
THE DENOMINATOR DILEMMA
CALCULATING SURGICAL SITE INFECTION RATESIN COLON SURGERY
NATIONAL HEALTH SAFETY NETWORKVS
NATIONAL SURGICAL QUALITY IMPROVEMENT PROGRAM
Albert W Dibbins MD, FACS Robert A Cormier, BSNB Stephen Prato AB, MSJennifer R Caiazzo RN
Maine Medical Center, Portland, Maine

Maine Medical Center

Maine Medical Center 2009-2010Organ Space Infection Rates
Colon Operations
Operation MMC OSI Rate NSQIP OSI Rate
All Colon CPT Codes 9.5% 5.5%
Intra-abdominal Colectomy/Anastomosis 8.2% 5.0%
Low Anterior Resection/Anastomosis 13.8% 4.8%

National Healthcare Safety Network (NHSN)Operative Procedure Category Mappings to ICD-9CM
Codes
Legacy Code – COLO
Operative Procedure – Colon Surgery
Description – Incision, resection, or anastomosis of the largeintestine: includes large-to-small and small-to-large bowel anastomosis; does not include rectal operations
ICD-9CM Codes – 17.31-17.36,17.39,45.03,45.26,45.41,45.49,45.5245.71-45.76,45.79,45.81-45.83,45.92-45.9546.03,46.04,46.10,46.11,46.13,46.14,46.43,46.5246.75,46.76,46.94

Problems in NHSN Reporting
1. ICD9-CM Codes
2. Coding Rules• use of multiple codes • selection of cases for inclusion• definition of a colon operation = segment resected• low anterior resection code is 48.63 - not included in COLO• colon biopsy (45.26) even if seromuscular only• suture of colotomy (46.75) whether transmural or not
3. Coders• use of proprietary software• human error

Problems in NHSN Reporting
4. Definitions“ The procedure represented by this ICD-9CM code may be performed
in a number of ways. However, if, at the end of the procedure, the skin incision edges do not meet because of drains, wires, or otherobjects extruding through the incision, the incision is not consideredprimarily closed. Therefore the procedure is not considered an NHSNoperative procedure and any subsequent infection is not considereda procedure associated infection (i.e. not an SSI..).”
5. Exclusions“There must be no evidence that the infection was present or incubatingat the time of admission to the health care setting.”
“The following infections are not considered healthcare associated- Infections associated with complications or extensions of infectionsalready present on admission, unless a change in pathogen or symptoms strongly suggests the acquisition of a new infection.”

Classic/Pediatric Targeted NHSN ? CMS 44025 44110 44111 44140 44140 4414044141 44141 4414144143 44143 4414344145 44145 4414544146 44146 4414644147 44147 4414744150 44150 4415044151 44151 4415144155 44155 44156 44157 44158 44160 44160 4416044188 44204 44204 4420444205 44205 4420544206 44206 4420644207 44207 4420744208 44208 4420844210 44210 4421044211 44211 44212 44212 44227 44227 44238* 44320 44322 44340 44345 44346 44620 44625 44626 44799
COLON CPT CODE COMPARISONS

Present At the Time Of Surgery
PATOS
1. Equivalent to the NHSN exclusion for infection present at admission
2. Workstation automatically deletes case from SSI list if PATOS collected
3. Need to keep PATOS file to know “true” SSI rate

Maine Medical Center“True” SSI Rates for Colon Operations 2011
NSQIP Comparison = All Hospitals, All Beds
MMC 358 cases NSQIP 35,385 casesSuperficial SSI 4.2% 6.4%Deep SSI 0.0% 1.4%Organ Space SSI 6.4% 3.5%
NSQIP Comparison = All NSQIP Pediatric Sites
MMC 35 cases NSQIP 1012 casesSuperficial SSI 5.7% 4.9%Deep SSI 0.0% 0.9%Organ Space SSI 8.6% 1.6%

Maine Medical CenterNSQIP Colon Targeted Option SSI Rates 2011
NSQIP Comparison – Academic/Teaching Hospitals 500 or more beds
MMC 320 cases NSQIP 15,898 cases
Superficial SSI 5.0% (4.2%) 6.7%
Deep SSI 0.0% (0.0%) 1.3%
Organ Space SSI 5.3% (6.4%) 4.0%
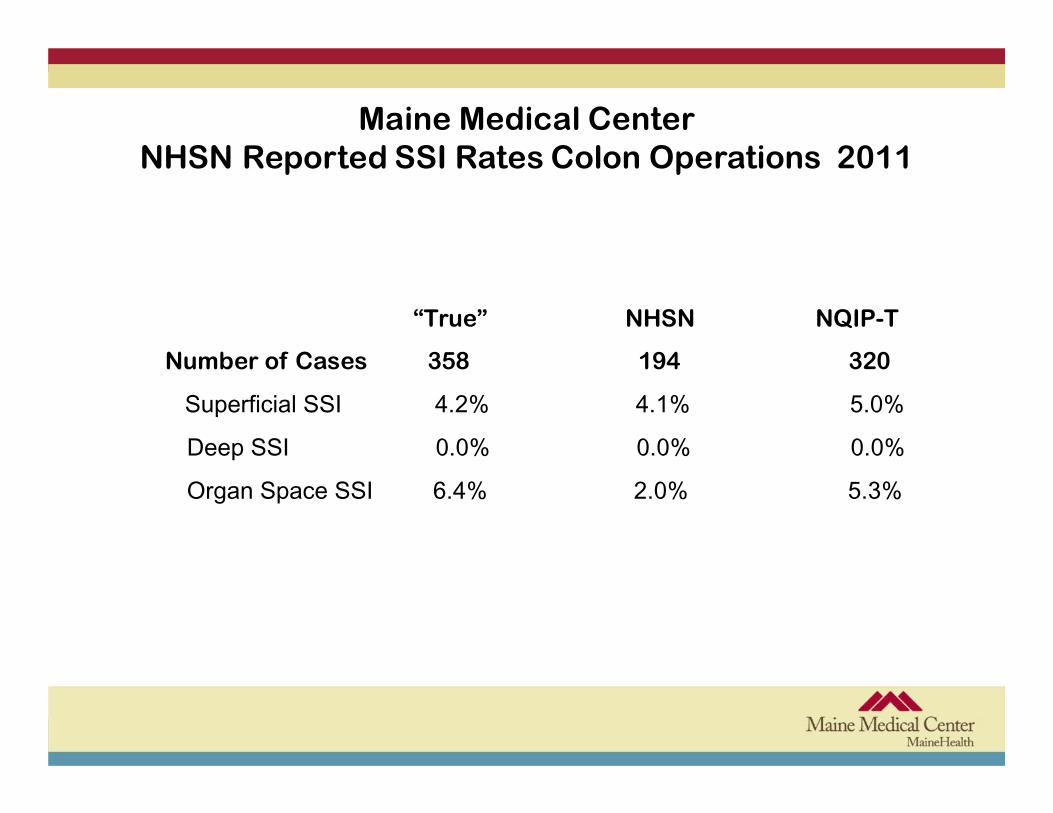
Maine Medical CenterNHSN Reported SSI Rates Colon Operations 2011
“True” NHSN NQIP-T
Number of Cases 358 194 320
Superficial SSI 4.2% 4.1% 5.0%
Deep SSI 0.0% 0.0% 0.0%
Organ Space SSI 6.4% 2.0% 5.3%
Calculating Hospital SSI rates
NHSN will calculate SSI rates based on their model using O/E ratios
The E comes from a multivariate logistic regression model constructed by NHSN to represent a standard population- it has been criticized as having poor predictive validity
“The Surgical Infection Rate will be calculated only if the number of hospital associated infections is >1”
The basic SSI Risk Index uses
1. duration of operation
2. wound class 3 or 4
3. ASA classification 3,4,5 BUT we don’t know how !

A Proposal
1. CMS and NHSN will define procedure by name i.e. low anteriorresection
2. CMS, NHSN and AHA coding group will assign ICD-9CM code, CPTcode for each operation
3. AHA coding group will work with CMS, NHSN to define coding rulesand provide education to coders.- interim solution for ICD-9CM, major effort for ICD-10CM
4. NSQIP and Colorectal societies should be heavily involved in theprocess
Recommended















![The Dilemma [Chapter 1: The Dilemma , Exponential Future]](https://img.pdfslide.net/doc/110x75/58eeb6841a28ab38788b4593/the-dilemma-chapter-1-the-dilemma-exponential-future.jpg)

