ESOPHAGEAL ATRESIA
&
TRACHEOESOPHAGEAL
FISTULA

Abberation in developmental of esophagus
with or with out communication with
trachea.
Incidence - 1 in 3,570 to 1 in 4,500.

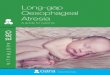
Successive stages in the development of the
tracheoesophageal septum during embryologic
development (A) The laryngotracheal
diverticulum forms as a ventral outpouching from the caudal part of the primitive pharynx.
(B) Longitudinal tracheoesophageal folds begin to fuse toward the midline to eventually form the tracheoesophageal septum.
(C) The tracheoesophageal septum has completely formed.
(D) If the tracheoesophageal septum deviates posteriorly, esophageal atresia with a tracheoesophageal fistula develops

• Esophageal occlusion & failure of recanalization.
Spontaneous posterior deviation of tracheoesophageal
septum.
• Mechanical factor pushing dorsal wall foregut anteriorly.
• Esophageal occlusion & failure of recanalization.
• Teratogen: doxorubicin.
• Component of cephalic neurocristopathy.
• HOX D group of genes. mutations in N-myc, Sox2, and
CHD7 genes - in syndromic EA-TEF with associated
anomalies.
• Defect in signaling pathway of the extracellular, organ
differentiation-promoting glycoprotein Shh
THEORIES OF EA & TEF

ANATOMIC VARIANTS
Are classified according to
• GROSS classification
• VOGT classification

7.8% 0.8% 85.7% 1.4% 4.2%

Anatomic Variations
85%
Most common
GROSS type C

Anatomic Variations
6%
2nd most common
Atresia alone,
no fistula
Small stomach,
gasless abdomen
Usually has a long
gap between the
esophageal ends
GROSS type A

Anatomic Variations
6%
No atresia of
the esophagus
Congenital
tracheoesophageal
fistula
"H" or "N" fistula
GROSS type E

Anatomic Variations
2%
Proximal tracheo-
esophageal fistula
No distal fistula
Small stomach,
gasless abdomen
Often has a long
gap between the
esophageal ends
GROSS type B

Anatomic Variations
l%
Proximal and
distal fistulas
("double fistula")
GROSS type D

VACTERL association: 20%
Vertebral: 17%
Anal 12%
Cardiac 20%
Renal 16%
Limb 5%
• CHARGE association: Cloboma, Heart defect, Atresia
choanae, developmental Retardation, Genital hypoplasia, Ear
deformity.
• Schisis association : Omphalocele, Neural Tube Defect,
Cleft Lip & Palate And Genital Hypoplasia.
SYNDROME ASSOCIATION:

ASSOCIATED ABNORMALITIES
Incidence of Associated Anomalies in Esophageal Atresia.
Anomaly Frequency (%)
Congenital heart disease 25
Urinary tract 22
Orthopaedic (mostly vertebral and radial) 15
Gastrointestinal (e.g., duodenal
atresia,imperforate anus) 22
Chromosomal (usually trisomy 18 or 21) 7
Total with one or more associated 58
anomalies

Associated Congenital Anomalies Reported in Patients
with Esophageal Atresia
System affected
Musculoskeletal
Gastrointestinal
Cardiac
Genitourinary.
Potential anomalies
Hemivertebrae, radial dysplasia or
amelia, polydactyly, syndactyly, rib
malformations, scoliosis, lower limb
defects
Imperforate anus, duodenal atresia,
malrotation, intestinal
malformations, Meckel's
diverticulum, annular pancreas
Ventricular septal defect, patent
ductus arteriosus, tetralogy of Fallot,
atrial septal defect, single umbilical
artery, right-sided aortic arch
Renal agenesis or dysplasia,
horseshoe kidney, polycystic kidney,
ureteral and urethral malformations,
hypospadias

Physiologic effects of distal tracheoesophageal
fistula
A-1. Hyaline membrane disease may necessitate higher ventilator pressures, which encourage air to pass through the distal fistula.
2. A distended abdomen elevates and "splints" the diaphragm.
3. Gastric distension may result in gastric rupture and pneumoperitoneum.
4. Passage of air through a distal tracheoesophageal fistula diminishes the effective tidal volume.

B- 1. Aspiration of gastric juices leads to soiling of the lungs and pneumonia
2. Gastroesophageal reflux
3. Direction of gastric fluid proximally through distal fistula.
4. Overflow of secretions or inadvertent feeding may contribute to aspiration and contamination of the airway. .
Physiologic effects of distal tracheoesophageal
fistula

DIAGNOSIS OF
ESOPHAGEAL ATRESIA
Antenatal Diagnosis:USG- (maternal
polyhydramnios, abnormal swallowing, a
distended upper esophageal pouch, a small
stomach)
Diagnostic suspicion is increased when
abnormalities known to be associated with
esophageal atresia are identified.
Predictive value- 20-40% only

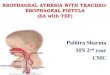
A B
1.Fluid filled stomach2.Bling ending pouch of oesophagus
Dilated blind ending proximal pouch

Fetal MRI
32 week fetus -esophageal atresia , absent stomach -marked polyhydramnios

Axial T2 of thorax-no oesophagus Sagittal T2: Fluid filled
blind ending
oesophgeal pouch

Clinical Diagnosis
Prematurity
Excessive salivation in form of drooling
(copious, fine, white, frothy bubbles of
mucus in the mouth and, sometimes, the
nose).
Episodes of choking,respiratory distress
after feeds

In pure oesophageal atresia (Type A)-scaphoid abdomen
In oesophageal atresis with only proximal fistula (Type B)-scaphoid abdomen
Type E-present later in 1st year.
with repeated respiratory infections , choking,coughing

Clinical Diagnosis
(A) Diagnosis of esophageal atresia is confirmed when a 10-Fr gauge catheter cannot be passed beyond 10 cm from the gums. (B) A smaller-caliber tube –not to be used –curling can give a false impression of esophageal
continuity.

The chest radiograph
A plain radiograph will
confirm the tube has not
reached the stomach
Type E-Not diagnosed

The Gasless Abdomen
Absence of gas in the
abdomen suggests
that the patient has
either atresia without
a fistula or atresia
with a proximal
fistula only

Contrast studies
Usually not needed
Should be performed by an
experienced pediatric
radiologist
With the use of a small
amount (0.5 to 1 mL) of
water-soluble non ionic
contrast.

Management
Goals of the initial treatment:1)Attention to ventilation 2)Keep upper pouch empty3)Treated on emergency basis

So:For ↓ aspiration risk:
1)elevate neonate’s head at least 30º in infant warmer
2)Use continuous suctionIV AB and electrolyte.

Management
In infants with respiratory failure, endotracheal
intubation should be performed.
Use oscillatory ventilation with high frequency
Gastrostomy may be neededplaced on the
water seal,elevated or Intermittently be
clamped

Summary of Preoperative
Investigations
Hb,S.electrolytes,BG cross match
A plain radiograph
2d Echocardiography
Renal ultrasonography

Type of Surgery
• Thoracotomy:
Extra-pleural
Trans pleural
• VAT







Post op
Adequate analgesia-fentanyl drip
Neck flexion
?intubation and sedation
Suction
After 5-7 days oesophagogram
-to see leak,distal patency ,motility.

EA without fistula
Problem is long gap (>3cm / 3vertebral bodies)
T/t- Cervical oseophagostomy+Gastrostomy
Definite repair after 12 wks

Maneuvers to lengthen oesophagus
Nonoperative
-Bougenaige
Proximal pouch
Distal pouch
Magnetic

Operative
Using native esophagus
-upper pouch mobilization
-upper pouch myotomy
-flap lengthening of upper pouch

Using oesophageal replacement
-Colon
-Stomach-Tube
-Jejenum-Pedicle graft or free graft
-Ileum

Comparison of technique
Thoracotomy
Scoliosis
Winged scapula
Shoulder weakness
Chest wall deformity
VATSuperior visualization
Improved cosmesis
Limited working space,
Lack of articulation of
instruments,
tying suture under
tension

Complications
• Early:
Anastomotic leak
Anastomotic stricture
Recurrent TEF
• Late:
GER
Tracheomalacia
Disordered esophageal peristalsis

Anastomotic leak
Major disruption occur 3% to 5% of postoperative
leak, typically recognized early
Factors for leak:
Poor surgical technique
Ischeamia of esophageal ends
Use of myotomy
Excessive tension at anastomotic site
Reoperation: control sepsis with drainage and repair by
pleural or pericardial patch, with or with out intercostals
muscle flap buttress.

Anastomotic stricture
Spitz & Hitchcock defined stricture as the
presence of symptoms: dysphagia & recurrent
respiratory problems from aspiration or foreign
body obstruction & narrowing noted on
endoscopy.
Stricture require dilatation occur upto 80% of
patient.
Prevention-PPI +/- Dilation

Factors responsible: Poor anastomotic
technique: excessive tension, two-layered
anastomosis, silk suture, ischemia at ends,
GER, Anastomotic leak.
Traditionally treated by dilatation:
antegrade or retrograde bouginage using Savory
dilator, Gruntzig balloon dilator
53% respond to single dilatation in the first
month.

Recurrent TEF In 3% to 14 %. Due to anastomotic leak with local
inflammation & erosion through the previous site of TEF.
Risk minimized by : Pleural flap;
Vascularized pericardial flap; Azygos vein
flap.

50% of recurrent fistula missed in routine
contrast study, esophagography in the prone
position under video fluroscopy;
Bronchoscopy with cannulation of fistula is
gold standard.
Traditionally repaired by thoracotomy &
interposition; Fibrin glue, Endoscopic eradication of TEF by chemicals
or diathermy.

GERD
Occurs up to 30% to 70% .
Probably relates to shortening of intra-abdominal portion or esophageal
motor dysfunction. 9% risk of developing barrett’s esophagus.
Suspected with GIT symptoms: vomiting, dysphagea & recurrent
anastomotic stenosis; Respiratory symptoms: stridor, cyanotic spells,
recurrent pneumonia, & reactive airway disease.
Diagnosed by, upper GI dye study, 24 H pH probe data, esophageal
manomatric study.
Medical management: thickening of feeding, H2 blocker, PPI, prokinetic
agent. 45% to 75% undergo anti reflux surgery.

Risk for death
Increased risk of death & long term morbidity
include:
1. Lower birth wt (<1500 g) &
prematurity.
2. Major CHD.
3. Severe associated anomaly &
ventilator dependent
4. Long gap EA.

Risk factor & Survival

Spitz Classification:

The end
Recommended