The Impact of Including Level III Trauma Centers in Pennsylvania
16th Annual PTSF/PaCOT Conference
October 25, 2012
Juliet Geiger RN, MSN –Executive Director, PTSFDavid Scaff, DO – Trauma Program Medical Director,
Pocono Medical Center

Historical Background
• 1985 – Standards of Accreditation for Adult L1/2 and Pediatric L1 trauma centers developed
• 1992 – L2 Pediatric Standards developed• 2004 – Act 15 0f 2004 signed mandating
L3 standards be developed• 2010 – L4 standards approved by PTSF
Board• 2012 – Five hospitals pursue L4
accreditation

Level III Accreditation History
• 2007 – First L3 accredited• 2008 – Two L3 centers in system• 2009 – Four L3 centers in system• 2010 – Two L3 center is system – 2
withdraw citing financial difficulties• 2011 – Two L3 in system. Pursuit funding
restored.• 2012 – One L3 in system. One withdraws.
Two hospitals pursuing L3 accreditation.

Level III Accreditation History
2007 2008 2009 2010 2011 20120
1
2
3
4
One withdrawsOne remainsTwo hospitals pursuing
2 withdraw citing financialdifficulties – state funding delayed Pursuit funding
restored

Questionnaire
• Questionnaire sent to eligible hospitals that received pursuit funding and those eligible hospitals that elected not to pursue accreditation in order to describe:– Reasons for pursuing or not pursuing Level III
accreditation– Barriers preventing a hospital from pursuing
accreditation– Barriers to becoming accredited for those that received
funding– Resources that would have helped with pursuit– Factors that would be necessary before pursuing
accreditation in the future.– Outcomes as a result of pursuit effort

Results:Reasons for Pursuing Accreditation
• Enhanced quality of care • Increased marketing of hospitals to
generate higher volumes of patients
• Receipt of grant funding

Results: Positive Outcomes
• Enhanced level of care of injured patients
• Improved care of all patients within hospital
• Implementing standardized protocols and policies for care of injured patients
• Energized nursing and physician staff in the care of injured patients
• Improved Performance Improvement efforts
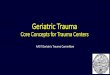
County A Injury Mortality Rates
2007 2008 2009 2010 2011
4.8
2 2.41.8 1.3
6.5
5.24.3 4.7
PTOS Mortality Rate DOH Mortality Rate
L3 Accreditation 11/1/09
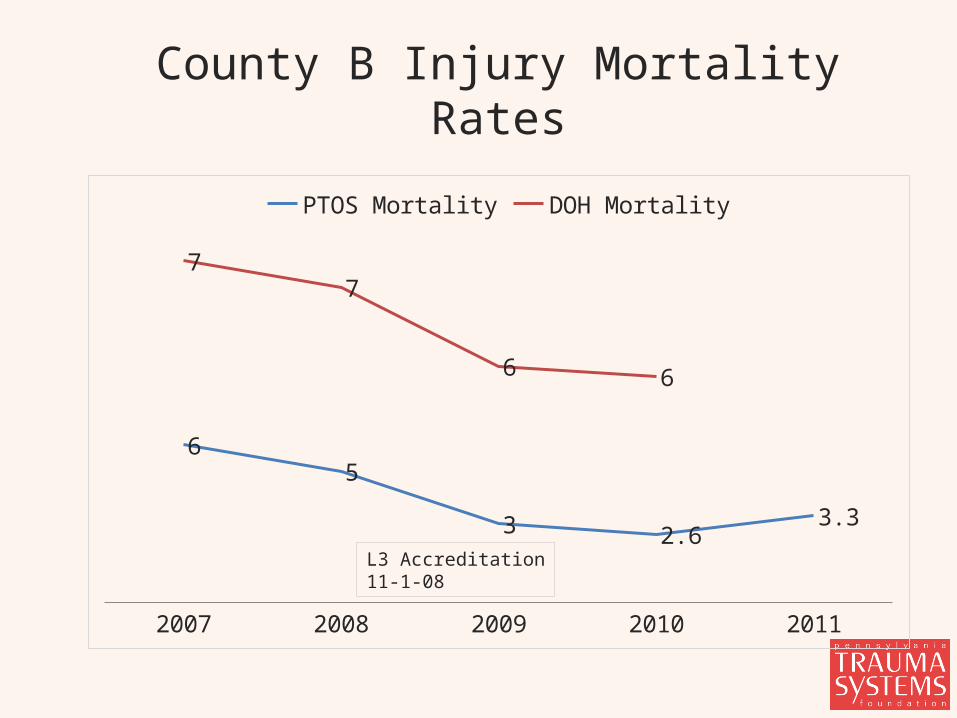
County B Injury Mortality Rates
2007 2008 2009 2010 2011
65
3 2.63.3
77
6 6
PTOS Mortality DOH Mortality
L3 Accreditation11-1-08

Barriers to Pursuing Accreditation: Surgeon Support
Feared increased patient volumes and injury severity
2 yr
s Pr
e-Acc
red
1 yr
Pre
-Acc
red
1st y
ear a
s TC
2nd
year
as T
C
0
40
80
120
160
AdmissionsTransfers outOrtho consultsAdmit to orthoAvg ISSGS admits
1 yr Pre-Accred
1st year as TC
2nd year as TC
3rd year as TC
050
100150200250300350400450500
AdmissionsTransfers OutOrtho consultsAdmit to OrthoAvg ISSGS Admits
County A (accredited 2009) County B (Accredited 2008)

Barriers to Pursuing Accreditation: Physician Leadership
• Trauma Medical Director must be a surgeon
• Rural areas predominately have private practice physician groups
• Peer Review process challenging

Barriers to Pursuing Accreditation: Funding
• Administration feared insufficient funding and disappearance of funding.
• In 2010 a two year delay did occur due to the West Virginia lawsuit that delayed trauma funding to all trauma centers and those pursuing accreditation.

Barriers to Pursing Accreditation:Education
• From PTSF– Education limited to state wide in-
person forums with limited 1:1 visits– L3 inclusion started almost 20 years
after L1/2 trauma centers developed
• From Trauma Centers – Unclear of role and how to support L3
development– Not fully supportive of L3 inclusion in
PA.
PTSF Next Steps… • Foster relationship building between
higher level trauma centers and their rural colleagues
• Enhance PTSF’s educational approach • Continue Level IV trauma center
development• Perform trauma system research geared
toward measuring the trauma center/system value.
• Continue to advocate for state and federal funding of trauma centers
• Embark on a public education campaign
Recommended