“Transcranial direct current stimulation (tDCS) – A general purpose
neuromodulator?”Dan Ofer.
Hebrew University of Jerusalem.
21.9.2013
Introduction:
The goal of this paper is to present transcranial direct current stimulation (tDCS)
and to argue that it is a general modulator of neuronal excitability and plasticity, as
evidenced by the extremely diverse mental functions and neuroanatomical regions
affected by tDCS in varied studies. This, as opposed to being specific to only a single
domain, cortical network, region or mental function. Towards this argument, I shall
present a wide array of different cortical regions and effects modulated in tDCS
experiments.

‘What is tDCS?’
Transcranial direct current stimulation (tDCS) is a form of non-invasive external
electric stimulation of the cortex. It works via a weak electrical current (typically 0.5-2
mA) passed between electrodes attached to the scalp, polarizing the underlying brain’s
cortex tissue with an electrical field.
(The following wording is adapted from reviews1–4): "tDCS can modulate
cortical excitability and spontaneous firing activities in the stimulated region by shifting
the resting membrane potential, thus altering the ‘intrinsic’ neuronal excitability.
Depending on the polarity of the current flow, cortical excitability can be increased via
anodal stimulation or decreased via cathodal stimulation. "
tDCS induces cortical and neural plasticity via subthreshold polarization of the neuronal
membrane via weak direct electrical currents and induced electric fields.5–7
tDCS’s Physical Basis - “What it Does”:
In terms of its relationship to neuroelectric activity, tDCS is a neuromodulator –
it alters excitability, increasing or decreasing the threshold of excitation and thus the
firing rate and activity of affected neurons. However, it does not cause neurons to fire
"independently"; that is, it modulates existing activity but does not induce
“independent” firing. In contrast, in TMS (Transcranial Magnetic Stimulation) or
electric shocks 40, “resting” or non-active neurons are induced to fire, independently of
“natural” activity because (static) electrical fields in this range do not yield the rapid
depolarization required to produce action potentials in neural membranes 2. The effects

of tDCS on cortical excitability can last for a varying amount of time8, depending on the
region affected, the function involved, and the strength and duration of the tDCS
stimulus itself.
Hence, tDCS is a neuromodulatory intervention. The tissue is polarized9 and
tDCS modifies spontaneous neuronal excitability and activity by depolarization or
hyperpolarization of the resting membrane potential (Vmr)”.
The extent of tDCS's effect depends on a number of factors2:
i. Current density (dependent on current strength and the size of the electrode).
This determines the strength of the induced electrical fields. It has been shown that
higher current densities result in stronger effects10–14.
ii. Duration - Longer stimulus' durations (all other factors being equal) determine
the occurrence and duration of effects in humans and animals2,14–20. It should be noted
that there can be significant differences in effects in cases where tDCS ‘treatments’ are
spaced out at intervals, rather than a single exposure2,3,20–23. Multiple spaced exposures
tend to have longer lasting and more potent effects than a single exposure 3,24. However,
the mechanisms underlying these changes are not well understood, as is any possible
relation to long term potentiation [LTP].25,26 It is currently unknown whether using
spaced intervals would result in greater (or longer lasting) effects for other studied
phenomena. The exact underlying differences between effects that last for days, weeks,
months or hours are as yet unknown.
iii. Orientation of the induced electric field set by the electrodes’ positions and
polarity (Anodal or Cathodal stimulation). The positioning determines the areas of the

cortex affected by the current flow and the induced electric field, while the polarity
determines the effect (increased or decreased excitability due to ‘depolarization’ or
‘hyperpolarization’ respectively).
(3:)“Early studies in animals15,27 […] using direct cortical stimulation showed
that if the anode was placed above or within the cortex, spontaneous neuronal activity
was increased, whereas cathodal polarity resulted in reduced spontaneous unit
discharges due to subthreshold changes in membrane polarization. […] However,
neurons throughout the cortex were not modulated in a homogenous manner. […]
different subpopulations of neurons appear to have different thresholds for
modulation.27”
It must be noted that the mechanisms underlying the changes in cortical
excitability induced by tDCS are different for those effects seen during stimulation and
those induced after the stimulation has stopped 3 – meaning, that there are differences in
the physiological effects and underlying facilitating mechanisms involved, depending on
the timeframe i.e. - during or after the tDCS stimulation.
“Effect of tDCS on Neurons during Stimulation: ∆Vmembrane”
(3:)“The effects of anodal {= increased excitability9} tDCS during stimulation
appear to be solely dependent on {depolarizatory} changes in membrane potential”. This
was established by Nitsche et al6, using pharmacological methods (flunarizine and
carbamezipine) that blocked calcium 105 (Ca2) or sodium (Na+) channels, reducing or
abolishing (respectively) the effects of anodal stimulation for the treated neurons. 9

During cathodal stimulation, the reduction in excitability caused is seemingly
unhindered6 by calcium or sodium channel blockers, as would be expected3 if the
neuron’s membrane is indeed hyperpolarized by the cathodal tDCS.
NMDA and GABA receptor antagonists had no effect on the ‘immediate’ effects
of either anodal or cathodal tDCS, as would be expected from a shift in Vmembrane/the
resting membrane potential (as opposed to an effect exclusively dependent on synaptic
plasticity) 26,3,6,7
“After-effects of tDCS on Neurons post Stimulation:
The mechanisms involved in tDCS effects lasting after the stimulation has passed are
more complicated and less understood. Generally speaking, the effects of a single tDCS
stimulation can last for hours18,28 or longer, in the case of multiple ‘spaced’ treatments,
with some cognitive effects seen to persist for days or weeks after. 13,22,29–32
It seems that the long term effects are the result of GABAergic (for anodal tDCS1) and/or
glutamergic (ex: NMDA receptors) modulation, with a major component in lasting effects
being synaptic plasticity and interneurons.1,3,5,6,8,9,22.
It also appears that tDCS promotes changes in levels of brain-derived neurotrophic factor
(BDNF), an important element for neuronal proliferation and survival. 1, 100
To summarize, these match what might be expected from a neuromodulator, with
immediate stimulation causing a moderate shift in the neuron's membrane potential
(hyperpolarization or depolarization, depending on the polarity), but said ∆Vmembrane shift

is not sufficient in itself to induce neurons to fire spontaneously, or to prevent their
activity altogether.
However, it does affect the critical threshold of ‘input’ from external stimuli required in
order for the neuron to fire an action potential. In the ‘long run’, we would indeed expect
any lasting effects to be similar to those seen in ‘normal’ long term changes in plasticity,
but “accelerated” due to the facilitation of activity and thus excitability. We might as well
postulate as an extension of Hebb’s law that “Neurons that fire together wire together" 33,
that increased/”accelerated” or decreased firing of the functionally related neurons found
together in a network or region, would likely lead to an increase or decrease respectively
in the strength of the relevant intersynaptic and/or intra-network connections at a faster
rate than the baseline, possibly via theorized LTP/LTD like mechanisms1,26,34,,
“strengthening the neuronal synaptic connections and making them more efficacious”35
tDCS as a Research Tool
Recent years have seen tDCS reintroduced (study of the effects of electricity on
the brain is quite ancient) as a noninvasive research tool for altering neuroplasticity,
modulation of cortical function, neurorehabilitation, and in linking between behaviors &
mental functions to varied regions of the brain 65.
Its exponentially increasing popularity in recent years 92 is derived from a
number of characteristics 2: 1. Rapid effect. 2. Exact neuroanatomical targeting (as
opposed to pharmacological means), albeit at a relatively “coarse” scale. 3. Cheap. 4.
Relatively easy to use and safe. 5. Noninvasive and can be used in conjunction with
other tasks. 6. Flexibility – can be used to investigate an extremely large variety of brain
regions, behaviors and mental functions. 7. Potential uses in healthy subjects.

5,10,12,13,17,19,21–24,26,29–32,46,47,57,58,66,67,70,77,78,81,86,87,89,91,92 . 8. Ability to serve as a tool for linking
neuroanatomical regions to behavioral functions.37
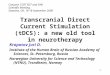
See Figure 1, supplementary material.
tDCS Effects on Mental Functions:
As mentioned in prior reviews, tDCS has been shown to have an effect on a very wide
range of mental functions and behaviors 1,2,3. In the following section, I shall present a
sampling of different effects, covering different behavioral and cognitive functions,
achieved using tDCS stimulation (anodal or cathodal, depending on the specifics) on
different neuroanatomical regions in humans, or different effects seen from stimulating
the same regions of the brain (in other studies which stimulated that region).
To reiterate, the overall goal of this paper is to argue that tDCS is a general
mental neuromodulator (via its modulation of neuronal excitability), rather than
being a “domain specific” effect 36 limited to only a single ‘modular’ a mental
function.
The majority of tDCS experiments focusedb on the prefrontal cortexc (PFC), the
dorsolateral prefrontal cortex region (dlPFC) and the motor cortexd, particularly the
a http://www.cognitiveatlas.org/concept/domain_specificity36
b Source: Probable association by Brainscanr, and overview of the review article, in particular 2.
http://www.brainscanr.com/Search?term_a=TDCSc This often includes, roughly speaking, the prefrontal (anterior and rostral) cortex itself (PFC),
the Orbitofrontal cortex (OFC) and dorsolateral prefrontal cortex (dlPFC).

primary motor cortex (M1). A number of other regions are also examined, in particular
the primary somatosensory cortex (S1) and visual cortex. 2
While most of the studies presented here focus on the effects on functions evoked
by tDCS, it must be noted that a major and growing use of tDCS is to infer the
involvement of neural regions in varied functions, such as for example; the role of the
cerebellum in verbal working memory37, or suppression of the non-dominant hand's
motor cortex by the M1 region controlling the dominant hand38,39. In the aforementioned
cases, this was investigated via inhibitory/cathodal tDCS on those regions in conjunction
with tasks involving the functions studied. Furthermore, in these studies, impairment of a
function following modulation of a neuroanatomical area, typically in the form of
cathodal tDCS "inhibition", is used as supporting evidence towards the hypothesis that it
does indeed play a role in the affected function, whether directly or indirectly.
The inclusion of a number of cortical structures and associated effects was
inspired by both articles2,3,24,26,40, and the brainSCANr engine (“Brain Systems,
Connections, Associations, and Network Relationships”).
http://www.brainscanr.com/Search?term_a=TDCS. 41
See Figure 2 & 3, supplementary material.
Motor Cortex Studies:
tDCS studies involving the motor cortex have shown potentially beneficial effects which
can be attained using tDCS even in healthy individuals42. The primary motor cortex (M1)
d This includes the primary motor cortex (M1), the premotor cortex, and supplementary
motor cortex

is a popular target in studies involving motor learning due to its suspected role in the
initial ‘encoding’ of motor skills (‘initial formation of memory’)43, 24, the relative ease of
quantifying results, and its being one of the earliest most studied areas in the field14,27,44.
M1 modulation may also affect other areas such as the premotor cortex 24,45,46. In addition,
there is a distinction24 between learning new motor skills and improving performance of
existing motor skills'.10,24,42,47 Review and meta-analysis studies have shown that anodal
tDCS increased corticomotor excitability.10,24
In regards to (lasting) effects; “tDCS produces lasting effects in the human motor cortex.
These are stable for up to about an hour if tDCS is applied for 9-13 minutes. Anodal
stimulation enhances, whereas cathodal tDCS diminishes excitability, as measured by
motor-evoked potential (MEP) amplitude”2,18
Hand Motor Performance: A study of non-dominant hand motor performance and
control48, as measured with the Jebsen Taylor Hand Function Test (JTT), reported the
following:
Anodal (excitatory) tDCS stimulation of theM1 contralateral to the non-dominant hand,
(= the Left hemisphere, for the right handed subjects), resulted in “significant
enhancement of JTT performance after 1mA anodal tDCS of M1 (mean improvement of
9.41%), but not after sham” 48. The study reported improvement in the non-dominant
hand, but not the dominant hand. This seeming contradiction with other studies reporting
‘all-around’ improvement is explained by the fact that the JTT task examines motor
performance and control, rather than motor learning. As the author notes, the non-
dominant hand’s “governing” motor cortex region is characterized by having a higher

motor threshold and lower motor evoked potential [MEP], as a corollary to its relatively
lower intrinsic excitability48,49 compared to the dominant hand’s motor cortex.
Motor Learning: A number of studies have shown tDCS evoked enhancement of
motor learning, in both healthy and sick individuals. Reported results vary due to the
differences between tasks, the complexity of the tasks and stages of learning studied 24, as
well as possible methodological inconsistencies1,2 (for example, differences in: electrode
montage placement and electrical field orientation, stimulation duration, and current
strength).
Still, a number of studies16,24,26,38,39,42–46,48,50–53 have shown improvements in motor
learning and/or rehabilitation with tDCS stimulation. A typical example is a study of non-
dominant hand motor function enhancement via (unilateral) anodal stimulation of the
contralateral motor cortex 24,44,51, or/and47,53 inhibition of the ‘opposing’ hemisphere’s
motor cortex via cathodal stimulation.38
The wide range of effects, most of which showed “improvements” (as measured
by varying criteria) include better results in recovering motor skills among stroke
patients10,47,50,54, enhanced retention of motor skills, 44,51 , the previously mentioned
effects24 on (non-dominant) hand motor skills' performance 38,39,48,54, implicit motor-
sequence learning24,44,35, modulation of long term motor memory, implicit and procedural
skills learning, retention and consolidation 3,55,104, explicit sequence learning (in a bilateral
stimulation experiment) 53, increased “practice-dependent plasticity” i.e. magnitude and
duration of newly acquired motor memories51 and visuomotor tracking/coordination task
performance following a-tDCS stimulation of the contralateral M1 or extrastriate visual
cortex area MT+/V5 (but not of the primary visual cortex) 52

Motor Studies Discussion:
To summarize, the overall consensus 42, 20 would seem to be that “tDCS {is} […]
capable of inducing lasting improvements in motor function. […and] has shown
preliminary success in improving motor performance and motor learning in healthy
individuals, and restitution of motor deficits in stroke patients.”42
An aspect worthy of reemphasis is the two types of functional enhancements seen
in the aforementioned studies (and the following section):
(1) Immediate ‘performance’ enhancement; for example, increased dexterity and
control in the JTT test48 (these effects are seen in tasks where tDCS improves
performance, even without training56)
(2) ‘Faster/enhanced’ learning and/or plasticity, as seen in memory retention and
formation44,51, reconstruction of (motor) skills in stroke patients10,10,47,50,54,57, or effects seen
when tDCS is applied during training24,46,58.
The connection or causation between these two ‘effects', if there is one, is
unclear20,24,28, and requires further study beyond the scope of this work. While it might
seem likely that a positive link exists, evidence is currently sparse, with some negative
examples showing a negative correlation between the learning slope, reaction time and/or
accuracy or control26, 44.
In addition, some effects or changes might be network specific, or due to
stimulation of ‘competing’ or inhibiting neighboring regions, thus impacting various
performance criteria for some tasks, but not others. For example, cathodal stimulation of
the opposing hemisphere-motor cortex region, rather than anodal stimulation of the

contralateral M1 hand region, has a similar but not identical facilitatory effect 47,53,56,59.
Repeating previous experiments with fresh experimental paradigms may well add new
insight to this issue. These measures might include: ±Left/Right/dual hemisphere
stimulation × ±anodal × ±cathodal, larger samples, different tasks (measuring the learning
or performance rates improvements, increases above the ‘baseline’ and retention),
uniform stimulation intensity/current strength2 and improved neuroanatomical resolution
via new “high definition tDCS” techniques5 which allow stimulation of smaller, more
focused regions.
Cognitive Studies:
A great many tDCS studies on higher mental functions or cognitive effects have
focused on stimulation or suppression of the prefrontal cortex (PFC) and its connected
regions, especially the dorsolateral prefrontal cortex (dlPFC)30,60 and the orbitofrontal
cortex (OFC)61–63. Interest in these regions is primarily due to their suspected roles in the
‘highest’ mental and cognitive functions such as planning64, ‘executive functions64’,
working memory [WM]20,30,32,65–68, behavioral regulation69 and decision making62,70–72; the
most “advanced” and ‘intellectual’ mental functions that we possess as “intelligent”
beings.
A diverse array of mental functions show potential for modulation by tDCS.
Many even show ‘enhancement’ – i.e. improvement beyond the baseline in healthy
individuals. Among the best established and most documented of tDCS evoked effects is
‘improved’ WM, via anodal-tDCS [a-tDCS] stimulation of the dlPFC 26,30,32,66,67,73.

WM is the limited capacity storage system involved in the maintenance and
manipulation of information over short periods of time. WM plays a key role in a wide
rangee of higher order cognitive functions”74. WM is one of the few known
“transferable”75 elements of general or “fluid” intelligence76, with a wide array of
cognitive functions benefiting from it.74 It is typically measured using a n-back task30, and
is suspected to be malleable with training30,75,76.
Anodal {excitatory} tDCS stimulation [a-tDCS] over the dlPFC has been shown
to improve verbal and visuospatial32 working memory30,67,77, both in patients
(poststrokes24,32,54,65,75, Parkinson’s disease73 or Alzheimer’s disease78), and in
healthy30,32,66,67 or elderly12,78,79 adults. Stimulation of the left PFC is associated with verbal
WM17 and naming ability improvement, while a-tDCS of the right PFC is associated with
improving visuospatial WM. 32
Other cognitive effects:
Explicit motor learning as noted in the previous, motor section, with
dlPFC modulation was also seen to have an effect in some cases 24,78,80.
Improved retention, consolidation21,55,80 and reconsolidation23 of (verbal)
declarative memories17,21,26,77 , following unilateral-left dlPFC a-tDCS. At the same
time, M1 stimulation was not found to affect verbal memory performance77.
e Examples of WM associated functions:
http://www.brainscanr.com/Search?term_a=working+memory

Anecdotally, strongly reported positive feelings of improved focus,
clarity29, concentration29,81 and a state of “flow”82,40,83 (flow is “a state of
concentration or complete absorption with the activity at hand and the
situation.”84).
The aforementioned effects make tDCS a potential tool for ‘speeding up’
learning,2,51,58,67,77,82,83,85,29,40, in a variety of real world tasks 86.For example, training
for “complex threat detection”, found a 2.3 fold improvement in the training time
required, via improved alertness-attentional control81, following a-tDCS of the
right inferior frontal cortex during training29. The difference between the test and
‘sham’ groups was retained for over 24 hours after the training ended.
Creativity and novel-insights 87: participants who underwent cathodal
stimulation of the left anterior temporal lobe (ATL) together with anodal
stimulation of the right ATL were three times as successful at solving an
insight/creativity task (“matchstick arithmetic”) compared to a control group
(reversing the hemispherical A/C stimulation showed less of an effect, possibly
due to a “ceiling effect”, reminiscent of the aforementioned M1 hand studies).48
“Long-lasting changes in numerical competence”: in this study, healthy
adults were stimulated via tDCS while learning artificial numerical valuesf. They
were later tested for “numerical competency”. The group which had anodal and
cathodal tDCS stimulation to the right and left (respectively) parietal lobes during
training showed “better and more consistent performance in both numerical tasks”
f They were stimulated for 20 minutes at the start of the 90-120 minute learning phase. They
were not stimulated during the testing.

compared with the control group. Interestingly, six months after the experiment,
that group still showed improvement. Another group with ‘reversed’ stimulation
polarity showed reduced performance. The training derived effect was seemingly
task-specific, with performance in the tasks using normal numbers not showing
change. 22
Inhibitory control of voluntary actions was enhanced or impaired via a-
tDCS or cathodal tDCS (respectively) to the pre-supplementary motor area. 106
Verbal & Lingual abilities: in addition to the aforementioned effects of left dlPFC a-
tDCS on verbal working memory, other studies have shown that:
o A-tDCS over the right temporal-parietal cortex combined with language
training significantly improved naming ability in patients suffering from chronic
anomic aphasia (severe problem with recalling words or names)88.
o a-tDCS of the left posterior perisylvian region (included Wernicke's area)
in healthy subjects, during a “visual picture naming task” also showed
significantly faster and equally accurate naming responses following
stimulation.89
o Cathodal tDCS over the Cerebellum impairs verbal working memory37,
implying cerebellar involvement in the function (excitatory/a-tDCS was not
tested).
o dlPFC a-tDCS affects “long term” verbal memory consolidation17 (initial
memorization) and reconsolidation23,23 (renewed consolidation/storing of a

memory following its retrieval), with both showing ‘enhancement’ i.e. Improved
speed and recognition accuracy when tested on verbal memories17.
o A-tDCS over Broca’s area was shown to enhance “implicit learning of an
artificial grammar”. 90 The effects were seen to be specific to rule-based
knowledge of the artificial grammar and detection of “syntactic violations” and
were not the result of differences in W M.
A-tDCS stimulation of the auditory cortex was found to improve the
abilities of healthy subjects in “temporal auditory processing abilities”, as
measured by the subjects’ ability to discern auditory temporal resolution. Cathodal
tDCS reduced performance compared to the control group.91
tDCS experiments with aged, healthy subjects have shown “reversal” of some age-
related impairments in mental abilities to a more ‘youthful’12 state92. Known effects
include:
Right temporoparietal cortex stimulating leading to improved object-location learning
(learning the positions of buildings on a street map), with improved recall lasting for at
least one week93. M1 stimulation affecting acquisition of complex motor skills, lasting for
over 24 hours 94. Age related hyperactivity in a number of neural networks involved in
semantic word generationg was notably ‘reduced’ with improved task performance,
following a-tDCS of the left inferior frontal gyrus.12
g This included the PFC and anterior cingulate gyrus

Other age related declines have been noted to be ‘alleviated’ by tDCS in studies
focusing on patients suffering from Alzheimer’s disease (for example, object
recognition).78,92
Additional Behavioral Effects:
Cathodal tDCS over M195 or primary somatosensory cortex (S1) has been
shown to reduce induced pain sensations/nociception. 96
dlPFC tDCS stimulation has also been found to reduce ‘craving’ for
specific foods97 and alcohol98, to alter probabilistic thinking 68, probabilistic
forecasting (switching between frequency matching and expectancy maximization
strategies70) and risk-taking ('risk-appetite') behavior71,72.
Polarization of the visual or parietal cortexes modulates the threshold for
motion or tactile perception, respectively (i.e – increased or reduced sensitivity).
101-103
tDCS applied during slow wave sleep affects verbal declarative memory,
improving retention of 'word pairs'21, and also facilitates "sleep dependent
consolidation" of procedural motor memories – enhancing retention
(consolidation) of these none-declarative memories 94,92. Different sleep frequency
bands were also affected 21.
Discussion
tDCS has a number of different modulatory effects on various mental, cognitive,
behavioral and neurobiological processes.. It is capable of inducing modulatory changes
in many different systems, and neural regions 1. tDCS induced physiological changes may

result in both local and distant changes in excitability, inhibition and potentially changes
in plasticity (local or synaptic).
The effects underlying the immediate or lasting effects involved in tDCS, and the
changes derived from and affected by it cannot be simplified narrowed down to only one
basic mechanism such as ’reduced dopamine reuptake‘ or ’spontaneous motor activity
induced by strong electrical shocks of the motor nerves‘.
As has been noted here previously, effects differ in regards to:
i) The mental, behavioral or cognitive functions affected. Effects modulated
include declarative memory 21,77, motor performance and control 38,39,48,
consolidation 55,104 and reconsolidation 23,24 of memories, attentional
control 56,81, visual and tactile-sensory perception and sensitivity 56,101,103,
visuomotor tracking 52,101, working memory 30,32,37,66,67, risk appetite
behavior 70-72, cravings 97,98, creativity 87, planning ability19 , language and
artificial grammar rule-learning90-92, and the many other effects previously
listed in both this text and existing literature 1-3,92.
ii) The cortical area(s) affected:1-3. Stimulation of different regions of the
brain can affect the same functions and/or different functions, depending
on the areas, their roles and the functional network involved in a function.
Given examples include: WM modulation via the cerebellum 25,37 or
dlPFC, and involvement of both M1 and the PFC in implicit learning of
motor skills 20,30,35,39,42,45,48,51. This as opposed to tasks found to be
unaffected by stimulation of one of the ‘generally involved’ areas (V1,
M1, dlPFC in the case of motor related tasks), in cases such as task-
specific differential effects on task switching performance 46 or visuomotor
tracking 52,101.
iii) While most investigated functions can be impaired, usually but not
exclusively, by cathodal tDCS, far fewer functions can be “enhanced”. For
example, dominant hand motor performance in healthy individuals, (at
least in existing studies) 48.

That said, a large number of effects show enhancement in healthy
adults10,19,24,38,67,68,70,87,89 or improved restoration (sometimes when combined with training
74,88) towards healthy or normal levels in the case of the elderly 92-94, post-stroke patients
47,50,54,65,and Alzheimer's or Parkinson's disease's patients 73,78.
These effects typically involve: A) broad, trainable ("training dependent plasticity" =
interactions between training with or without tDCS) mental functions such as WM 74-76 or
other effects of ‘executive planning' and so called 'higher mental functions' 56,58,80-87.
B) The other type that seems most 'amenable' to 'enhancement' are functions controlled
by regions which have deteriorated and have reduced plasticity or excitability. Examples
include age related decline in cognition and mental capabilities. tDCS has been shown
temporary reversal of many of the aforementioned age related symptoms or connectional
characteristics 12,92-94 and enhancement of motor control and performance in the non-
dominant hand38 (which is theorized to be 'suppressed' by the dominant hand 49). In all
these cases, the tDCS "resets" excitability towards what is likely the 'healthy baseline'.
What exactly determines if a function can be enhanced, with or without training
or enhanced in a lasting, training dependent or independent fashion29,40,56,58,83, is beyond
the scope of this work, save for speculation.
i) The duration of effects after the stimulation has ended can vary
immensely, both in regard to the post-immediate effects following the end
of the stimulation (typically occurring over hours 14,15,18,34), and in regards
to the duration of the functional changeswhich can persist for days 29 or
even months! 19,22 Multiple mechanisms are possibly involved in such long
lasting effects, likely including (but not necessarily identical to) neural
and/or synaptic plasticity 1,28,100 + LTP and/or LTD like effects 1-3,6,7,27,28,
modulation of GABA, Glutamate and/or NMDA receptors1,6,7,13,105,106-108,
involvement of regulation/effects from related neural networks 1,3,107 and
regulatory factors, such as BDNF 100.
ii) The numerous cases of left/right specificity of effects, not just for motor
effects 39,42,53 but also for abstract mental functions (such as declarative
verbal memory77 or working memory67) is somewhat peculiar. Perhapsthis

might prove to be an artifact of current leakage affecting surrounding
structures or shared inhibitory interneuronal networks, with bilateral a-
tDCS+ cathodal tDCS inadvertently focusing the effects to sub-structures.
Claims of tDCS being domain specific or a modulator of only a single effect
appear invalid, given the numerous listed examples of different effects for different
regions, and the wide range of effects.
Modulation of WM and attention could possibly have an influence on a number of
the effects 60,74,76 and possibly even some of the behavioral effects, such as reduced risk
appetite behavior being a consequence of improved probabilistic thought/numerical
competency, and that being somehow derived from a boost to WM – but it still fails to
explain all the dlPFC related effects (cravings97,98 for example), and completely fails at
explaining effects evoked from stimulation of regions remote from the PFC. Still, the
possibility of WM as an underlying 'cause' behind many known cognitive and behavioral
effects seen as a result of imprecise/"conventional"5 tDCS currents applied to the dlPFC
'leaking' is an interesting one, and could easily be investigated as a confounding effect via
testing for changes in WM using an n-back test, and examining the r-Pearson's correlation
for WM changes relative to whichever effects are being primarily examined.
The possibilities for further research are vast. A number of interesting questions
include: what other cognitive effects show lasting changes (relative to a control group)
for weeks or months following tDCS stimulation? Are any such effects training
independent (all given examples of long lasting effects have involved training88, albeit
with differential effects seen for novices in some cases 86)? Can effects from different
brain regions or networks "overlap" in an additive manner? (For example, this is
examinable via simultaneous a-tDCS of the dlPFC and other areas known to be involved
in a task, and comparison of results to see if interaction or additive effect(s?) exist).
Stimulation of novel areas and investigation at higher resolutions for which regions
within structures are involved in modulation of functions associated with the entire region
(sub-regions of the dlPFC and WM for example).

The potential "real world" uses are known, in particular for rehabilitation 2,16,50,65,
but the potential use as a so called "thinking cap"87 for healthy individuals is even more
exciting. Studies have already taken place in the real world with healthy individuals 29,40,81,82,83, but more are needed to help establish the generalizability of the potential
effects, to help establish the safety of long term use 2,11 and optimize parameters for such
usage (in terms of electrode orientation and location, current intensity and 'side-effects' 99). Two interesting ways to test this, with a large study group of healthy adults, would be
to try the following: i) A study of the effects of a-tDCS on language learning; given
stimulation of a combination (requiring an additional 'additive' experiment to establish
the most effective combination) of Broca's area, Wernicke's area and/or the dlPFC. This
could be applied in conjunction with an existing language course, or even a
code/programming language course. ii) Another idea is a-tDCS of the dlPFC, and/or the
anterior temporal lobes ("insight facilitation"87) with volunteers in an academic
environment, such as a theoretical training course or academic class, applied at the
midpoint of a course, so as to observe the effects on learning 40,82,83. Given such a large
group (even a sub-section of volunteers from one), any effects in grades or improvements
for the non-sham group can be easily compared to the rest of the class, and their own
previous performance.
This would be an excellent way to test applicability and potentially enhancing effects
with a large group of healthy subjects, and would not be overly expensive given the
relative simplicity and compactness of a basic tDCS kit. This would help in testing the
effects in challenging, noisy environments with a focus on uses that would have far
reaching implications for healthy people, while the large test groups would help in
establishing effects, as opposed to the large number of existing experiments with their
small sample sizes, a fact that makes rigorously testing something with multiple A/B/C
combinations statistically problematic. This could have obvious benefits 87 for
‘consumers’, with the added benefit of massively expanding the data available for use in
future rehabilitative or restorative92 studies, as well as other studies in the field, such as
examining neuroanatomical networks or the long term effects (and side-effects99).

Conclusion
tDCS modulates neural excitability1,2,6, increasing calcium levels at site of anodal
stimulation 5,7,92, altering the 'resting' electrical potential of neurons' membranes 1,3,14,27 ,
and possibly changing neuroplasticity and/or synaptic plasticity via inducing LTP or LTD
like changes6,34,38. Anodal tDCS creates an electric field, inducing a slight depolarization,
increasing the intrinsic excitability of neurons while cathodal tDCS decreases neuronal
excitability due to hyperpolarization. The after-effects of both anodal and cathodal tDCS
are influenced by glutamatergic receptors 1,3,6,7, and a-tDCS is influenced by "GABAergic
neurotransmission via interneurons" 92,106.
tDCS has been shown to affect a heterogonous array of different mental, behavioral,
cognitive and neurobiological functions. The mental and behavioral effects of tDCS
depend on the stimulation's parameters, cortical region(s) stimulated, the mental function
itself, and possible interactions with other factors, such as damage (in the case of
strokes), or decline (in the case of age related decline). Not all effects can be "enhanced"
beyond baseline abilities, and not all such effects (whether "enhancing" or "inhibitory")
are retained after the stimulation has ceased, though some tDCS-evoked effects may
persist for months. Some capabilities are "enhanced" (during stimulation) via increased
intrinsic excitability, while others benefit from cathodal tDCS reducing "noise"30.
tDCS should not be regarded as affecting only a single effect, function or region,
but rather as a general purpose neuromodulator that has different effect depending on the
variables at play, in particular the region of the brain stimulated, the polarity of the
induced electrical field, the mental or behavioral function involved and the time-period of
the stimulation.

I wish to thank everyone who helped with this paper, in particular my friends and
family, and my academic advisor.

Bibliography:
1. Medeiros, L. F. et al. Neurobiological effects of transcranial direct current stimulation: a review. Frontiers in psychiatry / Frontiers Research Foundation 3, 110 (2012).
2. Nitsche, M. a et al. TDCS: State of the art 2008. Brain stimulation 1, 206–23 (2008).
3. Stagg, C. J. & Nitsche, M. A. Physiological basis of transcranial direct current stimulation. The Neuroscientist: a review journal bringing neurobiology, neurology and psychiatry 17, 37–53 (2011).
4. Dhawale, A. K., Hagiwara, A., Bhalla, U. S., Murthy, V. N. & Albeanu, D. F. Non-redundant odor coding by sister mitral cells revealed by light addressable glomeruli in the mouse. Nature neuroscience 13, 1404–12 (2010).
5. Kuo, H.-I. et al. Comparing cortical plasticity induced by conventional and high-definition 4 × 1 ring tDCS: A neurophysiological study. Brain stimulation 1–5 (2012). doi:10.1016/j.brs.2012.09.010
6. Nitsche, M. A. et al. Pharmacological modulation of cortical excitability shifts induced by transcranial direct current stimulation in humans. The Journal of physiology 553, 293–301 (2003).
7. Liebetanz, D. Pharmacological approach to the mechanisms of transcranial DC-stimulation-induced after-effects of human motor cortex excitability. Brain 125, 2238–2247 (2002).
8. Nitsche, M. a et al. MRI study of human brain exposed to weak direct current stimulation of the frontal cortex. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology 115, 2419–23 (2004).
9. Stagg, C. J. et al. Polarity-sensitive modulation of cortical neurotransmitters by transcranial stimulation. The Journal of neuroscience: the official journal of the Society for Neuroscience 29, 5202–6 (2009).
10. Bastani, A. & Jaberzadeh, S. Does anodal transcranial direct current stimulation enhance excitability of the motor cortex and motor function in healthy individuals and subjects with stroke: a systematic review and meta-analysis. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology 123, 644–57 (2012).
11. Bikson, M., Datta, A. & Elwassif, M. Establishing safety limits for transcranial direct current stimulation. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology 120, 1033–4 (2009).
12. Meinzer, M., Lindenberg, R., Antonenko, D., Flaisch, T. & Flöel, A. Anodal transcranial direct current stimulation temporarily reverses age-associated cognitive decline and functional brain activity changes. The Journal of neuroscience: the official journal of the Society for Neuroscience 33, 12470–8 (2013).
13. Zheng, X., Alsop, D. C. & Schlaug, G. Effects of transcranial direct current stimulation (tDCS) on human regional cerebral blood flow. NeuroImage 58, 26–33 (2011).

14. Nitsche, M. A. & Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. The Journal of physiology 527 Pt 3, 633–9 (2000).
15. BINDMAN, L. J., LIPPOLD, O. C., REDFEARN, J. W. & Bindman LJ, Lippold OCJ, R. J. The action of brief polarizing currents on the cerebral cortex of the rat (1) during current flow and (2) in the production of long-lasting after-effects. J Physiol 172, 369–382 (1964).
16. Brunoni, A. R. et al. Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain stimulation 5, 175–95 (2012).
17. Javadi, A. H., Cheng, P. & Walsh, V. Short duration transcranial direct current stimulation (tDCS) modulates verbal memory. Brain stimulation 5, 468–74 (2012).
18. Nitsche, M. A. & Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 57, 1899–901 (2001).
19. Dockery, C. A., Hueckel-Weng, R., Birbaumer, N. & Plewnia, C. Enhancement of planning ability by transcranial direct current stimulation. The Journal of neuroscience: the official journal of the Society for Neuroscience 29, 7271–7 (2009).
20. Grimaldi, G. et al. Non-invasive Cerebellar Stimulation-a Consensus Paper. Cerebellum (London, England) (2013). doi:10.1007/s12311-013-0514-7
21. Marshall, L., Mölle, M., Hallschmid, M. & Born, J. Transcranial direct current stimulation during sleep improves declarative memory. The Journal of neuroscience: the official journal of the Society for Neuroscience 24, 9985–92 (2004).
22. Cohen Kadosh, R., Soskic, S., Iuculano, T., Kanai, R. & Walsh, V. Modulating neuronal activity produces specific and long-lasting changes in numerical competence. Current biology: CB 20, 2016–20 (2010).
23. Javadi, A. H. & Cheng, P. Transcranial direct current stimulation (tDCS) enhances reconsolidation of long-term memory. Brain stimulation 1–7 (2012). doi:10.1016/j.brs.2012.10.007
24. Reis, J. et al. Consensus: “Can tDCS and TMS enhance motor learning and memory formation?”1, 363–369 (2009).
25. Ferrucci, R. & Priori, A. Transcranial cerebellar direct current stimulation (tcDCS): Motor control, cognition, learning and emotions. NeuroImage, (2013).
26. Brasil-Neto, J. P. Learning, memory, and transcranial direct current stimulation. Frontiers in psychiatry / Frontiers Research Foundation 3, 80 (2012).
27. Purpura, D. P. & McMurtry, J. G. INTRACELLULAR ACTIVITIES AND EVOKED POTENTIAL CHANGES DURING POLARIZATION OF MOTOR CORTEX. J Neurophysiol 28, 166–185 (1965).
28. Ardolino, G., Bossi, B., Barbieri, S. & Priori, A. Non-synaptic mechanisms underlie the after-effects of cathodal transcutaneous direct current stimulation of the human brain. The Journal of physiology 568, 653–63 (2005).
29. Falcone, B., Coffman, B. A., Clark, V. P. & Parasuraman, R. Transcranial direct current stimulation augments perceptual sensitivity and 24-hour retention in a complex threat detection task. PloS one 7, e34993 (2012).

30. Mulquiney, P. G., Hoy, K. E., Daskalakis, Z. J. & Fitzgerald, P. B. Improving working memory: exploring the effect of transcranial random noise stimulation and transcranial direct current stimulation on the dorsolateral prefrontal cortex. Clinical neurophysiology: official journal of the International Federation of Clinical Neurophysiology 122, 2384–9 (2011).
31. Ferrucci, R. et al. Modulating Human Procedural Learning by Cerebellar Transcranial Direct Current Stimulation. Cerebellum (London, England) (2013). doi:10.1007/s12311-012-0436-9
32. Jeon, S. Y. & Han, S. J. Improvement of the working memory and naming by transcranial direct current stimulation. Annals of rehabilitation medicine 36, 585–95 (2012).
33. Hebb, D.. The Organization of Behavior. Hebb’s Law. (Wiley & Sons., 1949).34. Paulus, W. Outlasting excitability shifts induced by direct current stimulation of
the human brain. Supplements to Clinical neurophysiology 57, 708–14 (2004).35. Nitsche, M. A. et al. Facilitation of implicit motor learning by weak transcranial
direct current stimulation of the primary motor cortex in the human. Journal of cognitive neuroscience 15, 619–26 (2003).
36. Poldrack, R. A. et al. The cognitive atlas: toward a knowledge foundation for cognitive neuroscience. Frontiers in neuroinformatics 5, 17 (2011).
37. Boehringer, A., Macher, K., Dukart, J., Villringer, A. & Pleger, B. Cerebellar transcranial direct current stimulation modulates verbal working memory. Brain stimulation 6, 649–53 (2013).
38. Vines, B. W., Cerruti, C. & Schlaug, G. Dual-hemisphere tDCS facilitates greater improvements for healthy subjects’ non-dominant hand compared to uni-hemisphere stimulation. BMC neuroscience 9, 103 (2008).
39. Kidgell, D. J., Goodwill, A. M., Frazer, A. K. & Daly, R. M. Induction of cortical plasticity and improved motor performance following unilateral and bilateral transcranial direct current stimulation of the primary motor cortex. BMC neuroscience 14, 64 (2013).
40. Fox, B. Y. D. Brain buzz. (2011).41. Voytek, J. B. & Voytek, B. Automated cognome construction and semi-automated
hypothesis generation. Journal of neuroscience methods 208, 92–100 (2012).42. Reis, J. & Fritsch, B. Modulation of motor performance and motor learning by
transcranial direct current stimulation. Current opinion in neurology 24, 590–6 (2011).
43. Muellbacher W, Ziemann U, Wissel J, et al. Early consolidation in human primary motor cortex. Nature 640–644 (2002).
44. Cuypers, K. et al. Is Motor Learning Mediated by tDCS Intensity? PloS one 8, e67344 (2013).
45. Boros, K., Poreisz, C., Münchau, A., Paulus, W. & Nitsche, M. A. Premotor transcranial direct current stimulation (tDCS) affects primary motor excitability in humans. The European journal of neuroscience 27, 1292–300 (2008).
46. Leite, J., Carvalho, S., Fregni, F. & Gonçalves, Ó. F. Task-specific effects of tDCS-induced cortical excitability changes on cognitive and motor sequence set shifting performance. PloS one 6, e24140 (2011).

47. Fusco, A. et al. The ABC of tDCS: Effects of Anodal, Bilateral and Cathodal Montages of Transcranial Direct Current Stimulation in Patients with Stroke-A Pilot Study. Stroke research and treatment 2013, 837595 (2013).
48. Boggio, P. S. et al. Enhancement of non-dominant hand motor function by anodal transcranial direct current stimulation. Neuroscience letters 404, 232–6 (2006).
49. De Gennaro, L. et al. Handedness is mainly associated with an asymmetry of corticospinal excitability and not of transcallosal inhibition. Clinical neurophysiology?: official journal of the International Federation of Clinical Neurophysiology 115, 1305–12 (2004).
50. Khedr, E. M. et al. Effect of anodal versus cathodal transcranial direct current stimulation on stroke rehabilitation: a pilot randomized controlled trial. Neurorehabilitation and neural repair 27, 592–601 (2013).
51. Galea, J. M. & Celnik, P. Brain polarization enhances the formation and retention of motor memories. Journal of neurophysiology 102, 294–301 (2009).
52. Antal, A. et al. Facilitation of visuo-motor learning by transcranial direct current stimulation of the motor and extrastriate visual areas in humans. The European journal of neuroscience 19, 2888–92 (2004).
53. Sehm, B., Kipping, J., Schäfer, A., Villringer, A. & Ragert, P. A Comparison between Uni- and Bilateral tDCS Effects on Functional Connectivity of the Human Motor Cortex. Frontiers in human neuroscience 7, 183 (2013).
54. Hummel, F. et al. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain: a journal of neurology 128, 490–9 (2005).
55. Lang, N., Nitsche, M. A., Sommer, M., Tergau, F. & Paulus, W. Modulation of motor consolidation by external DC stimulation. Supplements to Clinical neurophysiology 56, 277–81 (2003).
56. Bolognini, N., Fregni, F., Casati, C., Olgiati, E. & Vallar, G. Brain polarization of parietal cortex augments training-induced improvement of visual exploratory and attentional skills. Brain research 1349, 76–89 (2010).
57. Tanaka, S. & Watanabe, K. [Transcranial direct current stimulation--a new tool for human cognitive neuroscience]. Brain and nerve = Shinkei kenky no shinpo 61, 53–64 (2009).
58. Clark, V. P. et al. TDCS guided using fMRI significantly accelerates learning to identify concealed objects. NeuroImage 59, 117–28 (2012).
59. Vines, B. W., Nair, D. G. & Schlaug, G. Contralateral and ipsilateral motor effects after transcranial direct current stimulation. Neuroreport 17, 671–4 (2006).
60. Blumenfeld, R. S. & Ranganath, C. Dorsolateral prefrontal cortex promotes long-term memory formation through its role in working memory organization. The Journal of neuroscience: the official journal of the Society for Neuroscience 26, 916–25 (2006).
61. Rolls, E. T. The functions of the orbitofrontal cortex. Brain and cognition 55, 11–29 (2004).
62. Kringelbach, M. L. The human orbitofrontal cortex: linking reward to hedonic experience. Nature reviews. Neuroscience 6, 691–702 (2005).
63. Gourion, D., Gourevitch, R., Leprovost, J.-B., Olié H lôo, J.-P. & Krebs, M.-O. [Neurodevelopmental hypothesis in schizophrenia]. L’Encéphale 30, 109–18

64. Dockery, C. A., Hueckel-Weng, R., Birbaumer, N. & Plewnia, C. Enhancement of planning ability by transcranial direct current stimulation. The Journal of neuroscience: the official journal of the Society for Neuroscience 29, 7271–7 (2009).
65. Brunoni, A. R., Boggio, P. S., Ferrucci, R., Priori, A. & Fregni, F. Transcranial direct current stimulation: challenges, opportunities, and impact on psychiatry and neurorehabilitation. Frontiers in Psychiatry 4, 19 (2013).
66. Fregni, F. et al. Anodal transcranial direct current stimulation of prefrontal cortex enhances working memory. Experimental brain research. Experimentelle Hirnforschung. Expérimentation cérébrale 166, 23–30 (2005).
67. Andrews, S. C., Hoy, K. E., Enticott, P. G., Daskalakis, Z. J. & Fitzgerald, P. B. Improving working memory: the effect of combining cognitive activity and anodal transcranial direct current stimulation to the left dorsolateral prefrontal cortex. Brain stimulation 4, 84–9 (2011).
68. Kincses, T. Z., Antal, A., Nitsche, M. A., Bártfai, O. & Paulus, W. Facilitation of probabilistic classification learning by transcranial direct current stimulation of the prefrontal cortex in the human. Neuropsychologia 42, 113–7 (2004).
69. Bigelow, H. J. & Barnard, J. Phineas Gage. Brain 3, 843–857 (2002).70. Hecht, D., Walsh, V. & Lavidor, M. Transcranial direct current stimulation
facilitates decision making in a probabilistic guessing task. The Journal of neuroscience: the official journal of the Society for Neuroscience 30, 4241–5 (2010).
71. Fecteau, S. et al. Activation of prefrontal cortex by transcranial direct current stimulation reduces appetite for risk during ambiguous decision making. The Journal of neuroscience: the official journal of the Society for Neuroscience 27, 6212–8 (2007).
72. Fecteau, S. et al. Diminishing risk-taking behavior by modulating activity in the prefrontal cortex: a direct current stimulation study. The Journal of neuroscience: the official journal of the Society for Neuroscience 27, 12500–5 (2007).
73. Boggio, P. S. et al. Effects of transcranial direct current stimulation on working memory in patients with Parkinson’s disease. Journal of the neurological sciences 249, 31–8 (2006).
74. Takeuchi, H., Taki, Y. & Kawashima, R. Effects of working memory training on cognitive functions and neural systems. Reviews in the neurosciences 21, 427–49 (2010).
75. Morrison, A. B. & Chein, J. M. Does working memory training work? The promise and challenges of enhancing cognition by training working memory. Psychonomic bulletin & review 18, 46–60 (2011).
76. Jaeggi, S. M., Buschkuehl, M., Jonides, J. & Perrig, W. J. Improving fluid intelligence with training on working memory. Proceedings of the National Academy of Sciences of the United States of America 105, 6829–33 (2008).
77. Javadi, A. H. & Walsh, V. Transcranial direct current stimulation (tDCS) of the left dorsolateral prefrontal cortex modulates declarative memory. Brain stimulation 5, 231–41 (2012).

78. Hansen, N. Action mechanisms of transcranial direct current stimulation in Alzheimer’s disease and memory loss. Frontiers in psychiatry / Frontiers Research Foundation 3, 48 (2012).
79. Peterson, C. C., Garnett, M., Kelly, A. & Attwood, T. Everyday social and conversation applications of theory-of-mind understanding by children with autism-spectrum disorders or typical development. European child & adolescent psychiatry 18, 105–15 (2009).
80. Tecchio, F. et al. Anodal transcranial direct current stimulation enhances procedural consolidation. Journal of neurophysiology 104, 1134–40 (2010).
81. Coffman, B. A., Trumbo, M. C. & Clark, V. P. Enhancement of object detection with transcranial direct current stimulation is associated with increased attention. BMC neuroscience 13, 108 (2012).
82. Fields, R. D. Amping Up Brain Function: Transcranial Stimulation Shows Promise in Speeding Up Learning: Scientific American. Scientific American (2011). at <http://www.scientificamerican.com/article.cfm?id=amping-up-brain-function>
83. Adee, S. Zap your brain into the zone: Fast track to pure focus life. New Scientist Issue 2850 (2012). at <http://www.mrn.org/files/news/Zap_your_brain_into_the_zone__Fast_track_to_pure_focus_-_life_-_06_February_2012_-_New_Scientist.pdf>
84. Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience. (New York: Harper and Row, 1990).
85. Kuo, M.-F. & Nitsche, M. A. Effects of transcranial electrical stimulation on cognition. Clinical EEG and neuroscience: official journal of the EEG and Clinical Neuroscience Society (ENCS) 43, 192–9 (2012).
86. Bullard, L. M. et al. Transcranial direct current stimulation’s effect on novice versus experienced learning. Experimental brain research. Experimentelle Hirnforschung. Expérimentation cérébrale 213, 9–14 (2011).
87. Chi, R. P. & Snyder, A. W. Facilitate insight by non-invasive brain stimulation. PloS one 6, e16655 (2011).
88. Flöel, A. et al. Short-term anomia training and electrical brain stimulation. Stroke; a journal of cerebral circulation 42, 2065–7 (2011).
89. Sparing, R., Dafotakis, M., Meister, I. G., Thirugnanasambandam, N. & Fink, G. R. Enhancing language performance with non-invasive brain stimulation--a transcranial direct current stimulation study in healthy humans. Neuropsychologia 46, 261–8 (2008).
90. De Vries, M. H. et al. Electrical stimulation of Broca’s area enhances implicit learning of an artificial grammar. Journal of cognitive neuroscience 22, 2427–36 (2010).
91. Ladeira, A. et al. Polarity-dependent transcranial direct current stimulation effects on central auditory processing. PloS one 6, e25399 (2011).
92. Voytek, B. & Gazzaley, A. Stimulating the aging brain. Annals of neurology 73, 1–3 (2013).
93. Flöel, A. et al. Non-invasive brain stimulation improves object-location learning in the elderly. Neurobiology of aging 33, 1682–9 (2012).

94. Zimerman, M. et al. Neuroenhancement of the aging brain: restoring skill acquisition in old subjects. Annals of neurology 73, 10–5 (2013).
95. Csifcsak, G. et al. Modulatory effects of transcranial direct current stimulation on laser-evoked potentials. Pain medicine (Malden, Mass.) 10, 122–32 (2009).
96. Antal, A. et al. Transcranial direct current stimulation over somatosensory cortex decreases experimentally induced acute pain perception. The Clinical journal of pain 24, 56–63 (2008).
97. Fregni, F. et al. Transcranial direct current stimulation of the prefrontal cortex modulates the desire for specific foods. Appetite 51, 34–41 (2008).
98. Boggio, P. S. et al. Prefrontal cortex modulation using transcranial DC stimulation reduces alcohol craving: a double-blind, sham-controlled study. Drug and alcohol dependence 92, 55–60 (2008).
99. Iuculano, T. & Cohen Kadosh, R. The Mental Cost of Cognitive Enhancement. Journal of Neuroscience 33, 4482–4486 (2013).
100. Fritsch, B., Reis, J., Martinowich, K., Schambra, H. M., Ji, Y., Cohen, L. G., et al. Direct current stimulation promotes BDNF-dependent synaptic plasticity: potential implications for motor learning. Neuron, 198–204
101. A. Antal et al. Direct current stimulation over V5 enhances visuomotor coordination by improving motion perception in humans.J. Cogn. Neurosci., 16 (2004), pp. 521–527
102. A. Antal et al. Direct current stimulation over MT+/V5 modulates motion aftereffect in humans. Neuroreport, 15 (2004), pp. 2491–2494
103. A. Rogalewski et al. Transcranial direct current stimulation disrupts tactile perception. Eur. J. Neurosci., 20 (2004), pp. 313–316
104. Reis J, Schambra HM, Cohen LG, et al. Noninvasive cortical stimulation enhances motor skill acquisition over multiple days through an effect on consolidation. Proc Natl Acad Sci U S A 2009;106: 1590–1595
105. Islam N, Aftabuddin M, Moriwaki A, et al. Increase in the calcium level following anodal polarization in the rat brain. Brain Res 1995; 684:206–208.
106. Nitsche, M. A., Liebetanz, D., Schlit- terlau, A., Henschke, U., Fricke, K., Frommann, K., et al. (2004a). GABAergic modulation of DC stimulation-induced motor cortex excitability shifts in humans. Eur. J. Neurosci. 19, 2720–2726.
106. Hsu, T.-Y. et al. Modulating inhibitory control with direct current stimulation of the superior medial frontal cortex. NeuroImage 56, 2249–57 (2011).
107. Molaee-Ardekani, B. et al. Effects of transcranial Direct Current Stimulation (tDCS) on cortical activity: A computational modeling study. Brain stimulation 6, 25–39 (2013).
108. Clark, V. P., Coffman, B. a, Trumbo, M. C. & Gasparovic, C. Transcranial direct current stimulation (tDCS) produces localized and specific alterations in neurochemistry: a 1H magnetic resonance spectroscopy study. Neuroscience letters 500, 67–71 (2011).

Supplementary Material
Fig.1 :
Source: (92) Voytek, B., & Gazzaley, A. (2013). Stimulating the aging brain. Annals of neurology, 73(1), 1–3. doi:10.1002/ana.23790
Fig 2: tDCS & TMS associations:

Source: 41 - http://www.brainscanr.com/Search?term_a=tDCS
Fig 3:
Source: 41 - http://www.brainscanr.com/Search?term_a=working+memory
Recommended