Type I Diabetes Prevention
Ronen Gurfinkel, PGY5April 3, 2013

Objectives
• Review the pathogenesis of T1DM• Review the prediction of T1DM• Review studies on prevention of T1DM

Pathogenesis of T1DM
• Autoimmune destruction of beta cells• Occurs in susceptible individuals
– Multiple polymorphisms known to influence risk (HLA and others)
• Probable environmental triggers• Multiple autoantigen targets involved
– Insulin, GAD65, IA-2, ZnT8• Progresses over months-years
– Long latent period

• Stages of T1DM– Genetic susceptibility– Triggering of autoimmunity– Appearance of islet cell antibodies– Progressive loss of islet β cells with metabolic
abnormalities– Complete loss of islet β cells and overt
hyperglycemia

Natural History of Type 1 Diabetes
CELLULAR (T CELL) AUTOIMMUNITY
LOSS OF FIRST PHASE INSULIN RESPONSE (IVGTT)
GLUCOSE INTOLERANCE(OGTT)
HUMORAL AUTOANTIBODIES(ICA, IAA, Anti-GAD65, ICA512 Ab, ZnT8A)
ENVIRONMENTALTRIGGER (?)
TIME
BE
TA C
EL
L M
AS
S
DIABETES
“PRE”-DIABETES
GENETICPREDISPOSITION
INSULITISBETA CELL INJURY
CLINICAL ONSET

T1DM Prediction
• Need to identify high risk individuals– Increased efficiency of prevention trials– Interventions likely more effective if administered
early in disease or prediabetic stages

T1DM Prediction
• Genome-wide association study analyses have identified large number of genetic variants associated with T1DM
• MHC HLA molecules are genetic determinants of T1DM– Class II alleles are a major determinant
• DQ and DR molecules
– Class I alleles are also a minor determinant

Human Leukocyte Antigens
• HLA molecules present peptides to T cells• HLA molecules are made of 2 chains
(heterodimers)– Each chain is coded by a separate gene
• HLA molecules are very polymorphic

HLA Molcules
• Class I – 3 major proteins– HLA A, HLA B, and HLA C
• Class II – 3 major proteins– HLA-DP, HLA-DQ, and HLA-DR

HLA Class II
• HLA-DP– α chain: HLA-DPA1– β chain: HLA-DPB1
• HLA-DQ– α chain: HLA-DQA1– β chain: HLA-DQB1
• HLA-DR– α chain: HLA-DRA– β chain: HLA-DRB1, DRB3, DRB4, or DRB5

MHC HLA
• Nomenclature– Usually only polymorphic loci are specified (eg DRB
chain, but not DRA chain)– Each variant designated with gene locus name
followed by *– 2 digits referring to serologic specificity– 2 digits referring to specific allele (DNA-based
typing)
– eg DRB1*0405

MHC HLA
• Groups of HLA alleles are usually inherited together, and referred to as haplotype
• Two MHC haplotypes MHC genotype

Diabetes Risk of Representative DR and DQ HaplotypesDRB1 DQA1 DQB1High Risk0401 or 0403 or 0405 0301 0302 (DQ8)
0301 0501 0201 (DQ2)
Moderate Risk0801 0401 0402
0404 0301 0302
0101 0101 0501
0901 0301 0303
Moderate Protection0403 0301 0302
0701 0201 0201
1101 0501 0301
Strong Protection1501 0102 0602 (DQ2)
1401 0101 0503
0701 0201 0303

HLA and T1DM Risk
• Highest risk with DR3-DQ2 with DR4-DQ8 (DR3/4,DQ8/2)– 1 in 16 will develop T1DM– Children age 10 with T1DM: 50% have this genotype
• 50% of offspring (of T1DM patients) with DQ2/8 will develop T1DM
• 95% of all T1DM have either DR3-DQ2 or DR4-DQ8– This is also present in 40% of general population

Diabetes Autoantibodies
Zheng L and Eisenbarth GS. Prediction and prevention of Type 1 diabetes mellitus. Journal of Diabetes 2011; 3:48-57

Insulin Autoantibodies (IAA)Background: • Detected in new-onset T1D prior to insulin Rx • Insulin the only β-cell specific autoantigen so far • Indistinguishable from antibodies due to exogenous insulin therapy (~ 2 weeks of Rx insulin)New-onset T1D ~ 50 - 70% positive (esp. kids)
Healthy controls < 3% positive

Glutamic Acid Decarboxylase 65 Antibodies (GAD65A)
Background: • 64-kDa protein immunoprecipitated by mixing sera from kids with new-onset T1D with homogenized islets • Subsequently identified as GAD65 (high volume assays using recombinant GAD65)
New-onset T1D ~ 70 - 80% positive
Healthy controls < 3% positive

IA-2 Antibodies (IA-2A/ICA512)
Background: Insulinoma-associated protein 2
• 40-kDa protein• Member of the protein tyrosine phosphatase family• Localized on the insulin granule membrane
New-onset T1D ~ 50 - 75% positive
Healthy controls < 2% positive

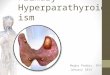
Antibodies and T1DM Prediction
• Risk increases as number of antibodies present increases
• 5-year risk in relatives of T1DM*
– 2 antibodies 68%– 3 antibodies >90%
• Antibodies have varying sensitivity for detecting T1DM– Testing for multiple antibodies will increase
sensitivity*Verge CF et al. Prediction of type I diabetes in first-degree relatives using a combination of insulin, GAD, and ICA512bdc/IA-2 autoantibodies. Diabetes 1996; 45:926-33.

1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Su
rviv
al D
istr
ibu
tio
n F
un
ctio
n
p-value < 0.001(Log Rank Test)n = 26,799
0 1 2 3 4 5 6 7
Years Followed
No. Positive Abs: 1 2 3
8
1718405378147
140129725595
104522919261
74316313040
5571187830
457914922
371663116
Number at Risk
19935148
1234
4
Future T1D Can Reliably Predicted in Persons with a Family History of T1D

Age
FPIR
OGTT
Isletantibodies
< 20 yrs
20 yrs
10th centile
<10th centile
Normal
IGT
1 10 100
Adjusted Hazard Ratio (95% CI)
Independent Predictors of T1D
endit
ICA alone+ 1 Ab+ 2 Ab+ 3 Ab

Prediction of T1DM
• Combination of– Family history (eg first-degree relatives)– Genetic markers (eg HLA class II & I)– Autoantibody markers– Metabolic markers (eg c-peptide, 2h-glucose,
FPIR)

Erlich HA et al. Prediction of Type 1 Diabetes. Diabetes 2013; 62:1020-1021

T1DM Interventions
• Primary intervention– Interval preceding detectability of disease
• Secondary intervention– In presence of disease but asymptomatic and
euglycemic preclinical phase• Tertiary intervention
– Overt diabetes• Quaternary
– Replacement of tissues/organsDupré J and Mahon JL. Preventive Interventions for Type 1 Diabetes: History, Appraisal and Prospects. Can J Diabetes 2007; 31:384-394.

T1DM Tertiary Intervention
• Basis for tertiary intervention– 10-20% of β-cells present at disease onset– Honeymoon phase from improved function of residual
β-cells– “Rescuing” residual β-cells from immune destruction
may improve clinical picture• Effective interventions in animal models (most are
secondary prevention) lead to human trials– Nonobese diabetic (NOD) mouse– Biobreeding (BB) rat

Type 1 Diabetes Prevention in NOD Mice
As of March, 2006
AAV murine IL-10AAV rat preproinsulin gene (vLP-1)Adenovirus expressing mIL-4Aerosol insulinAllogenic thymic macrophagesAlpha GalactosylceramideAlpha-interferon (rIFN-alpha)Alpha/beta T cell receptor thymocytes AminoguanidineAndrogensAnesthesiaAntioxidant MDL 29,311Antisense GAD mRNAAzathioprineAnti-B7-1Bacille Calmette Gue’rin (BCG)BaclofenBee venomBiolistic-mediated IL-4Blocking peptide of MHC class IIBone marrow transplantationCastrationAnti-CD3Anti-CD4CD4+CD25+regulatory T cellsAnti-CD8Anti-CD28 MAbCholera toxin B subunit-insulin proteinClass I derived self-I-A beta(g7) (54-76) peptideCold exposureAnti-complement receptorComplete Freund’s adjuvantAnti-CTLA-4Cyclic nucleotide phosphodiesterases (PDEs)CyclosporinCyclosporin ADC deficient in NF-kappaBDC from pancreatic lymph nodeDC with IL-4DeflazacortDeoxysperogualinDexamethasone/progesterone/growth hormone/estradiolDiazoxide1,25 dihydroxy Vitamin D3, KH10601,25 dihydroxycholecalciferol1,25 dihydroxyl Vitamin D3Elevated temperatureEmotionalityEncephalomyocarditis virus (ECMV)Essential fatty acid deficient dietsFK506FTY720 (myriocin)GAD 65 peptides in uteroAnti-GAD monoclonal antibodyGalactosylceramideGlucose (neonatal)Glutamic acid decarboxylase(intraperitoneal, intrathymic, intravenous, oral)Glutamic acid decarboxylase 65 Th2 cell cloneGlutamic acid decarboxylase peptides(intraperitoneal, intrathymic, intravenous, oral)
GonadectomyGuanidinoethyldisulphideHeat shock protein 65Heat shock protein peptide (p277)Hematopoietic stem cells encoding proinsulinHousing aloneHuman IGF-1I-A beta g7(54-76) peptideAnti-I-A monoclonal antibodiesAnti-ICAM-1IgG2a antibodiesImmobilizationInomideAnti-integrin alpha 4Insulin (intraperitoneal, oral, subcutaneous, nasal)Insulin B chain (plasmid)Insulin B chain/B chain amino acids 9-23 (intraperitoneal, oral, subcutaneous, nasal)Insulin-like growth factor I (IGF-I)Anti-intercellular adhesion molecule-1 (ICAM-1)Interferon-alpha (oral)Interferon-gammaAnti-interferon-gammaInterferon-gamma receptor/IgG1 fusion proteinInterleukin-1Interleukin-4Interleukin-4-Ig fusion proteinInterleukin-4-plasmidInterleukin-10Interleukin-10-plasmid DNAInterleukin-10-viralInterleukin 11-human Interleukin-12Intrathymic administration of mycobacterial heat shock protein 65 Intrathymic administration of mycobacterial heat shock peptide p277Islet cells-intrathymicL-Selectin (MEL-14)Lactate dehydogenase virus (LDH)Large multilamellar liposomeLazaroidAnti-leukocyte function associated antigen (LFA-1)Anti-LFA-1Linomide (quinoline-3-carboxamide)Lipopolysaccharide-activated B cellsLisofyllineLymphocyte choriomeningitis virus (LCMV)Anti-lymphocyte serumLymphoctyte vaccinationLymphocytic choriomeningitis virusAnti-L-selectinLymphotoxinLZ8MC1288 (20-epi-1,25-dihydroxyvitamin D3)MDL 29311Metabolically inactive insulin analogAnti-MHC class IAnti-MHC class IIMHC class II derived cyclic peptideMixed allogeneic chimerismMixed bone marrow chimerasMonosodium glutamateMurine hepatitis virus (MHV)
Mycobacterium aviumMycobacterium lepraeNatural antibodiesNatural polyreactive autoantibodiesNeuropeptide calcitonin gene-related peptideNicotinamideNicotineNinjin-to (Ren-Shen-Tang), a Kampo (Japanese traditional) formulationNKT cellsNY4.2 cellsOK432OvercrowdingPancreatectomyPentoxifyllinePertussigenPoly [I:C]Pregestimil dietPrenatal stressPreproinsulin DNAProbucolProlactinRampamycinRecombinant vaccinia virus expressing GADReg proteinReg proteinRolipramSaline (repeated injection)Schistosoma mansoniSemi-purified diet (e.g., AIN-76)Short term chronic stressSilicaSirolimus/tacrolimusSodium fusidateSoluble interferon-gamma receptorSomatostatinNon-specific pathogen free conditionsStreptococcal enterotoxinsStreptozotocinSulfatide (3’sulfogalactosylceramide)SuperantigensSuperoxide dismutase-desferrioxamineAnti-T cell receptorTGF-beta 1 somatic gene therapyTh1 clone specific for hsp60 peptideAnti-thy-1Thymectomy (neonatal)TolbutamideTolerogenic dendritic cells induced by vitamin D receptor ligandsTop of the rackTreatment combined with a 10% w/v sucrose-supplemented drinking water Tumor necrosis factor-alphaTX527 (19-nor-14,20-bisepi-23-yne-1,25(OH)(2)D(3))Vitamin EAnti-VLA-4

Tertiary Intervention• Insulin• Immunosuppression/Immunomodulation
– Cyclosporin– Azathioprine– GAD65 (GAD65-alum)– Anti-CD3 antibodies– Anti-CD20 antibodies (Rituximab)– Other
• Thymoglobulin• MMF• Sirolimus• BCG vaccine• Heat-shock protein 60-p277 peptide• Anti-CD25 antibody• Lisofylline• IFN-α2a

Insulin for T1DM Tertiary Intervention
• Small studies showed aggressive insulin therapy early in T1DM improved β cell function
• Shah et al, NEJM 1989– 26 patients– Randomized to either
• NPH 1 U/kg given BID• Continuous IV insulin infusion (target BG 3.3-4.4) x 2 weeks
then usual care
– At 1 year, IV insulin group had • Higher C-peptide level post mixed-meal• Better HbA1c (7.2% vs 10.8%)
Shah et al, A Randomized Trial of Intensive Insulin Therapy in Newly Diagnosed Insulin-Dependent Diabetes Mellitus. N Engl J Med 1989; 320:550-554.

Insulin for T1DM Tertiary Intervention
• DCCT, Ann Int Med 1998– 855 (of 1441) T1DM 1-5 years at baseline– 303/855 were “C-peptide responders”– Randomized to intensive vs conventional treatment– Responders in intensive therapy group
• Maintained higher stimulated C-peptide levels• Less likely to become “nonresponders”
– Among intensive treatment in entire DCCT cohort responders had
• Lower HbA1c• Lower rates of retinopathy• Lower risk of severe hypoglycemia
DCCT Research Group. Effect of intensive therapy on residual beta-cell function in patients with type 1 diabetes in the diabetes control and complications trial. A randomized, controlled trial. Ann Intern Med. 1998 Apr 1;128(7):517-23.

Cyclosporin for T1DM Tertiary Intervention
• Cyclosporin A prevented T1DM in rodents• Human pilot studies showed partial remission• Enhanced β cell function in 2 RCTs
– CERT– CCF Study Group Diabetes

Canadian-European Randomized Control Trial Group
• CERT Group, Diabetes 1988– Recent T1DM (< 6 weeks)– 188 participants, age 9-35– Randomized to cyclosporin or placebo
• Cyclosporin 10 mg/kg/day given q12h• Titrated based on trough levels
– Double-blinding for diabetes management• Unblinded management of cyclosporin
– Target BGs ≤ 7.8 mM (ac meals and hs)• Insulin doses minimized
– Stimulated C-peptide at 3-month intervals– Remission defined as:
• Stim CP ≥ 0.6 mM• Non-insulin receiving (NIR) state
CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.

Canadian-European Randomized Control Trial Group
CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.

Canadian-European Randomized Control Trial Group
CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes 1988;37:1574-82.

Cyclosporin/Diabetes French Study Group
• CCF Study Group Diabetes, Lancet 1986– Recent onset T1DM– 122 participants, age 15-40– Randomized to cylcosporin or placebo
• Cyclosporin 7.5 mg/kg/d
– At 6 months• Complete remission 25.4% of cyclosporin group vs. 18.6% of placebo
group
– Treatment continued for partial/complete remission (n=106)– At 9 months
• Complete remission 24.1% of cyclosporin group vs. 5.8% of placebo group
CCF Study Group Diabetes. Cyclosporin Increases the Rate and Length of Remissions in Insulin-dependent Diabetes of Recent Onset: Results of a Multicentre Double-blind Trial. Lancet 1986;328:119-124

Azathioprine for T1DM Tertiary Intervention
• Mixed results in newly diagnosed T1DM– Harrison LC et al, Diabetes 1985
• 24 patients, age 15-50• Azathioprine 2 mg/kg showed benefit on basal and stim
CP levels
– Cook JJ et al, Diabetes 1989• 49 patients, age 2-20• Azathioprine 2 mg/kg did not give significant difference
in remission rates, CP levels
Harrison LC, Colman PG, Dean B, et al. Increase in remission rate in newly diagnosed type 1 diabetic subjects treated with azathioprine. Diabetes 1985;34:1306–1308.Cook JJ, Hudson I, Harrison LC, et al. A double-blind controlled trial of azathioprine in children with newly-diagnosed type 1 diabetes. Diabetes 1989;38:779–783.

Azathioprine for T1DM Tertiary Intervention
• Silverstein, NEJM 1988– Newly diagnosed T1DM (< 2 weeks)– 46 patients, age 4-32– Randomized to azathioprine/prednisone or placebo
• Prednisone x 10 weeks + azathioprine x 1 year
– Unblinded study– “Satisfactory” outcome
• HbA1c < 6.8%, stim CP > 0.5 mM, insulin dose < 0.4 U/kg/d
Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.

Azathioprine for T1DM Tertiary Intervention
Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.

Azathioprine for T1DM Tertiary Intervention
• Silverstein, NEJM 1988– “Satisfactory” outcome
• HbA1c < 6.8%, stim CP > 0.5 mM, insulin dose < 0.4 U/kg/d
– At 1 year• Satisfactory outcome in 50% of immunosuppressed
group vs. 15% of placebo group
Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.

Anti-CD3 Ab for T1DM Tertiary Intervention
• Targets CD3 receptors on T cells• Beneficial effects possibly by activation of regulatory T
cells– ? selective deletion of activated Th1 cells and/or activation of
Th2 cells and their protective cytokines• OKT3 reversed diabetes in nonobese diabetic (NOD)
mice– Cytokine mediated side-effects
• Humanized monoclonal antibodies developed– Teplizumab– Otelixizumab

Teplizumab [hOKT3γ1(Ala-Ala)]
• Herold et al, NEJM 2002– T1DM < 6 weeks– 24 patients, age 7-30– Randomized to teplizumab or placebo
• Teplizumab single 14-day course
Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.

Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.

Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.

Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.

Teplizumab [hOKT3γ1(Ala-Ala)]
• Herold et al, NEJM 2002– At 1 year
• Improved insulin production in 9/12 in teplizumab group vs. 2/12 in placebo group
• Lower HbA1c and insulin doses in teplizumab group
Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.


Teplizumab (Protégé study)
• Sherry N et al, Lancet 2011 – T1DM ≤ 12 weeks– 516 patients, age 8-35– Randomized 2:1:1:1 ratio, double-blind
• Teplizumab 14-day full dose, 14-day low dose, 6-day full dose, or placebo
– Primary outcome: % patients at 1 year with both• Insulin dose < 0.5 U/kg/d• HbA1c < 6.5%
Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.

Teplizumab (Protégé study)
Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.

Teplizumab (Protégé study)
• Subgroup analysis– Reduction in median AUC of CP was lower in
treatment subgroups• Age 8-11• Randomized < 6 weeks after diagnosis
Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.

Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.

Otelixizumab (ChAglyCD3)
• Keymeulen et al, NEJM 2005– T1DM < 4 weeks– 80 patients, age 12-39– Randomized to Otelixizumab or placebo
• Otelixizumab single 6-day course
Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608

Otelixizumab (ChAglyCD3)
Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608

Otelixizumab (ChAglyCD3)
• Keymeulen et al, NEJM 2005– At 6, 12, and 18 months
• β-cell function better preserved in otelixizumab group• Lower insulin requirements in otelixizumab group
– 0.15 U/kg/d difference
• Higher stim CP levels in otelixizumab group
Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608

Otelixizumab (ChAglyCD3)
• Keymeulen et al, Diabetologia 2010– 4 year follow-up on 64/80 patients
Keymeulen et al. Four-year metabolic outcome of a randomised controlled CD3-antibody trial in recent-onset type 1 diabetic patients depends on their age and baseline residual beta cell mass. Diabetologia 2010; 53:614-623.

Keymeulen et al. Four-year metabolic outcome of a randomised controlled CD3-antibody trial in recent-onset type 1 diabetic patients depends on their age and baseline residual beta cell mass. Diabetologia 2010; 53:614-623.

Otelixizumab (ChAglyCD3)
• Keymeulen et al, NEJM 2005– At 6, 12, and 18 months
• β-cell function better preserved in otelixizumab group• Lower insulin requirements in otelixizumab group
– 0.15 U/kg/d difference
• Higher stim CP levels in otelixizumab group
Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608

Otelixizumab (ChAglyCD3)
• DEFEND-1 Study (Phase III)– 272 patients, age 12-45, T1DM < 3 months
• Followed 2008-2010• Study completed Jan 2012
– Randomized, double-blind, placebo controlled– Randomization in 2:1 ratio– Low dose of otelixizumab used– Results: not published
• News release Mar 2011 did not meet primary efficacy endpoint (change in C-peptide)
• DEFEND-2 Study Stopped?http://clinicaltrials.gov/ct2/show/NCT00678886http://clinicaltrials.gov/ct2/show/NCT01123083

Rituximab
• Pescovitz et al, NEJM 2009– Recent onset T1DM (< 3 months)– 87 patients, age 8-40, peak stim CP > 0.2 pmol/mL– 2:1 randomization to rituximab or placebo
• Rituximab 375 mg/m2 IV weekly x4
Pescovitz et al (T1D TrialNet Anti-CD20 Study Group). Rituximab, B-lymphocyte depletion, and preservation of beta-cell function. N Engl J Med 2009; 361:2143-52.

Pescovitz et al (T1D TrialNet Anti-CD20 Study Group). Rituximab, B-lymphocyte depletion, and preservation of beta-cell function. N Engl J Med 2009; 361:2143-52.

Rituximab
• Pescovitz et al, NEJM 2009– At 1 year, rituximab group had
• Higher mean AUC for CP (0.56 vs. 0.47 pmol/mL)• Lower HbA1c (6.76 vs. 7.00%)• Lower insulin requirements (0.39 vs. 0.48 U/kg/d)
Pescovitz et al (T1D TrialNet Anti-CD20 Study Group). Rituximab, B-lymphocyte depletion, and preservation of beta-cell function. N Engl J Med 2009; 361:2143-52.

Secondary Prevention
• Insulin• Nicotinamide• Others

Insulin for Secondary Prevention
• Insulin shown to have protective effect in animal models– Oral administration has no metabolic effect– Interaction with gut lymphoid tissue induces
immune tolerance

Insulin Pilot Studies
• Keller et al, Lancet 1993– 12 FDRs with ICA– 5 received insulin (IV & sc)– After 4 years, T1D developed in 1/5 treated vs. 7/7 controls
• Schwabing Insulin Prophylaxis Pilot Trial, Diabetologia, 1998– 14 FDRs with ICA– Randomized to IV+sc insulin or placebo– After 7 years, T1D developed in 3/7 treated vs. 6/7 controls– T1D delayed in treated group (5 vs. 2.3 years)
Keller RJ et al. Insulin prophylaxis in individuals at high risk of type 1 diabetes. Lancet. 1993; 341:927-928.Füchtenbusch M et al. Delay of type I diabetes in high risk, first degree relatives by parenteral antigen administration: the Schwabing Insulin Prophylaxis Pilot Trial. Diabetologia 1998; 41:536-41.

Diabetes Prevention Trial Type 1
• Conducted in 2 groups– High risk IV insulin vs placebo– Intermediate risk oral insulin vs placebo
The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.Skyler JS et al. Effects of oral insulin in relatives of patients with type 1 diabetes. The Diabetes Prevention Trial — Type 1. Diabetes Care. 2005;28:1068-1076.


Diabetes Prevention Trial Type 1• DPT-1 – IV insulin (NEJM 2002)
– Randomized, controlled, nonblinded– Screening of FDRs & SDRs (84,228) with genetic, immunologic, metabolic
markers– Included patient with 5-year risk > 50%
• ICA > 10 JDF units• Impaired first phase insulin response
– <10%ile for siblings, offspring, and SDRs– <1%ile for parents
• Abnormal 75g OGTT• Absence of HLA-DQA1*0102,DQB1*0602 (protective)
– 339 patients, age 3-45 (median age 11.2)– Randomized to insulin or observation
• Ultralente insulin 0.25 U/kg/d (given BID)• IV insulin infusion x 4 days yearly
– Primary endpoint: Diagnosis of diabetes
The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.

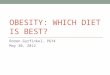
DPT-1 Parenteral Insulin Trial1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
169170
144131
96101
6969
3940
1314 1
Number at Risk
Su
rviv
al D
istr
ibu
tio
n F
un
ctio
n
P- Value= 0.796(Log Rank Test)
InterventionObservation
0 1 2 3 4 5 6 7
Years Followed
STRATA: Intervention Observation
Control
Treated
DPT-1 Study Group. NEJM 2002

Diabetes Prevention Trial Type 1
• After median 3.7 years of follow-up– No difference between 2 groups– Incidence of diabetes close to predicted– No difference in C-peptide levels– No difference in subgroup analyses
The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.

Diabetes Prevention Trial Type 1
• Conclusion:– This insulin regimen in this high-risk group did not
prevent T1DM
• Weakness:– Insulin dose (based on pilot studies) chosen to
avoid hypoglycemia
The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.


Diabetes Prevention Trial Type 1
• DPT-1 – Oral insulin (Diabetes Care 2005)– Randomized, controlled, double-blind– Screening of FDRs & SDRs (103,391) with genetic, immunologic,
metabolic markers– Included patient with 5-year risk 25-50%
• ICA > 10 JDF units• Impaired first phase insulin response
– >10%ile for siblings, offspring, and SDRs– >1%ile for parents
• Abnormal 75g OGTT• Absence of HLA-DQA1*0102,DQB1*0602 (protective)
– 372 patients, age 3-45 (median age 10.25)– Randomized to oral insulin or placebo
• Insulin 7.5 mg po daily
Skyler JS et al. Effects of oral insulin in relatives of patients with type 1 diabetes. The Diabetes Prevention Trial — Type 1. Diabetes Care. 2005;28:1068-1076.

DPT-1 Oral Insulin Study
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Su
rviv
al D
istr
ibu
tio
n F
un
ctio
n
0 1 2 3 4 5 6 7
Years Followed
186186
174170
146137
110102
8571
4037
2312
Number at Risk
P- Value= 0.176(Log Rank Test)
Oral InsulinOral Placebo
STRATA: Oral Insulin Oral Placebo
Control
Treated
DPT-1 Study Group. Diabetes Care 2005

Diabetes Prevention Trial Type 1
• After median 4.3 years– Similar annualized diabetes rates (6.4% vs. 8.2%,
HR 0.764, p=0.189)– Overall diabetes incidence similar in both groups
and close to predicted rates (23% vs 28%)– Secondary analysis showed benefit in subgroup
with high IAA titres• Annualized rates of 6.2% vs 10.4% (HR 0.566, p=0.015)
Skyler JS et al. Effects of oral insulin in relatives of patients with type 1 diabetes. The Diabetes Prevention Trial — Type 1. Diabetes Care. 2005;28:1068-1076.

Diabetes Prevention Trial Type 1
• Conclusion:– Oral insulin did not prevent or prevent T1DM in
this intermediate-risk group– Further study needed to explore role in those with
high IAA titres
• Weakness:– Oral insulin dose chosen arbitrarily (no dose-
finding studies available)
The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.

Nicotinamide for T1DM Secondary Intervention
• Nicotinamide showed benefit in animal models– Toxin-induced diabetes models– Spontaneous type 1 diabetes models
• Possible mechanisms– Free radical scavenger– Replenishing nicotinamide adenine dinucleotide (an essential
coenzyme) within damaged cells, thereby promoting DNA repair and limiting DNA damage
• Benefit in tertiary intervention (1996 meta-analysis of ~200 patients in 10 trials)
• Benefit in secondary intervention in small study of schoolchildren in New Zealand (Diabetologia 1991)

European Nicotinamide Diabetes Intervention Trial (ENDIT)
• Randomized, controlled, double-blind• Recruitment from 18 European countries, US, and
Canada• Screened FDRs (~30,000)• Included those with ICA > 20 JDF units and non-
diabetic OGTT• 552 patients, age 3-40 (median age 17)• Randomized to nicotinamide or placebo for 5 years
– Nicotinamide MR 1.2 g/m2 po daily• Primary outcome: development of diabetes
Gale EA et al. ENDIT Group. Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1 diabetes. Lancet. 2004;363:925-931 endit

Per
cen
tag
e d
evel
op
ing
dia
bet
es
Years since randomisation0 1 2 3 4 5
0
10
20
30
40
50
Placebo1
Niatrim
PlaceboNiatrim
275274
245260
232232
205208
184171
115107
European-Canadian Nicotinamide Trial
P-value = 0.97
ENDIT Study Group. Lancet 2004.endit

European Nicotinamide Diabetes Intervention Trial (ENDIT)
• After median follow-up of 4.7 years– Risk of developing diabetes similar in both groups
(30 vs. 28%, HR 1.07, p=0.69)– Similar results after adjusting for age, OGTT
results, antibody status, FPIR results
Gale EA et al. ENDIT Group. Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1 diabetes. Lancet. 2004;363:925-931 endit

European Nicotinamide Diabetes Intervention Trial (ENDIT)
• Conclusion– Nicotinamide (at this dose) was ineffective to
prevent T1DM
• Weakness– Lower dose used in humans than animal studies– Given at later stage of disease in humans
Gale EA et al. ENDIT Group. Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1 diabetes. Lancet. 2004;363:925-931 endit

Primary Intervention
• Genetic factors do not completely predict T1DM• Environmental factors implicated in T1DM
– Infectious– Toxins– Nutritional
• Nutritional factors studied in primary intervention trials– Vitamin D– Allogenic nutrient proteins

Vitamin D in Primary Intervention
• EURODIAB substudy, Diabetologia 1999– Case control study in 7 European countries– Vitamin D in early infancy was protective
• Hyppönen et al, Lancet 2001– Birth-cohort study in Finland– >10,000 infants, born 1966, followed x30 years– Vit D > 2000 IU/d associated with reduced T1DM
risk (RR 0.22)

Vitamin D in Primary Intervention
• Winnipeg DVD Study Group, Ann NY Acad Sci 2006– Feasibility study– Infants with high risk HLA genes
• Heterozygous for DRB1*03, DQA1*0501, DQB1*0201 / DRB1*04, DQA1*03011, DQB1*0302 (DRB1*04 ≠ *0403 or related alleles)
• Homozygous for DRB1*03, DQA1*0501, DQB1*0201• Homozygous for DRB1*04, DQA1*03011, DQB1*0302 (DRB1*04 ≠ *0403
or related alleles)
– Randomized to Vit 2,000 or 400 IU daily– Larger study planned? ($10 million proposal submitted
in 2012)
Wicklow BA, Taback S. Feasibility of a type1 diabetes primary prevention trial using 2000 IU Vitamin D3 in infants from the general population with increased HLA-associated risk. Ann NY Acad Sci. 2006;1079:310-312.

Cow’s Milk and T1DM
• No T1DM in Western Samoa prior to introduction of cow-milk formula in 1970s
• Association between worldwide decrease in breastfeeding and increase in T1DM incidence
• T1DM incidence in Puerto Rico is 26x higher than in Mexico– Incidence increased as cow-milk formula use increased
• Rat studies showed– >70% T1DM with standard cow-milk-based chow– Complete prevention of T1DM by hydrolysis of feed
• Meta-analysis (Diabetes Care 1994)– T1DM more likely to be breast-fed < 3 months– More likely to be exposed to cow’s milk before 4 months

Trial to Reduce Insulin-Dependent Diabetes in the Genetically at Risk - TRIGR Study
• Pilot study, Diabetologia 2005– 242 newborn FDRs with high-risk HLA-DQB1 alleles– Breastfeeding encouraged– Randomized to either casein hydrolysate or
conventional cow’s milk formula until age 6-8 months
– Primary outcome: development of antibodies– After a mean of 4.7 years, casein hydrolysate group
had significantly lower rate of ICA
Akerblom HK et al; National TRIGR Study Groups. Dietary manipulation of beta cell autoimmunity in infants at increased risk of type 1 diabetes: a pilot study. Diabetologia. 2005;48:829-837.


Trial to Reduce Insulin-Dependent Diabetes in the Genetically at Risk - TRIGR Study
• Knip et al, NEJM 2010– Follow-up of pilot study to age 10– Outcomes
• Rates of beta-cell autoimmunity– Insulin, GAD, IA2, and ZnT8 antibodies– ICA
• Rates of progression to diabetes (not primary endpoint)
– Autoantibody samples available on 208 children, mean follow-up 7.5 years
Knip M et al. Finnish TRIGR Study Group. Dietary intervention in infancy and later signs of beta-cell autoimmunity. N Engl J Med 2010; 363:1900-8.

Knip M et al. Finnish TRIGR Study Group. Dietary intervention in infancy and later signs of beta-cell autoimmunity. N Engl J Med 2010; 363:1900-8.

Trial to Reduce Insulin-Dependent Diabetes in the Genetically at Risk - TRIGR Study
• Results– Adjusted HR for 1+ autoantibodies 0.51 in casein vs. control
group (95% CI 0.28-0.91)• 17 vs 33 children
– Adjusted HR for 2+ autoantibodies 0.47 in casein vs control group (95% CI 0.19-1.07)
– Rate of T1DM similar (6 vs. 8%)
• Larger multicentre, international study is ongoing– 2,159 children in 15 countries recruited– Results ~2017
Knip M et al. Finnish TRIGR Study Group. Dietary intervention in infancy and later signs of beta-cell autoimmunity. N Engl J Med 2010; 363:1900-8.

Staeva TP et al. Recent Lessons Learned From Prevention and Recent- Onset Type 1 Diabetes Immunotherapy Trials. Diabetes 2013; 62:9-17.

Staeva TP et al. Recent Lessons Learned From Prevention and Recent- Onset Type 1 Diabetes Immunotherapy Trials. Diabetes 2013; 62:9-17.

Future of T1DM Prevention
Staeva TP et al. Recent Lessons Learned From Prevention and Recent- Onset Type 1 Diabetes Immunotherapy Trials. Diabetes 2013; 62:9-17.

Summary
• Prediction of T1DM is possible• Studies on prevention are important and
feasible• To date, no effective prevention

References• Eisenbarth GS. Prevention of Type 1A Diabetes. Endocr Pract 2012; 18:745-749• Zheng L and Eisenbarth GS. Prediction and prevention of Type 1 diabetes mellitus. Journal of Diabetes 2011; 3:48-57• Verge CF et al. Prediction of type I diabetes in first-degree relatives using a combination of insulin, GAD, and ICA512bdc/IA-2 autoantibodies. Diabetes 1996; 45:926-33.• Erlich HA et al. Prediction of Type 1 Diabetes. Diabetes 2013; 62:1020-1021• Dupré J and Mahon JL. Preventive Interventions for Type 1 Diabetes: History, Appraisal and Prospects. Can J Diabetes 2007; 31:384-394.• Shah et al, A Randomized Trial of Intensive Insulin Therapy in Newly Diagnosed Insulin-Dependent Diabetes Mellitus. N Engl J Med 1989; 320:550-554.• DCCT Research Group. Effect of intensive therapy on residual beta-cell function in patients with type 1 diabetes in the diabetes control and complications trial. A randomized,
controlled trial. Ann Intern Med. 1998 Apr 1;128(7):517-23.• CERT Group. Cyclosporin-lnduced Remission of IDDM After Early Intervention Association of 1 yr of Cyclosporin Treatment With Enhanced Insulin Secretion. Diabetes
1988;37:1574-82.• CCF Study Group Diabetes. Cyclosporin Increases the Rate and Length of Remissions in Insulin-dependent Diabetes of Recent Onset: Results of a Multicentre Double-blind Trial.
Lancet 1986;328:119-124.• Harrison LC, Colman PG, Dean B, et al. Increase in remission rate in newly diagnosed type 1 diabetic subjects treated with azathioprine. Diabetes 1985;34:1306–1308.• Cook JJ, Hudson I, Harrison LC, et al. A double-blind controlled trial of azathioprine in children with newly-diagnosed type 1 diabetes. Diabetes 1989;38:779–783.• Silverstein et al. Immunosuppression with Azathioprine and Prednisone in Recent-Onset Insulin-Dependent Diabetes Mellitus. N Engl J Med 1988; 319:599-604.• Herold et al. Anti-CD3 Monoclonal Antibody in New-Onset Type 1 Diabetes Mellitus. N Engl J Med 2002; 346:1692-1698.• Sherry N et al. Teplizumab for treatment of type 1 diabetes (Protégé study): 1-year results from a randomised, placebo-controlled trial. Lancet 2011; 378:487-97.• Keymeulen et al. Insulin Needs after CD3-Antibody Therapy in New-Onset Type 1 Diabetes. N Engl J Med 2005; 352:2598-608• Keymeulen et al. Four-year metabolic outcome of a randomised controlled CD3-antibody trial in recent-onset type 1 diabetic patients depends on their age and baseline residual
beta cell mass. Diabetologia 2010; 53:614-623.• http://clinicaltrials.gov/ct2/show/NCT00678886• http://clinicaltrials.gov/ct2/show/NCT01123083• Pescovitz et al (T1D TrialNet Anti-CD20 Study Group). Rituximab, B-lymphocyte depletion, and preservation of beta-cell function. N Engl J Med 2009; 361:2143-52.• Keller RJ et al. Insulin prophylaxis in individuals at high risk of type 1 diabetes. Lancet. 1993; 341:927-928.• Füchtenbusch M et al. Delay of type I diabetes in high risk, first degree relatives by parenteral antigen administration: the Schwabing Insulin Prophylaxis Pilot Trial. Diabetologia
1998; 41:536-41.• The Diabetes Prevention Trial — Type 1 Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685-1691.• Skyler JS et al. Effects of oral insulin in relatives of patients with type 1 diabetes. The Diabetes Prevention Trial — Type 1. Diabetes Care. 2005;28:1068-1076.• Gale EA et al. ENDIT Group. Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1 diabetes. Lancet.
2004;363:925-931• Wicklow BA, Taback S. Feasibility of a type1 diabetes primary prevention trial using 2000 IU Vitamin D3 in infants from the general population with increased HLA-associated risk.
Ann NY Acad Sci. 2006;1079:310-312.• Akerblom HK et al; National TRIGR Study Groups. Dietary manipulation of beta cell autoimmunity in infants at increased risk of type 1 diabetes: a pilot study. Diabetologia.
2005;48:829-837. • Knip M et al. Finnish TRIGR Study Group. Dietary intervention in infancy and later signs of beta-cell autoimmunity. N Engl J Med 2010; 363:1900-8.• Staeva TP et al. Recent Lessons Learned From Prevention and Recent- Onset Type 1 Diabetes Immunotherapy Trials. Diabetes 2013; 62:9-17.

Questions?
Recommended