at SciVerse ScienceDirect
Parkinsonism and Related Disorders 19 (2013) 1061–1063
Contents lists available
Parkinsonism and Related Disorders
journal homepage: www.elsevier .com/locate/parkreldis
Letter to the Editor
Transcranial sonography in mitochondrial membraneprotein-associated neurodegeneration
Keywords:Transcranial sonographyNeurodegeneration with brain ironaccumulation (NBIA)Mitochondrial membraneprotein-associatedneurodegeneration (MPAN)
1353-8020/$ – see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.parkreldis.2013.06.020
sizes � 0was perfo
Pantothenate kinase-associated neurodegeneration (PKAN),caused by a mutation in the PANK2 gene, accounts for at least one-half of all neurodegeneration with brain iron accumulation (NBIA)cases [1]. A new NBIA subtype, mitochondrial membrane proteinassociated neurodegeneration (MPAN) was observed recently.MPAN is an autosomal recessive inherited subtype of NBIA thatwas newly identified in 2009 in a Polish cohort of 18 patients withNBIA [2]. It is caused bymutation in the orphangene C19orf12, whichencodes a protein expressed inmitochondria. The role of this proteinhas not been fully understood, but is likely involved in the synthesisof free fatty acids and in the biochemical pathways of valine, leucine,and isoleucine [2]. Although the extrapyramidal syndrome associ-ated with MPAN is similar to that of PKAN, the age of onset ofMPAN is later and its expression of symptoms is milder [2].
Transcranial sonography (TCS) is an alternative neuroimagingtechnique that displays characteristic changes of deep brain struc-tures in several neurodegenerative disorders [3]. Hyperechogenic-ity of substantia nigra (SN) has been observed in idiopathicParkinson’s disease (PD). Increased area of echogenicity of the SNhas been associated with increased tissue iron concentration [3].Considering the role of iron in SN hyperechogenicity TCS shouldbe a useful diagnostic tool in patients with NBIA.
TCS studies in PKAN patients have consistently revealed hyper-echogenicity of SN and lenticular nucleus (LN) [4]. We performedTSC in 3 MPAN patients admitted to our department to compareTCS results with PKAN patients.
After receiving informed written consent from the patients, weobtained information about their disease history, therapy, anddemographics. Patients were clinically examined by neurologists(AS and BK), blinded to imaging results.
TCS was performed through the preauricular acoustic bone win-dow with a 2.5-MHz phased array ultrasound system (Vivid 7; GE,Wisconsin, USA). The chosen ultrasound parameters were: penetra-tion depth 14–16 cm, dynamic range 50 dB. Image contrast andbrightness were adjusted visually to obtain the optimum image.The measurements were performed as described previously [4]. SNechogenic sizes �0.25 cm2 were classified as hyperechogenic and
All rights reserved.
.20 cm2 as normal for the ultrasound system used. TCSrmed by an investigator (MS) blinded toMRI results; a sec-
ond off-line analysis of anonymized TCS images was undertaken byan independent rater (UW). MRI was performed using a 1.5-T scan-ner (Philips Achieva, Eindhoven, The Netherlands). T1-weighted(TR ¼ 596 ms, TE ¼ 15 ms) and T2-weighted (TR ¼ 6783 ms,TE ¼ 140 ms) images were acquired in axial planes with 5-mm slicethickness. Gradient echo T2* images were obtained as a single-echosequence (TR ¼ 693 ms, TE ¼ 23 ms; flip angle ¼ 20�). MR imageswere assessed by a senior radiologist (RP) blinded to the TCS results.MRI and TCS studies were conducted on the same day.
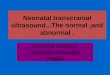
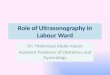
Demographic and clinical data are presented in Table 1. Two pa-tients (numbers 1 and 3) carried a heterozygous C19orf12mutation;one (number 2) carried a homozygous mutation. All patients hadaxonal neuropathy; two had dystonia and two had pyramidal signs.One patient had severe optic atrophy and another had paranoidschizophrenia. In all cases, the T2- and T2*-weighted MR images ofthe brain revealed low bilateral signal intensity in the GP and SN,with no other abnormal findings (Table 1; Fig. 1A,B). None of our pa-tients exhibited the “eye of the tiger” sign on T2-weighted MRI.
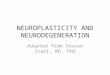
All patients had sufficient transtemporal bone windows for TCS.TCS revealed alterations restricted to the medial LN, correspondingto the anatomical area of GP. Patients 1 and 3 had bilateral and sym-metrical hyperechogenicity of medial LN and patient 2 exhibited nochanges in the LN. Only patient 2 exhibited increased diameter of thethird ventricle. Other basal gangliawere normal in all subjects. Noneof our patients exhibited SN hyperechogenicity (Table 1; Fig. 1C,D).
In NBIA patients, MRI has consistently revealed T2* hypointen-sity of GP and SN due to iron accumulation [1]. We also observedthese MRI features in our MPAN patients. A main result of our studyis that unlike previously reported PKAN patients, who consistentlyexhibited GP and SN hyperechogenicity, all MPAN patients hadnormal SN echogenicity [4].
Together with these findings, the results of the present studysuggest that TCS might support the discrimination betweendifferent genetic subtypes of NBIA.
Interestingly, in our study MPAN patients with different muta-tions also differed with respect to TCS findings in the GP. MPAN pa-tients 1 and 3, who carried the same heterozygous mutation, bothexhibited hyperechogenicity of GP even though their clinical symp-toms were diverse. In contrast, MPAN patient 2, who had a homo-zygous mutation, exhibited no GP hyperechogenicity.
TCS results differ despite obvious iron accumulation and similarMR features regarding GP and SN hypointensity in T2/T2* indifferent NBIA syndromes. The reason for the difference in TCS re-sults remains unclear; however, it might be explained by the ge-netic and biochemical heterogeneity of NBIA. In concordance

Table 1Demographic and clinical data.
Patient 1 2 3
Age 31 21 18Age of onset 15 12 7Sex F M MFamily history – – –
Consanguinity – – –
Mutation c.[32C > T]þ[204_214del11],p.[Thr11Met]þ[Gly69ArgfsX10]
c.[204_214del11]þ[ ¼ ]p.[Gly69ArgfsX10]þ[ ¼ ]
c.[32C > T]þ[204_214del11],p.[Thr11Met]þ[Gly69ArgfsX10]
Initial symptoms Psychiatric Disturbance of visual acuity,spastic tetraparesis
Gait impairment
Pyramidal signs þþ þþþ –
Dystonia þþ þ –
Parkinsonism þ – –
Dysarthria þþþ – –
Optic atrophy – þþ (Amaurosis) –
Axonal neuropathy þ þ þþþ (Severe muscular atrophy)Psychiatric signs þ – –
TCS echogenicity in cm2
SN (r) 0.2 0.2 0.19SN (l) 0.2 0.2 0.19GP (r) 0.9 – 1.22GP (l) 0.7 – 0.86Third ventricle diameter (mm) 5 9 5.8
GP, globus pallidus; SN, substantia nigra.
Fig. 1. Representative MRI and TCS images from Patient 1. MR T2*-weighted imaging of the substantia nigra (A, blue arrow) and the globus pallidus (B, red arrow). Note the hypo-intense signal due to iron accumulation. Corresponding TCS images depict the substantia nigra in the midbrain (C, blue arrow) and the globus pallidus (D, red arrow). The whitearrow (B, D) highlights the third ventricle. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Letter to the Editor / Parkinsonism and Related Disorders 19 (2013) 1061–10631062

Letter to the Editor / Parkinsonism and Related Disorders 19 (2013) 1061–1063 1063
with our TCS findings, post-mortem analysis in a MPAN patientwith C19orf12 mutation showed widespread iron deposits in theGP but minimal iron deposition in the SN [5]. Different iron com-pounds and binding partners as well as tissue-specific iron deposi-tion may be responsible for different imaging results.
Acknowledgements
None.
References
[1] Schneider SA, Hardy J, Bhatia KP. Syndromes of neurodegeneration with brainiron accumulation (NBIA): an update on clinical presentations, histologicaland genetic underpinnings, and treatment considerations. Mov Disord2012;27:42–53.
[2] Hartig MB, Iuso A, Haack T, Kmiec T, Jurkiewicz E, Heim K, et al. Absence of anorphanmitochondrial protein, c19orf12, causes a distinct clinical subtype of neu-rodegenerationwith brain iron accumulation. Am J HumGenet 2011;89:543–50.
[3] Berg D, Godau J, Walter U. Transcranial sonography in movement disorders.Lancet Neurol 2008;7:1044–55.
[4] Kostic VS, Svetel M, Mijajlovic M, Pavlovic A, Jecmenica-Lukic M, Kozic D. Trans-cranial sonography in pantothenate kinase-associated neurodegeneration.J Neurol 2012;259:959–64.
[5] Hogarth P, Gregory A, Kruer MC, Sanford L, Wagoner W, Natowicz MR, et al.New NBIA subtype: genetic, clinical, pathologic, and radiographic features ofMPAN. Neurology 2013;80:268–75.
Marta Skowronska*2nd Department of Neurology, Institute of Psychiatry and Neurology,
Warsaw, Poland
Uwe WalterDepartment of Neurology, University of Rostock, Rostock, Germany
Tomasz KmiecDepartment of Neurology and Epileptology, The Children’s Memorial
Health Institute, Warsaw, Poland
Anna Czlonkowska2nd Department of Neurology, Institute of Psychiatry and Neurology,
Warsaw, Poland
* Corresponding author.E-mail address: [email protected]
12 March 2013
Recommended