5/9/2015
1
The Who, What and When: Candidate Selection in Lung
Transplantation
Steven Hays, MDAssociate Professor
Medical Director, Lung TransplantationUCSF Medical Center
Disclosures
I have nothing to disclose
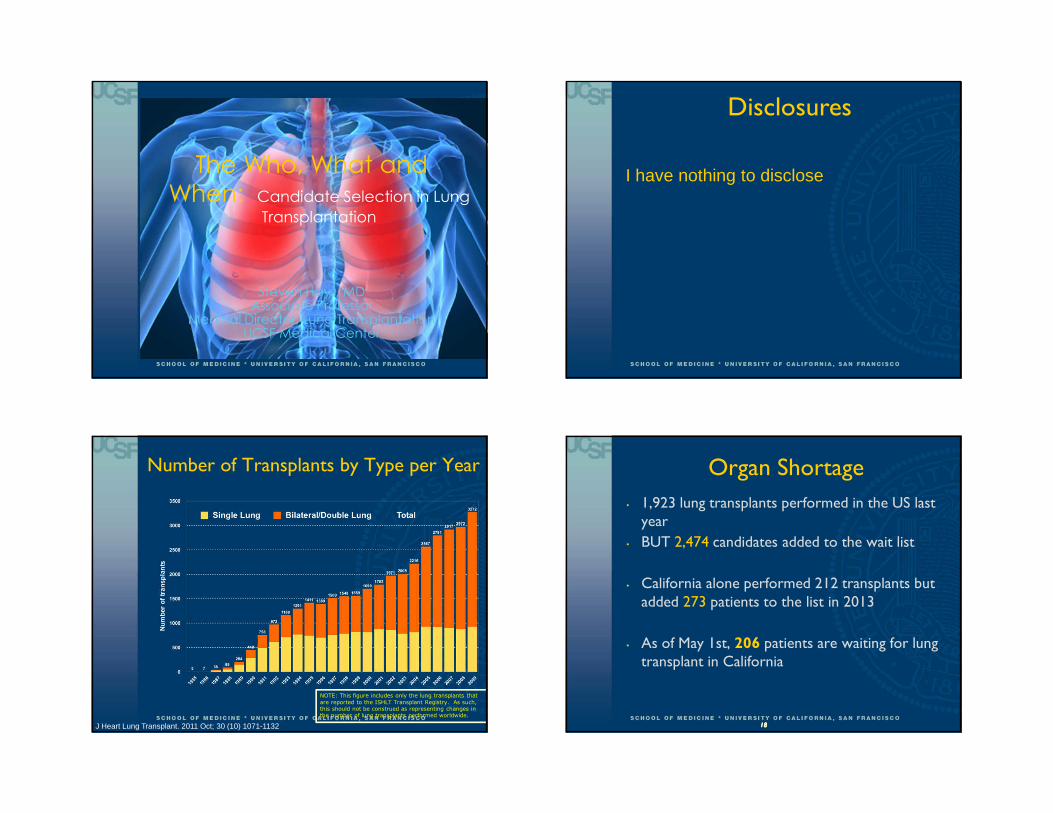
Number of Transplants by Type per Year
NOTE: This figure includes only the lung transplants that
are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
J Heart Lung Transplant. 2011 Oct; 30 (10) 1071-1132 18181818
Organ Shortage
• 1,923 lung transplants performed in the US last year
• BUT 2,474 candidates added to the wait list
• California alone performed 212 transplants but added 273 patients to the list in 2013
• As of May 1st, 206 patients are waiting for lung transplant in California
5/9/2015
2
Given the limits of organ availability, it is imperative that teams select patients who are likely to sustain a survival benefit
18181818
Lung TransplantationIndications
• A consensus document for the selection of lung transplant candidates - JHLT January 2015
• Chronic advanced lung disease
• Failed medical management
• Primary goal is improved duration of life but improved quality of life is also a consideration
• For most patients the ultimate “treatment” rather than cure
• Trading one medical condition for another
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
The Who and What?
• Pulmonary Vascular Disease
• PAH
• PH secondary to systemic disease
• Eisenmenger’s syndrome
• Obstructive Lung Disease
• COPD
• A1ATd
• Suppurative Lung Disease
• Cystic Fibrosis
• Bronchiectasis
• Restrictive Lung Disease
• IPF
• NSIP
• Sarcoidosis
• Eosinophilic granuloma
• LAM
• Occupational lung disease
• Hypersensitivity neumonitis
• Bronchiolitis obliterans
JHLT. 2013 Oct; 32(10): 965-978
Lung TransplantMajor Indications By Year

5/9/2015
3
UCSF Transplant Recipient CharacteristicsDeceased Donor Transplants Patients transplanted between 01/01/2010 and
12/31/2010
UCSF Region US
PAH 8.7 5.8 5.5
CF 8.7 14.0 14.5
IPF 65.2 47.5 45.8
COPD 17.4 31.9 29.9
Other 0 0.8 4.2
Timing of ReferralGeneral Recommendations
• High risk (>50%) of death due to lung disease within 2 years if lung transplant not performed
• High likelihood (>80%) of surviving at least 90 days after lung transplantation
• High likelihood (>80%) of 5–year post – transplant survival from a general medical perspective provided there is good graft function
• Early referral is highly desirable
• Aids in the psychology of accepting and confronting life-threatening illness
• Aids in actively managing end-stage illness
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
Absolute Contraindications� Malignancy
• Within 2 years except basal and squamous cell of skin
• 5 years disease free for breast CA > stage 2, colon > Dukes A, melanoma > level III or extra-capsular renal cell CA
• Untreatable advanced organ dysfunction
• Untreatable atherosclerotic disease
• Acute medical instability
• Active TB
• Heart disease
• Cardiomyopathy
• Ungraftable CAD
• Significant chest wall/spinal deformity
• Class II or III obesity (BMI > 35)
• Major psychosocial derangement or Non-adherence
• Current tobacco or drug use
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
Relative Contraindications
• Age > 65 years if low reserve or other relative contraindications
• Critical or unstable condition
• Severely limited functional status
• Colonization with highly resistant or virulent bacteria
• Class I obesity: BMI 30-35
• Severe malnutrition
• Severe osteoporosis
• Extensive prior chest surgery
• Hepatitis B or C, HIV
• Infections with B. cepacia, B gladioli, M. abscessus
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
5/9/2015
4
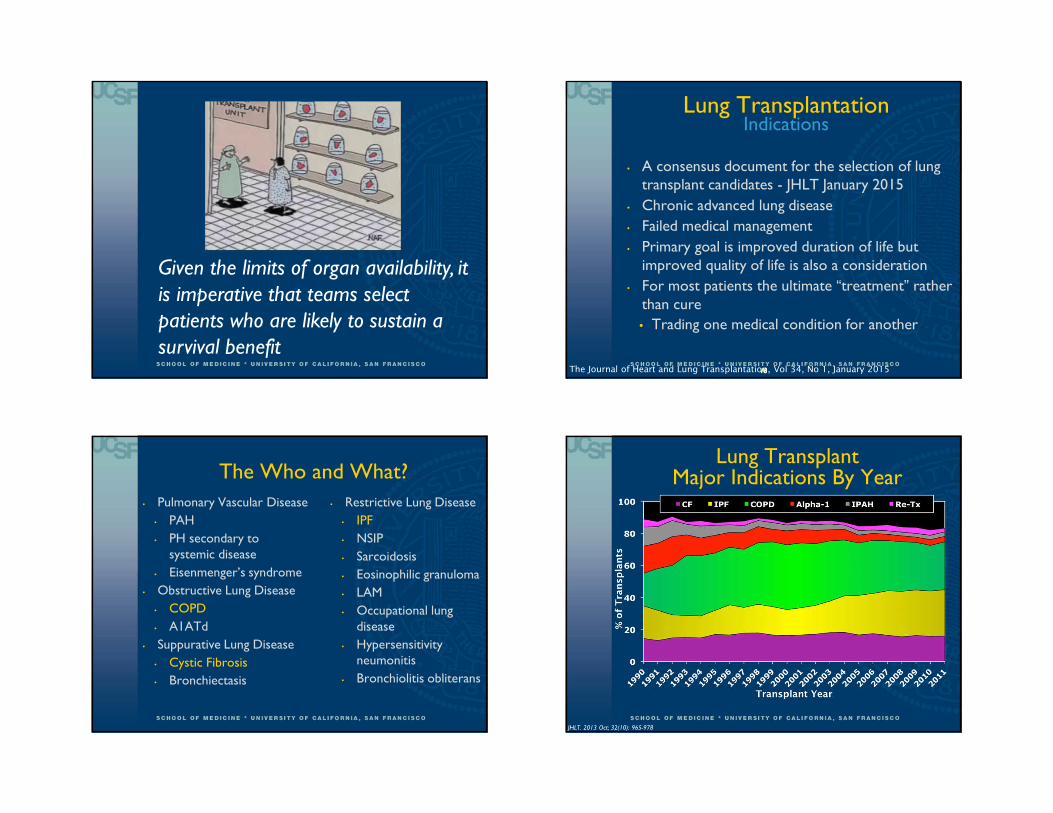
Recipient Age Distribution by Era
0000
5555
10101010
15151515
20202020
25252525
18-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-65 >65
% o
f Tra
nspl
ants
Recipient Age
1985-1994 (N=4,740)
1995-2004 (N=16,277)
2005-6/2012 (N=22,406)
p < 0.0001Median age by era (years)
1985-1994 = 47
1995-2004 = 51
2005-6/2012 = 55
Adult Lung TransplantsKaplan-Meier Survival by Age Group (Transplants: January 1990 – June 2011)
All pair-wise comparisons were significant at p < 0.05 except 18-34 vs. 35-49
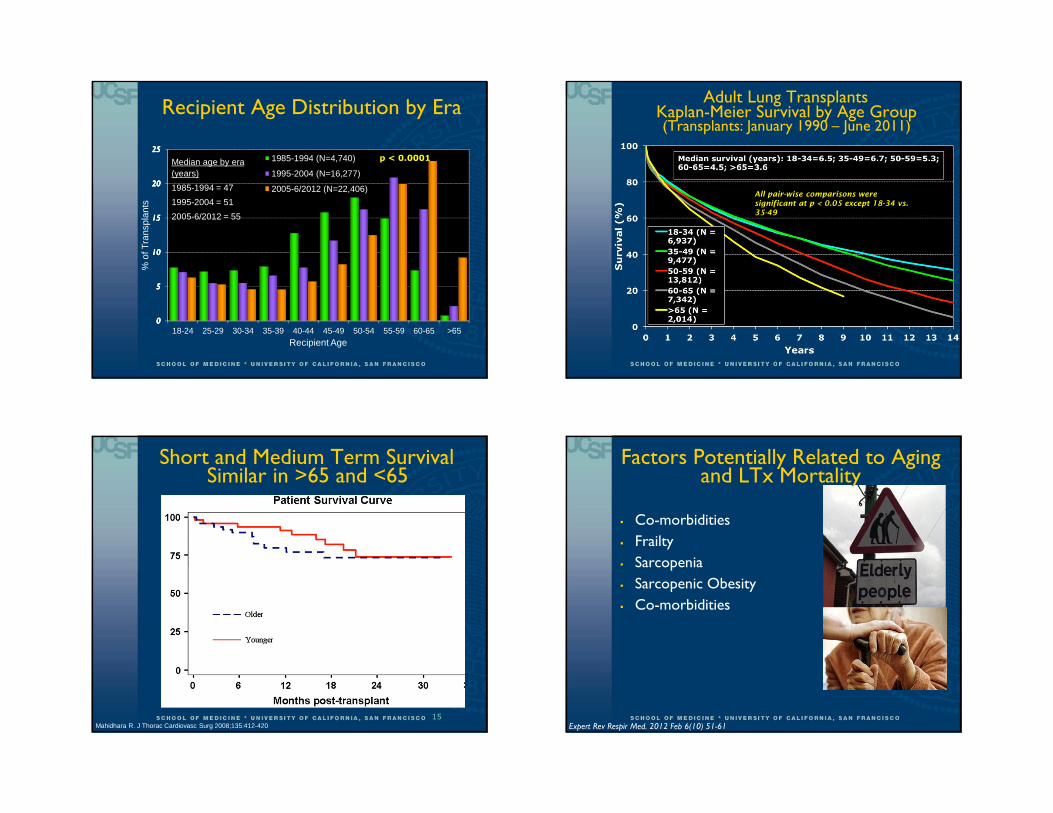
Short and Medium Term Survival Similar in >65 and <65
15Mahidhara R. J Thorac Cardiovasc Surg 2008;135:412-420 Expert Rev Respir Med. 2012 Feb 6(10) 51-61
Factors Potentially Related to Aging and LTx Mortality
� Co-morbidities
� Frailty
� Sarcopenia
� Sarcopenic Obesity
� Co-morbidities
5/9/2015
5
Body Composition and Survival
� 9073 adults who underwent transplantation in the US between 2005-2011
� Multi-variable regression adjusted models examined the associations between BMI and 1 year mortality
� Underweight (BMI < 18.5) was associated with a 35% increased rate of death
� Class II-III obesity (BMI > 35) was associated with a 2 fold increase in mortality
� Class 1 obesity (BMI 30-34.9) not associated with one year mortality
18
Body Composition and Survival
American Journal of Respiratory and Critical Care Medicine 190:9, 971-973
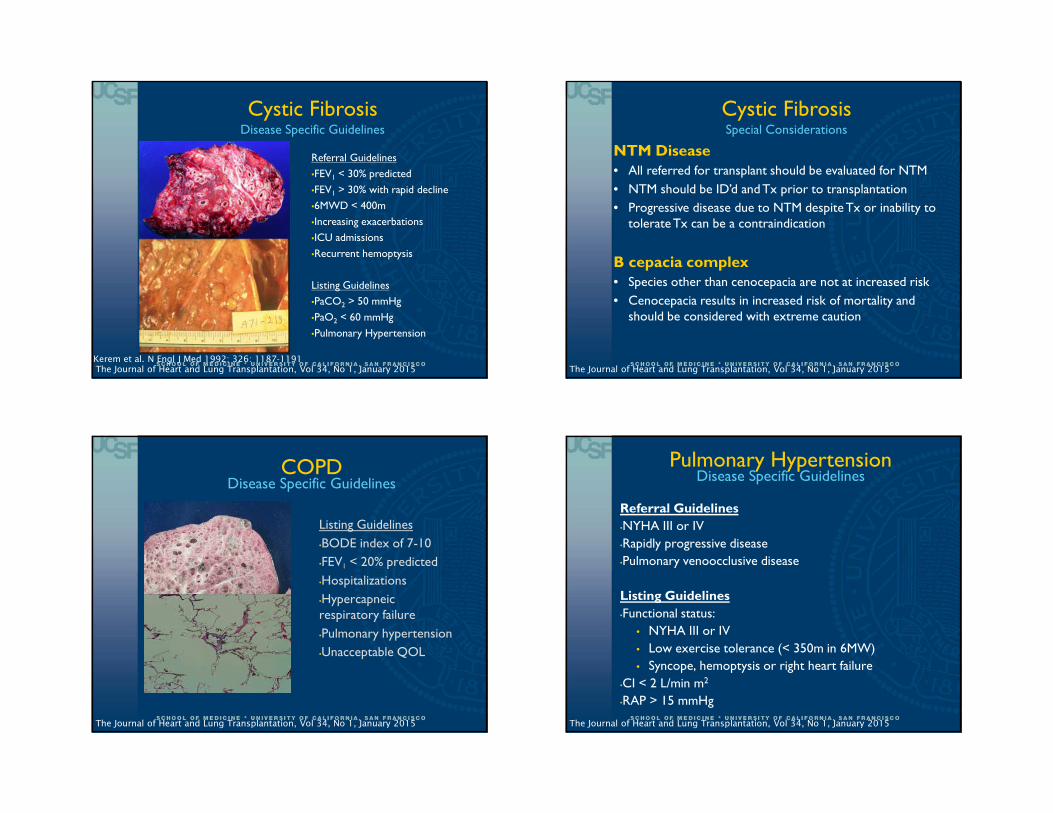
Thabut. J Thorac Cardiovasc Surg 2003;126:469
Pulmonary FibrosisPre-LAS
J Heart Lung Transplant 2006; 25: 745-55
Pulmonary FibrosisDisease Specific Guidelines
If IPF
REFER EARLY

5/9/2015
6
Referral Guidelines
•UIP
•Fibrotic NSIP
•Oxygen requirement
•FVC < 80% or DLCO < 40%
Listing Guidelines
•10% drop in FVC over 6 months
•15% drop in DLCO over 6 months
•Desaturation with 6MWT or drop in 6MWT distance
•Pulmonary hypertension or hospitalization
Pulmonary FibrosisDisease Specific Guidelines
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
• Rare, progressive ILD triggered by inhaled antigens
• Primary treatment is removal of antigen from environment
• Offending agent only ID’d in 40% of cases
• A subset of patients develop progressive fibrosis
• Can Lung Transplantation help this group?
• What is the outcome including survival?
• Does it recur?
Hypersensitivity Pneumonitis
• Retrospective cohort study of 31 patients transplanted for HP between 2001-2013
• 12 of 31 had known inciting exposure (39%)
• 5 of the 31 had diagnosis of IPF prior to transplant
Hypersensitivity Pneumonitis
Lung Transplantation for Hypersensitivity Pneumonitis. Chest. 2014
• 2 of the 31 patients developed recurrent HP
• Both cases were associated with:
• Exposure to presumed antigen
• Granulomas on biopsy
• Drop in lung function
• No infectious cause
• Improvement/stabilization with treatment with steroids
Hypersensitivity Pneumonitis
Lung Transplantation for Hypersensitivity Pneumonitis. Chest. 2014

5/9/2015
7
Hypersensitivity Pneumonitis
Lung Transplantation for Hypersensitivity Pneumonitis. Chest. 2014
Hypersensitivity Pneumonitis
Lung Transplantation for Hypersensitivity Pneumonitis. Chest. 2014
Connective Tissue Disease-Related ILD
Adult Lung Transplantation: Indications (1/1995-6/2010)
DIAGNOSIS SLT (N = 12,339) BLT (N = 18,334) TOTAL (N = 30,673)
COPD/Emphysema 5,769 ( 46.8% ) 4,839 ( 26.4% ) 10,608 ( 34.6% )
Idiopathic Pulmonary Fibrosis 3,995 ( 32.4% ) 2,938 ( 16.0% ) 6,933 ( 22.6% )
Cystic Fibrosis 214 ( 1.7% ) 4,941 ( 26.9% ) 5,155 ( 16.8% )
Alpha-1 728 ( 5.9% ) 1,225 ( 6.7% ) 1,953 ( 6.4% )
Idiopathic Pulmonary Arterial Hypertension
78 ( 0.6% ) 894 ( 4.9% ) 972 ( 3.2% )
Pulmonary Fibrosis, Other 424 ( 3.4% ) 537 ( 2.9% ) 961 ( 3.1% )
Bronchiectasis 50 ( 0.4% ) 815 ( 4.4% ) 865 ( 2.8% )
Sarcoidosis 236 ( 1.9% ) 547 ( 3.0% ) 783 ( 2.6% )
Re-Transplant: Obliterative Bronchiolitis 253 ( 2.1% ) 219 ( 1.2% ) 472 ( 1.5% )
Connective Tissue Disease 127 ( 1.0% ) 232 ( 1.3% ) 359 ( 1.2% )
Obliterative Bronchiolitis (Not Re-Transplant)
80 ( 0.6% ) 237 ( 1.3% ) 317 ( 1.0% )
LAM 101 ( 0.8% ) 207 ( 1.1% ) 308 ( 1.0% )
Re-Transplant: Not Obliterative Bronchiolitis
127 ( 1.0% ) 162 ( 0.9% ) 289 ( 0.9% )
Congenital Heart Disease 43 ( 0.3% ) 224 ( 1.2% ) 267 ( 0.9% )
Cancer 6 ( 0.0% ) 26 ( 0.1% ) 32 ( 0.1% )
Other 108 ( 0.9% ) 291 ( 1.6% ) 399 ( 1.3% )
J Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

5/9/2015
8
Lung transplantation in scleroderma compared with IPF and IPAH
Arthritis & Rheumatism 2006. pages 3954-3961
Freedom from BOSScleroderma vs. IPF
Transplantation. 2013 Apr 15;95(7):975-80.
Lung Transplant SurvivalScleroderma vs IPF
Transplantation. 2013 Apr 15;95(7):975-80.
Scleroderma and Aspiration Risk

5/9/2015
9
Scleroderma and Aspiration Risk
34343434
• Severe pulmonary fibrosis (FVC and DLCO <40%), unresponsive to medical treatment
• Creatinine clearance above 60 mL/min
• Absence of severe skin involvement (severe cutaneous thickening)
• Absence of severe esophageal dysmotility and aspiration
• Absence of significant conduction abnormalities
• Absence of severe small intestine, gastroparesis, colorectal and rectum involvement such as pseudo-obstruction, diverticulitis, and perforation
Scleroderma Evaluation
• Retrospective case series of 14 lung transplant recipients with telomerase complex mutations
• All had fibrotic lung disease but only 43% had UIP pattern on CT imaging
• High incidence of cytopenias, particularly leukopenia, post transplantation (83%)
• Of these, 5 could not tolerate anti-proliferative agents – but not associated with acute rejection or CLAD
• CLAD occurred in 33% of recipients at median 3.1 years
Outcomes of Lung Transplantation in Patients with Telomerase Mutations
Outcomes of Lung Transplantation in Patients with Telomerase Mutations
J Heart LungTransplant in press

5/9/2015
10
IPF Exacerbation
• Acute Deterioration due to right heart strain
• Intubation can make worse
• Traditionally lung transplantation has not been on option for those with respiratory failure
• Reluctance because of concern for dismal outcome
• Allocation of lungs (based on time on wait list)
• Experience with ECLS and MV as well as change in LAS have shifted this paradigm
Nathan SD, Noble PW, and Tuder RM AJRCCM Vol 175. pp. 875-880, (2007)
ECMO as a Bridge to Lung Transplant
UCSF ExperienceECMO Bridge to Transplant
• 31 patients bridged to transplant using ECMO
• 93% survival at 1 year
• 80% survival at 3 years
• 66% survival at 5 years
J Thorac Cardiovasc Surg. 2013 Mar;145(3):862-7
ConsensusECMO Bridge to Transplant
• Recommended
• Young age
• Absence of multiple organ dysfunction
• Good potential for rehabilitation
• Not Recommended
• Septic shock
• Multi-organ dysfunction
• Severe arterial occlusive disease
• HIT
• Prior prolonged mechanical ventilation
• Advanced age and Obesity
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
5/9/2015
11
Referral Guidelines
•FEV1 < 30% predicted
•FEV1 > 30% with rapid decline
•6MWD < 400m
•Increasing exacerbations
•ICU admissions
•Recurrent hemoptysis
Listing Guidelines
•PaCO2 > 50 mmHg
•PaO2 < 60 mmHg
•Pulmonary Hypertension
Cystic FibrosisDisease Specific Guidelines
Kerem et al. N Engl J Med 1992; 326: 1187-1191The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
NTM Disease
• All referred for transplant should be evaluated for NTM
• NTM should be ID’d and Tx prior to transplantation
• Progressive disease due to NTM despite Tx or inability to tolerate Tx can be a contraindication
B cepacia complex
• Species other than cenocepacia are not at increased risk
• Cenocepacia results in increased risk of mortality and should be considered with extreme caution
Cystic FibrosisSpecial Considerations
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
COPDDisease Specific Guidelines
Listing Guidelines
•BODE index of 7-10
•FEV1 < 20% predicted
•Hospitalizations
•Hypercapneicrespiratory failure
•Pulmonary hypertension
•Unacceptable QOL
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015
Pulmonary HypertensionDisease Specific Guidelines
Referral Guidelines
•NYHA III or IV
•Rapidly progressive disease
•Pulmonary venoocclusive disease
Listing Guidelines
•Functional status:
• NYHA III or IV
• Low exercise tolerance (< 350m in 6MW)
• Syncope, hemoptysis or right heart failure
•CI < 2 L/min m2
•RAP > 15 mmHg
The Journal of Heart and Lung Transplantation, Vol 34, No 1, January 2015

5/9/2015
12
ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival by Era (Transplants: January 1988 – June 2009)
1988-1994: 1/2-life = 4.7 Years; Conditional 1/2-life = 7.9 Years
1995-1999: 1/2-life = 4.8 Years; Conditional 1/2-life = 7.5 Years
2000-6/2009: 1/2-life = 5.9 Years; Conditional 1/2-life = 8.0 Years
N at risk =552
N at risk = 702
N at risk = 841
J Heart Lung Transplant. 2011 Oct; 30 (10) 1071-1132
UCSF, National and Expected Lung Transplant SurvivalData from the Scientific Registry of Transplant Recipients
July 2014
46
*
*
Thank youQuestions?
Lung Transplant Referrals: (415) 353-4145
Recommended