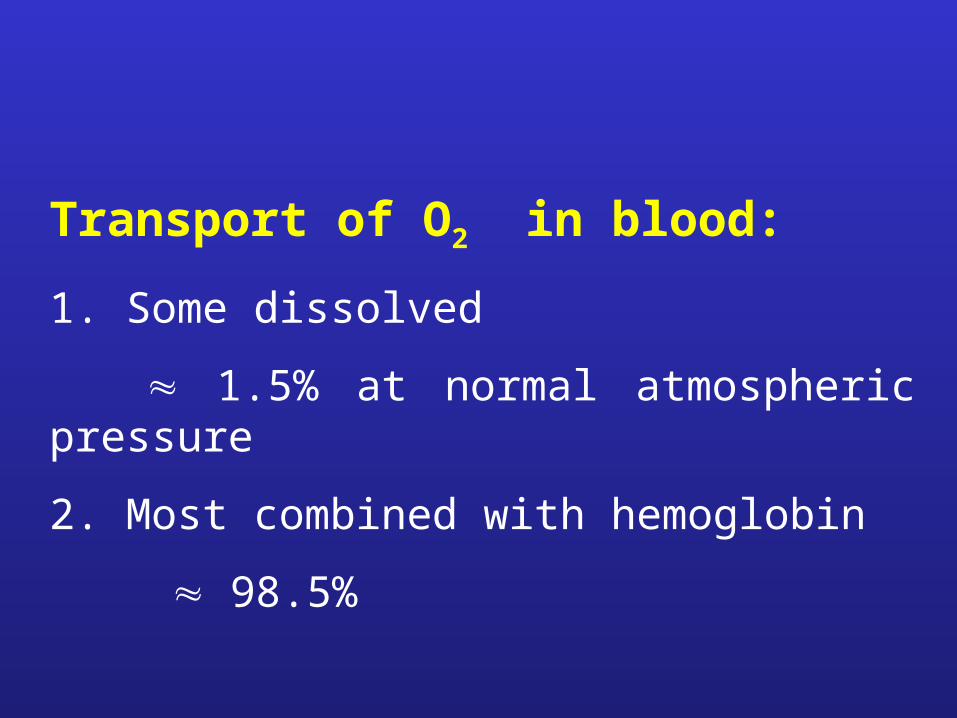
Transport of O2 in blood:
1. Some dissolved
1.5% at normal atmospheric pressure
2. Most combined with hemoglobin
98.5%
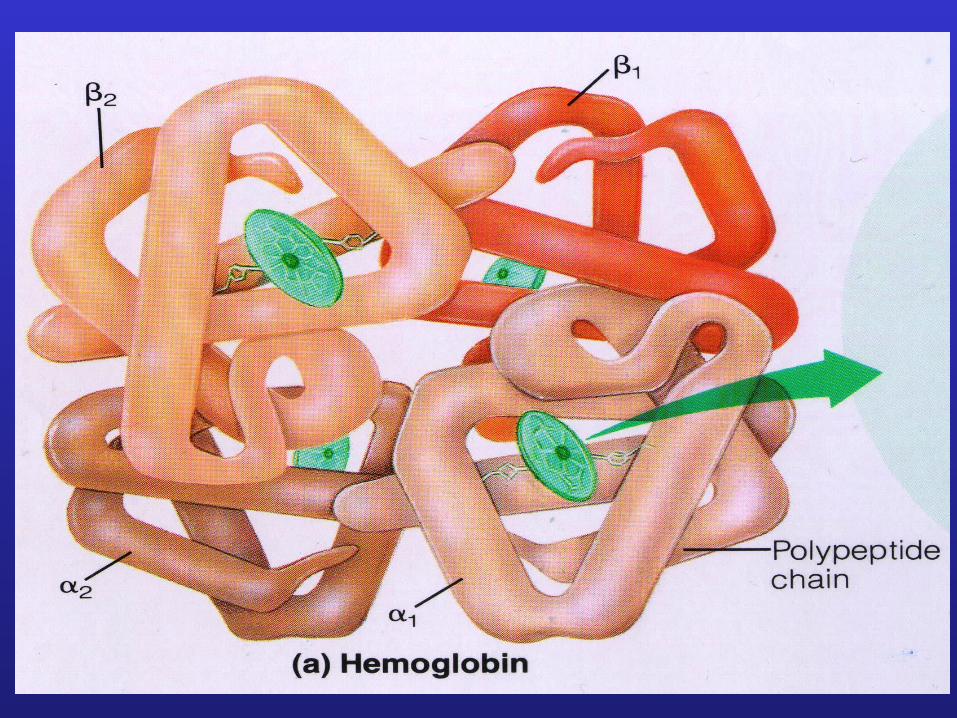
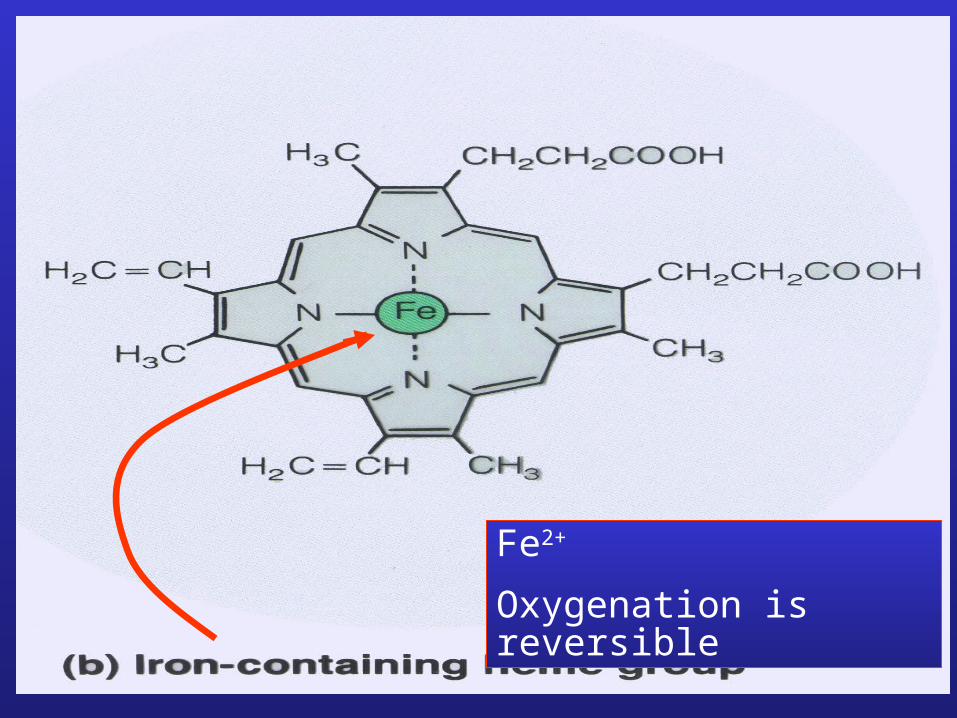
Fe2+
Oxygenation is reversible
ml O
2 /
10
0 m
l blo
od
2
1
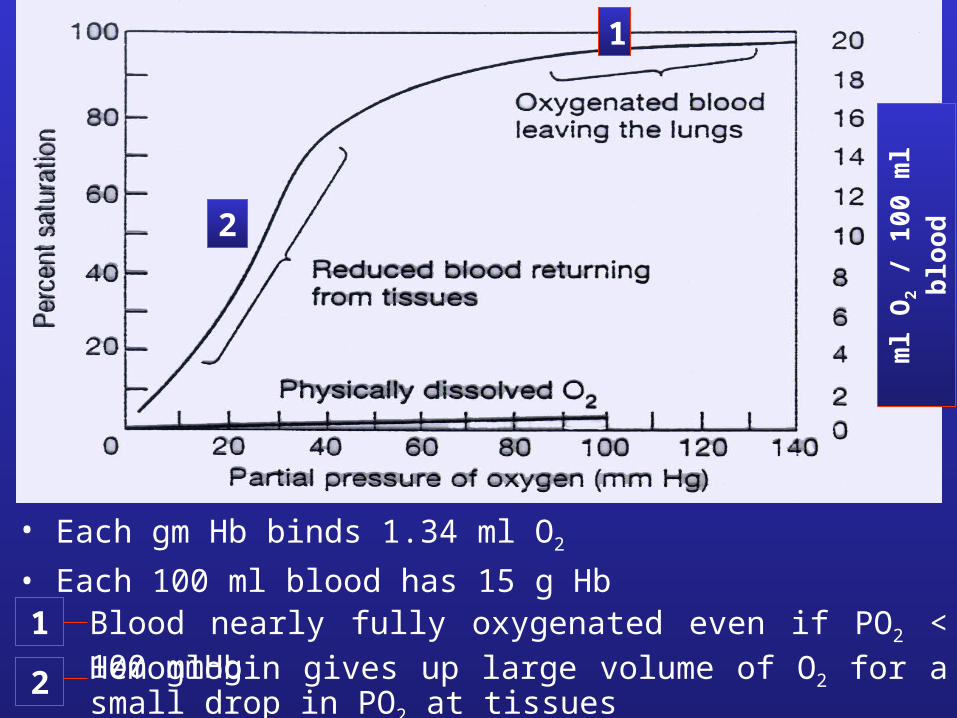
• Each gm Hb binds 1.34 ml O2
• Each 100 ml blood has 15 g Hb1
2
Blood nearly fully oxygenated even if PO2 < 100 mmHg
Hemoglobin gives up large volume of O2 for a small drop in PO2 at tissues
Factors which influence O2 binding to HB
O2 affinity for Hb* is decreased by:
PCO2
pH acidosis
temperature
2,3 diphosphoglycerate
* affinity = shift of O2–Hb curve to right
= easier unloading of O2
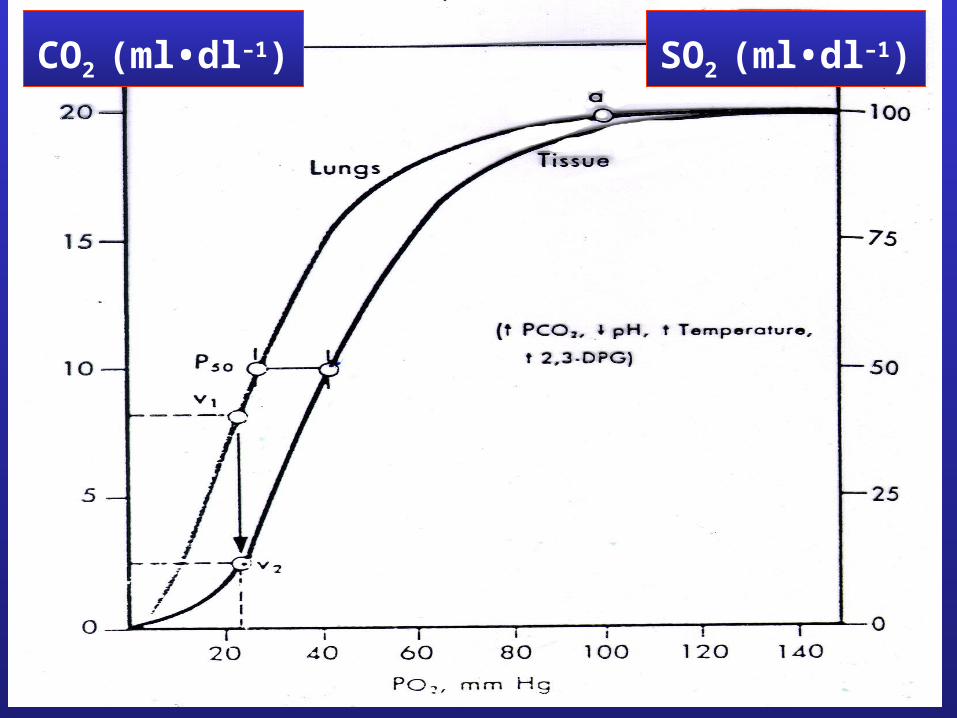
CO2 (ml•dl–1) SO2 (ml•dl–1)
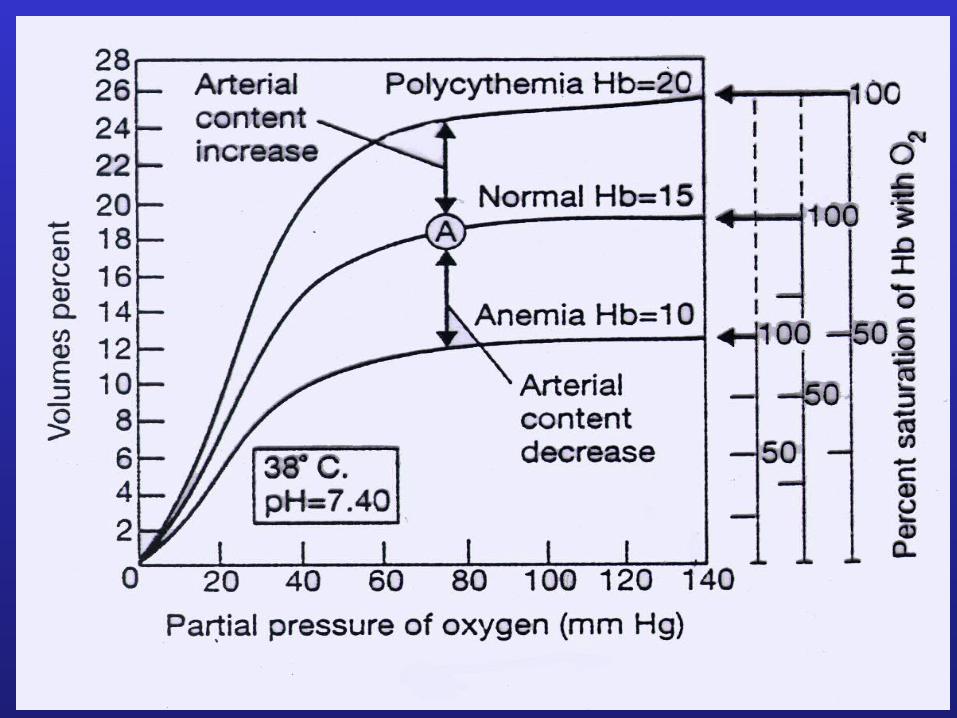
O2 carrying capacity of Hb at a particular
PO2 is decreased by PCO2 (Bohr effect)

Carbon monoxide CO1. Odourless, colourless, non-irritant, no cyanosis
2. Combines with Hb at O2 binding site
3. CO affinity for Hb is 200 times that of O2 for Hb, so if CO at 0.1% in air and O2 at 21%
1/2 Hb—CO and 1/2 Hb—O2
at CO of 0.2% ~ nearly all Hb—CO
4. Management
~ remove from source CO
~ provide Pure O2 ( relative O2 pressure)
~ stimulate ventilation with some CO2
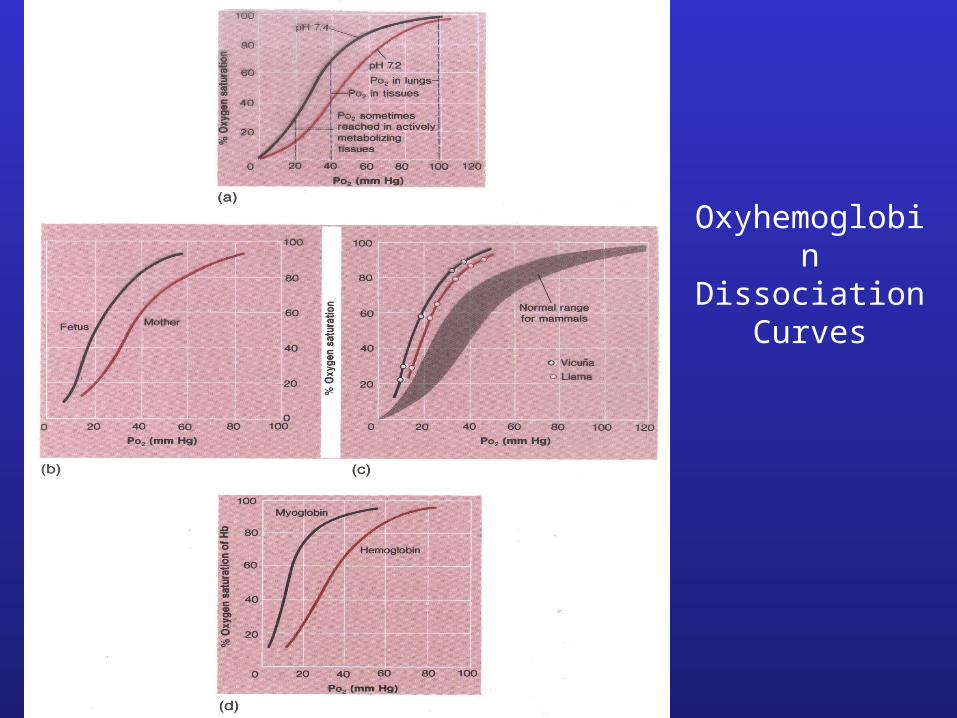
Oxyhemoglobin Dissociation
Curves
In Training:
Vital Capacity Provision of O2
Hb
Cardiac Output
Muscle capillary density
Red blod cell 2,3-DPG
Mitochondria + oxidative enzymes
O2 carrying capacity
Hypoxia: availability of O2 for use by cells
1. availability O2 2. Pulmonary problems:
i) ventilationii) ventilation / perfusion inequalitiesiii) diffusion
3. Venous arterial shunts4. Inadequate transport and delivery
i) anemia; abnormal Hbii) general circulationiii) local circulationiv) edema ( diffusion)
5. Inadequate ability to use O2
i) poisoning cellular enzymes e.g. cyanideii) oxidative enzyme activity e.g. vit B1 deficiency
O2 Transport Summary
• Forms in which O2 is transported in blood
• Hemoglobin
• Hb—O2 dissociation curve
• Factors affecting affinity of Hb for O2
• Carbon Monoxide
• Effects of training
• Causes of hypoxia
Recommended