Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
Springvale Monash Legal Service Inc
The Coronial Process: Delays From Death To Inquest
1
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
Contents
1. INTRODUCTION 4
2. CORONER’S COURT PROCESS 6
A. ROLE OF THE CORONER 6
B. REPORTING A DEATH AND INITIAL PROCEDURES 7
C. THE INVESTIGATION 7
(i) The Major Collision Investigation Unit 8
(ii) Homicide Squad Investigation 9
D. NOTIFICATION – WHEN AN INQUEST WILL NOT BE HELD 12
E. WHEN AN INQUEST WILL BE HELD 12
(i) When an Inquest must be held 12
(ii) Other Circumstances 12
(iii) Requesting an Inquest 13
F. NOTIFICATION OF INQUEST 13
G. THE INQUEST 14
(i) The Hearing 14
(ii) The Finding 14
3. DELAYS IN THE CORONER’S COURT PROCESS 15
A. REPORTING A DEATH AND INITIAL PROCEDURES 15
B. THE INVESTIGATION 15
(i) Time Constraints and Lack of Resources within Victoria Police
15
(ii) Obtaining witness statements 16
(iii) Technical and Expert Reports 16
C. REQUESTING AN INQUEST 17
D. THE INQUEST 17
(i) Initial Listing and Case Management 17
(ii) Interested Parties 18
(iii) Adjournments to Clarify Issues or Obtain Additional Evidence
18
2
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
4. CONCLUSION 19
(i) The Investigation 19
(ii) The Inquest 19
5. APPENDIX A 21
6. REFERENCES 25
3

Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
1. INTRODUCTION
The Office of the Coroner is charged with the role of investigating circumstances of
death. This is with a view to averting preventable deaths.1 In addition to this, the
Coroner’s finding is important to family members who may be relying on the finding in
litigation related to the death or to gain closure from knowledge of the circumstances of
the death. For these reasons it is in the public interest that the Coroner balance the need to
seek the full truth against the time taken to deliver the finding.
The length of time between death and inquest varies significantly from case to case. On
average it is approximately 2 years from death to inquest. The averages below have been
calculated from the information provided in Appendix A.
Circumstances of Death Number of Deaths Average time taken from
Death to Inquest
Police Shootings 16 2 years 2 months
Police Pursuits 6 1 year 9 months
Baby Death 7 2 years 1 month
Workplace Death 4 3 years 1 month
Medical/Hospital Death 6 2 years 4 months
Aviation Death 2 2 years 1 month
Fire 2 1 year
Drowning 2 2 years 4 months
Death involving Motor
Vehicle
4 11 months
A solicitor experienced in dealing with the coronial system indicated that there has been a
move towards a case management approach, where the Coroner assumes a greater role in
setting a timeline for the proceedings, however this approach has not been adopted
1 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
4
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
throughout the coronial system2. It is hoped that the proposed system to deal exclusively
with work related deaths will result in speedier findings which in turn will serve the
public better by making work places safer, sooner.3
We have identified three specific consequences of delays in the coronial process:
i. The adverse effects on family members of the deceased can be
characterised as:
a. Need for family to find closure.
b. Difficulty in pursuing legal rights stemming from death.
ii. The adverse effects on the accuracy of the finding can be classified as:
a. Accuracy of witness statements
b. Difficulty in locating witnesses
iii. The public interest in speedier findings is in the prevention of preventable
deaths.
These adverse effects are best illustrated by way of a case study.
Case study: Mark Kauffman
Mark died on 19 January 2002 as a result of wounds sustained when shot by police. Mark
was suffering from a psychotic episode at the time. Due to these circumstances the death
was reportable and an inquest was to be held. The inquest was set down for 16 November
2004 and conducted in December 2004, concluding in March 2005. To date, the findings
have not been submitted by the Coroner and the family feels that the protracted coronial
process has extended their grieving period as they are unable to move past the death of
their son. They feel isolated from the coronial process as there has been minimal
communication between the Office of the Coroner and the family, apart from the
notification of inquest date. Throughout the investigation process they remained
uninformed of the progress or content.
2 Interview with solicitor 11 October 2004. Firm anonymous. 3 Coroner tackles fatal culture of repetition, The Age, 28 October 2004.
5
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
2. CORONER’S COURT PROCESS
A. ROLE OF THE CORONER
The primary role of the Coroner is to determine the identity of the deceased, the cause of
death and the particulars needed to register the death. In some cases the Coroner may also
comment and make recommendations about public health, safety or the administration of
justice.
Even where a death is not the result of a suspected homicide or other crime there are a
number of reasons why a cause of death should be adequately identified. Plueckhahn4
identifies the following reasons as important in determining a cause of death:
• Drawing attention to the existence of circumstances which if not remedied may
lead to further deaths
• To preserve the legal interests of the deceased person’s family, heirs and other
interested parties
• To assist in insurance claims or civil litigation
• To assist generally in medical care, medical education and medical research
• To provide an accurate statistical base of medical causes of death for medical and
educational purposes.
Plueckham believes that it is in the community’s interest to accurately identify the cause
of death because ‘these have a bearing on public health, the discovery of unidentified
diseases, safety in industry and on the roads, vehicle construction, health hazards and the
treatment and care of patients’5
It is not the Coroner’s role to establish whether a crime has been committed, to find a
person guilty of a crime or to establish the negligence of any party. The Coroner’s role is,
therefore, limited to fact finding and making recommendations.
4 V Pleuckhahn, Ethics Legal Medicine and Forensic Pathology (Melbourne University Press, 1983) p 9
6
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
B. REPORTING A DEATH AND INITIAL PROCEDURES
The Coroner’s Act 1985 (“the Act”) requires certain deaths to be reported to the Coroner.
A ‘Reportable Death’ is a death that must be reported to the Coroner where:
• The person died unexpectedly
• The person died from accident or injury
• The person died in a violent or unnatural way
• The person died during or as a result of an anesthetic
• The person was ‘in care’ including
o deaths in police custody
o deaths in gaol
o death of an involuntary patient in a psychiatric institution
o death of a child in a juvenile justice centre
• A doctor has been unable to sign the death certificate giving the cause of death
• The identity of the person who died is not known
Immediately after ‘a reportable death’ the body is taken to the mortuary and a ‘Form 83’
is completed. Police provide a preliminary report to assist the pathologist performing the
autopsy.6
C. THE INVESTIGATION
The investigation into identity, cause of death and the circumstances surrounding the
death is undertaken by either Victoria Police or the State Coroner’s Assistants’ Unit .
Victoria Police generally investigate motor vehicle accidents, suicide, murder and
workplace deaths. The Coroner’s Assistants will investigate all medical or aviation
deaths. Within Victoria Police there are specialized investigation teams which will
investigate deaths according to the circumstances and type of death. Suspected murder
5 V Plueckhan, ‘Light at the end of the Forensic Tunnel’ (1986) 60 Law Institute Journal 60, p1059 6 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
7
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
and manslaughter is investigated by the Homicide Squad and road deaths are investigated
by the Major Collision Investigation Unit.
In the case of workplace deaths the Victorian Workcover Authority provides a
comprehensive report to Victoria Police on any work related death.
All information gathered during an investigation is provided to the Coroner’s Office in
the Brief of Evidence. The Coroner’s Office is responsible for setting the deadline for the
submission of the Brief. This often depends on the complexity of the issues, the nature
and circumstances of the death and the number of witness statements that need to be
obtained. Often police officers will request, and are granted, an extension for submission
of the Brief.
Any Brief of Evidence received from Victoria Police is checked and any additional
investigation that is required is undertaken by the Coroner’s Assistant or the police
officer preparing the Brief.
The Coroner’s Assistant will then meet with the Coroner to discuss whether any
additional information is required.
(i) The Major Collision Investigation Unit
The Major Collision Investigation Unit (MCIU) is responsible for investigating all fatal
and life-threatening injury crashes. When MCIU initially attend the scene of an accident
they document all physical evidence at the scene and take photographs and measurements
which are used for any subsequent reconstruction of the collision.7
Formal statements are obtained from all parties involved and certain persons may be
formally interviewed. Autopsy reports on deceased persons are performed and blood
samples are analysed for alcohol and drugs.8
7 VACC interview with Sgt Peter Bellion, Victoria Police Major Collision Investigation Unit entitled ‘Crash Course’ [Internet – http://www.motor.net.au/VACC/Media/] 8 Id
8
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
Every vehicle that is involved in a fatality will have a mechanical inspection performed
by qualified mechanics attached to the Unit. There are currently three Senior Constables
and a Senior Sergeant that perform this role. The mechanical investigators receive a
‘jobcard’ from investigating police summarizing the circumstances found at the scene of
the accident. The mechanical investigators examine components of the vehicle involved
to determine whether there was any mechanical defect that caused or contributed to the
accident. Approximately 500 vehicles involved in fatal or life threatening accidents are
inspected by mechanical investigators each year.9
Other investigators apply physics and engineering skills to the physical evidence obtained
from the scene to assess how the accident occurred. Factors examined include speed,
perception-reaction responses, restraint systems, steering input, road conditions and force
of impact. Investigators also use computer simulation software to run simulations of the
crash. These look at braking inputs, speed changes during impact and the positions of
those injured or killed in the accident.10
Witness statements, mechanical investigations, physical evidence, simulations and
reconstructions form the basis of the export reports in the Brief of Evidence. Once the
Brief of Evidence is completed it is provided to the Coroner and/or the Prosecutor. The
complexity of the investigation depends on the nature of the collision, how many witness
statements are obtained and the nature and number of expert evidence reports required.11
(ii) Homicide Squad investigation
The Homicide Squad become involved in the coronial investigation upon referral of the
case from the Coroner. They are charged with compiling the Brief of evidence on which
the Coroner relies when delivering the finding. The Brief consists of:
• summary of death
• all details of death
9 Id 10 Id 11 Id
9
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
• details of witnesses
• statement of witnesses
• Statements of experts consulted
• Possibly a police recommendation
The length of the Brief will depend on the complexity of the circumstances of death. For
example, a police shooting would require input from many expert witnesses such as
ballistic experts and treating psychiatrists. There could be up to 30 statements in any
Brief. The homicide squad generally work in a collegial manner in order prepare the
Brief, with a senior officer coordinating the efforts of the department.12
The length of time varies based on the extent of investigation required. A member of the
homicide squad indicated that on average the Brief would take two years to compile. The
police officers would work on the Brief more intensively if the matter necessitated urgent
response in the public interest. Multiple deaths arising out of a single incident would be
such a case.13
We note that Public Interest Law Clearing House (PILCH) regards eligible matters of
public interest as those that:
1. require a legal remedy or other legal assistance; and
2. affect a significant number of people; or
3. raise matters of broad public concern; or
4. impact on disadvantaged or marginalised groups.14
We believe that points 2, 3, and 4 relate the coronial process and stand to be prejudiced
by delays.
Upon completion the Brief is passed to the Coroner who may direct that further
investigation take place, or other avenues be pursued.
12 Interview with senior constable, Homicide Squad, 25 October 2004 13 Id 14 www.pilch.org.au
10
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
The police officer consulted in the Homicide Squad indicated that the time constraints did
not induce pressure in those involved, however it was acknowledged that it was preferred
to complete the investigation sooner than later. The officer did not believe that the
findings of the Coroner would be tainted by inaccurate witness recollection as statements
were taken soon after the event, and in most cases witnesses could be located.15
Once the matter proceeds to inquest the police remain involved by organizing the
proceedings in calling witnesses and tendering evidence. As inquests often deal with
systemic issues, and also do not actively involve criminal law, police interest and
enthusiasm in this part of the inquest (beyond the initial investigatory stage) may be less
intense.16 Essentially, the police are interested in how the individual died, as the Coroner
is interested in: “how… the deceased came about his death”.17
The above quote relates to circumstances leading to the fatality (which often are not
relevant to a criminal investigation), as opposed to the immediate act. For example, if an
individual suffering from mental illness was fatally wounded in a confrontation with the
police, police interest would essentially involve the criminal aspect of the case,
identifying the immediate circumstances leading to the death. They may interview
witnesses, conduct a series of technical tests and examinations of the scene, so as to
determine the level culpability of the shooter. On the other hand, the Coronial interest
would lie with long-term issues which led to the shooting. Were the police aware of the
severity of this individual’s illness? How much involvement have the various mental
health organizations had with this individual? Did various mental health workers attend
the scene? Was current police procedure appropriate given the circumstances? Was this
fatality avoidable?
15 Id 16 Interview with Coroner 28 June 2005 17 Criminal Law Investigation and Procedure, Vol 2, Freckleton 1, [2.23.330] Section 19 – Coronial findings and comments
11
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
D. NOTIFICATION – WHEN AN INQUEST WILL NOT BE HELD
Family members and interested parties are formally notified 21 days prior to the Coroner
making a finding ‘in Chambers’. Parties then have an opportunity to submit any
particular questions, or to request that an inquest be held.
E. WHEN AN INQUEST WILL BE HELD
There are a number of circumstances in which an inquest will be held. The minimum
period between death an inquest is approximately 8 months. In more complex cases and
cases involving a large number of parties the period between death and inquest may be
considerably longer.18
(i) When an Inquest must be held
Under s17 of the Act the Coroner MUST hold an inquest where:
Homicide is suspected (however the Coroner usually awaits criminal proceedings
and can decide NOT to hold an inquest if someone has been charged and
convicted)
The person was ‘in care’
The person’s identity is not known
The Attorney General directs
(ii) Other Circumstances
The Coroner will also hold an inquest in other circumstances if the Coroner believes it is
desirable. An assessment is made by the Coroner before deciding whether an inquest will
18 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
12
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
be held. This may occur where facts are unclear or there is an issue of public
importance.19
(iii) Requesting an Inquest
Interested parties can request the Coroner hold an inquest. This is done by writing to the
Coroner giving reasons why an inquest should be held20. Most inquests held in
circumstances outside of those which require an inquest under the Act are at the request
of families and interested parties. Under s17(2A) of the Act the Attorney General may
direct the Coroner to hold an inquest, however this is very rare21.
If the Coroner refuses or has not agreed to an inquest within three months of a party’s
request under s18 of the Act a person may apply to the Supreme Court for an order that
an inquest be held.
F. NOTIFICATION OF INQUEST
The Coroner’s Court ‘Listing Clerk’ is responsible for issuing summons and advice to
interested parties in relation to upcoming inquests. Family members are notified of an
inquest date by the Coroner. Under s42 of the Act the Coroner must publish the place,
date and time of the inquest at least 14 days before the hearing.
Interested parties must contact the registrar if they wish to formally participate in
proceedings. They are required to demonstrate their involvement in the death and the
reasons why they should formally participate in the hearing. 22
19 State Coroner’s Office Victoria website, The Coronial Process [Internet – http://www.Coronerscourt.vic.gov.au] 20 State Coroner’s Office Victoria website, The Coronial Process [Internet – http://www.Coronerscourt.vic.gov.au] 21 Interview with Coroner’s Assistant, Coroners Court 28 August 2004. 22 State Coroner’s Office Victoria website, The Coronial Process [Internet – http://www.Coronerscourt.vic.gov.au]
13
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
G. THE INQUEST
(i) The Hearing
An inquest is a public hearing conducted by the Coroner. Hearings are held in the
Coroner’s Court at the Coronial Services Centre or, in the case of country hearings, at the
local Magistrates’ Court.
Although an inquest is similar in some ways to a civil or criminal court proceeding, most
rules of evidence and procedure do not apply and the inquest is conducted in an
inquisitorial rather than adversarial manner. The purpose of an inquest is to establish
certain facts and its purpose has been described as “seeking truth rather than justice”.23
During an inquest witnesses are sworn in, statements are read out and witnesses are
subjected to examination and cross-examination. A member of the State Coroner’s
Investigation Unit initially leads evidence from the witness. The legal representative of
interested parties also has the opportunity to question the witness. The Coroner may also
ask questions during the process. Where the victim’s family is unrepresented, a member
of the Coroner’s Investigation Unit will also ask the family if they would like any
questions answered.24
At any time the Coroner may request other witnesses or information if further evidence is
needed to clarify an issue or new issues arise. Hearings may be adjourned during this
process.
(ii) The Finding
Once all evidence is heard the Coroner will adjourn the case to complete their finding.
The finding may be given on the same day, but often is adjourned to a date in the future
23 Interview with Coroner’s Assistant, Coroners Court 28 August 2004. 24 State Coroner’s Office Victoria website, The Coronial Process [Internet – http://www.Coronerscourt.vic.gov.au]
14
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
depending on the nature and complexity of the case25. The Coroner’s finding then
becomes public record.
3. DELAYS IN THE CORONER’S COURT PROCESS
A. REPORTING A DEATH AND INITIAL PROCEDURES
We did not identify any specific delays in this process as a ‘Reportable Death’ is reported
to the Coroner’s Office immediately and the body is transported to the mortuary at the
Coronial Services Centre. The Act clearly identifies those deaths which must be reported.
Autopsies and pathology reports must be performed as soon as possible after death. In
Melbourne, this process is assisted by the centralised nature of the Coronial Services
Centre. Autopsies are performed by a Forensic Pathologist at the Victorian Institute of
Forensic Medicine.
B. THE INVESTIGATION
The investigative process introduces delays into the Coronial process. As noted, the
minimum time noted from our research between death and inquest is eight months and
can be much longer depending on the case. The length of time required to investigate a
death depends largely on the nature and circumstances of the death and the complexity of
the issues that arise.
(i) Time Constraints and Lack of Resources within Victoria Police
We were advised that police officers responsible for the investigation of deaths often
request, and are granted, extensions for the submission of the Brief26. We have been
25 State Coroner’s Office Victoria website, The Coronial Process [Internet – http://www.Coronerscourt.vic.gov.au] 26 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
15
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
unable to determine how, and to what extent, resource issues impact the investigative
process and the request and granting of these extensions.
There is no formal process for requesting or granting an extension and the decision to do
so is at the discretion of the Coroner’s Office27. It would appear however that it is
relatively easy to obtain an extension.
(ii) Obtaining witness statements
The number of witness statements that need to be obtained during an investigation and
any difficulties associated with this has a significant impact on the preparation and
submission of the Brief and the investigative process in general.
During our investigations we discovered that witnesses often refuse to provide the police
with a formal statement for legal reasons. In these cases the Coroner is forced to call
witnesses at the inquest28. We were advised by Margy Wilde-Brown, whose partner died
in psychiatric care in the ACT, that it was these difficulties that contributed to the
substantial delay between his death and the finding made by the Coroner (over 2½ years). 29
Although the Coroner has the power to call witnesses who refuse to give statements to
the inquest, the most efficient manner of investigating the death is to obtain these
statements prior to the inquest. As was the case with Margy Wilde-Brown, the calling and
questioning of witnesses who refused to provide police with statements often raised
additional facts and issues which required further investigation. In some cases this meant
that the inquest had to be adjourned for lengthy periods.
(iii) Technical and Expert Reports
Obtaining technical and expert reports clearly has some impact on the time taken to
complete the investigative process. Again, the length of time required clearly depends on
the nature and circumstances of the case and the complexity of the issues involved. This
27 Interview with Coroner’s Assistant, Coroners Court 28 August 2004. 28 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
16
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
is illustrated in the discussion of the investigative role of the Major Collision and
Investigation Unit (MCIU). It would appear that mechanical inspections are undertaken
relatively quickly however the extent of any further investigation depends on the nature
of the collision, the number of cars involved, the number of witnesses and the
circumstances surrounding the incident. Information from other sources such as
manufacturers may also be required.30
Investigations carried out by the Homicide Squad are often subject to delays as the
investigating police officers await reports from other parties such as medical
practitioners.31
C. REQUESTING AN INQUEST
We did not identify any specific delays relating to the request of an inquest by interested
parties. It should be noted however that the Act provides that a person can apply to the
Supreme Court if they have not received a response from the Coroner’s Office within
three months of making the request. This would indicate that the Coroner must respond
within this period.
D. THE INQUEST
(i) Initial Listing and Case Management
We were unable to establish if there were any specific issues surrounding case
management and the initial listing of matters however listing and case management is
certainly identified as having a significant impact when inquests are adjourned.32
29 Interview with Margy Wilde-Brown, 23 September 2004 30 Information sourced from a VACC interview with Sgt Peter Bellion, Victoria Police Major Collision Investigation Unit entitled ‘Crash Course’. 31 Interview with senior constable, Homicide Squad, 25 October 2004 32 Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
17
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
(ii) Interested Parties
The number of interested parties involved in an inquest also appears to have some impact
on delays. As the number of interested parties increase so do the number and complexity
of the issues raised and the potential for adjournments during the process.
Inquests may also be adjourned where an interested party, in particular the victim’s
family, is attempting to obtain legal representation at the inquest. Sometimes funding or
pro-bono is sought by the family from organisations such as Legal Aid or PILCH. This
can also contribute to the delays.
Interested parties may also seek adjournments in order to obtain and examine additional
evidence.
(iii) Adjournments to Clarify Issues or Obtain Additional Evidence
Adjournments and the subsequent re-listing of inquests to obtain additional evidence or to
clarify or explore additional issues raised at the inquest clearly have a significant impact
on the delays in the process. Where inquests are adjourned in these circumstances there
are often long periods between the initial hearing and the re-listing of the matter. The
period of time may relate to the extent of investigation required and also to the ability of
the Coroner’s Court to re-list within the existing case management structure.
The ABC program ‘A Case for the Coroner’ aired in 2003 illustrated this issue. During
an inquest into the death of a woman who had overdosed on Quinine, the Court heard
evidence regarding the possibility that the pathology reports at the time of death may
have been incorrect. The matter was adjourned so that blood samples retained could be
re-tested. Although the testing was completed within a short period, the matter was not
re-listed for approximately 6 months. 33
4. CONCLUSION
18
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
The primary cause of delay in the coronial system appears to be by way of investigation
and adjournment.
Accurate fact finding should never be compromised by haste in the investigation stage.
However, while performing these tasks it is important to be conscious of the time taken to
complete the investigation and the effects of this on interested parties such as family
members of the deceased.
Adjournments may be integral to ensuring that the coronial system affords its participants
natural justice. If a party that became interested at a later stage was not given the
opportunity to be heard or represented it would have an adverse impact on the public
interest of accurate fact finding. However, while adjournments are necessary they should
not be granted unreasonably or unconditionally so as to prejudice the interests of other
parties.
(iii)The Investigation:
a. We have been informed that on average approximately 2 years
elapse between death and inquest. Is the time taken for the
police to complete the Brief a reflection of the lack of
availability of resources?
(iv) The Inquest:
a. We note from our enquiries that there are delays at the listing
and re-listing stages. Can case management be improved in
order to reduce the time taken to hand down findings while not
prejudicing the interests of the parties?
33 ‘A Case for the Coroner’ Australian Broadcasting Corporation, Sydney, 2003
19
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
b. We note that interested parties often seek adjournments and
that this results in delay as the matter needs to be re-listed. Can
the number and length of adjournments be reduced in any
way?
c. We note that one of the adverse effects of coronial delays is
that preventable deaths may occur prior to a finding being
made. Can interim recommendations be made earlier so that
more deaths are prevented prior to the final finding being
made?
d. We note that in some instances matters of “public interest” are
informally prioritized in order to deliver quicker findings.
Should matters of broad public interest (according to the
PILCH definition) be formally prioritized in the coronial
process?
i. Should these matters be subjected to an expedited
investigative procedure?
ii. Should these matters take priority in listing in order to
provide quicker findings?
iii. Who would determine which matters are in the “public
interest” and hence their priority?
20
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
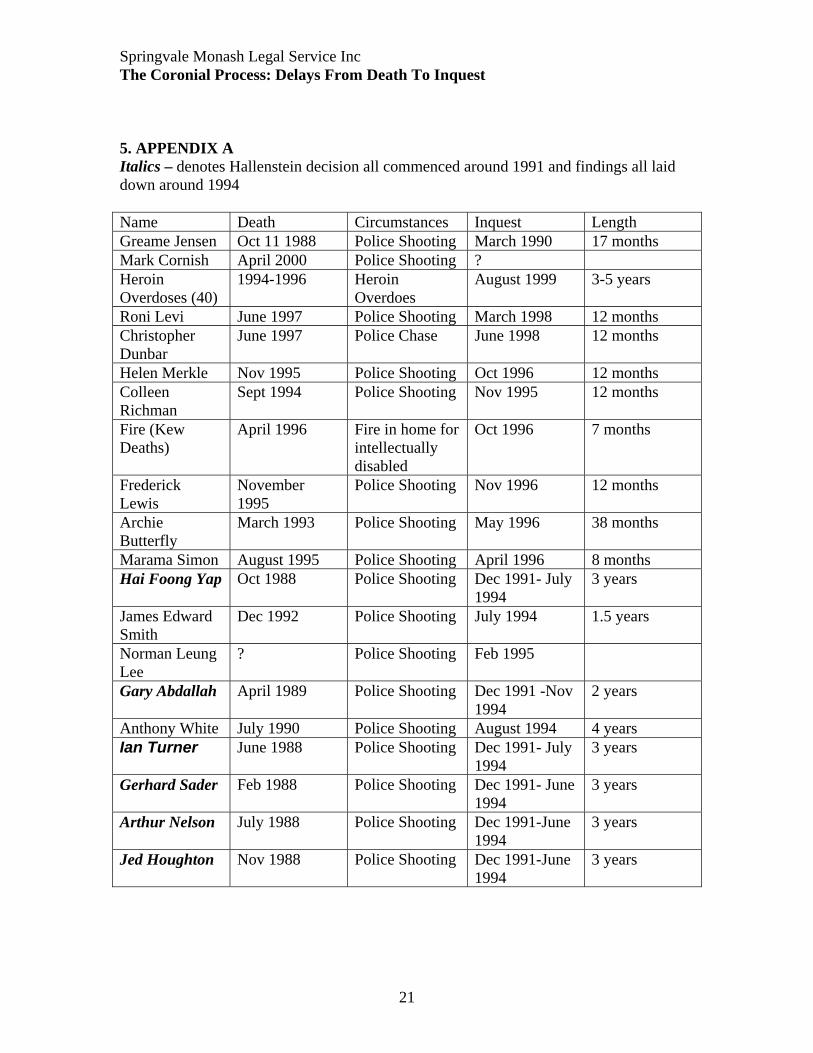
5. APPENDIX A Italics – denotes Hallenstein decision all commenced around 1991 and findings all laid down around 1994 Name Death Circumstances Inquest Length Greame Jensen Oct 11 1988 Police Shooting March 1990 17 months Mark Cornish April 2000 Police Shooting ? Heroin Overdoses (40)
1994-1996 Heroin Overdoes
August 1999 3-5 years
Roni Levi June 1997 Police Shooting March 1998 12 months Christopher Dunbar
June 1997 Police Chase June 1998 12 months
Helen Merkle Nov 1995 Police Shooting Oct 1996 12 months Colleen Richman
Sept 1994 Police Shooting Nov 1995 12 months
Fire (Kew Deaths)
April 1996 Fire in home for intellectually disabled
Oct 1996 7 months
Frederick Lewis
November 1995
Police Shooting Nov 1996 12 months
Archie Butterfly
March 1993 Police Shooting May 1996 38 months
Marama Simon August 1995 Police Shooting April 1996 8 months Hai Foong Yap Oct 1988 Police Shooting Dec 1991- July
1994 3 years
James Edward Smith
Dec 1992 Police Shooting July 1994 1.5 years
Norman Leung Lee
? Police Shooting Feb 1995
Gary Abdallah April 1989 Police Shooting Dec 1991 -Nov 1994
2 years
Anthony White July 1990 Police Shooting August 1994 4 years Ian Turner June 1988 Police Shooting Dec 1991- July
1994 3 years
Gerhard Sader Feb 1988 Police Shooting Dec 1991- June 1994
3 years
Arthur Nelson July 1988 Police Shooting Dec 1991-June 1994
3 years
Jed Houghton Nov 1988 Police Shooting Dec 1991-June 1994
3 years
21
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
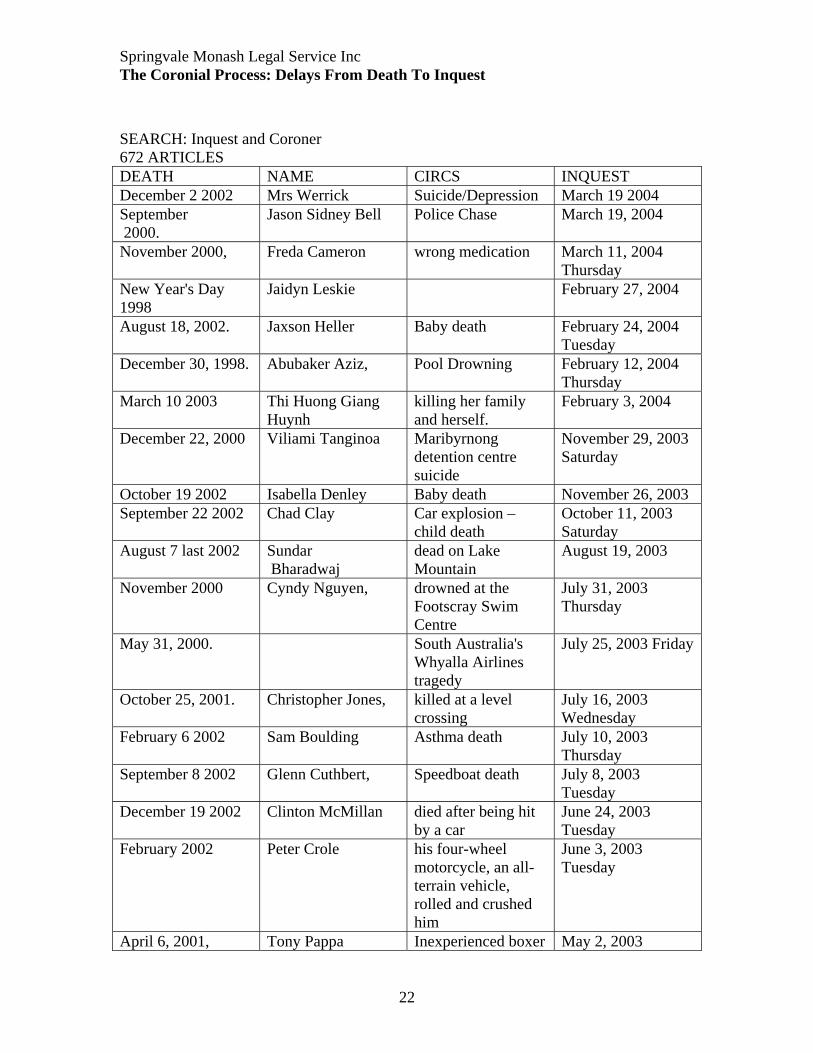
SEARCH: Inquest and Coroner 672 ARTICLES DEATH NAME CIRCS INQUEST December 2 2002 Mrs Werrick Suicide/Depression March 19 2004 September 2000.
Jason Sidney Bell Police Chase March 19, 2004
November 2000, Freda Cameron wrong medication March 11, 2004 Thursday
New Year's Day 1998
Jaidyn Leskie February 27, 2004
August 18, 2002. Jaxson Heller Baby death February 24, 2004 Tuesday
December 30, 1998. Abubaker Aziz, Pool Drowning February 12, 2004 Thursday
March 10 2003 Thi Huong Giang Huynh
killing her family and herself.
February 3, 2004
December 22, 2000 Viliami Tanginoa Maribyrnong detention centre suicide
November 29, 2003 Saturday
October 19 2002 Isabella Denley Baby death November 26, 2003 September 22 2002 Chad Clay Car explosion –
child death October 11, 2003 Saturday
August 7 last 2002 Sundar Bharadwaj
dead on Lake Mountain
August 19, 2003
November 2000 Cyndy Nguyen, drowned at the Footscray Swim Centre
July 31, 2003 Thursday
May 31, 2000. South Australia's Whyalla Airlines tragedy
July 25, 2003 Friday
October 25, 2001. Christopher Jones, killed at a level crossing
July 16, 2003 Wednesday
February 6 2002 Sam Boulding Asthma death July 10, 2003 Thursday
September 8 2002 Glenn Cuthbert, Speedboat death July 8, 2003 Tuesday
December 19 2002 Clinton McMillan died after being hit by a car
June 24, 2003 Tuesday
February 2002 Peter Crole his four-wheel motorcycle, an all-terrain vehicle, rolled and crushed him
June 3, 2003 Tuesday
April 6, 2001, Tony Pappa Inexperienced boxer May 2, 2003
22
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
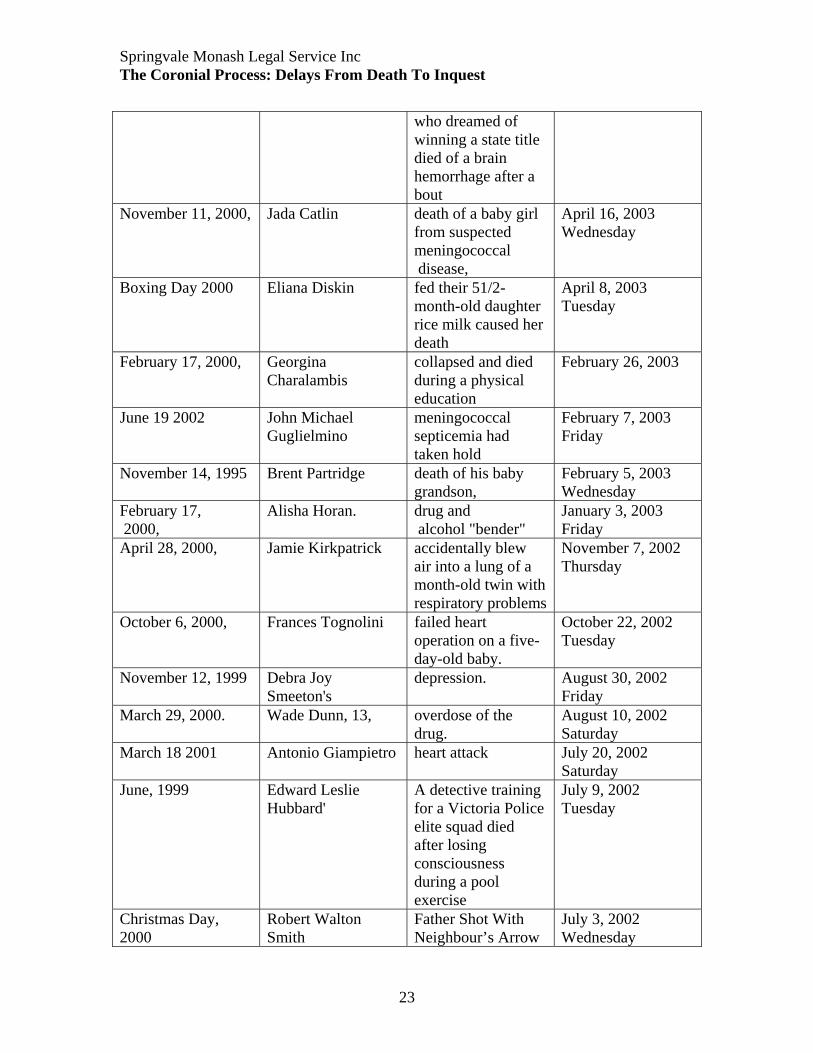
who dreamed of winning a state title died of a brain hemorrhage after a bout
November 11, 2000, Jada Catlin death of a baby girl from suspected meningococcal disease,
April 16, 2003 Wednesday
Boxing Day 2000 Eliana Diskin fed their 51/2-month-old daughter rice milk caused her death
April 8, 2003 Tuesday
February 17, 2000, Georgina Charalambis
collapsed and died during a physical education
February 26, 2003
June 19 2002 John Michael Guglielmino
meningococcal septicemia had taken hold
February 7, 2003 Friday
November 14, 1995 Brent Partridge death of his baby grandson,
February 5, 2003 Wednesday
February 17, 2000,
Alisha Horan. drug and alcohol "bender"
January 3, 2003 Friday
April 28, 2000, Jamie Kirkpatrick accidentally blew air into a lung of a month-old twin with respiratory problems
November 7, 2002 Thursday
October 6, 2000, Frances Tognolini failed heart operation on a five-day-old baby.
October 22, 2002 Tuesday
November 12, 1999 Debra Joy Smeeton's
depression. August 30, 2002 Friday
March 29, 2000. Wade Dunn, 13, overdose of the drug.
August 10, 2002 Saturday
March 18 2001 Antonio Giampietro heart attack July 20, 2002 Saturday
June, 1999 Edward Leslie Hubbard'
A detective training for a Victoria Police elite squad died after losing consciousness during a pool exercise
July 9, 2002 Tuesday
Christmas Day, 2000
Robert Walton Smith
Father Shot With Neighbour’s Arrow
July 3, 2002 Wednesday
23
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
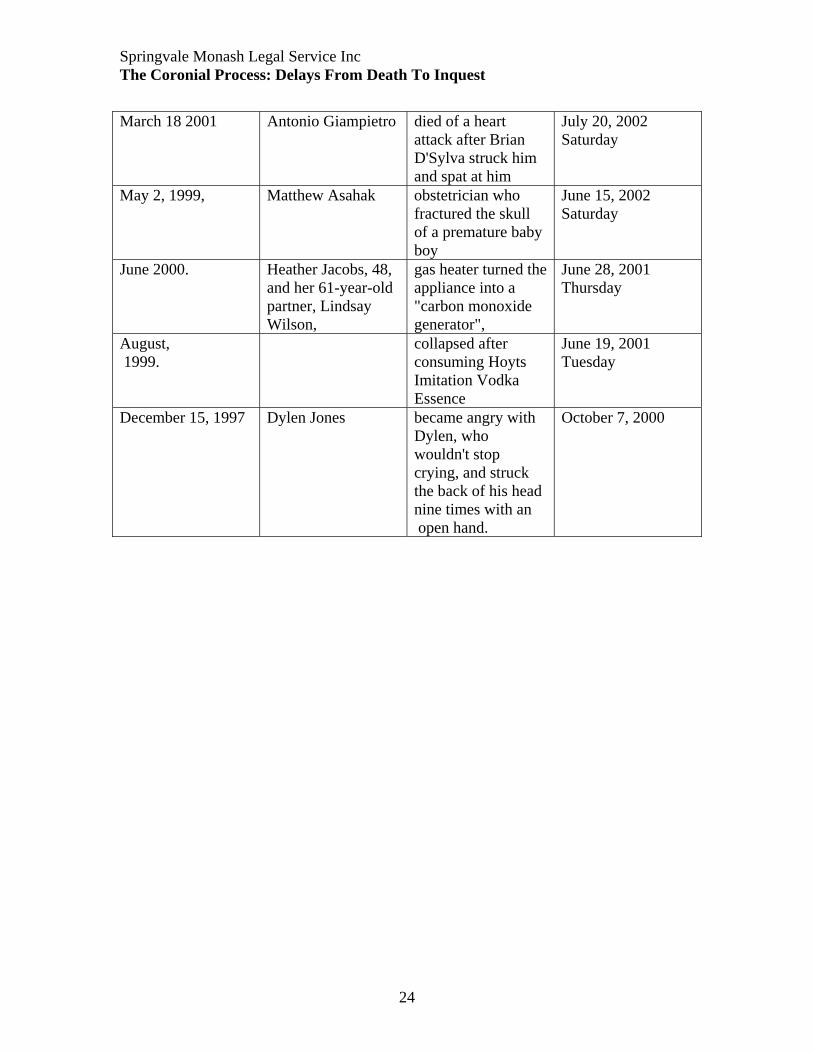
March 18 2001 Antonio Giampietro died of a heart
attack after Brian D'Sylva struck him and spat at him
July 20, 2002 Saturday
May 2, 1999, Matthew Asahak obstetrician who fractured the skull of a premature baby boy
June 15, 2002 Saturday
June 2000. Heather Jacobs, 48, and her 61-year-old partner, Lindsay Wilson,
gas heater turned the appliance into a "carbon monoxide generator",
June 28, 2001 Thursday
August, 1999.
collapsed after consuming Hoyts Imitation Vodka Essence
June 19, 2001 Tuesday
December 15, 1997 Dylen Jones became angry with Dylen, who wouldn't stop crying, and struck the back of his head nine times with an open hand.
October 7, 2000
24
Springvale Monash Legal Service Inc The Coronial Process: Delays From Death To Inquest
6. REFERENCES
‘A Case for the Coroner’ Australian Broadcasting Corporation, Sydney, 2003
Coroner tackles fatal culture of repetition, The Age, 28 October 2004.
Interview with Coroner’s Assistant, Coroners Court 28 August 2004.
Interview with solicitor 11 October 2004. Firm anonymous.
Interview with senior constable, Homicide Squad, 25 October 2004
Interview with Margy Wilde-Brown, 23 September 2004
Dr David Ranson, “The role of the Pathologist in Homicide Investigations and Coronial
Inquiries”, Victorian Institute of Forensic Pathology. www.aic.gov.au/publications/proceedings/17/ranson.pdf
Unit entitled ‘Crash Course’ [Internet – http://www.motor.net.au/VACC/Media/]
State Coroner’s Office Victoria website, The Coronial Process [Internet –
http://www.Coronerscourt.vic.gov.au]
V Pleuckhahn, Ethics Legal Medicine and Forensic Pathology (Melbourne University
Press, 1983) p 9
V Plueckhan, ‘Light at the end of the Forensic Tunnel’ (1986) 60 Law Institute Journal
60, p1059
VACC interview with Sgt Peter Bellion, Victoria Police Major Collision Investigation
25
Recommended

















