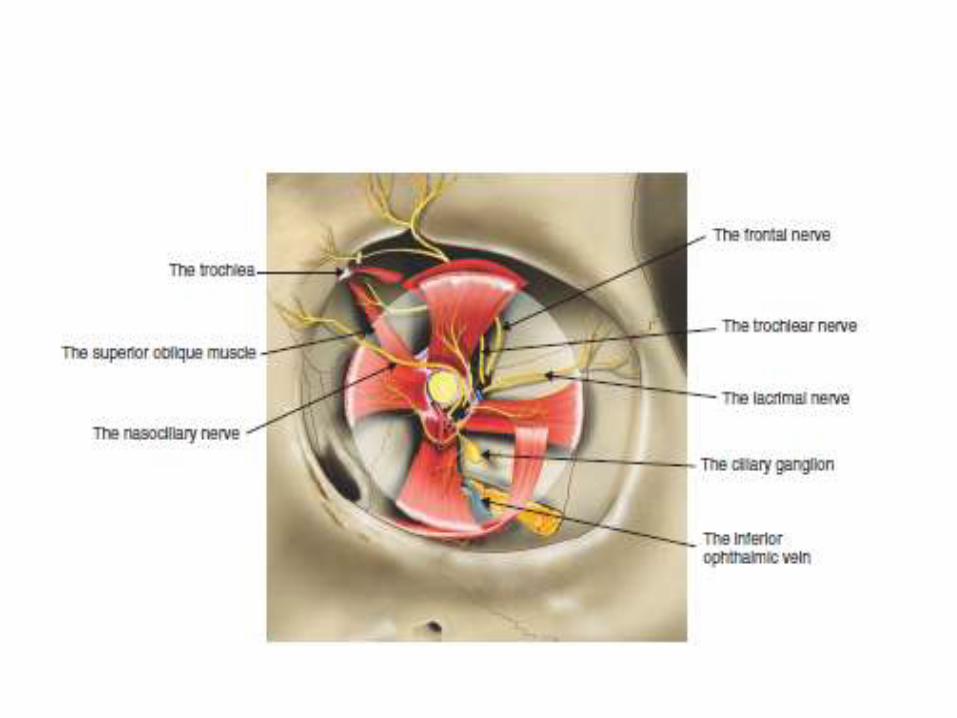
The Anatomy




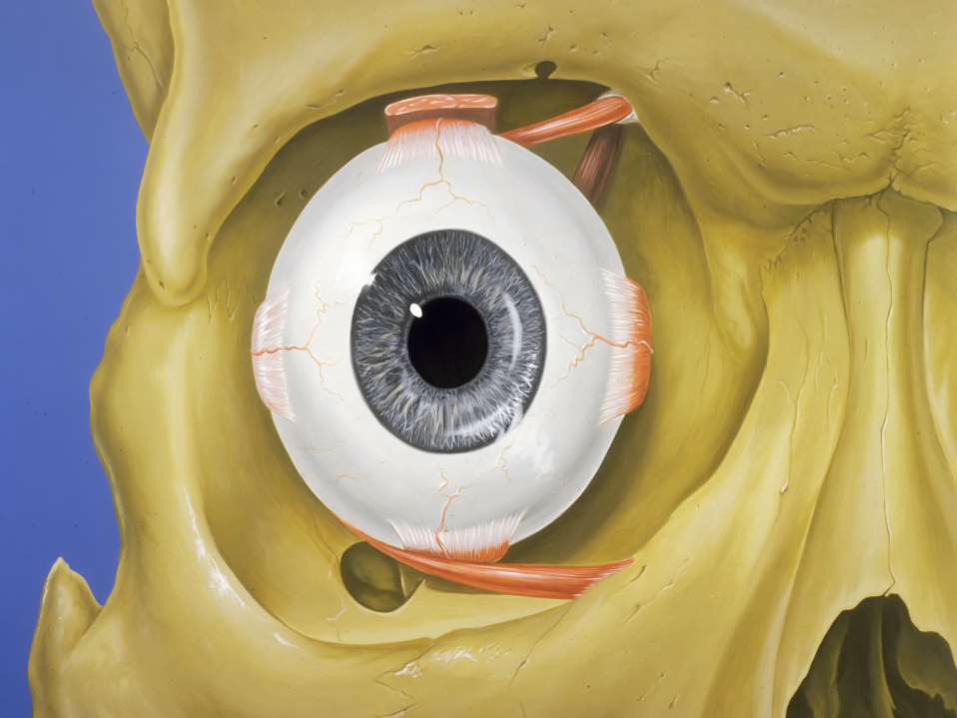
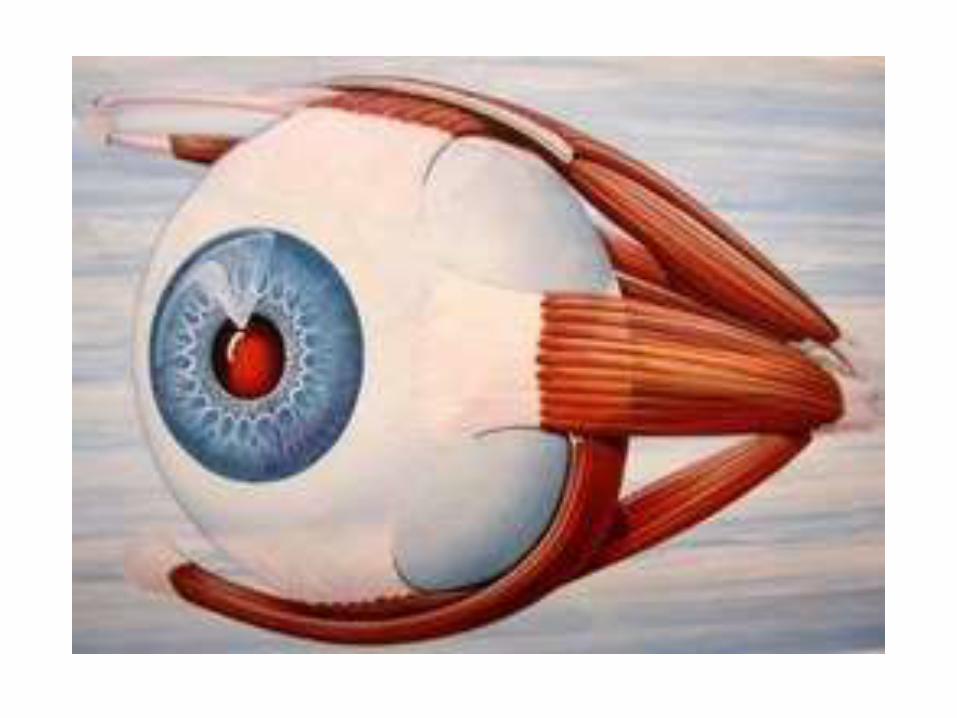
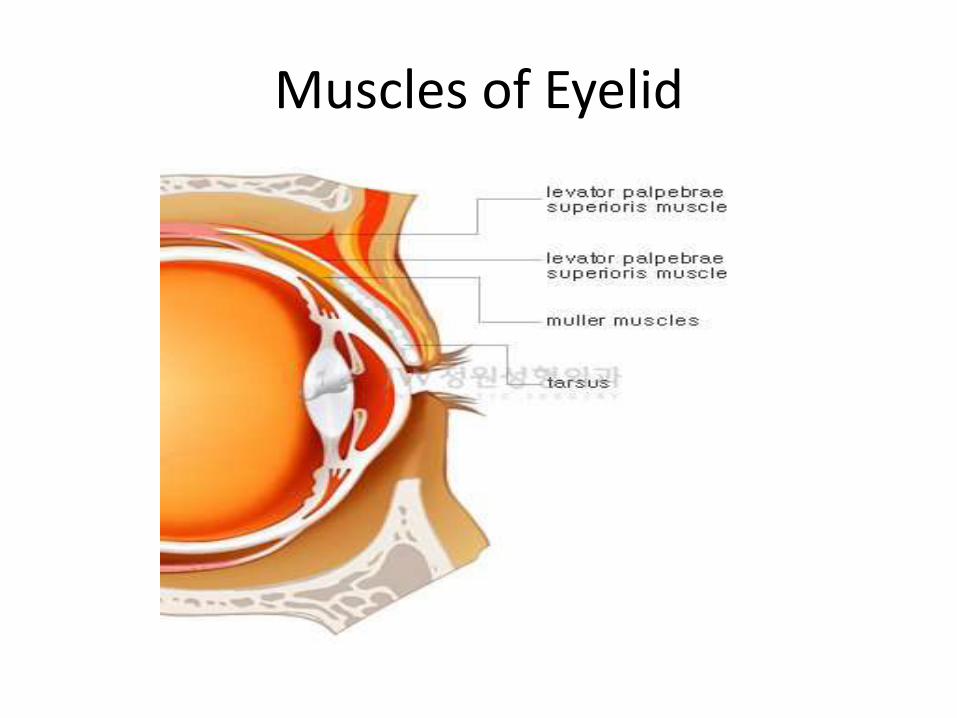
Muscles of Eyelid
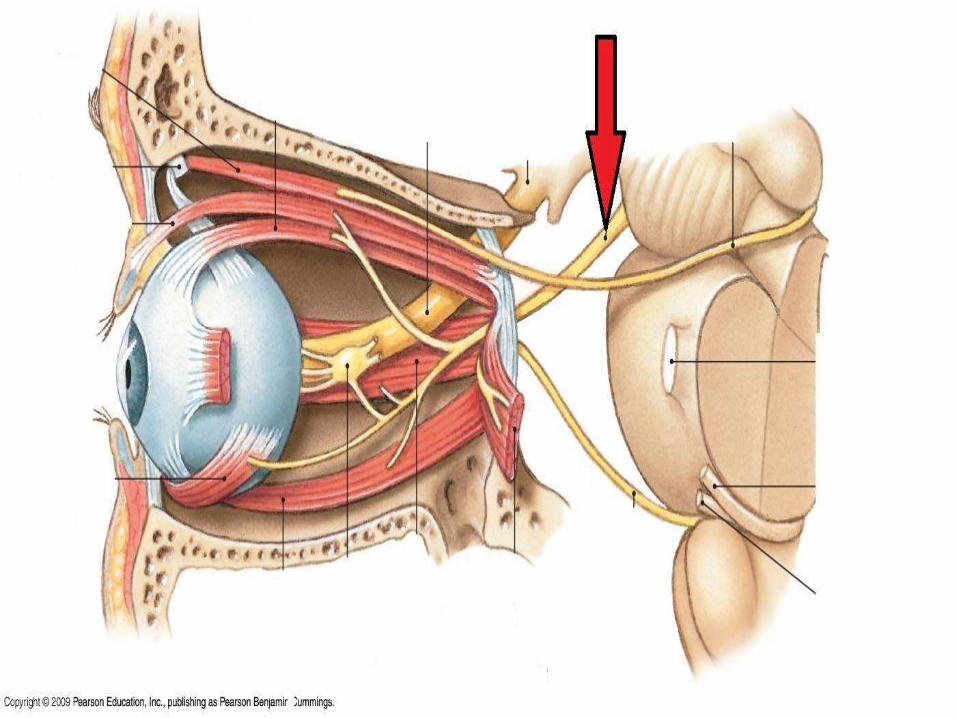
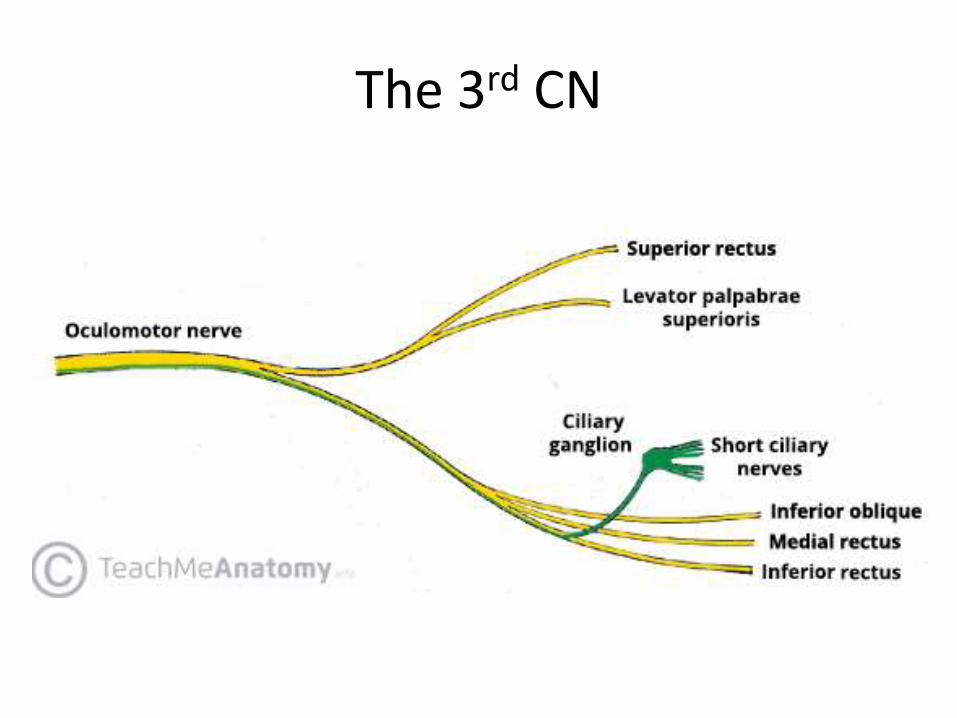
The 3rd CN
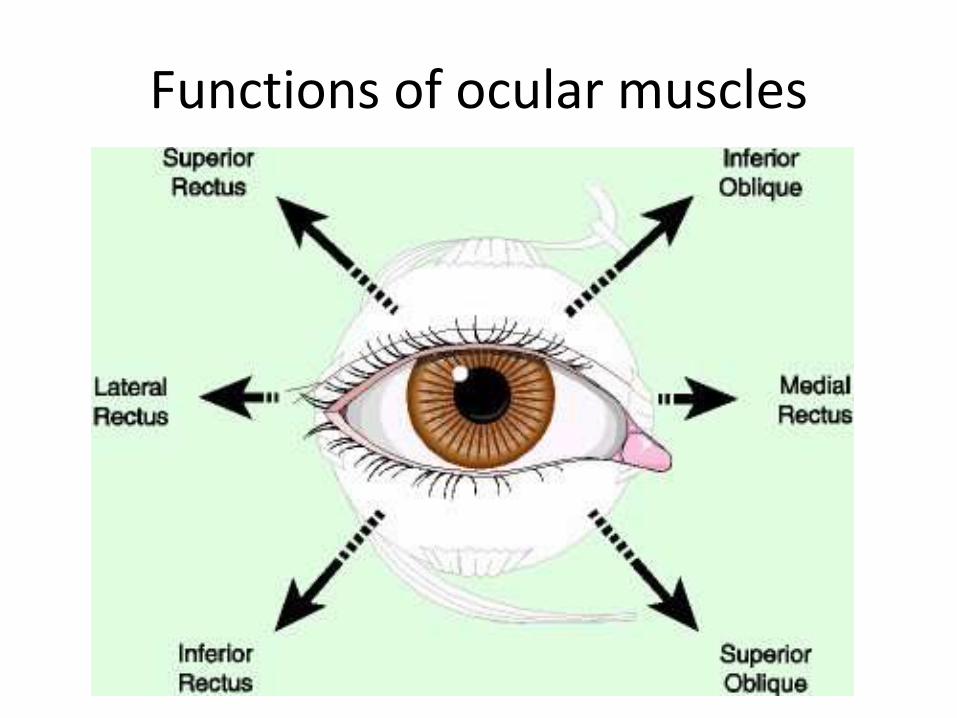
Functions of ocular muscles

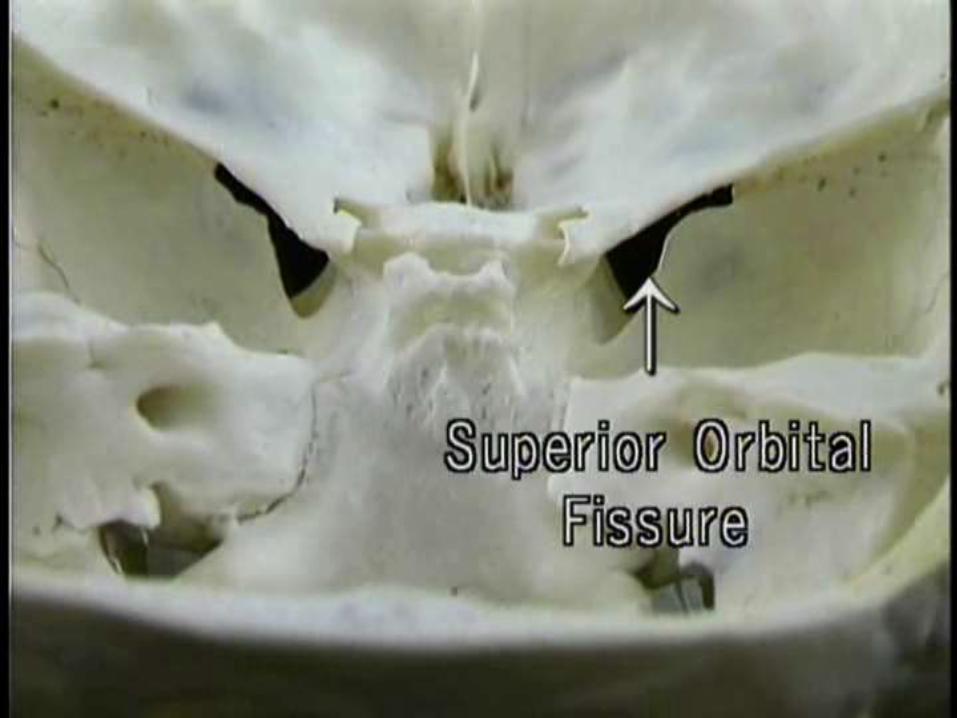
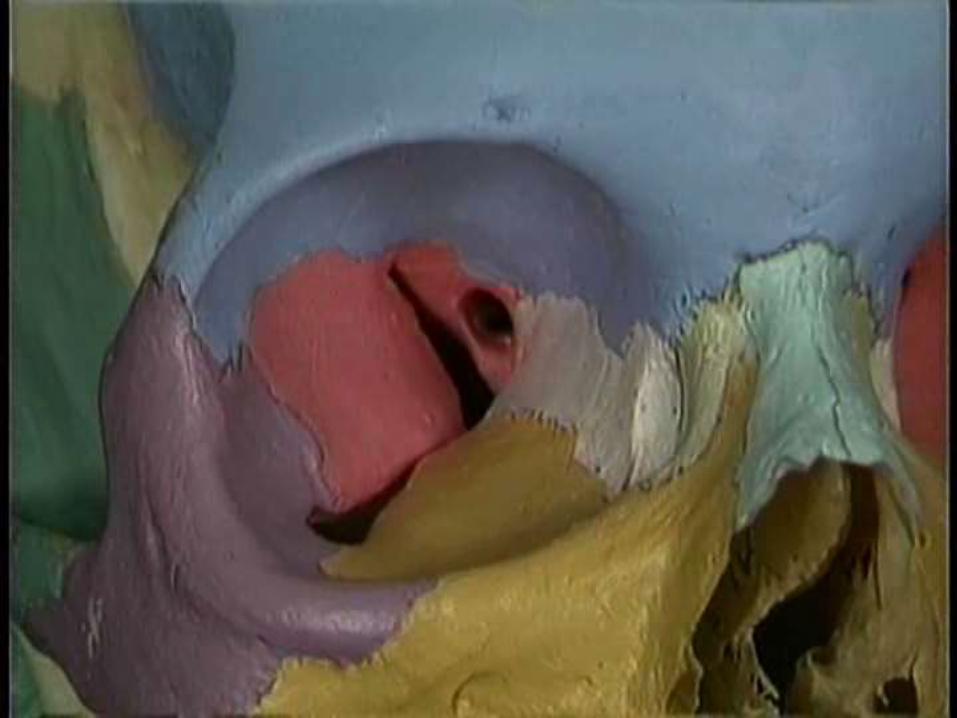
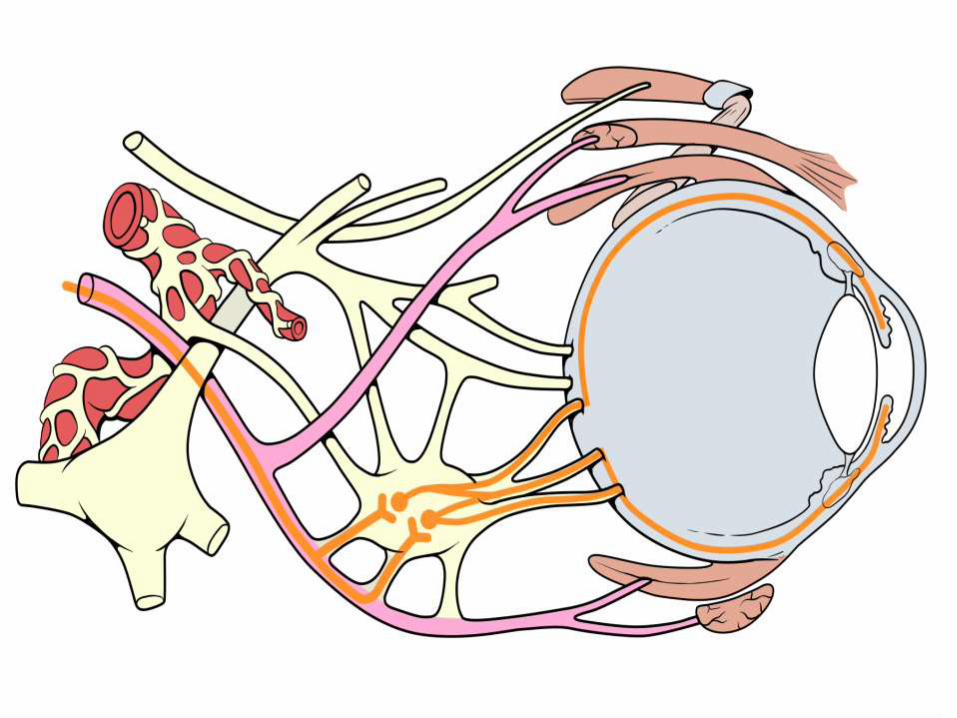
The SOF and Annular ring of Zinn

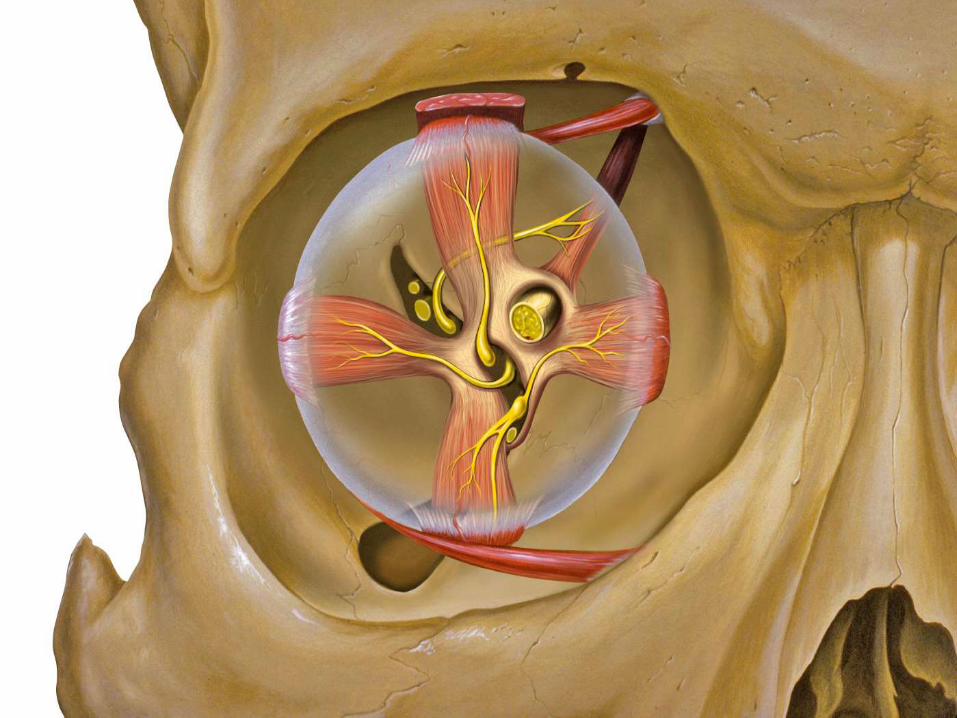
The Peripheral Nerves
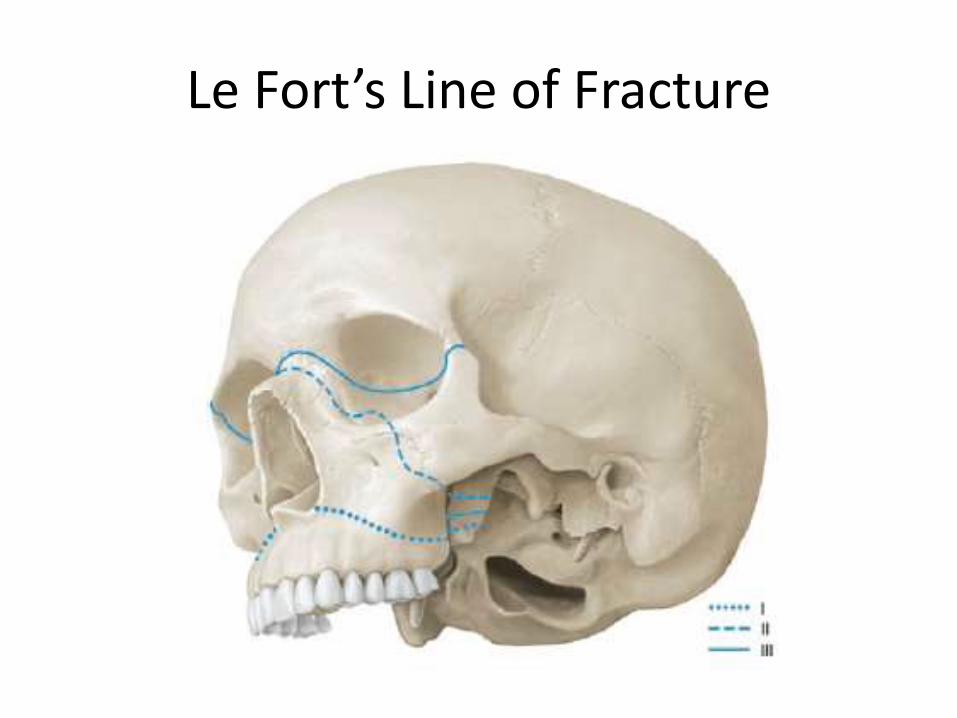
Le Fort’s Line of Fracture
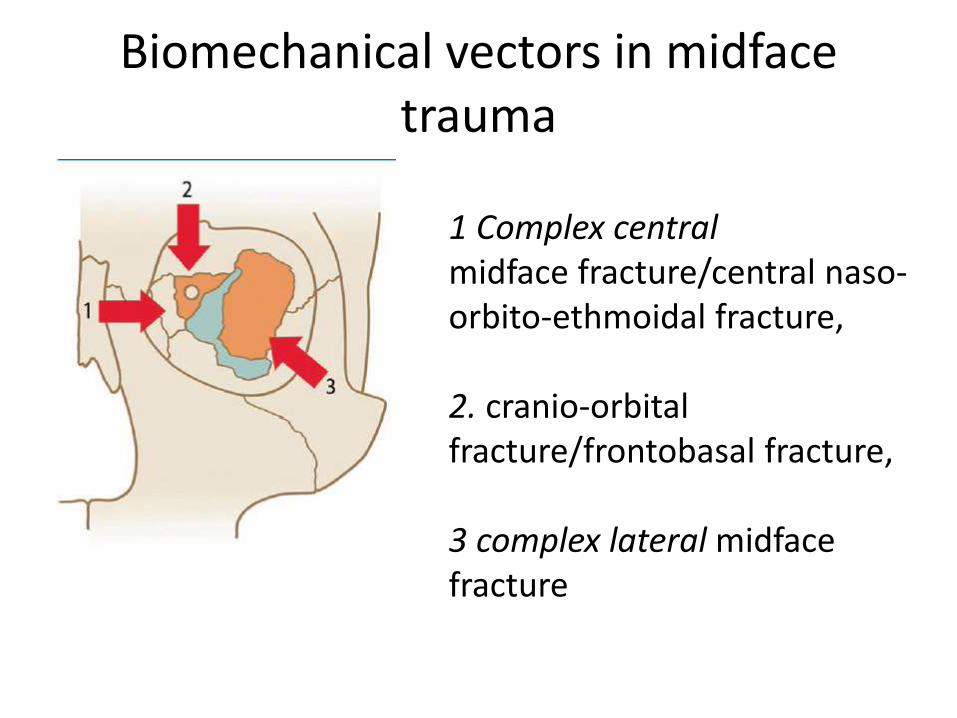
Biomechanical vectors in midfacetrauma
1 Complex centralmidface fracture/central naso-orbito-ethmoidal fracture,
2. cranio-orbital fracture/frontobasal fracture,
3 complex lateral midfacefracture
Complete & Incomplete SOFS
Complete SOFS : when all the cranial nerves entering through the SOF are involved.
Incomplete SOFS : when any of the cranial Nerves ( generally CN VI) is spared

The Complete SOFS
The complete SOFS results from a paresis of the cerebralnerves III, IV, and VI.
Clinically there is an ophthalmoplegia with ptosis and an exophthalmus due to disruption of the venous drainage
In addition, a mydriasis and an accommodation paralysis (cycloplegia) occur due to loss of the parasympaticinnervation
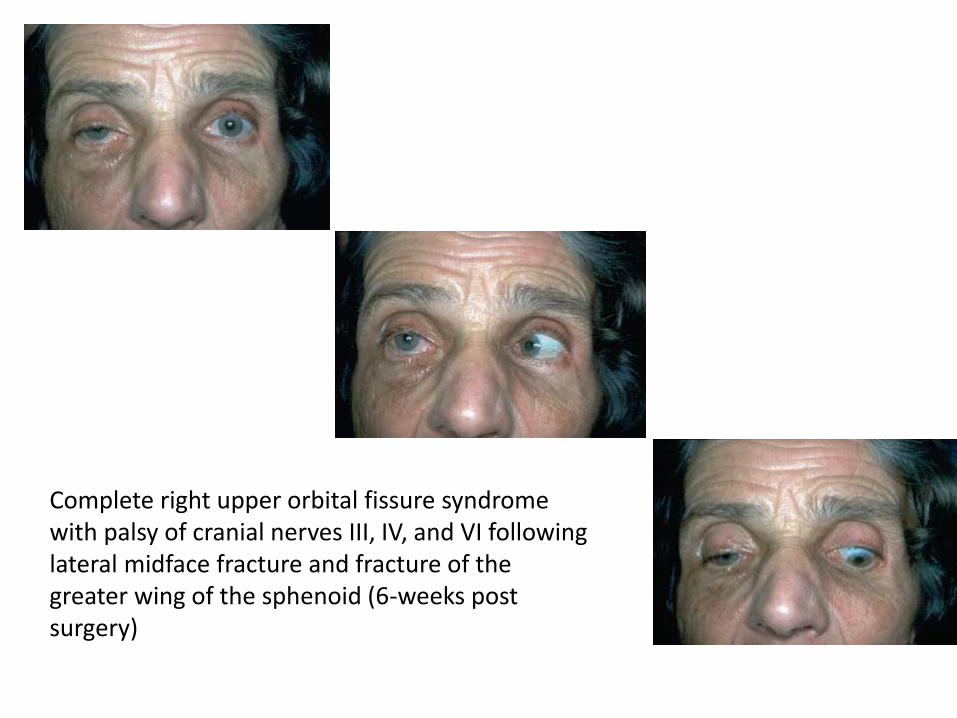
Complete right upper orbital fissure syndrome with palsy of cranial nerves III, IV, and VI following lateral midface fracture and fracture of the greater wing of the sphenoid (6-weeks post surgery)
Anesthesia in the areas of sensory innervation is inevitable if the sensory branches of the ophthalmic nerve and Nasociliary Nerve are involved.
A severe retroorbital pain sometimes occurs in combination with a supraorbital neurogenic pain as a result of the complex damage that has occurred
………………. (Hardt and Sgier 1991).
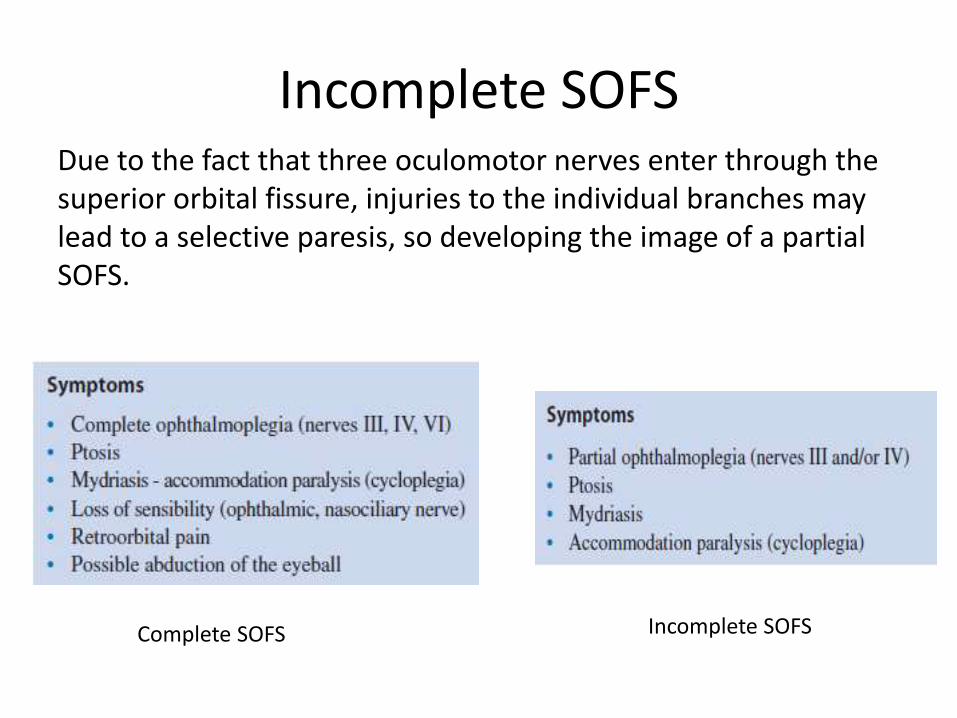
Incomplete SOFSDue to the fact that three oculomotor nerves enter through the superior orbital fissure, injuries to the individual branches may lead to a selective paresis, so developing the image of a partial SOFS.
Complete SOFS Incomplete SOFS


Let us nevigate in CNS…
White Board Please
Recommended