Tobacco101PartTwo,LessonFour
2016
ASELF-GUIDEDE-BOOKINTWOPARTS

©2016EmoryCentersforTrainingandTechnicalAssistance2
IntroductiontoTobacco101WelcometoTTAC’sTobacco101!Tobacco101isaself-guidedtutorialthatprovidestheinformationandresourcesnecessarytounderstandwhytobaccouseisconsideredthe#1preventablecauseofdeathintheUS,aswellastheevidence-basedandpromisingstrategiesthatcanreducetobacco’stoll.Youcanbenefitfromthiscoursewhetheryouarenewtotobaccocontrolandneedanintroductiontokeytopics,orareanexperiencedprofessionallookingtorefreshandupdateyourknowledge.
Tobacco101wasrevisedinthespringof2013tocontainthelatestinformation,resources,andtoolsavailable.Theuser-friendlyself-guidedformatallowsyoutocompletethetutorialatyourownpaceandexplorethevariousexternalresourcesandtoolsasneeded.Tobacco101isorganizedintotwopartscomprisedoffourlessonseach.Optionalreviewquestionsareofferedattheendofeachlessontoallowyoutocheckyourunderstandingofthecontent,trysomeoftheresources,andreflectonhowtheinformationappliestoyourroleintobaccocontrol.
Youcanstartatthebeginningandreadthroughthecoursefrombeginningtoendorsimplyselectthosesectionsthatareofgreatestinterest.
Part1:IntroductiontoPreventionandControlofTobaccoUse• Lesson1:TheEvolutionofTobaccoControl• Lesson2:TobaccoUseintheUnitedStates• Lesson3:ImpactofTobaccoUse• Lesson4:FactorsthatDetermineTobaccoUse
Part2:ReducingtheProblemofTobaccoUse• Lesson1:CredibleTobaccoControlResourcesandKeyPartners• Lesson2:TobaccoControlModels• Lesson3:EffectiveTobaccoControlPolicies• Lesson4:StrategiesforSuccess
TTACalsoprovidestailored,on-siteTobacco101trainingsfororganizationswhowanttoincludeitinconferencesandworkshops.Tolearnmore,visitourwebsitewww.tacenters.emory.eduorcontactusattacenters@emory.edu.
©2016EmoryCentersforTrainingandTechnicalAssistance3
TableofContentsPART2: REDUCINGTHEPROBLEMOFTOBACCOUSELESSON4
StrategiesforSuccess Page4
CheckforUnderstanding Page33
Sources Page36
©2016EmoryCentersforTrainingandTechnicalAssistance4
Tobacco101PartTwo,LessonFour
StrategiesforSuccess
Inpreviouslessons,wetalkedaboutthepoliciesthatareeffectiveatreducingtobaccouse,butwehavenotdiscussedthestrategiesthatmakethesepoliciesandprogramssuccessful.Thatwillbeourfocusforthisnextlesson.Wewilldiscussthehowofplanning,implementing,evaluating,andsustainingeffectiveprogramstoachievethefourgoalsdescribedinBestPractices.Attheendofthislessonyouwillbeableto:
1. Identifythefivestepsthatgointoimplementingatobaccocontrolprograminyourstateandcommunity.Therearefivemajorstepstogetaprogramupandrunningandtomakesureitissustainedlongterm.
2. Describewaystosustainadequatefundingfortobaccocontrolprograms.Tobaccocontrol
programsmustlastlong-terminordertohaveasignificantimpact,soplanninghowtosustainaprogramshouldoccurthroughoutthelifeoftheprogram.
3. DescribeeffectivestrategiestoachieveNationalTobaccoControlProgramgoals.Wewilllookat
eachofthefourgoalsoutlinedinBestPracticesandtalkaboutstrategiesthatworkinbothstatesandcommunities.
©2016EmoryCentersforTrainingandTechnicalAssistance5
ImplementingPrograms
Implementingtobaccocontrolprogramsisaprocessthatrequirespatienceandperseverance.Muchtimeandeffortisputforthbyprogramstaffandcommittedcommunityorganizationstoplanfor,carryout,andevaluatetobaccopreventionandcontrolprograms.Thesearethefivemajorstepstogettingaprogramupandrunningandtomakingsureitcanbesustainedlongterm:
1. Engagestakeholders2. Developastrategicplan3. Implementtheprogram4. Evaluatetheprogram5. Sustaintheprogram
We’lltalkabouteachstepinturn.
©2016EmoryCentersforTrainingandTechnicalAssistance6
Step1:EngageStakeholdersThefirststepintheprocessoftobaccocontrolprogramimplementationisfindingstakeholderstoworkwithyou.Stakeholdersarepeopleinthecommunitywhoareinterestedinorareaffectedbytobaccouse.Engagingstakeholdersandpartnersforyourprogramisoftenthehardestpartofgettingaprogramupandrunning.Thekeytoyoursuccessinacquiringpartnersliesin:
• Knowingwheretolookforthem• Buildingrelationshipsandnetworking• Providingthemwithinformationabouttobaccouse,suchasratesofuseandtheassociatedhealth
andeconomiceffects• Helpingcommunitygroupsunderstandhowtobaccouseaffectsthemandtheirobjectives• Communicatingthevalueatobaccocontrolprogramhastothem• Determiningtheroletheywouldplayinsupportingtobaccocontrolpolicies
Eachcommunitygrouphasitsuniquestakeinreducingtobaccouseandthereforerequiresadifferentwayofpersuadingdecisionmakerstochangepolicies,topromotetobaccocontrolprograms,andultimatelytoreducetobaccouse.Engagingstakeholderswillhelptomobilizethecommunityintowantingtochangeandthenworkingtowardschange.Awell-informed,diverse,andbroad-basedcommunitycollaborationisnecessarytochangepoliciesandsocialnorms.

©2016EmoryCentersforTrainingandTechnicalAssistance7
Step1:EngageStakeholders–WhotoIncludeAssemblinginfluentialkeystakeholdersisessentialforasuccessfulprogram.Sometimestalkingtotherightpeoplehasadominoeffect-oneinterestedpartywillintroduceyoutoanother.Whoyouwantaspartnersvariesdependingonwhetheryouareestablishingagovernment(state,county,orcity)programoranongovernmentprogram.Belowisjustapartiallistofsomeofthetobaccocontrolstakeholderswhocanhelpadvocateandsupportpolicies:
− ConcernedCitizens − Medicalproviderassociations− CommunityLeaders − BusinessCommunity− YouthGroups − TribalCouncils− LocalBoardsofHealth − Faith-BasedOrganizations− HealthCareProviders − NeighborhoodAssociations− Voluntaryhealthorganizations − ParentOrganizations− DepartmentsofHealthandChronicDisease
Programs− TeachersandOtherEducation
Professionals

©2016EmoryCentersforTrainingandTechnicalAssistance8
Step1:EngageStakeholders–CommunityCollaborationTobuildadvocacysupportforpolicyinterventions,youmustworkcollaborativelywithothersinyourcommunity.Givingeverystakeholderandpartneravoiceandanopportunitytoparticipatemeaningfullyinyourprogramandpolicychangeeffortswillleadtothegreatestopportunitiesforsuccess.Theskillfulpartofthisprocessisrecognizingwhichgroupswouldbegoodpartners,howtopersuadethemtopartnerwiththeprogram,andhowtousetheirvoicestobestadvantage.
Thiscollaborationcantypicallybeachievedthroughcoalitions.Acoalitionbringstogetherindividualsandorganizationswithdiverseskillsandexpertisetoaddressaspecificissue.Coalitionsenhancestateandlocaltobaccocontroleffortsbymobilizingcommunities,advocatingforpolicies,andchangingsocialnorms.Tobaccocontrolcoalitionsformtoreducetheburdenoftobaccouseandshapetobacco-freenormssothattobaccobecomeslessdesirable,acceptable,andaccessible.Coalitionshavealsobeenproventobeeffectivecommunityinterventions,astheireffortsworktochangesocialnormsthroughpolicychangeandleadtodecreasedmorbidityandmortality.Becauseofthis,coalitionsareahighpriorityinvestmentfortobaccocontrol.
Formoreinformation…abouttobaccocontrolcoalitions:
DownloadtheBestPracticesUserGuide:CoalitionsfromtheCDC:http://www.cdc.gov/tobacco/stateandcommunity/bp_user_guide/pdfs/user_guide.pdf
©2016EmoryCentersforTrainingandTechnicalAssistance9
Step2:DevelopaStrategicPlanThenextsteptogettingaprogramupandrunningisdevelopingastrategicplan.Strategicplansareessentialtothesuccessofatobaccocontrolprogram.Astrategicplanislikeamap,definingthedirectioninwhichtoheadandgivinginstructionsonhowtoreachyourdestination.Astrategicplanforatobaccocontrolprogramisaframeworkthatshows:
• Goals• Objectives• Plannedinterventionsandrelatedactivities• Methodsofevaluation
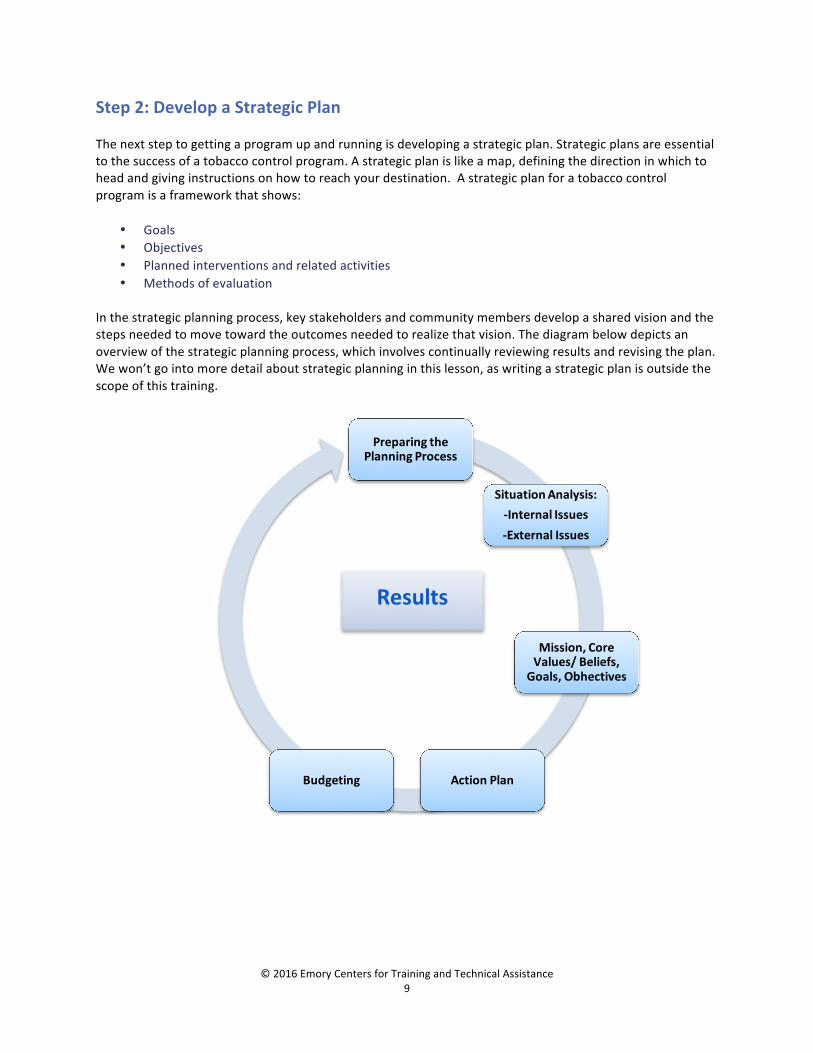
Inthestrategicplanningprocess,keystakeholdersandcommunitymembersdevelopasharedvisionandthestepsneededtomovetowardtheoutcomesneededtorealizethatvision.Thediagrambelowdepictsanoverviewofthestrategicplanningprocess,whichinvolvescontinuallyreviewingresultsandrevisingtheplan.Wewon’tgointomoredetailaboutstrategicplanninginthislesson,aswritingastrategicplanisoutsidethescopeofthistraining.
Results
PreparingthePlanningProcess
SituationAnalysis:-InternalIssues-ExternalIssues
Mission,CoreValues/Beliefs,Goals,Obhectives
ActionPlanBudgeting

©2016EmoryCentersforTrainingandTechnicalAssistance10
Step3:ImplementtheProgramOnceyouhaveyourstrategicplan,itistimetobeginachievingobjectivesoutlinedinyourplanthroughplannedactivities.TheseactivitiesshouldreflecttheessentialelementsofacomprehensiveprogramdescribedbyBestPracticesandutilizeinterventionsproventobeeffective,suchasthosedescribedinTheCommunityGuide.WewilldiscussimplementationofstrategiesandactivitiesfurtherinthenextsectionofthisLesson.Successoftendependsonbeingabletobuildinfrastructureforyourprogramandincreaseitscapacitytotakeonprojects.Trainedstaffandadequatefundingareessentialforeffectiveprogramcapacity.Programcapacitypairedwithstableandadequatefundingarerequiredtoachievelong-termresults.

©2016EmoryCentersforTrainingandTechnicalAssistance11
Step4:EvaluatetheProgramEvaluationisanessentialstepinestablishingwhetherornotyourprogramiseffective–whichiskeytosecuringfundingandsustainingyourprogram.Severalpublicationsonevaluationareavailabletohelpyouplanandimplementprogramevaluationanddeterminetheeffectivenessofyourprograms:
• EvaluationToolkitforSmoke-freePoliciesisdesignedspecificallytohelpevaluatelocalsmoke-freelaws.
• KeyOutcomeIndicatorsforEvaluatingComprehensiveTobaccoControlProgramshasinformation
on120keyoutcomeindicatorsusedinevaluatingstatecomprehensivetobaccopreventionandcontrolprograms.
• IntroductiontoProcessEvaluationinTobaccoUsePreventionandControlhelpswithdesigningand
implementingvalidandreliableprocessevaluations.Italsoshowsthelinksbetweenprogramactivitiesandresults.
• IntroductiontoProgramEvaluationforComprehensiveTobaccoControlPrograms:isa"howto"
guideforplanningandimplementingevaluations.Ithelpsinplanning,designing,implementing,andusingtheresultsofcomprehensiveevaluationsoftobaccocontrolprograms.
©2016EmoryCentersforTrainingandTechnicalAssistance12
Step5:SustaintheProgramTohavesignificantimpact,tobaccocontrolprogramsmustlastforyears.Planninghowtosustainyourprogramshouldbeginassoonasyouhavetheideaforaprogram,continueduringstrategicplanning,andneverstopthroughoutthelifeoftheprogram.Everysuccessfulelementofacomprehensiveprogramhelpscreatethecaseforsustainingsupportfortobaccocontrol.Sustainingatobaccocontrolprogramcanbechallengingforseveralreasons:budgetcuts,lobbyingpressurebycompetingcommercialinterestgroups,otherhealthissuestakingpriority,andpoliticalconcerns.Inrecognitionofthesechallenges,theCDCequipsstateswithresearchandtoolstohelpthemsustainorbuildtheirtobaccocontrolprogramsby:
• Consultingwithstatesandterritoriesonhowtodevelopsustainabilityplanstailoredtotheirenvironmenttobuildsupportfortheirfuturetobaccocontrolendeavors.
• Researchingbestpracticesfortobaccocontrolprogramsandprovidingtheresultstostatetobaccocontrolprograms.
• Trainingstateprogramstaffinmethodsforsustainingprogramslongterm.
ForMoreinformationaboutsustainingtobaccocontrolprograms:
CheckouttheSustainingStateFundingforTobaccoControlpagefromtheCDC:http://www.cdc.gov/tobacco/tobacco_control_programs/program_development/sustainingstates/sustaining_funding/index.htm

©2016EmoryCentersforTrainingandTechnicalAssistance13
Step5:SustaintheProgramSustainingacomprehensivetobaccocontrolprogramshouldbeanon-goingactivityforyouandyourpartners.Somewaystosustainadequatefundingare:
• Createastrategicplanthatclearlycommunicatestheprogram’svision,goalsandobjectives.Sharetheplanwithpotentialfunderstoshowthemhowtheprogramwillsavelivesandreducehealthcarecosts.
• Educatefundersandpolicymakersaboutthecontinualsocietalcostoftobaccouse.Focuson
howthetobaccoindustrychangesitsproductsandmarketpracticestoattractyouth.
• FollowthemanagementandadministrationproceduresinBestPractices.Funderslookfororganizationsthatareefficient,wellorganizedandwellmanaged.
• Engagediverse,skilled,andactivestakeholderleaderstorepresentyourimpactincommunities.
Theirvoiceswillbeheardasauthenticconcernedcitizenswhoseethelong-termbenefitsofcomprehensivetobaccocontrolprograms.
• Buildrelationshipsthroughnetworking.Muchsuccessinfundingisattributedtohavinggood
personalandprofessionalrelationships.
• Evaluateyourprogramsoyouhaveevidenceofsuccess.Turndataintounderstandableinformationbyprovidingclearandconciseprogressreportsthatquantifytheprogram’sresults.
• Keeptobaccoissuesinthenewsmediawithstoriesaboutboththedangersthattobacco
presentsandtheaccomplishmentsoftheprogram.Keepingtobaccointhemediashouldbepartofthestrategicplan.Toberelevanttoseveraldifferentaudiences,thesestoriesshouldbepresentedinavarietyofmedia.
Let’stakealookathowonestateusedsomeofthesestrategiestoovercomefundingcutstoitstobaccocontrolprogram.

©2016EmoryCentersforTrainingandTechnicalAssistance14
Step5:SustaintheProgram-AStateExampleIn2003and2004,ColoradolegislatorscuttobaccocontrolfundingtolessthanonesixthoftheminimumrecommendedbyCDC.CitizensforaHealthierColoradoandtheStateTobaccoEducationandPreventionPartnershipworkedtogethertoreturnfundingtoadequatelevelsbyraisingvoterawarenessofthelegislature’scutinfundingthroughawell-fundedmediacampaign.ThecampaigneducatedvotersandlegislatorsaboutahealthcarecrisisoccurringinColoradothatcouldbeaddressedbytobaccoexcisetaxrevenues.Itfocusedonhowthefundingwouldbeprotectedtoaddressnotjusttobaccoprevention,butalsothedetectionandtreatmentofcancerandheartandlungdiseases.ItalsoexplainedhowincreasingtobaccotaxeswoulddecreaseyouthtobaccoinitiationandnotedthatColorado’scigaretteexcisetaxeswereamongthelowestinthecountryatthetime.Asaresultoftheseefforts,astatewidereferendumwaspassedthatincludeda$0.64perpackincreaseincigaretteexcisetaxesaswellasanewexcisetaxof40%ofthemanufacturer'slistpriceonnon-cigarettetobaccoproducts.Fundswereearmarkedrevenuesforhealthprogramsandatleast$25million(16%ofexpectedrevenue)wasallocatedeachyearspecificallyfortobaccopreventionandtreatment.ThisbroughtColoradototheCDC-recommendedminimumfundinglevelforitscomprehensivetobaccocontrolprogramin2005.
Formoreinformationabouthowstateshaveworkedtosustaintheirtobaccocontrolprograms:
Lookunder“StateSnapshots”ontheSustainingStateFundingforTobaccoControlpagefromtheCDC:http://www.cdc.gov/tobacco/tobacco_control_programs/program_development/sustainingstates/index.htm

©2016EmoryCentersforTrainingandTechnicalAssistance15
StrategiesforSuccess:BestPracticesNowthatwe’vediscussedthefivestepsoftobaccocontrolprogramimplementation,wewillexpandonthefourgoalsthataredescribedinCDC’sBestPractices:
1. Preventinitiationamongyouthandyoungadults.2. Promotequittingamongadultsandyouth.3. Eliminateexposuretosecondhandsmoke.4. Identifyandeliminatetobacco-relateddisparitiesamong
populations.Inthenextsectionofthislesson,wewillfocusonstateandcommunitypolicyandsystem-basedapproachesproventoreducingtobaccousethatworktowardsachievingthesegoals.TheGuidetoCommunityPreventiveServices(oftenreferredtoastheCommunityGuide)analyzesresearchfindingstolearnwhichinterventionsworktoachievethesegoals.TheCommunityGuideisanessentialresourcetohelpprogramstoselectstrategiesandinterventionsthatareevidence-basedandaddresspopulationneeds.

©2016EmoryCentersforTrainingandTechnicalAssistance16
StrategiestoPreventInitiationamongYoungSmokersThefirsttobaccocontrolgoaldescribedinCDC’sBestPracticesistopreventyoungpeoplefromstartingtousetobacco.Itiswidelybelievedthatpreventingadolescentsandyoungadultsfrombecomingsmokerswill,inthelongrun,dothemosttoreducesmokingprevalenceandtheresultingdeathanddiseasecausedbytobacco.The2012SurgeonGeneral’sReportPreventingTobaccoUseAmongYouthandYoungAdultsstatesthecasequiteclearly:
“Preventioneffortsmustfocusonbothadolescentsandyoungadultsbecauseamongadultswhobecomedailysmokers,nearlyallfirstuseofcigarettesoccursbyage18(88%),with99%offirstusebyage26.”
Sowhatworkstopreventinitiationamongyouth?1. Raisethepriceoftobacco.Aswehavestatedalready,oneofthe
mosteffectivepoliciestodiscourageyouthfromstartingistoraisethepriceoftobaccoproducts.Forevery10%increaseinthepriceofcigarettes,youngadultsmokingdropsbyabout3.5%,andyouthsmokingdropsabout6-7%.Raisingthepricecanbeaccomplishedthroughincreasingexcisetaxesontobaccoproductsatthefederal,state,andlocallevel.
2. Changehowtobaccoismarketed.The2012SurgeonGeneral’sReportfoundthatadvertisingand
promotionalactivitiesbytobaccocompaniescausetheonsetandcontinuationofsmokingamongadolescentsandyoungadults.The2009FamilySmokingPreventionActprohibitstobaccocompaniesfromtargetingyoungpeoplebyputtinginplaceseveralproductregulationsandrestrictionsthatprotectyouth.Italsoremovedafederalprohibitionforstatesandcommunitiessettingtheirownmorestrictstandardsfortobaccomarket.
TheTobaccoControlLegalConsortiuminits2012publicationCauseandEffect:TobaccoMarketingIncreasesYouthTobaccoUsepresentsseveralpolicyoptionsforstatesandlocalcommunitiesthatimpactpoint-of-saletobaccomarketingtoyouth.Theimpactandefficacyofthesepolicyoptionsarestillbeingevaluatedandsomehaveresultedinlegalchallenges.

©2016EmoryCentersforTrainingandTechnicalAssistance17
StrategiestoPreventInitiationamongYoungSmokers3. Changesocialnormssurroundingtobacco.Another
importanttacticinprotectingadolescentsandyoungadultsfromtobaccoischangingsocialnorms.Thiscanbeaccomplishedthroughpoliciesthatreducetobaccouse,suchasincreasedexcisetaxesandsmoke-freelaws.Thesepolicesmakebeingtobacco-freethe“norm,”therebyreducinginitiation.
Anotherwaytochangesocialnormsisthroughcounter-marketingthetobaccoindustry’smarketing.Counter-marketingmeansthattobaccocontrolorganizationsproduceanddisseminateadvertisementsthatrespondtotheadvertisingclaimsofthetobaccoindustry.Justasyoungpeoplearesusceptibletomessagesthatencouragethemtobegintobaccouse,theyarealsosusceptibletomessagesthatencouragethemnottostartortoquit.AnexampleofthisistheAmericanLegacyFoundation’sTruth®Campaign,thelargestyouthfocusedsmokingpreventioncampaigninthecountry.Truth’sadvocacycampaignseducateyoungpeopleabouttobaccoindustrytacticsandappealtoyoungpeople’ssenseofjustice.
4. Empoweryoungpeoplebyinvolvingtheminyourprogram.Youngpeoplearepersuasiveadvocates
withpeers,families,andpolicymakers.TheBestPracticesUsersGuideforYouthEngagementfocusesontheroleyouthplayinadvancingpolicyaspartofacomprehensivetobaccocontrolprogramandencourageslocaltobaccocontrolprogramstoenlistyoungpeopletoadvocateforyourprograminyourcommunityandtohelpwithsmoke-freepoliciesintheirschools.

©2016EmoryCentersforTrainingandTechnicalAssistance18
StrategiestoPromoteQuittingThenextgoalinCDC’sBestPracticesistoencourageadultandyoungpeoplewhousetobaccotoquit.AmongcurrentU.S.adultsmokers,about70%reportthattheywanttoquitcompletely,andmillionsofthemhaveattemptedtodoso.Itisimportanttorememberthatsuccessfulquittingisdifficult,andoftenrequiresmultipleattemptsoveraperiodofyears.Sowhichstrategiesworktohelptobaccousersquit?1. Enactsmoke-freeandtobacco-freepolicies.Smoke-freepoliciescanmotivatepeopletoquitasthese
policiesmakeitmoredifficulttofindasociallyacceptableplacetosmoke.Tobacco-freepoliciesmayalsohavethesameeffectforusersofsmokelesstobaccoproducts.
Weknowthatthenumberoftobaccousersattemptingtoquitaftersmoke-freelawspassishigherthanbeforeasmoke-freelawispassed,givingusauniqueopportunitytomaximizethepositiveeffectthatanewsmoke-freelawhasonbothexposuretosecondhandsmokeandonquitrates.
2. Increasethecostoftobaccoproducts.Lawsthatincreasethecostoftobaccoproductshavealsobeen
showntoincreasetobaccoquitratesashighcigarettepricesinducesmokerstoquit.Forexample,every10%increaseinthepriceofcigarettesreducesoverallcigaretteconsumptionbyapproximately3-5%.
©2016EmoryCentersforTrainingandTechnicalAssistance19
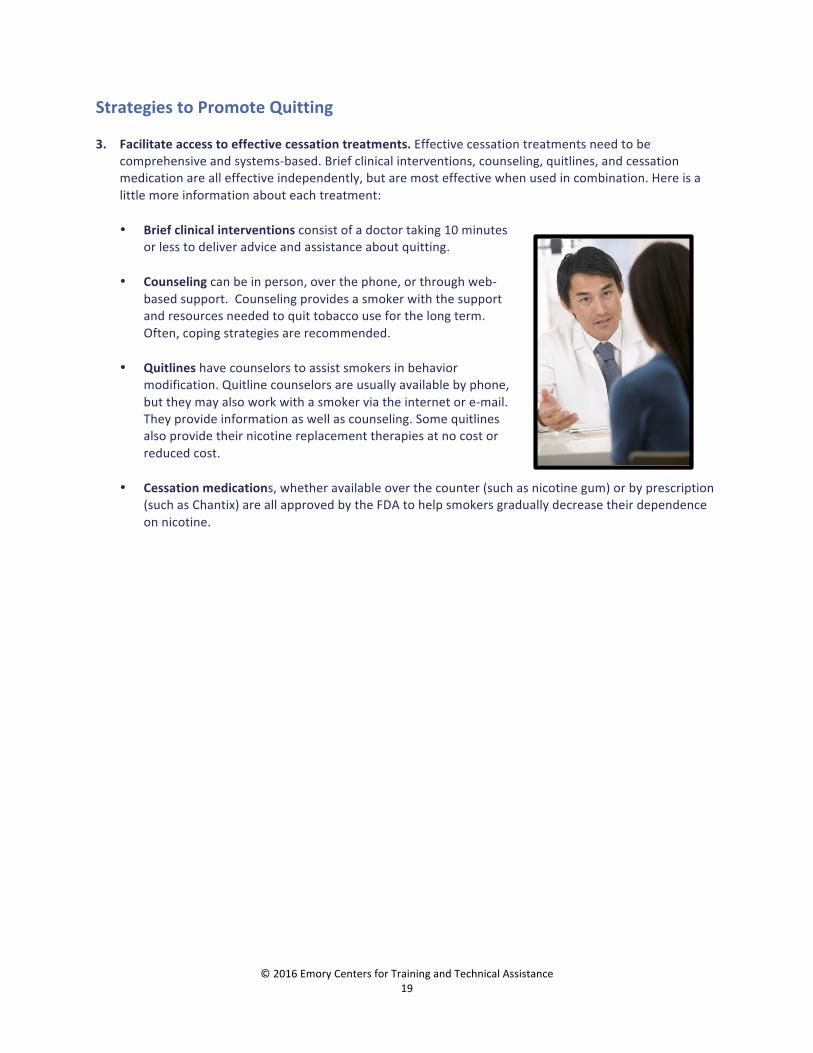
StrategiestoPromoteQuitting3. Facilitateaccesstoeffectivecessationtreatments.Effectivecessationtreatmentsneedtobe
comprehensiveandsystems-based.Briefclinicalinterventions,counseling,quitlines,andcessationmedicationarealleffectiveindependently,butaremosteffectivewhenusedincombination.Hereisalittlemoreinformationabouteachtreatment:
• Briefclinicalinterventionsconsistofadoctortaking10minutes
orlesstodeliveradviceandassistanceaboutquitting.• Counselingcanbeinperson,overthephone,orthroughweb-
basedsupport.Counselingprovidesasmokerwiththesupportandresourcesneededtoquittobaccouseforthelongterm.Often,copingstrategiesarerecommended.
• Quitlineshavecounselorstoassistsmokersinbehavior
modification.Quitlinecounselorsareusuallyavailablebyphone,buttheymayalsoworkwithasmokerviatheinternetore-mail.Theyprovideinformationaswellascounseling.Somequitlinesalsoprovidetheirnicotinereplacementtherapiesatnocostorreducedcost.
• Cessationmedications,whetheravailableoverthecounter(suchasnicotinegum)orbyprescription
(suchasChantix)areallapprovedbytheFDAtohelpsmokersgraduallydecreasetheirdependenceonnicotine.

©2016EmoryCentersforTrainingandTechnicalAssistance20
StrategiestoPromoteQuitting4. Utilizeacomprehensiveapproachtocessationinterventions.Forcessationinterventionstobeeffective
ingettingalargepopulationtoquittobacco,theapproachesmustbecomprehensiveandwellintegrated.Forexample:
• Peopleneedtoknowthatresourceslike1-800QUIT-
NOWexisttohelpwithquitting.Thatrequiresusingallthecommunicationmethodsavailablenowadays—notjustbrochures,butmassmediaadvertisingcampaignsthatincludesocialnetworkingmethodslikeFacebookandTwitter.
• Healthcareprovidersmustbetrainedtoeffectivelyintervenewiththeirpatientsaboutthehazardsoftobaccouseandreferthemtoquitlinesandothertreatmentoptions.Thehealthcaresystemneedstomakeaskingabouttobaccouseasroutineascheckingbloodpressure.
• Worksitewellnessandhealthcenterprogramsneedtoincludeeducationabouttheharmsof
tobaccoandreferraltocessationprogramsincludingquitlines.
• PaymentforcessationtreatmentsneedtobecoveredbyMedicaid,privateandpublichealthinsuranceandmanagedcare.

©2016EmoryCentersforTrainingandTechnicalAssistance21
StrategiestoEliminateExposuretoSecondhandSmokeThethirdgoaldescribedinCDC’sBestPracticesistoeliminatenonsmokers’exposuretosecondhandsmoke.Thebestwaytodothisisthrough100%smoke-freelawsandpoliciesforpublicplacesandworksites.Smoke-freeairpoliciesprotectnonsmokersfromexposuretosecondhandsmokeandalsoreducethenumberofsmokersandnumberofcigarettessmoked.AsdescribedinPartTwo,LessonThree,therehasbeenmuchprogressinincreasingthenumberofsmoke-freepoliciesthroughoutthecountry.However,therearestillseveralbarrierstoeffectivelyimplementingsmoke-freepolicy.Wewilldiscussafewofthemostcommonbarriersandtrapstoavoidwhenenactingsmoke-freelawsnext.
Formoreinformationonhowtodevelopsmoke-freepolicies…CheckoutthisToolkitforImplementingSmoke-FreeLaws:http://goingsmokefree.org/index.html

©2016EmoryCentersforTrainingandTechnicalAssistance22
StrategiestoEliminateExposuretoSecondhandSmoke:PitfallstoAvoid1. Avoidvoluntarysmoke-freepolicieswheneverpossible.Smoke-freepoliciescanbeeithervoluntaryor
regulatoryefforts.Voluntarypoliciesareoftenusedinprivatesettingswherethereislessprecedenceforgovernmentalregulation.Promotingvoluntarysmoke-freeenvironmentscanalsoactasafirststeptolaythegroundworkforacitywideordinanceorastatewidelaw,andcanbeusefulineducatingbusinessownersandthepublic.However,theconsensusamongtobaccocontrolorganizationsisthatcomprehensivesmoke-freepoliciesshouldbeputintoplacebyordinance,regulation,orlawratherthanvoluntarily.Thisisbecause:
• Voluntarysmoke-freepoliciesdonotnecessarilyleadtothepassageofsmoke-freeordinances,and
canevenbeseenbylawmakersasareasontonotpassregulations.• Itcanbemuchmoredifficultandtimeconsumingtoconvincebusinessownerstoenactvoluntary
policiesonebyonethantoworkdirectlywithamayororcitycouncil.• Therearefewconsequencesfornoncompliancewithvoluntarypolicies,comparedtoregulatory
efforts,wherelegalconsequences(e.g.fines)arepossible.• Voluntarypoliciesarenotpermanentandcanbeeliminatedeasilywithchangesinownershipor
management.
©2016EmoryCentersforTrainingandTechnicalAssistance23
StrategiestoEliminateExposuretoSecondhandSmoke:PitfallstoAvoid2. Don’tforgettohaveimplementationandenforcementplansinplace.Inthepast,mostlocalsmoking
ordinanceswereconsideredself-enforcing,andthevastmajorityofbusinessesandsmokerscompliedwithalaw'sprovisions.Althoughmostbusinessownersandsmokersstillreadilycomplywithsmoke-freelaws,acomprehensiveimplementationplan,includingwell-draftedregulationsandpenalties,shouldbeinplacetoanticipateandaddresspotentialenforcementproblems.
3. Avoidaddingapreemptionclausetothepolicyatallcosts.Preemptionisaprovisionatonelevelof
government(usuallyfederalorstate)thatpreventsalowerlevelfromenactingstrongerlawsonanissuethatexistatthehighergovernmentlevel.Oneofthetobaccoindustry’sfavoritetacticshasbeentolobbystatelegislaturestopreemptlocalsmoke-freelaws.Thistacticshiftsthestruggleforsmoke-freeairfromlocaljurisdictions,wheregrassrootssmoke-freeadvocateshavetheupperhand,tothestatelegislature,wherethetobaccoindustrywieldssubstantialinfluence.
Formoreinformationonwhylocalcontrolissoimportant…VisittheProtectLocalControlwebsite:http://www.protectlocalcontrol.org/whylocal.php

©2016EmoryCentersforTrainingandTechnicalAssistance24
StrategiestoEliminateExposuretoSecondhandSmoke:PitfallstoAvoid
4. Avoidprovisionsandexemptionsthatinhibittheeffectsofsmoke-freepolicies.TheFundamentalsofSmoke-freeWorkplaceLawsprovidesaverygoodfoundationofthestepstofollowleadingtothepassageofaneffectivesmoke-freepolicyandlistsseveralprovisionstoavoidintheprocessofdraftingandnegotiatingsmoke-freepolicies.Thelistbelowhighlightsafewofthem:• VentilationProvisions:Havingventilationsystemscannotcompletelyremovethecancer-causing
andtoxicchemicalsinsecondhandsmoke.Going100%smoke-freenotonlyprotectsemployeesandpatrons,butalsoprotectsbusinessowners’bottomlineforboththeshortandlongterms.
• “MinorsOnly”orAgeRestrictionProvisions:Theseprovisionsprohibitsmokingonlyinsettings
whereminorsarepresent.Smokingispermittedinrestaurants,bars,bowlingalleys,and/orotherbusinessesaslongasthesevenuesareoff-limitstominors.Theseprovisionsareinconsistentwiththepurposeofsmoke-freepolicy,whichistoprotectallpeople,includingworkers,fromsecondhandsmoke.
• Exemptionsformembershipassociations(privateclubs):Membershipassociations(alsoreferredto
as“privateclubs”)arerarelyprivateatall.Thepublicmaybemisledtobelievetheyare“private”spaces,butinpractice,theyareoftenopentothepublicatcertaintimesandmayhavepaidemployees.Ifanorganizationhasemployees,itshouldbetreatedlikeanyotherworkplaceandofferthesameprotectionsfortheiremployees.
• Exemptionsfortobaccoretailshops,cigarbars,andhookahbars:Theseexemptions,althoughonce
common,arenolongerthenorm.Thetobaccoindustryandotheroppositiongroupscontinuetoassertthattheseestablishmentswarrantexemption.Inreality,thesebusinessesarenodifferentthananyotherworkplaceorpublicplace.Allemployees,nomatterwheretheyareemployed,deservetherighttobreathecleanairatwork.
• Exemptionsfor(non-tribal)casinosandgamingestablishments:Casinoworkers,likeotherworkers,
deservecompleteprotectionfromsecondhandsmoke.Thegamingindustryhasextremelydeeppocketsandiswillingtospendcountlessdollarsjoiningthetobaccoindustryandfightingsmoke-freelaws.Althoughtribalcasinosareunderthejurisdictionofatribe,non-tribalcasinosshouldbeincludedincomprehensivesmoke-freepolicies.
• “Hardship”Exemptions:Hardshipexemptionsallowrestaurants,bars,orotherhospitality
businessestoobtainawaiverfromcomplyingwithasmoke-freelawbecausedoingsosupposedlycausesthemeconomicharm.Peer-reviewedstudiesthatexamineobjectivemeasuressuchassalestaxreceiptsandemploymentlevelshaveconsistentlyfoundthatthisisnotthecase.

©2016EmoryCentersforTrainingandTechnicalAssistance25
StrategiestoEliminateExposuretoSecondhandSmoke:NewFrontiersTheprogressintheadoptionofcomprehensivesmoke-freepublicandworkplacespoliciesdoesn’tmeanthebattlesforsmoke-freeplacesareover.Itjustmeansthefocusshiftstootherfronts:Multi-unithousing:Manypropertiesaregoingcompletelysmoke-free,andseveralstatesnowhaveprogramsunderwaytosupporttheadoptionofsmoke-freehousingpolicies.Publichousingauthoritiesareexpandingtheirnumberofsmoke-freeunitsandinsomecasesmakingalloftheirpropertiessmoke-free.Policiesinprivatelyownedhousingarevoluntaryandcomeaboutbytenantstakingactionandeducatingownersandlandlordsabouteconomicadvantagesofbecomingsmoke-free.
Residentialtreatmentfacilities:Smokingbansandcessationsupportinresidentialtreatmentfacilities(e.g.formentalhealthandsubstance-abusetreatment)canreducetobacco-relateddisparitiesamongpeoplewithmentalillnessandaddictions.One2010studyfoundthatamongstate-ownedtreatmentfacilitiesinOregon,only15%hadvoluntarilyimplemented100%smoke-freecampuspolicies,and47%offeredcessationresourcesatpatientdischarge.However,lessthan10%offacilitiesexpressedoppositiontothesefuturerequirements.
Collegeandworksitecampuses:Smoke-freeandtobacco-freecampusinitiativesforworksitesandcollegecampusesareunderwayinmanycommunities.Tobacco-freecampusescreateenvironmentsinwhichtobaccousersfinditeasiertoreducetheirconsumptionorquitaltogether.Inacollegesetting,thiswillhelpdecreasethehighertobaccouseratesamongyoungadults.
Formoreinformation…onnewfrontiersinsmoke-freepolicy:
• VisittheAmericansforNon-SmokersRightswebsiteforanexcellentlistofsmoke-freemulti-unithousingresourcesandtools.
• CheckoutthisCDCfactsheetandlistofresourcesfortobacco-freeworksites.• VisittheTobacco-FreeCollegeCampusInitiativewebsiteforinformationontobacco-free
collegecampusefforts.

©2016EmoryCentersforTrainingandTechnicalAssistance26
StrategiestoEliminateTobacco-RelatedDisparitiesNowwecometothefourthgoalofatobaccocontrolprogram,eliminatingtobacco-relateddisparities.Healthdisparitiesaretypesofunfairhealthdifferencescloselylinkedwithsocial,economicorenvironmentaldisadvantagesthatadverselyaffectgroupsofpeople.Relatedtohealthdisparitiesisthebroaderconceptofhealthequity.Healthequityisachievedwheneachpersonhastheopportunitytorealizehisorherfullhealthpotentialandnopersonisdisadvantagedfromachievingthispotentialbecauseofsocialpositionorothersociallydeterminedcircumstances.Eliminatinghealthdisparities,likethoseseensurroundingtobaccouse,isasteptowardsachievinghealthequity
Aswesaidpreviously,somepopulationshaveahigherthanaveragerateoftobaccouseandtobacco-relateddeathanddisease.Theseabove-averageratesarereferredtoas“tobacco-relateddisparities.”Examplesofpopulationswithknowntobacco-relateddisparitiesinclude:
• LGBTs• AfricanAmericans• NativeAmericans/AlaskanNatives• Hispanics• Youngadults• Peoplewithlowincomes
Next,wewilldiscussstrategiesthatmoveuse closertohealthequitybyworkingtoeliminatetobacco-relateddisparities.

©2016EmoryCentersforTrainingandTechnicalAssistance27
StrategiestoEliminateTobacco-RelatedDisparities1. Identifywhichpopulationsexperiencedisparitiesinyour
community.Populationswithtobacco-relateddisparities,aswellasthecausesofthesedisparitiesinthepopulation,canvarysignificantlyfromplacetoplace.Checkyourstateandlocaldatatoidentifytobacco-relateddisparitiesinthepopulationsyoureach.Localandstatedepartmentsofhealthareoftengoodsourcesforthisdata.NationaldatafromnationalsurveyresultsarepostedontheCDCwebsite,andtheNationalNetworksforTobaccoControlandPreventionarealsoimportantresourcesforprogramsastheyplanandimplementactivitiestoreducetobaccorelateddisparities.
Itisimportanttonotethatnationalandevenstatedatamaynotcorrespondwiththedataforyourcommunity.Thepopulationgroupsmayberelativelysmall,necessitatingtheuseofsupplementalsurveystoobtainreliabledata.
2. Incorporateachievinghealthequitybyeliminatingdisparitiesintoprogramactivityplans.Theseactivitiesshouldberelatedtopreventinginitiationamongyoungpeople,promotingcessation,andeliminatingsecondhandsmokeexposure.Youwillneedtousestrategiesthathavebeenshowntoworkbestwiththeparticularpopulationathand,andengagethepopulationintheprocess.Plantoreachouttothesepopulationsutilizingacommunitymembertoactasaspokespersonfortheprogram.

©2016EmoryCentersforTrainingandTechnicalAssistance28
StrategiestoEliminateTobacco-RelatedDisparities3. UtilizeBestPracticesasaguidetoaddressdisparities.TheCDC’sBestPracticesguidealsorecommends
programsincludetheseactivitieswhenaddressingtobacco-relateddisparities:
• Conductingapopulationassessmenttoguideefforts• Identifyingandassemblingadiverseandinclusivestakeholdergroup• Prioritizingreductionintobacco-relateddisparitiesandassessingcapacity• Developingastrategicplan• Fundingcommunityorganizationstoimplementprovenorpromisinginterventions• Providingculturallycompetenttechnicalassistanceandtrainingtogranteesandpartners• Evaluatinginterventionefficacyandrefiningefforts
Evaluatingtheprocessusedandtheresultswillleadtomoreeffectiveuseofresourcesinthefuture.Documentingtheimprovementsinreducingdisparitiesbroughtaboutbyyourprogramhelpsbuildthecaseforcontinuedfundingandalong-termprogram.

©2016EmoryCentersforTrainingandTechnicalAssistance29
EliminatingTobacco-RelatedDisparities:PolicyandSystemChangesWhenyouusecomprehensive,evidence-basedpracticesthatfocusonpolicyandsystemschange,theresultscanbebothpopulationwideandcommunityspecific,andoftenleadtoreductionsintobacco-relateddisparities.Someexamples:
• Acountysmoke-freeworkplacelawbenefitstheentirepopulation,butbenefitsworkersintheaffectedestablishmentsthemost.Frequentlyworkersinthehospitalityindustryarelowerincomeandmayrepresentminoritypopulationsdisproportionately.Acomprehensivebanofsmokinginrestaurantbarscanleadtoeliminatingdisparitiesinexposuretosecondhandsmoke.
• Changinghealthcaresystemsoftencreatesopportunitiestotargetprovidersandsystemsthatserve
populationswithtobacco-relateddisparities.ThestateofMassachusettsexpandedMedicaidinsurancebenefitstoincludecessationtreatmentsandpairedthatchangewithaneducationcampaignforbothhealthcareprovidersandpeopleonMedicaid.Theresultwasmoresuccessfulquitattemptsanddecreasedsmokingprevalenceamongapopulationwithhistoricallyhighratesofsmoking.
• TheAmericanLegacyFoundationsupportsinnovativeapproachestoreachingpopulationswith
tobacco-relateddisparities.TheHeadStartTobaccoCessationInitiativeisanexampleofintegratingtobaccocontrolpracticesintoanestablishededucationalprogramservinglow-incomefamilies.TheInitiativeallowedHeadStartandtobaccocontrolprogramstoachievetheirsharedobjectivesrelatedtothedevelopmentofhealthyenvironmentsforchildrenandfamiliesandtosystematicallyaddresstheissueoftobaccocessationandsecondhandsmokeexposure.

©2016EmoryCentersforTrainingandTechnicalAssistance30
MovingForward:StrategiesforSuccessOnecommonprincipleinachievingresultsacrossallfourofthegoalsdiscussedisthattobaccocontrolprogramscannotdoitalone.Successwillcomethroughworkinginpartnershipswithorganizationsandcommunitymembers.Manystateshaveadoptedahealthycommunityapproachwhereindividuals,agencies,andorganizationsworktogethertotakeonacomplexmixofsocial,cultural,economic,andpoliticalissuesinordertodiscouragetobaccouse.
Restrictionsontobaccoads
Identifiabletobaccocontrol
Hightaxesontobacco
Nosalesoftobaccotominors
Publiceducationcampaigns
Cessationservices
Tobacco-freepublicplacesand
Detailedplanofaction
Monitor&countertobaccoinfluence
Tobacco-freeschoolcampuses
FormoreinformationaboutCommunitiesofExcellence…
CheckoutCommunitiesofExcellencePlus,atrainingdevelopedbyTTACthroughgrantsfromtheRobertWoodJohnsonFoundation,theAmericanLegacyFoundation,andtheAmericanCancerSociety.Theprogrambuildsskillsamongcommunitymemberstoassess,planandimplementeffectivetobaccocontrolprogramsbasedonCDC-recommendedbestpractices.
©2016EmoryCentersforTrainingandTechnicalAssistance31
Part2,LessonFourConclusion
Inthislesson,wediscussedthefivestepsthatgointoimplementingatobaccocontrolprogram:
1. Engagestakeholders2. Developastrategicplan3. Implementtheprogram4. Evaluatetheprogram5. Sustaintheprogram
Welookedatseveralwaysinwhichtobaccocontrolprogramscanworktobecomesustainableoverthelong-term.WealsorevisitedthefourgoalsoftheNationalTobaccoControlProgram,
1. Preventinitiationamongyouthandyoungadults.2. Promotequittingamongadultsandyouth.3. Eliminateexposuretosecondhandsmoke.4. Identifyandeliminatetobacco-relateddisparitiesamongpopulations
andexaminedseveralstrategiesthatworktoachievethosegoalsatthestateandcommunitylevel.

©2016EmoryCentersforTrainingandTechnicalAssistance32
Tobacco101Conclusion:MovingForwardwithStrategiesforSuccess
Thefieldoftobaccocontrolmobilizescommunitiestoapplyevidence-basedstrategiesthatrepeatedlydemonstratethatthepublichealthapproachtotobaccocontroliseffectiveatreducingtobaccouse.Theroadtosuccesscanbealongone,butisworththeeffort.Therearemanywaysthattobaccousetakesatollonthepeople,businesses,andhealthcaresystemswhereyouliveandwork.Yourjobistoreducethattoll,andmanycommunitiesacrosstheUnitedStateshavebeguntomakeamazingprogressbyengaginginstrategiesthatworktoreducetobaccouseandeliminatedisparitiesbyincreasingthepriceoftobacco,enactingandenforcingsmoke-freeairlawsandpolicies,andprovidingsystems-basedcessationservices.
Canyouimagineaworldwithouttobacco?
Withoutthedeathanddiseasethattobaccocausespeople?
Weknowthesolutiontotheproblem.Nowlet’smakeatobacco-freeworldareality.
©2016EmoryCentersforTrainingandTechnicalAssistance33
LessonFourCheckforUnderstanding
1. TrueorFalse:Pleasedeterminewhetherthefollowingstatementsaretrueorfalse.
___ a.Thefivestepsthatgointoimplementingatobaccocontrolprogramare:1)Engagestakeholders,2)Developastrategicplan,3)Implementtheprogram,4)Evaluatetheprogram,and5)Sustaintheprogram.
___ b.Thesamemessagescanbeusedtorecruitalltypesofcommunitypartners,sincetobacco
affectsthemallinessentiallythesameway.
___ c.Sustainingacomprehensivetobaccocontrolprogramshouldbeanon-goingactivityforyouandyourpartners.
___ d.Populationswithtobacco-relateddisparitiescanvarysignificantlyfromplacetoplace.___ e.Cessationtreatmentsandservicesaremosteffectivewhenusedaloneinsteadofin
combination.2. WhichofthefollowingstrategieswasNOTmentionedinthislessonasaneffectivewaytoprevent
youthtobaccoinitiation?a. Changingsocialnormssurroundingtobacco.b. Raisingthepriceoftobacco.c. Educatingretailersaboutsellingtobaccotominors.d. Changinghowtobaccoismarketed.e. Empoweringyoungpeoplebyinvolvingthemintobaccocontrol.
3. Whichofthefollowingstatementsbestdescribeaneffective100%smoke-freepolicy?Chooseall
thatapply.a. Thepolicyisvoluntarilyputinplacebybusinessowners.b. Thepolicyisbackedbyimplementationandenforcementplans.c. Thepolicyincludesapreemptionclause.d. Thepolicydoesnothaveexemptionsforprivateclubs,tobaccoshops,andcasinos.e. Thepolicyhasprovisionsthatonlyallowsmokinginspeciallyventilatedareas.
4. HowwelldoyouthinkyourstateisdoingintermsofmeetingthefourgoalsoutlinedinBest
Practices?Whataresomestrategiesfromthislessonthatyourstatecouldusetoimproveprogress?FeelfreetoreferencethisinfographicandchartfromtheTobaccoControlNetworktogetstarted.
5. Whatpopulationismostaffectedbytobaccorelateddisparitiesinyourownstate?Whydoyou
thinkthatis?FeelfreetoreferencetheCDC’swebsitetocheckthedataforyourstate.

©2016EmoryCentersforTrainingandTechnicalAssistance34
LessonFourCheckforUnderstandingAnswers
1. TrueorFalse:Pleasedeterminewhetherthefollowingstatementsaretrueorfalse.
___ a.Thefivestepsthatgointoimplementingatobaccocontrolprogramare:1)Engagestakeholders,2)Developastrategicplan,3)Implementtheprogram,4)Evaluatetheprogram,and5)Sustaintheprogram.
___ b.Thesamemessagescanbeusedtorecruitalltypesofcommunitypartners,sincetobacco
affectsthemallinessentiallythesameway.
___ c.Sustainingacomprehensivetobaccocontrolprogramshouldbeanon-goingactivityforyouandyourpartners.
___ d.Populationswithtobacco-relateddisparitiescanvarysignificantlyfromplacetoplace.___ e.Cessationtreatmentsandservicesaremosteffectivewhenusedaloneinsteadofin
combination.
CorrectAnswers:a. True-Needtoreview?Gobacktothe“ImplementingPrograms”page.b. False–Needtoreview?Gobacktothe“Step1:EngageStakeholders”pages.c. True–Needtoreview?Gobacktothe“Step5:SustaintheProgram”pages.d. True–Needtoreview?Gobacktothe“StrategiestoEliminateTobacco-RelatedDisparities”pages.e. False–Needtoreview?Gobacktothe“StrategiestoPromoteQuitting”pages.2. WhichofthefollowingstrategieswasNOTmentionedinthislessonasaneffectivewaytoprevent
youthtobaccoinitiation?a. Changingsocialnormssurroundingtobacco.b. Raisingthepriceoftobacco.c. Educatingretailersaboutsellingtobaccotominors.d. Changinghowtobaccoismarketed.e. Empoweringyoungpeoplebyinvolvingthemintobaccocontrol.
CorrectAnswer:c-Needtoreview?Gobacktothe“StrategiestoPreventInitiationamongYoungSmokers”pages.

©2016EmoryCentersforTrainingandTechnicalAssistance35
3. Whichofthefollowingstatementsbestdescribeaneffective100%smoke-freepolicy?Chooseallthatapply.
a. Thepolicyisvoluntarilyputinplacebybusinessowners.b. Thepolicyisbackedbyimplementationandenforcementplans.c. Thepolicyincludesapreemptionclause.d. Thepolicydoesnothaveexemptionsforprivateclubs,tobaccoshops,andcasinos.e. Thepolicyhasprovisionsthatonlyallowsmokinginspeciallyventilatedareas.
CorrectAnswer:bandd–Needtoreview?Gobacktothe“StrategiestoEliminateExposuretoSecondhandSmoke”pages.
4. HowwelldoyouthinkyourstateisdoingintermsofmeetingthefourgoalsoutlinedinBest
Practices?Whataresomestrategiesfromthislessonthatyourstatecouldusetoimproveprogress?FeelfreetoreferencethisinfographicandchartfromtheTobaccoControlNetworktogetstarted.
Answerswillvary.5. Whatpopulationismostaffectedbytobaccorelateddisparitiesinyourownstate?Whydoyou
thinkthatis?FeelfreetoreferencetheCDC’swebsitetocheckthedataforyourstate.
Answerswillvary.

©2016EmoryCentersforTrainingandTechnicalAssistance36
SourcesThroughout:CentersforDiseaseControlandPrevention.Bestpracticesforcomprehensivetobaccocontrolprograms,2007.Availableat:http://www.cdc.gov/tobacco/stateandcommunity/best_practices/index.htmThroughout:CommunityPreventiveServicesTaskForce:TheCommunityGuide–Tobacco.Availableat:http://www.thecommunityguide.org/tobacco/index.htmlSlide3,4,5:FawcettSB,Paine-AndrewsA,FranciscoVT,SchultzJA,RichterKP,LewisRK,WilliamsEL,HarrisKJ,BerkleyJY,FisherJL,LewisCM.Usingempowermenttheoryincollaborativepartnershipsforcommunityhealthanddevelopment.AmericanJournalofCommunityPsychology.23(5):1995:677-697.Slide3,4,5:CentersforDiseaseControlandPrevention.BestPracticesforComprehensiveTobaccoControlPrograms:UserGuide–Coalitions:StateandCommunityInterventions.(n.d.)Availableat:http://www.cdc.gov/tobacco/stateandcommunity/bp_user_guide/pdfs/user_guide.pdfSlide9,10:CentersforDiseaseControlandPrevention.SustainingStateProgramsforTobaccoControl:OSHStrategicPriority.Availableat:http://www.cdc.gov/tobacco/tobacco_control_programs/program_development/sustainingstates/pdfs/strategic.pdfSlide11:CentersforDiseaseControlandPrevention.SustainingStateProgramsforTobaccoControl:AStoryfromColorado.Availableat:http://www.cdc.gov/tobacco/tobacco_control_programs/program_development/sustainingstates/pdfs/colorado.pdf
Slide13:CampaignforTobacco-FreeKids.TobaccoUseamongYouth.Availableat:http://www.tobaccofreekids.org/research/factsheets/pdf/0002.pdfSlide13:CenterforPublicHealthandTobaccoPolicy.CauseandEffect:TobaccoMarketingIncreasesYouthTobaccoUse-Findingsofthe2012SurgeonGeneral’sReport.Availableat:http://www.tobaccopolicycenter.org/documents/SGR%20NY%205-25-12.pdfSlide13:CampaignforTobacco-FreeKids.FederalBanonCandyandFruit-FlavoredCigarettes.Availableat:http://www.tobaccofreekids.org/Script/DisplayPressRelease.php3?Display=1176Slide13,14:U.S.DepartmentofHealthandHumanServices.PreventingTobaccoUseAmongYouthandYoungAdults:AReportoftheSurgeonGeneral.Atlanta,GA:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention,NationalCenterforChronicDiseasePreventionandHealthPromotion,OfficeonSmokingandHealth,2012.Availableat:http://www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-use/index.htmlSlide13,14:CentersforDiseaseControlandPrevention.BestPracticesUserGuide:YouthEngagement–StateandCommunityInterventions.Atlanta:U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention,NationalCenterforChronicDiseasePreventionandHealthPromotion,OfficeonSmokingandHealth,2010.Availableat:http://www.cdc.gov/tobacco/stateandcommunity/bp_userguide_youth/pdfs/youth_engagement.pdfSlide13,14,15:CampaignforTobacco-FreeKids.RaisingCigaretteTaxesReducesSmoking,EspeciallyAmongKids(andtheCigaretteCompaniesKnowit).Availableat:http://www.tobaccofreekids.org/research/factsheets/pdf/0146.pdf

©2016EmoryCentersforTrainingandTechnicalAssistance37
Slide15:Wilson,N,Sertsou,G,Edwards,R,Thomson,G,Grigg,M,andLi,J.ANewNationalSmokefreeLawIncreasedCallstoaNationalQuitline.BMCPublicHealth.2007;7:75.Slide15:Shields,M.SmokingBans:InfluenceonSmokingPrevalence.HealthReports(StatisticsCanada,Catalogue82-003)2007;18(3):9-25.Slide15,16,17:CentersforDiseaseControlandPrevention(CDC).SmokingandTobaccoUse:SmokingCessation.Availableat:www.cdc.gov/tobacco/data_statistics/fact_sheets/cessation/quitting/index.htmSlide15,16,17:FioreMC,JaénCR,BakerTB,etal.TreatingTobaccoUseandDependence:2008Update.ClinicalPracticeGuideline.Rockville,MD:U.S.DepartmentofHealthandHumanServices.PublicHealthService.May2008.Availableat:http://www.ncbi.nlm.nih.gov/books/NBK63952/Slide18:OfficeoftheSurgeonGeneral.TheHealthConsequencesofInvoluntaryExposuretoTobaccoSmoke:AReportoftheSurgeonGeneral,2006.Availableat:http://www.surgeongeneral.gov/library/secondhandsmoke/report/index.htmlSlide19,20,21:AmericanforNonsmokers’Rights.FundamentalsofSmokefreeWorkplaceLaws.Availableat:http://www.no-smoke.org/pdf/CIA_Fundamentals.pdfSlide19,20,21:TobaccoTechnicalAssistanceConsortium(TTAC).DevelopingSmokefreeImplementationRegulations.Availableat:http://www.ttac.org/services/DSIR/index.htmlSlide20:AmericansforNonsmokers’Rights.StateswithanyTypeofPreemptionofSmokefreeAirLaws.Availableat:http://www.no-smoke.org/pdf/preemptionmap.pdfSlide21:AmericansforNonsmokers’Rights.WhattoExpectDuringImplementation.Availableat:http://goingsmokefree.org/overview/expectations.htmlSlide22:AmericanLungAssociation.Smoke-FreeMulti-UnitHousing:BringingHealthyAirHome.Availableat:http://www.lung.org/assets/documents/healthy-air/smuh-policy-brief-update.pdfSlide22:DrachLL,MorrisD,CushingC,RomoliC,HarrisRL.Promotingsmoke-freeenvironmentsandtobaccocessationinresidentialtreatmentfacilitiesformentalhealthandaddictions,Oregon,2010.Availableat:http://www.cdc.gov/pcd/issues/2012/pdf/11_0080.pdfSlide22:UniversityofMichiganTobacco-freeCollegeCampusInitiative.Availableat:http://sph.umich.edu/tfcci/partners.htmlSlide23:CentersforDiseaseControlandPrevention(CDC).ChronicDiseasePreventionandhealthPromotion:HealthEquity.Availableat:http://www.cdc.gov/chronicdisease/healthequity/index.htmSlide23,24:CentersforDiseaseControlandPrevention,SpecificPopulations.Availableat:http://www.cdc.gov/tobacco/data_statistics/by_topic/populations/index.htmSlide26:MassachusettsDepartmentofPublicHealthTobaccoCessationandPreventionProgram.MassHealthSmokingCessationBenefitBriefingNotes.Availableat:http://makesmokinghistory.org/uploads/Briefing%20Notes%20on%20MassHealth%20Smoking%20Cessation%20Benefit%201-6-12.pdfSlide26:Legacy.Legacy’sHeadStartTobaccoCessationInitiative.Availableat:http://www.legacyforhealth.org/4070.aspx

©2016EmoryCentersforTrainingandTechnicalAssistance38
Slide27:TobaccoTechnicalAssistanceConsortium.CommunitiesofExcellencePlus:Afreshapproachtobuildingtobaccocontrolcapacity.Availableat:http://www.ttac.org/services/pdfs/Communities_Excellence_Plus.pdf
ImagesSlide9:CentersforDiseaseControlandPrevention.SustainingStateProgramsforTobaccoControl:OSHStrategicPriority.Availableat:http://www.cdc.gov/tobacco/tobacco_control_programs/program_development/sustainingstates/pdfs/strategic.pdfSlide12:CentersforDiseaseControlandPrevention.Bestpracticesforcomprehensivetobaccocontrolprograms,2007.Available:http://www.cdc.gov/tobacco/stateandcommunity/best_practices/index.htm
Slide12:CommunityPreventiveServicesTaskForce:TheCommunityGuide–Tobacco.Availableat:http://www.thecommunityguide.org/tobacco/index.html
Recommended







![[Insert your name and information here] 1 Tobacco 101](https://img.pdfslide.net/doc/110x75/56649d125503460f949e5b8a/insert-your-name-and-information-here-1-tobacco-101.jpg)