SPECIAL FEATURE New strategy for HER-2 testing and trastuzumab therapy
The role of trastuzumab in the management of HER2-positivemetastatic breast cancer: an updated review
Yutaka Tokuda Æ Yasuhiro Suzuki ÆYuki Saito Æ Shinobu Umemura
Received: 11 January 2009 / Accepted: 21 May 2009 / Published online: 17 July 2009
� The Japanese Breast Cancer Society 2009
Abstract Currently, trastuzumab is one of the key drugs
in the treatment strategy for HER2-positive breast cancer.
Although metastatic breast cancer is unlikely to be cured,
some HER2-positive patients have survived for a long time
with complete response to trastuzumab therapy. In HER2-
positive metastatic breast cancer, single agent trastuzumab
is effective and less toxic. Combination of trastuzumab
with cytotoxic drugs is also effective. Therefore, major
guidelines recommend using trastuzumab as a key drug in
the management of HER2-positive metastatic breast can-
cer. However, many clinical questions still need to be
solved. In this article, recent evidence was reviewed to find
some answers about these issues.
Keywords Metastatic breast cancer � HER2-positive �Trastuzumab
Introduction
Currently, trastuzumab is one of the key drugs in the
treatment strategy for HER2-positive breast cancer.
Although metastatic breast cancer is unlikely to be cured,
some patients have survived for a long time with complete
response to trastuzumab therapy [1]. In HER2-positive
metastatic breast cancer, single agent trastuzumab is
effective with favorable toxicity. Combination of trast-
uzumab with cytotoxic drugs is also effective. Therefore,
major guidelines recommend using trastuzumab as a key
drug in the treatment strategy of HER2-positive metastatic
breast cancer. However, many clinical questions still need
to be solved. In this article, recent evidence is reviewed to
find some answers about these issues.
Trastuzumab combined with hormone therapy for
HER2 and hormone receptor-positive breast cancer
To select proper treatment, tumor biology and clinical
factors should be considered for each patient. Approxi-
mately half of breast cancers are HER2-positive as well as
hormone receptor-positive. Generally, endocrine therapy is
preferred for initial treatment of hormone receptor-positive
metastatic breast cancer because of its favorable toxic
profile. The National Comprehensive Cancer Network
(NCCN) guideline recommends trastuzumab for beyond
first-line therapy in patients refractory to standard endo-
crine therapy [2]. However, preclinical [3] and clinical [4]
evidence suggests that HER2 positivity gives intrinsic
resistance to hormone therapy. The targeting of both hor-
mone receptors and HER2 signaling pathways in hormone
receptor and HER2-positive breast cancers may overcome
resistance to anti-estrogen therapy. Thus, another option
for HER2-positive and hormone receptor-positive meta-
static breast cancer patients is the combination of trast-
uzumab and endocrine therapy.
In terms of this issue, a randomized trial was conducted
[5]. The TAnDEM study randomly assigned 208 post-
menopausal patients with HER2-positive and hormone
receptor-positive metastatic breast cancer to anastrozole
alone or anastrozole plus trastuzumab. Anastrozole 1 mg
Y. Tokuda (&) � Y. Suzuki � Y. Saito
Department of Breast and Endocrine Surgery, Tokai University
School of Medicine, 143 Shimokasuya, Isehara,
Kanagawa 259-1193, Japan
e-mail: [email protected]
S. Umemura
Department of Pathology, Tokai University School of Medicine,
143 Shimokasuya, Isehara, Kanagawa 259-1193, Japan
123
Breast Cancer (2009) 16:295–300
DOI 10.1007/s12282-009-0142-8

was administered daily, and trastuzumab 4 mg/kg of
loading dose was administered on week 1 followed by
2 mg/kg weekly until disease progression. Crossover to
receive trastuzumab was actively offered to all patients
who progressed on anastrozole alone. A preliminary anal-
ysis reported that benefits of combination showed a sig-
nificantly better overall response rate (20 vs. 7%) as well as
progression-free survival (4.8 vs. 2.4 months, P = 0.0016).
Seventy percent of the patients initially assigned to anas-
trozole alone received trastuzumab later during the course
of the disease. Overall survival of the combination group
was 28.5 months compared with 23.9 months for the an-
astrozole alone group (P = 0.325). Cardiac toxicity
developed in 13 of 103 patients of the combination group
compared with 2 of 104 patients of the anastrozole alone
group. Therefore, combinations of hormone therapy plus
trastuzumab for patients with HER2-positive metastatic
breast cancer seem to be safe and have promising efficacy.
Trastuzumab alone versus trastuzumab plus
chemotherapy as first-line treatment
Trastuzumab monotherapy has shown efficacy and is well
tolerated. Thus, the NCCN guideline recommends both
trastuzumab alone and combination of trastuzumab and
chemotherapy as first-line treatment for HER-positive
metastatic breast cancer patients [2]. However, the clinical
question of whether trastuzumab monotherapy followed by
trastuzumab and chemotherapy at disease progression has
equal efficacy to an initial combination therapy of trast-
uzumab and chemotherapy remains to be answered. A
randomized phase III study of trastuzumab monotherapy
followed by docetaxel and trastuzumab versus the combi-
nation of trastuzumab and docetaxel as first-line treatment
was conducted in Japan.
A result of the first-analysis was reported at the San
Antonio Breast Cancer Symposium in 2008 [6]. Eligible
patients had HER2-positive metastatic breast cancer with a
measurable tumor based on RECIST, ECOG performance
status 0 or 1, and left ventricular ejection fraction more than
50%. Patients with prior chemotherapy for metastatic breast
cancer, adjuvant trastuzumab and docetaxel were excluded.
The patients were randomly assigned to sequential weekly
trastuzumab 2 mg/kg (loading 4 mg/kg) alone followed by
a combination of docetaxel (60 mg/m2 every 3 weeks) and
trastuzumab at disease progression or concurrent combi-
nation of trastuzumab and docetaxel. Primary endpoints
were time to progression of trastuzumab alone and combi-
nation of trastuzumab and docetaxel and overall survival.
Secondary endpoints were overall response rates, progres-
sion-free survival of sequential trastuzumab monotherapy
followed by docetaxel and trastuzumab, time to treatment
failure of trastuzumab monotherapy versus the initial
combination group and safety in both arms.
The planned sample size was 80 patients in each group.
The Independent Data Management Committee recom-
mended stopping recruitment because there was a signifi-
cant difference in death rate. Finally, 112 patients were
enrolled, and 107 patients were analyzed. Statistically
significant progression-free survival was observed for the
trastuzumab and docetaxel group compared with the
trastuzumab monotherapy group (HR: 4.24, P \ 0.0001).
In terms of overall survival, the results suggested that the
combination group was superior to the sequential group
(HR: 2.72, P = 0.0352), though the number of deaths was
insufficient. Time to treatment failure was significantly
superior in the combination group. Overall response rates
were 67.9% for the combination group, 14.8% for trast-
uzumab monotherapy and 47.2% for sequential trast-
uzumab and docetaxel. According to the above evidence, a
combination of trastuzumab and cytotoxic drugs could be
considered as standard for first-line therapy.
Trastuzumab combined with anthracyclines
In preclinical studies, cisplatin, thiotepa and etoposide
were found to be synergistic with trastuzumab. Additive
interactions were observed with doxorubicin, paclitaxel,
methotrexate and vinblastine [7]. Thus, to determine the
efficacy and safety of trastuzumab in combination with
chemotherapy as a first-line treatment for patients with
HER-2-overexpressing metastatic breast cancers, a ran-
domized, placebo-controlled, multicenter, multinational
phase III trial was designed [8]. Patients without prior
anthracycline treatment were randomly grouped to receive
trastuzumab plus anthracycline (doxorubicin or epirubicin)/
cyclophosphamide (AC) or AC alone. Cyclophosphamide
(600 mg/m2) was administered in combination with
doxorubicin (80 mg/m2) or epirubicin (75 mg/m2). Che-
motherapy was repeated every 3 weeks for six cycles.
Patients with prior anthracycline treatment in the adjuvant
setting received either trastuzumab plus paclitaxel or just
paclitaxel. Paclitaxel (175 mg/m2) was administered by IV
infusion over a 3-h period, after premedication. Four
hundred sixty-nine HER-2-overexpressing breast cancer
patients without prior chemotherapy for metastatic disease
were enrolled.
The overall response rates were 60% for trastuzumab
plus AC and 42% for AC alone. Median duration of
response was 9.1 months for trastuzumab plus AC and
6.5 months for AC alone (P = 0.0025). Median time to
progression was 8.1 months for trastuzumab plus AC and
6.0 months for AC alone. Median overall survival was
31 months for trastuzumab plus AC and 21 months for AC
296 Breast Cancer (2009) 16:295–300
123
alone. Therefore, trastuzumab plus concomitant anthracy-
clines demonstrated significant clinical activity.
A syndrome of cardiac dysfunction was reported more
commonly with trastuzumab plus AC (27%; NYHA class
III or IV) than with AC alone (8%), paclitaxel alone (1%),
or trastuzumab plus paclitaxel (13%). To date, the mech-
anism of adverse effects of trastuzumab on cardiac function
has not been fully explained. These results led to the
general recommendation that combined use of anthracy-
clines and trastuzumab should be avoided. However,
combining trastuzumab with anthracyclines is still attrac-
tive. Thus, some recent trials showed impressive efficacy
and no significant cardiotoxicity with the combination. At
the neoadjuvant setting, trastuzumab was used concurrently
with fluorouracil, epirubicin and cyclophosphamide with-
out significant cardiotoxicity [9]. For metastatic breast
cancer, epirubicin or liposomal doxorubicin was also
investigated to obtain more than 60% overall response rates
without significant cardiotoxicity [10–12] (Table 1).
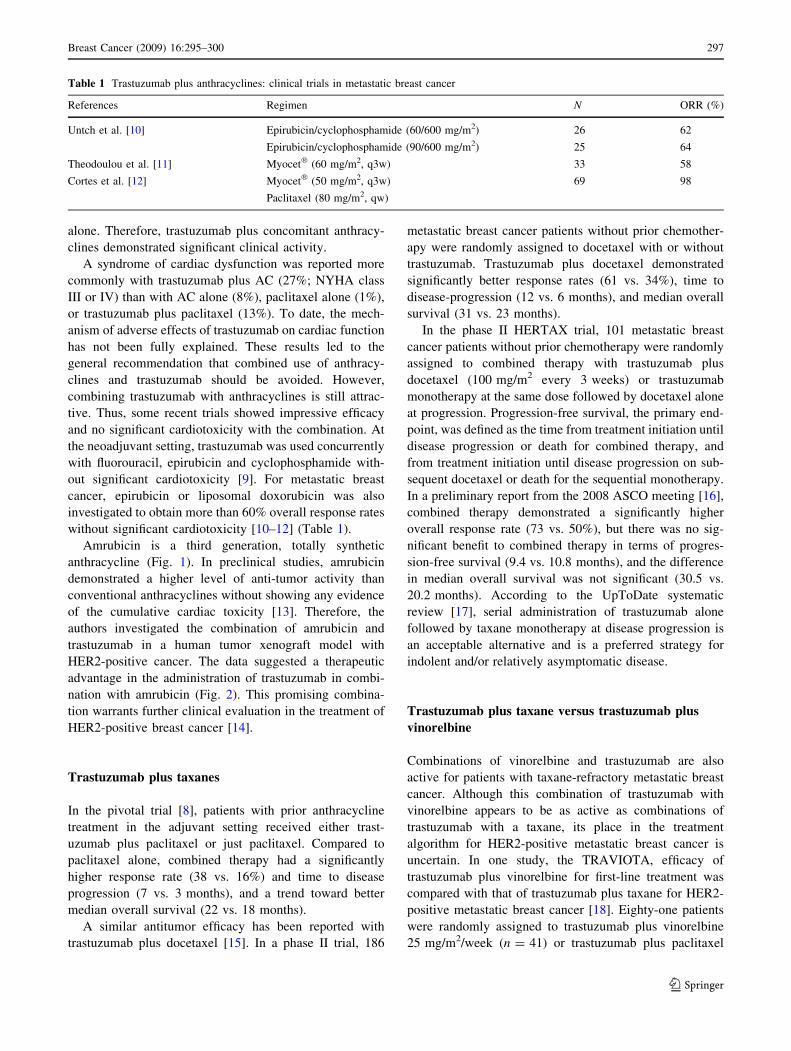
Amrubicin is a third generation, totally synthetic
anthracycline (Fig. 1). In preclinical studies, amrubicin
demonstrated a higher level of anti-tumor activity than
conventional anthracyclines without showing any evidence
of the cumulative cardiac toxicity [13]. Therefore, the
authors investigated the combination of amrubicin and
trastuzumab in a human tumor xenograft model with
HER2-positive cancer. The data suggested a therapeutic
advantage in the administration of trastuzumab in combi-
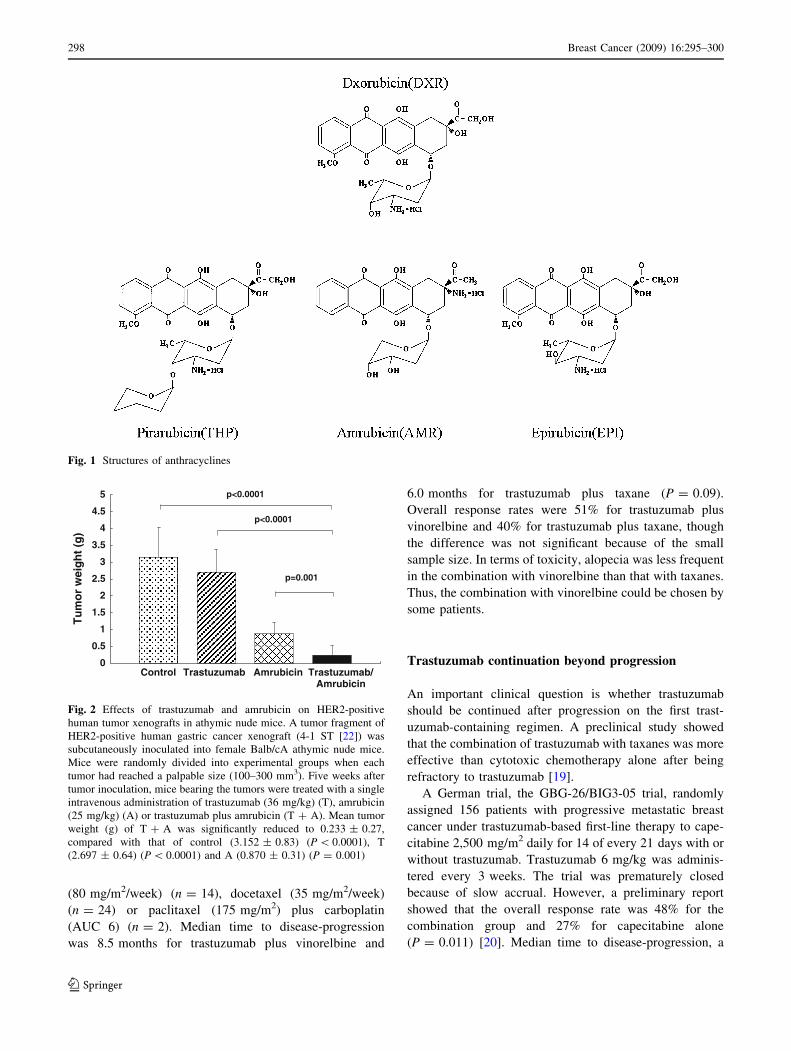
nation with amrubicin (Fig. 2). This promising combina-
tion warrants further clinical evaluation in the treatment of
HER2-positive breast cancer [14].
Trastuzumab plus taxanes
In the pivotal trial [8], patients with prior anthracycline
treatment in the adjuvant setting received either trast-
uzumab plus paclitaxel or just paclitaxel. Compared to
paclitaxel alone, combined therapy had a significantly
higher response rate (38 vs. 16%) and time to disease
progression (7 vs. 3 months), and a trend toward better
median overall survival (22 vs. 18 months).
A similar antitumor efficacy has been reported with
trastuzumab plus docetaxel [15]. In a phase II trial, 186
metastatic breast cancer patients without prior chemother-
apy were randomly assigned to docetaxel with or without
trastuzumab. Trastuzumab plus docetaxel demonstrated
significantly better response rates (61 vs. 34%), time to
disease-progression (12 vs. 6 months), and median overall
survival (31 vs. 23 months).
In the phase II HERTAX trial, 101 metastatic breast
cancer patients without prior chemotherapy were randomly
assigned to combined therapy with trastuzumab plus
docetaxel (100 mg/m2 every 3 weeks) or trastuzumab
monotherapy at the same dose followed by docetaxel alone
at progression. Progression-free survival, the primary end-
point, was defined as the time from treatment initiation until
disease progression or death for combined therapy, and
from treatment initiation until disease progression on sub-
sequent docetaxel or death for the sequential monotherapy.
In a preliminary report from the 2008 ASCO meeting [16],
combined therapy demonstrated a significantly higher
overall response rate (73 vs. 50%), but there was no sig-
nificant benefit to combined therapy in terms of progres-
sion-free survival (9.4 vs. 10.8 months), and the difference
in median overall survival was not significant (30.5 vs.
20.2 months). According to the UpToDate systematic
review [17], serial administration of trastuzumab alone
followed by taxane monotherapy at disease progression is
an acceptable alternative and is a preferred strategy for
indolent and/or relatively asymptomatic disease.
Trastuzumab plus taxane versus trastuzumab plus
vinorelbine
Combinations of vinorelbine and trastuzumab are also
active for patients with taxane-refractory metastatic breast
cancer. Although this combination of trastuzumab with
vinorelbine appears to be as active as combinations of
trastuzumab with a taxane, its place in the treatment
algorithm for HER2-positive metastatic breast cancer is
uncertain. In one study, the TRAVIOTA, efficacy of
trastuzumab plus vinorelbine for first-line treatment was
compared with that of trastuzumab plus taxane for HER2-
positive metastatic breast cancer [18]. Eighty-one patients
were randomly assigned to trastuzumab plus vinorelbine
25 mg/m2/week (n = 41) or trastuzumab plus paclitaxel
Table 1 Trastuzumab plus anthracyclines: clinical trials in metastatic breast cancer
References Regimen N ORR (%)
Untch et al. [10] Epirubicin/cyclophosphamide (60/600 mg/m2) 26 62
Epirubicin/cyclophosphamide (90/600 mg/m2) 25 64
Theodoulou et al. [11] Myocet� (60 mg/m2, q3w) 33 58
Cortes et al. [12] Myocet� (50 mg/m2, q3w) 69 98
Paclitaxel (80 mg/m2, qw)
Breast Cancer (2009) 16:295–300 297
123
(80 mg/m2/week) (n = 14), docetaxel (35 mg/m2/week)
(n = 24) or paclitaxel (175 mg/m2) plus carboplatin
(AUC 6) (n = 2). Median time to disease-progression
was 8.5 months for trastuzumab plus vinorelbine and
6.0 months for trastuzumab plus taxane (P = 0.09).
Overall response rates were 51% for trastuzumab plus
vinorelbine and 40% for trastuzumab plus taxane, though
the difference was not significant because of the small
sample size. In terms of toxicity, alopecia was less frequent
in the combination with vinorelbine than that with taxanes.
Thus, the combination with vinorelbine could be chosen by
some patients.
Trastuzumab continuation beyond progression
An important clinical question is whether trastuzumab
should be continued after progression on the first trast-
uzumab-containing regimen. A preclinical study showed
that the combination of trastuzumab with taxanes was more
effective than cytotoxic chemotherapy alone after being
refractory to trastuzumab [19].
A German trial, the GBG-26/BIG3-05 trial, randomly
assigned 156 patients with progressive metastatic breast
cancer under trastuzumab-based first-line therapy to cape-
citabine 2,500 mg/m2 daily for 14 of every 21 days with or
without trastuzumab. Trastuzumab 6 mg/kg was adminis-
tered every 3 weeks. The trial was prematurely closed
because of slow accrual. However, a preliminary report
showed that the overall response rate was 48% for the
combination group and 27% for capecitabine alone
(P = 0.011) [20]. Median time to disease-progression, a
Fig. 1 Structures of anthracyclines
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Tu
mo
r w
eig
ht
(g)
Control Trastuzumab Amrubicin Trastuzumab/Amrubicin
p<0.0001
p<0.0001
p=0.001
Fig. 2 Effects of trastuzumab and amrubicin on HER2-positive
human tumor xenografts in athymic nude mice. A tumor fragment of
HER2-positive human gastric cancer xenograft (4-1 ST [22]) was
subcutaneously inoculated into female Balb/cA athymic nude mice.
Mice were randomly divided into experimental groups when each
tumor had reached a palpable size (100–300 mm3). Five weeks after
tumor inoculation, mice bearing the tumors were treated with a single
intravenous administration of trastuzumab (36 mg/kg) (T), amrubicin
(25 mg/kg) (A) or trastuzumab plus amrubicin (T ? A). Mean tumor
weight (g) of T ? A was significantly reduced to 0.233 ± 0.27,
compared with that of control (3.152 ± 0.83) (P \ 0.0001), T
(2.697 ± 0.64) (P \ 0.0001) and A (0.870 ± 0.31) (P = 0.001)
298 Breast Cancer (2009) 16:295–300
123

primary endpoint, was 8.2 months for the combination
group and 5.6 months for the capecitabine alone group
(HR = 0.69, P = 0.034). Median overall survival was
25.5 months for the combination and 20.4 months for the
capecitabine group (HR = 0.76, P = 0.26). Therefore,
continuing trastuzumab beyond progression appears to
improve the efficacy of second-line capecitabine treatment.
Trastuzumab plus lapatinib versus lapatinib
monotherapy
A benefit for continued trastuzumab after progression was
also suggested in a randomized trial, EGF104900, pre-
sented at the 2008 ASCO meeting [21]. The trial assigned
296 patients with progressive metastatic breast cancer
under trastuzumab-based therapy to lapatinib alone
(1,500 mg, daily) and lapatinib (1,000 mg, daily) plus
continuation of trastuzumab. The overall response rate was
10.3% for combined therapy and 6.9% for lapatinib alone
(P = 0.46). Clinical benefit rates were 24.7 and 12.4% for
combined therapy and lapatinib alone, respectively (P =
0.01). Median progression-free survival was 2.8 months for
combined therapy and 1.9 months for lapatinib alone
(P = 0.008), although overall survival was not signifi-
cantly different.
In conclusion, according to the data obtained so far, the
authors recommend a treatment algorithm as shown in the
Fig. 3. Hormone receptor-positive patients with favorable
prognosis such as bone or soft tissue metastases only are
recommended to be treated by endocrine therapy and
concurrent trastuzumab. Hormone receptor- negative
patients, hormone receptor-positive and endocrine refrac-
tory patients, or hormone receptor-positive patients with
unfavorable prognosis should be treated by trastuzumab
combined with chemotherapy. After disease progression on
a first-line trastuzumab-containing regimen, trastuzumab
should be continued with a second- or third-line chemo-
therapy. After approval of lapatinib in Japan, the regimen
of capecitabine and lapatinib is also an option for patients
progressive on a trastuzumab-containing regimen.
References
1. Ohta M, Tokuda Y, Suzuki Y, Kubota M, Watanabe T, Fujii H,
et al. A case with HER2-overexpressing breast cancer completely
responded to humanized anti-HER2 monoclonal antibody. Jpn J
Clin Oncol. 2001;31:553–6.
2. National Comprehensive Cancer Network (NCCN). http://www.
nccn.org/professionals/physician_gls/default.asp.
3. Pietras RJ, Arboleda J, Reese DM, Wongvipat N, Pegram MD,
Ramos L, et al. HER-2 tyrosine kinase pathway targets estrogen
receptor and promotes hormone-independent growth in human
breast cancer cells. Oncogene. 1995;10:2435–46.
4. Carlomagno C, Perrone F, Gallo C, De Laurentiis M, Lauria R,
Morabito A, et al. c-erb B2 overexpression decreases the benefit
of adjuvant tamoxifen in early-stage breast cancer without axil-
lary lymph node metastases. J Clin Oncol. 1996;14:2702–8.
5. Mackey JR, Kaufman B, Clemens M, Bapsy PP, Vaid A, Wardley
A, Tjulandin S, Jahn M, Lehle M, Jones A. Trastuzumab prolongs
progression-free survival in hormone-dependent and HER2-
positive metastatic breast cancer. San Antonio Breast Cancer
Symposium 2006; abstract 3.
6. Nakagami K, Inoue K, Mizutani M, Hozumi Y, Fujiwara Y,
Masuda N, Tsukamoto F, Saito M, Ohashi Y, Sano M, Noguchi
S. Randomized Phase III study of trastuzumab monotherapy
followed by docetaxel and trastuzumab versus the combination of
trastuzumab and docetaxel as first-line treatment in patients with
HER2 positive metastatic breast cancer. San Antonio Breast
Cancer Symposium 2008; abstract 3132.
7. Pegram M, Hsu S, Lewis G, et al. Inhibitory effects of combi-
nations of HER-2/neu antibody and chemotherapeutic agents
used for treatment of human breast cancers. Oncogene. 1999;
18:2241–51.
8. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V,
Bajamonde A, et al. Use of chemotherapy plus a monoclonal
antibody against HER2 for metastatic breast cancer that overex-
presses HER2. N Engl J Med. 2001;344:783–92.
9. Buzdar AU, Ibrahim NK, Francis D, Booser DJ, Thomas ES,
Theriault RL, et al. Significantly higher pathologic complete
remission rate after neoadjuvant therapy with trastuzumab, pac-
litaxel, and epirubicin chemotherapy: results of a randomized trial
in human epidermal growth factor receptor 2-positive operable
breast cancer. J Clin Oncol. 2005;23:3676–85.
10. Untch M, Eidtmann H, du Bois A, Meerpohl HG, Thomssen CH,
Ebert A, et al. Cardiac safety of trastuzumab in combination with
epirubicin and cyclophosphamide in women with metastatic
breast cancer: results of a phase I trial. Eur J Cancer. 2004;
40:988–97.
systemic disease
hormone receptor positive hormone receptor negative or
hormone receptor positive and symptomatic visceral tumor
trastuzumab+
1st-line 2nd-line 3rd-line
……
chemotherapy
trastuzumab+
1st-line 2nd-line ……
endocrine therapy
trastuzumab+
1st-line 2nd-line 3rd-line
……
chemotherapy
Fig. 3 Algorithm for treatment selection for HER2-positive meta-
static breast cancer
Breast Cancer (2009) 16:295–300 299
123

11. Theodoulou M, Campos SM, Batist G, Winer E, Norton L, Hudis
C, et al. TLC D99 (D, Myocet) and Herceptin (H) is safe in
advanced breast cancer (ABC): final cardiac safety and efficacy
analysis. Proc Am Soc Clin Oncol. 2002;21:55a. abstract.
12. Cortes J, Dicosimo S, Climent MA, Cortes-Funes H, Lluch A,
Gascon P, et al. Nonpegylated liposomal doxorubicin (TLC-
D99), paclitaxel, and trastuzumab in HER-2-overexpressing
breast cancer: a multicenter phase I/II Study. Clin Cancer Res.
2009;15:307–14.
13. Suzuki T, Minamide S, Iwasaki T, Yamamoto H, Kanda H.
Cardiotoxicity of a new anthracycline derivative (SM-5887)
following intravenous administration to rabbits: comparative
study with doxorubicin. Invest New Drugs. 1997;15:219–25.
14. Tokuda Y, Umemura S, Saito Y, Suzuki Y. Enhanced anti-tumor
effect of trastuzumab combined with less cardiotoxic anthracy-
cline, amrubicin, in HER2 positive human cancer xenografts in
athymic mice. J Clin Oncol. 2008;26:abstract 14641.
15. Marty M, Cognetti F, Maraninchi D, Snyder R, Mauriac L,
Tubiana-Hulin M, et al. Randomized phase II trial of the efficacy
and safety of trastuzumab combined with docetaxel in patients
with human epidermal growth factor receptor 2-positive meta-
static breast cancer administered as first-line treatment: the
M77001 study group. J Clin Oncol. 2005;23:4265–74.
16. Bontenbal M, Seynaeve C, Stouthard J, Bos M, Braun H,
Erdkamp FL, et al. Randomized study comparing efficacy/toxicity
of monotherapy trastuzumab followed by monotherapy docetaxel
at progression, and combination trastuzumab/docetaxel as first-
line chemotherapy in Her2-neu positive, metastatic breast cancer
(HERTAX study). J Clin Oncol. 2008;26:44s. abstract 1014.
17. Hayes D. Systemic therapy for HER2-positive metastatic breast
cancer. UpToDate version 16.3.
18. Burstein HJ, Keshaviah A, Baron A, Hart R, Lambert-Falls R,
Marcom PK, et al. Trastuzumab and vinorelbine or taxane che-
motherapy for HER2 ? metastatic breast cancer: the TRAVI-
OTA study. J Clin Oncol. 2006;24:18s. abstract 650.
19. Fujimoto-Ouchi K, Sekiguchi F, Mori K. Preclinical study of
continuous administration of trastuzumab as combination therapy
after disease progression with trastuzumab monotherapy. Proc
Amer Assoc Cancer Res. 2005;46:abstract 5062.
20. Von Minckwitz G, Zielinski C, Maarteense E, Vogel P, Schmidt M,
Eidtmann H, et al. Capecitabine vs. capecitabine ? trastuzumab in
patients with HER2-positive metastatic breast cancer progressing
during trastuzumab treatment: The TBP phase III study (GBG 26/
BIG 3-05). J Clin Oncol. 2008;26:47s. abstract 1025.
21. O’Shaughnessy J, Blackwell KL, Burstein H, Storniolo AM,
Sledge G, Baselga J, et al. A randomized study of lapatinib alone
or in combination with trastuzumab in heavily pretreated
HER2 ? metastatic breast cancer progressing on trastuzumab
therapy. J Clin Oncol. 2008;26:44s. abstract 1015.
22. Tokuda Y, Ohnishi Y, Shimamura K, Iwasawa M, Yoshimura M,
Ueyama Y, et al. In vitro and in vivo anti-tumor effects of a
humanized monoclonal antibody against c-erbB-2 product. Br J
Cancer. 1996;73:1362–5.
300 Breast Cancer (2009) 16:295–300
123
Recommended





![HER2/neu: an increasingly important therapeutic target. · PDF filedomain II that permit heterodimerization [21,22], the relative activity of anti-HER2 antibodies (trastuzumab and](https://img.pdfslide.net/doc/110x75/5a76d20d7f8b9a0d558d7720/her2neu-an-increasingly-important-therapeutic-target-domain-ii-that-permit.jpg)