Undersanding the EarLawrence M. Simon, M.D.
Department of Pediatrics Noon Lecture SeriesLouisiana State University Health Sciences Center
Children’s Hospital of New OrleansSeptember 17, 2010

Anatomy of the ear

External Ear Middle Ear Inner Ear• Cerumen impaction• Auricular hematoma• Perichondritis• Otiis Externa• Otomycosis• Foreign Body•External ear canal laceration -temporal bone fracture
• Acute otitis media• Serous otitis media• Chornic otitis media• Hemotympanum•Tympanic membrane perforation• Cholesteatoma• Mastoiditis
• Vestibular neuritis• Meniere’s Disease• Vestibular
migraine
Differential Diagnosis of Ear Disease

External Ear

The auricle and EAC
• Cartilaginous structure designed to funnel sound to TM
• Embryology: first branchial arch (Hillocks of His)
• Very poor vascular supply
• EAC: 2/3 cartilaginous (poor innervation) and 1/3 bony (very sensitive)
• Protected by cerumen and very delicate ecosystem
• Very sensitive to water

Cerumen impaction
• Not always pathologic
• 2 “flavors”1. Thin sheet of cerumen occluding EAC
− Often resolves with drops
2. Thick plug blocking entire EAC− Requires debridement under microscope

Cerumen impaction

Cerumen impaction
• Not always pathologic
• 2 “flavors”1. Thin sheet of cerumen occluding EAC
− Often resolves with drops
2. Thick plug blocking entire EAC− Requires debridement under microscope
• Avoid irrigation
• Use maintenance drops weekly once clear
• Refer to ENT if any concerns

Auricular hematoma
• Hematoma between perichondrium and auricular cartilage
• Precipitated by trauma (wrestling)
• May result in loss of cartilage
• Treatment:
• Immediate drainage and pressure dressing
• Topical antimicrobial
• Oral anti-staphylococcal antibiotic
• Close follow-up (~48 hours)


Perichondritis
• Bacterial infection of perichondrium of auricle
• Usually precipitated by trauma
• May result in loss of cartilage
• Most common pathogen: Pseudomonas
• Treatment:
• Admission
• topical antimicrobials
• iv anti-pseudomonal antibiotics (convert to po with improvement)
• Drain any associated abscess/fluid collection

Perichondritis

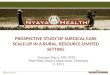
Otitis Externa
• Bacterial overgrowth in external auditory canal
• Prevented by cerumen
• Most common pathogen: Pseudomonas
• Common causes: water exposure, picking/ tramua (q-tips)
• Exam: • Purulent debris in EAC, possible granulation
• Edema of EAC (may be completely closed off)
• Normal auricle
• Pain with movement of auricle (different than perichondritis and otitis media)
Otitis Externa

Otitis Externa- treatment
• Aural toilet
• Dry ear precautions
• Topical antimicrobials
• May need ear wick• Special sponge placed in EAC to facilitate
administration of drops
• Place under microscope
• Remove at 3-5 days
• Floxin-HC
• Cortisporin (topical dermatitis)
• Floxin
• Ciprodex

Otitis Externa- treatment
• IV antibiotics only for severe complications
• “Malignant otitis externa”
• May have associated perichondritis
• Chronic OE can result in scar/stenosis of EAC
• “Keratosis Obturans”
Otomycosis
• Fungal overgrowth of EAC skin
• Prevented by cerumen
• Usually associated with prolonged topical antibiotic use
• Also seen after radical mastoidectomy and with hearing aid use
• Treatment: topical antimicrobials
• Aural toilet
• Dry ear precautions
• Topical anti-funal (Acetic acid, clotrimazole, ketoconazole)

Otomycosis

Foreign body

Ear Foreign Body
• Unless battery, can be removed in clinic the next day
• Ciprodex if pain/purulent otorrhea
• Treatment:
– Removal in office OK if isolated to cartilaginous EAC (lateral, immediately at opening)
– Removal in OR if in medial/bony EAC or touching TM

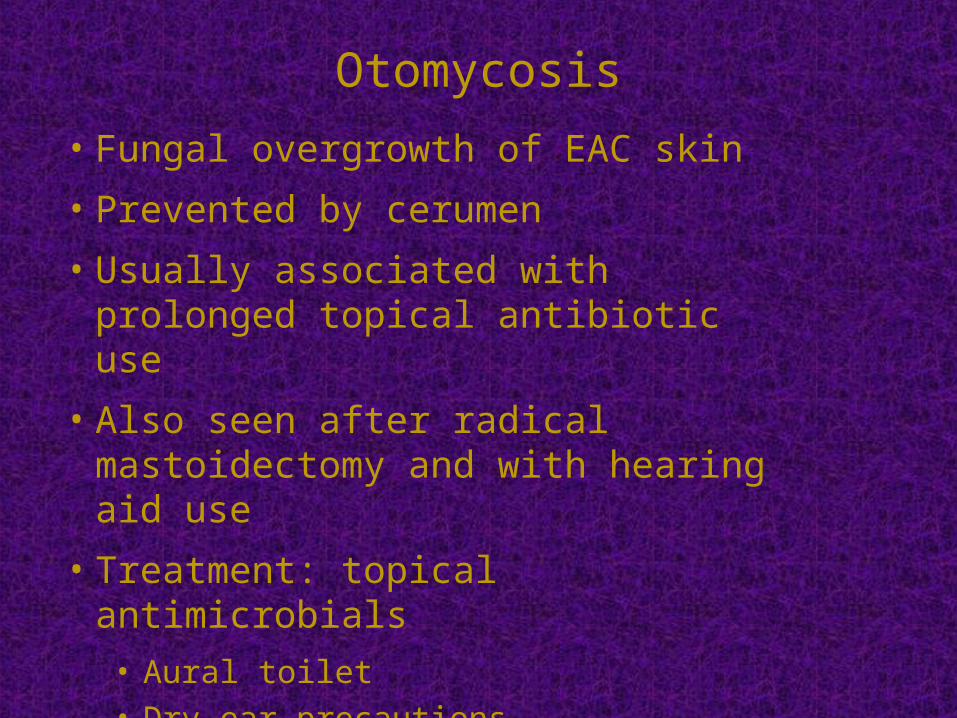
Special foreign body cases
• Button Battery: – Remove immediately
• Bean: – Will swell with water and frequently fragments
• Insect in ear:– Kill insect with lidocaine, ointment
– Typically remove with suction and microscope

Special foreign body cases

Special foreign body cases
• Button Battery: – Remove immediately
• Bean: – Will swell with water and frequently fragments
• Insect in ear:– Kill insect with lidocaine, ointment
– Typically remove with suction and microscope
• Q-tip injury− EAC laceration often mistaken for TM perf/rupture
− Ask about vertigo
− Audiogram once healed
Special foreign body cases

Temporal Bone Fracture
• Diagnosis: CT of Temporal bones (can often reformat from CT head)
• Classification: Longitudinal, Transverse, Oblique

Complications
• Vertigo• CSF otorhinorrhea• Meningitis• Intracranial hemorrhage• Pneumocephalus
• EAC laceration
• EAC stenosis
• Hemotympanum
• TMJ dysfunction
• TM perforation
• Facial weakness
• Hearing loss

Complications
• EAC laceration
• Frequently mistaken for perforation
• Treat with Floxin or Ciprodex for 7-10 days
• Usually heal spontaneously
• Small risk of residual stenosis

EAC Laceration
EAC Laceration
• Acute management: – Ciprodex
– monitor for facial weakness
– monitor for CSF otorhinorrhea
– neurosurgical care

Hemotympanum

Facial Paralysis Classification

Facial Paralysis Management
• Immediate versus delayed onset• Complete versus incomplete
– Immediate, complete: decompression
– Delayed and/or incomplete: steroids +/- valtrex
– Surgery if >90-95% degeneration in 14-21 days
– Must decompress entire nerve in order to get genu
– Genu most common site of impaction

Temporal Bone Fracture
• Long term management– audiogram once healed
– possible middle ear exploration;
– increased risk for meningitis (especially if otic capsule fractured)
Recommended