Surgery of the liver including transplantation
Prof Dr Dr Ernst HanischDirector
Department of Surgery
Asklepios Hospital LangenAffiliated Teaching Hospital University of Frankfurt/Main

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:783-785
Mangement of major abdominal trauma

Clinical features of serious liver injury Hypovolaemic shock Hypotension Tachycardia Decreased urine outpu Low central venous pressure Abdominal distension

Criteria for non-operative management of liver injuries Haemodynamically stable following
resuscitation No persistent or increasing
abdominal pain or tenderness No other peritoneal injuries that
require laparotomy <4 units of blood transfusion
required

Indications for laparotomy Stab or gunshot wounds that have
penetrated the abdomen Signs of peritonitis Unexplained shock Evisceration Uncontrolled haemorrhage Clinical deterioration during
observation

Liver Trauma – Surgical management Stop haemorrhage (Pringle) Remove dead or devitalised liver
tissue Ligate or repair damaged blood
vessels and bile ducts

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:783-785
Stellate fracture of right lobe of the liver

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:783-785
Packing of bleeding liver

Postoperative Complications Rebleeding from injury Bile leaks Ischaemic segments of the liver Infected fluid collections

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:783-785
Large intrahepatic haematoma in patient with blunt trauma

Liver Trauma - Prognosis Overall mortality 10-15 % Mortality after blunt trauma > 20
% If three major organs are injured
mortality approaches 70 %

Pyogenic liver abscess – typical features Right upper quadrant pain and
tenderness Nocturnal fevers and sweats Anorexia and weight Raised right hemidiaphram in
chest radiograph Raised white cell count with mild
anaemia

Origins and causes of pyogenic liver abscess Biliary tract – Gall stones,
cholangiocarcinoma, strictures Portal vein – Appendicitis, diverticulitis,
Crohn‘s disease Direct extension of: Gallbladder empyema Trauma Iatrogenic – Liver biopsy, blocked biliary
stent

Microbiology E. coli, Klebsiella pneumoniae,
bacteroides, enterococci Fungal or opportunistic organisms
due to immunosuppression as a result of AIDS, intensive chemotherapy and transplantation

Copyright ©2001 BMJ Publishing Group Ltd.
Krige, J E J et al. BMJ 2001;322:537-540
Chest radiograph showing air-fluid level and raised right hemidiaphragm in pyogenic liver abscess

Treatment Antibiotics – Penicillin,
aminoglycoside (or cephalosporin), metronidazole
Treatment for two to four weeks depending on the clinical response

Drainage requirements for liver abscesses None – multiple small abscesses
that respond to antibiotics Percutaneous aspiration –
abscesses <6cm Percutaneous catheter drainage –
abscesses >6cm

Drainage requirements for liver abscesses – Open surgery Failed percutaneous drainage Very large or multilocular
abscesses Associated intra-abdominal
infection requiring surgery such as bile duct stones

Copyright ©2001 BMJ Publishing Group Ltd.
Krige, J E J et al. BMJ 2001;322:537-540
Computed tomogram showing multifocal liver ascess in segment IV. Note drain in segment VII

Amoebic liver abscess - Epidemiology About 10 % of the world‘s
population is chronically infected with Entamoeba histolytica
Amoebiasis is the third commonest parasitic cause of death, surpassed only by malaria and schistosomiasis

Symptoms of amoebic liver abscess Pain Enlarged liver with maximal tenderness
over abscess Intermittent fever with night sweats Weight loss Nausea Vomiting Cough Dyspnoea

Amoebic liver abscess - Diagnosis Serological tests Stool may contain protozoal cysts Abscess usually solitary – right
lobe in 80% of cases Abscess contains sterile pus and
reddish-brown liquefied necrotic liver tissue

Amoebic abscess - Treatment 95 % resolve with metronidazole
alone (800 mg three times a day for five days)
After the abscess – diloxanide furate 500 mg, eight hourly for seven days to eliminate intestinal amoebae

Amoebic abscess - Surgery Surgical drainage is required only
if the abscess has ruptured causing amoebic peritonitis

Hydatid disease - Presentation Liver enlargement Right upper quadrant pain Rupture of the cyst into the
peritoneal cavity –urticaria, anaphylactic shock, eosinophilia
Erosion into bile duct – jaundice, cholangitis

Copyright ©2001 BMJ Publishing Group Ltd.
Krige, J E J et al. BMJ 2001;322:537-540
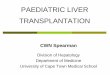
Lifecycle of Echinococcus granulosus

Hydatid disease – Diagnosis Ultrasonography, computed
tomography Serological tests ERCP

Copyright ©2001 BMJ Publishing Group Ltd.
Krige, J E J et al. BMJ 2001;322:537-540
Computed tomogram showing hydatid cyst: daughter cysts containing hydatid larvae are visible within the main cyst

Copyright ©2001 BMJ Publishing Group Ltd.
Krige, J E J et al. BMJ 2001;322:537-540
Operative specimen of opened hydatid cyst showing multiple daughter cysts

Hydatid disease – Treatment I Surgery – 1. Aspiration of cysts and
replacement by a scolicidal agent such as 0.5% sodium hypochlorite
Surgery - 2. The cysts are carefully shelled out by peeling the endocyst off the host ectocyst layer along ist cleavage plane

Hydatid disease –Treatment II Bile leakages are sutured The cavity is drained and filled
with omentum Liver resection seldom necessary Albendazole is given for two weeks
postoperatively

Liver tumours Cysts Benign tumours – Haemagiomas,
liver cell adenoma, focal nodular hyperplasia
Malignant tumours – Hepatocellular carcinoma, metastatic tumours

Characteristics of simple cysts Thin walled Contain clear fluid Contain no septa or debris Surrounded by normal liver tissue Usually asymptomatic Present in 1 % of population

Liver cysts Treatment only when symptomatic –
usually laparoscopic cyst fenestration NOTE - Thick walled cysts and those
containing septa, nodules or echogenic fluid may be cystic tumours
Cystic dilatations of the bile ducts (Caroli‘s disease) are premalignant (cholangiocarcinoma)

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Polycystic liver disease

Haemangiomas Incidence 3 % Malignant transformation and
spontaneous rupture are rare Diagnosis by contrast enhanced
computed tomography Resection is indicated only for
large symptomatic tumours

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
T2 weighted magnetic resonance image of large benign haemangioma

Liver cell adenoma Predominantly in women of
childbearing age Risk of rupture 10 % Risk of malignant transformation
10 % Liver resection necessary

Focal nodular hyperplasia Usually asymptomatic Not premalignant It does not require treatment
unless symptomatic Sometimes diagnosis difficult to
establish – histology should be determined by surgical resection

Hepatocellular carcinoma Commonest malignant tumour
worldwide One million new cases a year
worldwide 80 % occur with cirrhotic livers Established viral infection – 10 years
to develop chronic hepatitis – 20 years to develop cirrhosis – 30 years to develop carcinoma

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Distribution of hepatocellular carcinoma

Hepatocellular carcinoma Ultrasonography Alpha fetoprotein >500 ng/ml Surgical resection feasible in less
than 20 % of patients Average operative mortality is 12
% in cirrhotic patients 5-year survival 15 %

Hepatocellular carcinoma <5 cm tumours – LTX Contraindication to LTX – alcohol
injection, radiofrequency ablation Larger tumours – transarterial
embolisation with lipiodol and cytotoxic drugs (cisplatin or doxorubicin)

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Large hepatocellular carcinoma

Colorectal liver metastasis 8-10 % of patients undergoing
curative resection of colorectal tumours have isolated liver metastasis suitable for liver resection
5-year survival after resection 30 %

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Solitary liver metastasis in segment IV

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Inoperable extensive liver metastasis

Liver resection A fit patient with a healthy liver will
regenerate a 75 % resection within three months
Segmental anatomy with each of the eight segments supplied by ist own branch of the hepatic artery, portal vein and bile ducts (Couinaud 1957)
Mortality 5 %

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Couinaud’s segmental anatomy of the liver

Copyright ©2001 BMJ Publishing Group Ltd.
Beckingham, I J et al. BMJ 2001;322:477-480
Intraoperative view after left hepatectomy – raw surfaces of liver are coated with fibrin glue after resection to aid hemostasis and
prevent small bile leaks

Liver transplantation - Indications Primary biliary cirrhosis Primary sclerosing cholangitis Cryptogenic cirrhosis Chronic active hepatitis (Hep B and
C) Alcoholic liver disease (after a
period of abstinence)

Timing of LTX – Signs of decompensations Tiredness, Ascites, Encephalopathy Peripheral oedema Jaundice Spontaneous bacterial peritonitis Bleeding oesophageal varices Low albumin concentration Raised prothrombin time

Acute liver failure – Paracetamol overdose Renal failure develops as a
hepatorenal syndrome Early deaths result from raised
intracranial pressure Death in later stages – multiorgan
failure and systemic sepsis Mortality from fulminant liver
failure can be as high as 90 %

Copyright ©2001 BMJ Publishing Group Ltd.
Prasad, K R et al. BMJ 2001;322:845-847
Implantation of liver transplantation after hepatectomy

Immunosuppressive drugs Cyclosporin Tacrolimus Azothioprine Mycohenolate mofetil Steroids

Copyright ©2001 BMJ Publishing Group Ltd.
Prasad, K R et al. BMJ 2001;322:845-847
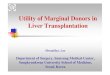
One year survival after first liver transplant according to primary disease, UK 1985-94
Recommended