The Whole Truth About IUDsNurses are perfectly positioned to offer women accurate information about an often-neglected contraceptive method.
M any women spend most of their reproductive years trying to avoid
pregnancy, and they do so for a variety of reasons. For instance, a busy young mother of two desires more children—but in the future, after life settles down a bit; a graduate student intends to marry her fiancé and start a family—but not for a few years; a highpowered career woman is pursuing her professional goals before starting a family.
Modern contraception options provide women with the opportunity to plan when they attempt to have children. Choosing a contraceptive method that’s both effective and safe is an important decision for every woman of childbearing age. There are many personal variables that a woman must consider in making her decision, but convenience and ease of use will be high on any woman’s list of priorities in picking a contraceptive method that fits her lifestyle.
Although health care providers usually suggest oral contraceptives for family planning,1 women should also be provided with information about an overlooked and misunderstood contraceptive method—the intrauterine device (IUD). It’s up to nurses to provide the public with accurate facts to facilitate educated choices.
A BLEMISHED PASTAccording to Family Planning Worldwide: 2008 Data Sheet
from the Population Reference Bureau (available at www.prb. org/pdf08/fpds08.pdf), only 2% of married American wo men use IUDs, compared with 7% in Latin America and the Car i bbean, 11% in northern Europe (use ranges widely throughout the European continent, from 0.4% in Macedonia to 6% in the United Kingdom to nearly 26% in Belarus), and 18% over all in Asia. Misinformation about IUDs appears to be one of the main reasons that it isn’t more popular. Although evidence shows that IUDs are safe and effective, old fears and miscon ceptions often steer women toward other methods. A historical view of IUDs sheds some light.
IUDs became available to U.S. women in the 1960s. Their popularity plummeted, however, in the late 1970s after adverse events involving the Dalkon Shield were reported. When the device was in place, a multifilament tail string leading from the uterus to the vagina wasn’t sealed on either end, creating an open portal for bacteria to ascend into the uterus, which put women at higher risk for serious pelvic infection. The Dalkon Shield was responsible, according to some sources, for more than “200,000 infections, miscarriages, hysterectomies, and other gynecological complications and led to an untold number of birth defects,” as well as 18 deaths.2 Media coverage exposed the adverse events, as well
as shoddy premarketing research in the case of the Dalkon Shield, and contributed to the end of the manufacturing of almost all the IUDs in the United States by the 1980s.
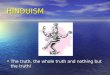
In spite of this, a few U.S. companies continued to develop and improve IUDs. The copper T 380A (ParaGard) was introduced in the United States in 1988 (Figure 1). The levonorgestrelreleasing
By Ruth Monchek, MSN, CNM
[email protected] AJN t June 2010 t Vol. 110, No. 6 53
Copper wire Copper band
Monofilament threads
Figure 1. The Copper T 380A (ParaGard) Intrauterine Device. LifeART image. © 2008 Lippincott Williams and Wilkins. All rights reserved.

and the potential risks of pelvic infection, infertility, and ectopic pregnancy.
An IUD is a small plastic or plasticandmetal object that’s inserted into the uterus using a sterile technique during a pelvic examination. It has a tail string that hangs down into the upper part of the vagina to facilitate removal. Once in place, the IUD provides immediate contraceptive protection and is 99% effective against preventing pregnancy, ac cording to the Centers for Dis ease Control and Prevention (http://bit.ly/9SoVtj). The copperreleasing T 380A IUD and the LNGIUS are the only two IUDs available in the United States. Each is a Tshaped device that has a unique composition and a different means of providing contraceptive protection. Both offer the user safe, longlasting family planning benefits.3 In addition, a 2008 metaanalysis of 10 studies shows that all IUDs have a protective effect against endometrial cancer.4
The T 380A. The polyethylene T 380A has copper bands on both arms and copper wire wrapped around its vertical stem with a string attached to its base (see Figure 1). The device is thought to act by releasing copper ions into uterine and tubal fluids and impairing sperm motility so fertilization doesn’t occur. It can be used effectively for up to 10 years, possibly as long as 12 years as a 1991 study showed.5
The copper IUD can also be used for emergency contraception. When inserted within five days of unprotected intercourse, it is 99% effective in protecting against pregnancy.6 The exact mechanism of action of this IUD as an emergency contraceptive hasn’t been clearly identified. It’s possible that when used in this capacity, copper IUDs may work
by disrupting a pregnancy after fertilization has occurred.7
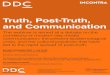
The LNG-IUS. The LNGIUS contains a reservoir core that over time releases a therapeutic level of the hormone levonorgestrel, which thickens cervical mucus, inhibiting sperm from entering the uterine cavity (see Figure 2). It also impairs sperm function, suppresses endometrial growth, and may even inhibit ovulation in some women. The approved duration of use is five years.
Because of its hormonal features, the LNGIUS may be the treatment of choice for select gynecologic problems. For example, women with heavy menses or dysmenorrhea find relief after the first few months after insertion, when the IUD suppresses the monthly growth of endometrial tissue and reduces menstrual flow some 70% to 90%.8 Some women—as many as 23.9%, according to the device’s prescribing information—will experience amenorrhea within one year of use.9 Both perimenopausal and postmenopausal women have also found symptom relief when this IUD is used as part of hormone replacement therapy.10 Although more research is needed, current studies show promising results for the treatment of endometriosis, adenomyosis, and chronic pelvic pain with use of the LNGIUS.11
Mechanism of action. Women considering an IUD need an accurate explanation of how the IUD prevents fertilization rather than disrupts an established pregnancy. It was originally thought that an IUD acted as a foreign body, causing an inflammatory response in the lining of the uterus that made the implantation of a fertilized ovum impossible. According to the prescribing information for the T 380A, that’s
intrauterine system, or LNGIUS (Mirena), was made available for use in the United States in 2001 (Figure 2).
Because of the Dalkon Shield events, many women have been afraid to use IUDs, and health care providers have hesitated to insert them for fear of litigation, a fear that persists. It’s time for health professionals to sort through the fallacies and examine the facts about the IUDs available today.
IUD BASICS FOR NURSESTo provide accurate information to patients, nurses need to know the facts about the modern IUD—how it works and the kinds that are available. Clarifying the misinformation that surrounds IUDs can enable nurses to help women to make informed decisions about using this contraceptive method. Some of the most troublesome concerns for women are how the IUD works
54 AJN t June 2010 t Vol. 110, No. 6 ajnonline.com
Figure 2. The Levonorgestrel-Releasing Intrauterine System, or LNG-IUS (Mirena). LifeART image. © 2009 Lippincott Williams and Wilkins. All rights reserved.
Monofilamentthreads
HormonecylinderHormone cylinder
Monofilament threads

After an IUD is removed, the risk of ectopic implantation in future pregnancies remains low.23
PATIENT EDUCATIONNurses are often a patient’s first and best source of current evidencebased information on health care issues. Women are constantly bombarded with popular media reports and advertising about contraception. With knowledge of the IUDs available today, a nurse can educate women who are considering their family planning options. A discussion of the different types of IUDs, how they work, and the risks and benefits associated with their use can be very useful to women who are trying to determine whether the method would be right for them. Nurses come into contact with women of reproductive age in
many different clinical settings and can empower them to make educated decisions about their birth control method.
Nurses can point out to patients that the modern IUD has a number of benefits as an effective method of contraception. It’s easy to use and maintain; a woman just has to perform a monthly check to ensure that the string is still in place. The IUD provides reversible contraception with no systemic adverse effects.
In the public sector, the cost for the T 380A is about $225 plus the insertion fee; the cost for the LNGIUS is about $450 plus the insertion fee.8 In the private sectors, costs for the T 380A and the LNGIUS are approximately $494 and $585, respectively,
associated with IUD use and prove that both types of IUD can be safely used by nulliparous women.17, 18 Research has demonstrated that there’s no causal relationship between infertility and the past use of a coppercontaining IUD.19 Although the same is thought to be true for the LNGIUS, there hasn’t yet been enough research. For most women, there is a rapid return to fertility after they discontinue the use of the IUD.20 The IUD is being touted as an efficacious alternative to permanent sterilization because both are comparably effective in preventing pregnancy.21 And because the sterilization caused by the device is reversible, the IUD may be a pleasing option for women who are not 100% certain that they want to end their reproductive capability.
Ectopic pregnancy. Because of the confusion surrounding the IUD’s mechanism of action, it was believed that it could increase the risk of ectopic pregnancy caused by interference with the movement of a fertilized ovum through the fallopian tubes. A recent study demonstrates that women using IUDs have a lower incidence of ectopic pregnancy than women who use no contraception at all.22 The IUD doesn’t protect against ectopic pregnancy as effectively as it prevents an intrauterine pregnancy; if a woman with an IUD conceives, it’s possible that it could be an ectopic pregnancy. However, because the IUD failure rate is less than 1%, its use reduces the absolute incidence of ectopic pregnancies.22
still considered a possible mechanism of action.12 Current data consistently demonstrate that both the T 380A and the LNGIUS promote changes in the reproductive tract that are lethal to both sperm and ova and prevent the formation of embryos.13 The notion that an IUD might cause the abortion of a developing pregnancy may make this an unacceptable method of birth control for many women. Women need reassurance that the IUD averts pregnancy by inhibiting fertilization.
Risk of pelvic infection. One of the misconceptions most commonly held by both patients and some providers is that IUDs cause pelvic inflammatory disease (PID), a serious infection that spreads up into the uterus and fallopian tubes. Damage to these reproductive organs can often result in infertility. However, the risk of pelvic infection among IUD users appears to be low.14 Clinical studies show that there is an increased risk of infection during the first 20 days after insertion, which is most likely caused by uterine contamination from vaginal bacteria at the time of insertion.15 According to one 2007 review, after this initial period the incidence of PID appears to be low among IUD users and is likely similar to that of women in the general population.16 PID is caused primarily by sexually transmitted disease, most notably gonorrhea and Chlamydia. Women who are sexually active and not using safer sex practices are at risk for PID regardless of the type of contraception they use.
Infertility. In the past, most women who had not yet had children were advised that IUD use could result in infertility because of the risk of pelvic infection. Many studies have disputed the increased incidence of PID
[email protected] AJN t June 2010 t Vol. 110, No. 6 55
The risk of pelvic infection among IUD users
appears to be low.

11. Bahamondes L, et al. Use of the levonorgestrelreleasing intrauterine system in women with endometriosis, chronic pelvic pain and dysmenorrhea. Contraception 2007;75(6 Suppl): S134S139.
12. FEI Women’s Health LLC. ParaGard T 380A intrauterine copper contraceptive [Prescrib ing information]. 2005. http://www.accessdata.fda. gov/drugsatfda_docs/label/2005/ 018680s060lbl.pdf.
13. Ortiz ME, Croxatto HB. CopperT intrauterine device and levonorgestrel intrauterine system: biological bases of their mechanism of action. Contraception 2007;75(6 Suppl):S16S30.
14. Mohllajee AP, et al. Does insertion and use of an intrauterine device increase the risk of pelvic inflammatory disease among women with sexually transmitted infection? A systematic review. Contraception 2006;73(2):14553.
15. Cheng D. The intrauterine device: still misunderstood after all these years. South Med J 2000;93(9):85964.
16. Meirik O. Intrauterine devices—upper and lower genital tract infections. Contraception 2007;75(6 Suppl):S41S47.
17. Prager S, Darney PD. The levonorgestrel intrauterine system in nulliparous women. Contraception 2007; 75(6 Suppl):S12S15.
18. Hubacher D. Copper intrauterine device use by nulliparous women: review of side effects. Contraception 2007;75(6 Suppl):S8S11.
19. Hubacher D, et al. Use of copper intrauterine devices and the risk of tubal infertility among nulligravid women. N Engl J Med 2001;345(8):5617.
20. Hov GG, et al. Use of IUD and subsequent fertility—followup after participation in a randomized clinical trial. Contraception 2007;75(2):8892.
21. Grimes DA, Mishell DR, Jr. Intrauterine contraception as an alternative to interval tubal sterilization. Contraception 2008;77(1):69.
22. Sivin I, et al. Prolonged intrauterine contraception: a sevenyear randomized study of the levonorgestrel 20 mcg/day (LNg 20) and the Copper T380 Ag IUDS. Contraception 1991;44(5):47380.
23. Skjeldestad FE. The impact of intrauterine devices on subsequent fertility. Curr Opin Obstet Gynecol 2008;20(3):27580.
24. Trussell J, et al. Cost effectiveness of contraceptives in the United States. Contraception 2009;79(1):514.
25. American College of Obstetricians and Gynecologists. ACOG practice bulletin. Clinical management guidelines for obstetriciangynecologists. Number 59, January 2005. Intrauterine device. Obstet Gynecol 2005;105(1): 22332.
26. Nelson AL. Contraindications to IUD and IUS use. Contraception 2007;75 (6 Suppl):S76S81.
use is a high risk of contracting sexually transmitted infections.
Erroneous beliefs and fears— on the part of patients and providers—based on outdated information create barriers that prevent women from considering the IUD as a possible contraceptive option. Working as patient advocates and educators, nurses can convey the facts about intrauterine contraception and help women, such as those mentioned at the beginning of the article, to determine whether this method fits their lifestyle and meets their birth control needs. t
Ruth Monchek is a certified nurse midwife and an associate professor at the University of Medicine and Dentistry of New Jersey School of Nursing, Newark. Contact author: [email protected].
REFERENCES 1. Mosher WD, et al. Use of contracep
tion and use of family planning services in the United States: 19822002. Adv Data 2004(350):136.
2. Tone A. Devices and desires: a history of contraceptives in America. 1st ed. New York: Hill and Wang; 2001.
3. Hubacher D, Cheng D. Intrauterine devices and reproductive health: American women in feast and famine. Contraception 2004;69(6):43746.
4. Beining RM, et al. Metaanalysis of intrauterine device use and risk of endometrial cancer. Ann Epidemiol 2008;18(6):4929.
5. World Health Organization, Department of Reproductive Health and Research. Medical eligibility criteria for contraceptive use: a WHO family planning cornerstone. Geneva, Switzerland; 2009. 4th edition. http://whqlibdoc.who.int/publications/2009/ 9789241563888_eng.pdf.
6. Trussell J, Ellertson C. Efficacy of emergency contraception. Fertility control reviews 1995;4(2):811.
7. Zhou L, Xiao B. Emergency contraception with Multiload Cu375 SL IUD: a multicenter clinical trial. Contraception 2001;64(2):10712.
8. Morgan KW. The intrauterine device: rethinking old paradigms. J Midwifery Womens Health 2006;51(6):46470.
9. Casey PM, Pruthi S. The latest contraceptive options: what you must know. J Fam Pract 2008;57(12):797805.
10. SitrukWare R. The levonorgestrel intrauterine system for use in peri and postmenopausal women. Contraception 2007;75(6 Suppl):S155S160.
not including the insertion fee.24 Although the initial cost of an IUD may seem relatively high, because it lasts so long it’s very costeffective and, in the long run, is one of the least expensive contraceptives available.
Nurses must also inform their patients of the disadvantages of IUDs. IUD insertion must be performed by a health care provider and an office visit is required. Men strual disturbances are possible: users of the T 380A may experience heavy menstrual bleeding; users of the LNGIUS may have irregular bleeding initially, and overall they may have a reduced menstrual flow. Cramping and pain are possible at the time of insertion, and T 380A users may have increased menstrual pain. Finally, nurses must remind patients that the IUD offers no protection against sexually transmitted infections.
INTO THE FUTUREThe IUD can provide longterm, highly effective contraception to most women of reproductive age. Medical groups such as the World Health Organization (WHO) and the American Congress of Obstetricians and Gynecologists propose that eligibility for use of the IUD includes all healthy women of any age re gardless of whether or not they have had children.5, 25 According to the WHO’s analysis of the available research, “There are conflicting data regarding whether IUD use is associated with infertility among nulliparous women, although wellconducted studies suggest no increased risk.”5 Although there are some medical conditions that preclude its use, among the most common being uterine abnormalities, uterine or cervical neoplasia, unexplained genital bleeding, and hypersensitivity to components of the IUD,26 the main contraindication to IUD
56 AJN t June 2010 t Vol. 110, No. 6 ajnonline.com
Recommended