The Case Against Bariatric Surgery Centers of Excellence
Edward H. Livingston, MD, FACS, AGAF
Professor and Chairman, Division of Gastrointestinal Surgery University of Texas Southwestern School of Medicine-DallasContributing Editor, JAMA

History
• Highly publicized bad outcomes
• Insurers pulled out of the market
• CMS MCAC 2004
• ASMBS asks for CMS NCD 2005– Offer COE requirement that they would
administer through SRC
Were COEs necessary?
• Bariatric surgery mortality and morbidity steadily decreasing
• Associated with greater acceptance for these operations and referral of lower risk candidates
• There was no outcomes crises requiring regulation of bariatric surgery
Argument: Insurers will not cover bariatric surgery
• True but not because of bad outcomes
• Bad outcomes occurred but current COEs do not address these matters
• Reticence to cover bariatric results from inadequate data to support the use of bariatric surgery
Bariatric Surgery Evidence
• Cause weight loss: Level 1
• Cause complications: Level 1
• Improve comorbidities: Level 2 and below
• The greatest risk to bariatrics is the low quality of evidence to support its use.
• Few ongoing studies will overcome this limitation
Evidence
• VA/DOD Obesity treatment CPG
• http://www.healthquality.va.gov/Obesity_Clinical_Practice_Guideline.asp

Recommendation Sources of Evidence QE Overall Quality R
1. Bariatric surgery (RYGB, AGB, & VBG) to promote substantial long-term (3 years) weight loss.
ECRI, 2005Maggard et al., 2005Shekelle et al., 2004
I Good A
2. Bariatric surgery (RYGB, AGB, & VBG) to improve or resolve comorbid conditions.
ECRI, 2005 I Fair* B
3. Bariatric surgery (RYGB, AGB, & VBG) to improve quality of life. ECRI, 2005Shekelle et al., 2004
I Fair* B
4. Long-limb RYGB to promote weight loss. ECRI, 2005 I Fair B
5. Mortality from bariatric surgery (all procedures). Shekelle et al., 2004ECRI, 2005
I Good A
6. Adverse events from bariatric surgery (all procedures). ** ECRI, 2005Shekelle et al., 2004
I Good A[SU1]
7. RYGB promotes greater weight loss than VBG at three years. ECRI, 2005Shekelle et al., 2004
I Fair B
8. VBG promotes greater weight loss than ABG at one year. ECRI, 2005 I Fair B
9. Biliopancreatic Diversion and Duodenal Switch Procedures. ECRI, 2005Shekelle et al., 2004
II-2 Fair I
10. Bariatric surgery in those over 65 years of age. ECRI, 2005Shekelle et al., 2004
II-3 Fair I
11. Bariatric surgery for patients with BMI less than 40 kg/m2. Shekelle et al., 2004 I Poor I[SU2]
12. Long-term (greater than 3 years) complications of bariatric surgery. Shekelle et al., 2004 II-1 Poor I
13. Preoperative weight loss. Expert Opinion III Poor I
14. Preoperative psychiatric assessment. Expert Opinion III Poor I
15. Bariatric surgery in patients with uncontrolled psychiatric disorders, substance abuse, severe cardiovascular disease, status post MI, wheelchair bound, or oxygen dependence.
Expert Opinion III Poor I
16. Bariatric surgery to improve long-term (greater than 5 years) survival. Christou et al., 2004Flum & Dellinger, 2004
II-2 Poor I
* Evidence quality was rated as fair, because few studies reported these outcomes consistently, and few studies were designed to examine the impact of surgery on these outcomes. **Adverse Events and need for reoperation.QE = Quality of Evidence; R = Recommendation (see Appendix A)
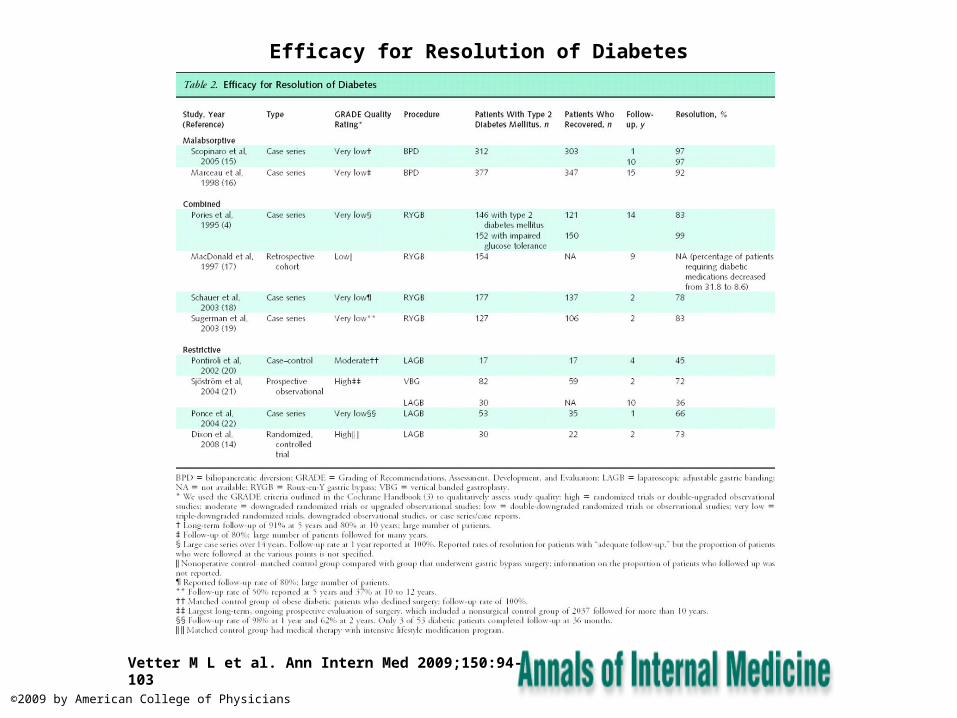
Efficacy for Resolution of Diabetes
Vetter M L et al. Ann Intern Med 2009;150:94-103
©2009 by American College of Physicians

Why would insurance companies support COEs?

Insurance Company CEO Pay
Name Company 1-Year ($mil) 5-year ($mil)
Ronald A Williams Aetna 38.12 77.86
Joel F Gemunder Omnicare 12.55 67.01
H Edward Hanway Cigna 10.27 121.35
Stephen J Hemsley UnitedHealth Group 5.03 NA
Angela F Braly WellPoint 4.07 NA
Michael B McCallister Humana 2.39 56.91
Jay M Gellert Health Net 1.34 37.69
Source http://www.forbes.com/lists/2009/12/best-boss-09_CEO-Compensation-Health-Care-Equipment-Services_9Rank.html
Why would insurance companies support COEs?
• Quality?• Cost?• How can they best limit bariatric surgery?
– Not cover it at all• Works for some but they are selling insurance products in a
competitive market
– Make it difficult to attain• Arbitrary requirements (pre op weight loss)
– Get surgeon buy in to make it difficult• COE

What is the evidence that COEs are effective?

Conclusions do not follow data
Stats incorrect, erroneous conclusion based on p-value


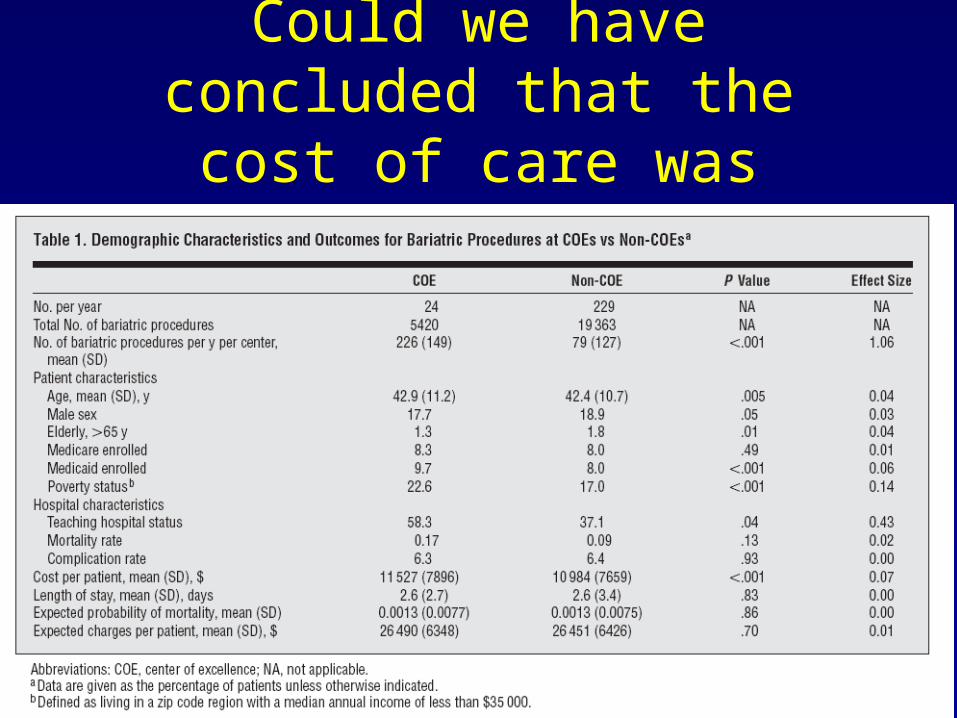
Could we have concluded that the cost of care was greater in
COEs?



Conclusion
• COEs were not necessary
• COE standards are not evidence based
• COEs are very expensive
• COEs are harming general surgery practice
• COE outcomes are no better than non COEs
Recommended