Update in Management of
Chronic Hepatitis B Prepared By
Almetwally Zakaria Abdelbaset
Prof. and Head of Department of Hepatology and Gastroenterology
Faculty of Medicine , Benha University, Egypt

Approximately one third of the world’s
population has serological evidence of
past or present infection with HBV and
350–400 million people are chronic HBV
surface antigen (HBsAg) carriers


The spectrum of disease and natural
history of chronic HBV infection are
diverse and variable, ranging from an
inactive carrier state to progressive
chronic hepatitis B (CHB), which may
evolve to cirrhosis and hepatocellular
carcinoma (HCC).


HBV-related end stage liver disease or HCC
are responsible for over 0.5–1 million deaths
per year and currently represent 5–10% of
cases of liver transplantation

Host and viral factors, as well as coinfection
with other viruses, in particular hepatitis C virus
(HCV), hepatitis D virus (HDV), or HIV together
with other co-morbidities including alcohol
abuse and obesity, can affect the natural course
of HBV infection as well as efficacy of antiviral
strategies

CHB may present either as HBeAg-positive or
HBeAg-negative CHB.
The prevalence of the HBeAg-negative form of
the disease has been increasing over the last
decade as a result of aging of the HBV-infected
population and predominance of specific HBV
genotypes and represents the majority of cases
in many areas.

Morbidity and mortality in CHB are linked to
persistence of viral replication and evolution to
cirrhosis and/or HCC.
Longitudinal studies of untreated patients
indicate that, after diagnosis, the 5-year
cumulative incidence of developing cirrhosis
ranges from 8% to 20%.

The 5-year cumulative incidence of
hepatic decompensation is approximately
20% for untreated patients with
compensated cirrhosis
Untreated patients with decompensated
cirrhosis have a poor prognosis with a 14–
35% probability of survival at 5 years

The worldwide incidence of HCC has
increased, mostly due to persistent HBV
and/or HCV infections; presently it
constitutes the fifth most common cancer,
representing around 5% of all cancers.
The annual incidence of HBV-related HCC in
patients with CHB is high, ranging from 2%
to 5% when cirrhosis is established.

The annual incidence of HBV-
related HCC in patients with CHB
is high, ranging from 2% to 5%
when cirrhosis is established

Treatment of Chronic Hepatitis B
What is the evidence that treatment improves
outcome?
Who should be treated?
When should treatment be initiated?
How long should antiviral treatment be given?
How do we deal with antiviral resistance?

Antiviral treatment has been
shown to be effective in suppressing
hepatitis B virus replication,
decreasing inflammation and
fibrosis in the liver, and preventing
progression of liver disease
• However, current medications do not
eradicate hepatitis B virus; therefore, a
key question is which patients need to
start treatment and which patients can
be monitored.

However, current medications do
not eradicate hepatitis B virus; so
a key question is which patients
need to start treatment and
which patients can be monitored.

Drugs available for the treatment of CHB include
IFN, PEG-IFN and six NAs.
NAs for HBV therapy can be classified into:
Nucleosides (lamivudine, telbivudine,
emtricitabine, entecavir)
Nucleotides (adefovir and tenofovir).
PEG-IFN-2b and emtricitabine are not licensed for
HBV treatment in most European countries

Lamivudine, adefovir, entecavir, telbivudine and tenofovir
have been approved in Europe for HBV treatment, and the
combination of tenofovir and emtricitabine in one tablet has
been licensed for the treatment of human HIV infection.
The efficacy of these drugs has been assessed in randomized
controlled trials at 1 year (2 years with telbivudine).
Longer-term results are now available from extension of the
randomized trials sometimes in patient subgroups and
several cohort studies.

Which Drugs to Choose •First line drugs
–Peg-Interferon: Expensive, no resistance
–Entecavir: Very potent, less resistance , expensive
–Tenofovir: very potent, less expensive, resistance?
•Second line drugs
–Lamivudine: Potent, high resistance rate, cheapest
–Telbivudine: Potent, expensive, resistance common
–Emtricitabine: Potent, expensive, resistance common
–Adefovir: Less potent, Fails in 30%, expensive

How to Follow Patients ?
•ALT, AST, HBV DNA every 3-6 months
•If HBV DNA level increases 1 log or
above 2,000 units, test for resistance

Duration of Treatment
•HBeAg-positive:
–Until at least 6 months after loss of HBeAg and
appearance of anti-HBe
•HBeAg-negative (anti-HBe positive)
–Interferon: 1 year
–Nucleoside analogues: Indefinitely

Currently, there are two different strategies
for both eAg-positive and eAg-negative CHB
patients:
Treatment of finite duration with PEG-IFN or
a NA
Long-term treatment with NAs

An attempt for finite NA treatment should use the
most potent agents with the highest barrier to
resistance to rapidly reduce levels of viremia to
undetectable levels and avoid breakthroughs due to
HBV resistance

Long-term treatment with NA(s)
This strategy is necessary for patients who are not
expected or fail to achieve a sustained off-treatment
virological response and require extended therapy,
i.e. for HBeAg-positive patients who do not develop
anti-HBe seroconversion and HBeAg-negative
patients.
This strategy is also recommended in patients with cirrhosis irrespective of HBeAg status or anti-HBe seroconversion on treatment

This strategy is also
recommended in patients with
cirrhosis irrespective of HBeAg
status or anti-HBe
seroconversion on treatment

The most potent drugs with the optimal
resistance profile, i.e. tenofovir or entecavir,
should be used as first-line monotherapies
Treatment with either tenofovir or entecavir
monotherapy for ⩾3 years achieves
maintained virological remission in the vast
majority of patients

Tenofovir is preferred in:
patients who received lamivudine previously
young women who plan to start a family in next
few years
patients who want more flexibility with regard to
the time of day at which they take their medicine
Entecavir is preferred in:
older patients
patients with medical conditions that increase risk
of renal failure

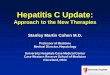
Pegylated Interferon
Effect of Genotype
A large multicenter study of 52
weeks of pegylated interferon
alfa-2b, alone or in combination
with LAM, according to
genotype:
HBeAg-positive patients with
genotype A responded
significantly more frequently
than those with genotypes B, C,
or D in descending order.
Percent HBeAg response irrespective
of treatment assignment (pegylated
interferon/placebo vs pegylated
interferon/LAM).

Pegylated Interfon
Poor response in Egyptian patients with
predominant Genotype D.
HbeAg positive patients with high liver enzymes
could be offered a chance of treatment with peg
Inf alfa for 24 weeks.
Seroconversion to HBeAb →continue for 48 wks
No seroconversion →stop ttt and shift to oral
antiviral therapy according to previous guidelines

The main theoretical advantages of (PEG-)IFN
are the absence of resistance and the potential
for immune-mediated control of HBV infection
with an opportunity to obtain a sustained
virological response off-treatment and a chance
of HBsAg loss in patients who achieve and
maintain undetectable HBV DNA.
Frequent side effects and subcutaneous injection
are the main disadvantages of (PEG-)IFN
treatment

Frequent side effects and subcutaneous injection
are the main disadvantages of (PEG-)IFN treatment
PEG-IFN is contraindicated in patients with
decompensated HBV-related cirrhosis or autoimmune
disease, in patients with uncontrolled severe
depression or psychosis, and in female patients during
pregnancy



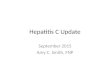
Liver biopsy(Indications)
HBV DNA > 2000 IU/ML with persistently normal enzymes .
HBV DNA < 2000 IU/ML with persistently elevated enzymes .
Patients < 2000 IU/ML with normal enzymes who show clinical
evidence of liver disease or have a family history of HCC
Treatment is recommended for those with >A1
and / or >F1 on the Metavir score

Liver biopsy : METAVIR scoring system
F1 F2 F3 F4
From Z. Goodman


Special Groups Compensated Cirrhosis:
Naive Cirrhotic patients with any detectable level of HBV
DNA should receive Entecavir 0.5 mg or Tenofovir
300mg.
Decompensated Cirrhosis:
Entecavir 1 mg may be appropriate. The dose of all NA,s
needs to be adjusted in patients with low creatinine
clearance (< 50ml/min)

Dialysis and Renal patients
All renal patients should be screened for HBV
Seronegative patients should be vaccinated.
Entecavir is preferred for treatment.
All drugs should be dose adjusted according
to creatinine clearance.

Pregnancy
For mothers:
- All pregnant females should be screened for HBsAg
- Newly diagnosed pregnant women in the last trimester showing an
HBV DNA level > 100.000 IU/ML are candidates for Lamivudine 100
mg or Tenofovir 300 mg starting last trimester and for 3 months
after delivery to decrease chance of new-born infection . Re-
evaluate the condition after 3 months of delivery and consider
treatment according to the previous guidelines

Pregnancy
For newborns:
HB Ig and HBV vaccine first (birth) dose for the
baby in the first 6-12 hours after delivery.
Birth dose vaccination is recommended for all
newborns.

Females who become pregnant while on treatment
– On Lamivudine monotherapy: Continue on treatment
– On Other lines of treatment : shift to class B drug
(Tenofovir 300 mg O.D.)

HBV/HDV Coinfection
Peg –INF is the only effective drug against HDV.
Efficacy of Peg –INF is assessed during treatment after 3-6 months by measuring HDV RNA levels.
Optimal duration of therapy is not well defined but therapy for at least 72 wks .
NAs have no impact on HDV replication and related disease.
Refer the patient to a specialized HBV center.

Immunosupressed Patients
Patients with high HBV DNA level should receive NA with high viral potency according to guidelines.
HBsAg neg patients with positive anti- HBc antibodies should be tested for HBV DNA. Patients with detectable viremia should be treated as HBsAg positive cases.
Follow up of cases with undetectable viremia every 1-2 months during treatment by liver enzymes and HBV DNA.

HBV/HCV Co infection
-Treat predominant virus according to PCR level.
-Patients fulfilling the inclusion criteria for HBV
treatment and have co-infection with active HCV
(HCV RNA +ve by quantitative PCR)
Monitoring for HBV is performed every 3-6
months.
Reassessment of the condition after termination
of the course and starting oral HBV treatment if
needed.
.
Peg IFN + Ribavirin

Follow up
Follow up visits (every 2-3 months)for receiving
medications & follow up for side effects and relapsing
symptoms.
Checking liver enzymes every 3 months.
Serum creatinine is done every 3 months in those
receiving Adefovir. For Tenofovir in addition monitor
creat.clearance and serum phosphate for risk of renal
impairement and osteomalacia.
Liver function tests, complete blood count, A.F.P.,
Abdominal U/S & HBV/DNA by PCR quantitative is
done every 6 months

Conclusions • Persons with chronic HBV infection need
lifelong follow-up
• Patients with moderate or advanced fibrosis or
inflammation can benefit by treatment
• Patients undergoing chemo or
immunosuppressive therapy need HBV
serology testing
• Perform surveillance of HBV infected persons
for HCC as per AASLD guidelines

Acute HBV
Spontaneous recovery in more than 95% of cases and seroconversion to anti HBs without antiviral therapy. Supportive management and close monitoring for early identification of fulminant hepatitis or liver cell failure
Fulminant or impending liver cell failure:
Entecavir 0.5 mg during the condition and for at least 6 months after seroconversion to anti HBs or for at least 12 months after seroconversion to anti HBe without HBs Ag loss

Vaccination
-Mass vaccination is recommended.
-Vaccination is highly recommended for:
Health care workers
Close contacts of viremic patients
Chronic renal failure patients before they start renal
dialysis.
Chronic hepatitis C patients.
Immunosupressed patients.
Multitransfused individuals

Although much has been
accomplished in the therapy
of HBV infection over the
past decade, much work still
remains to be done

Antiviral treatment for
CHB is effective, and
cost effective

Early Cirrhosis Can be Completely
Reversed! •Remove the cause of cirrhosis and reversal will
take place over about 10 years
•Even 30% to 50% of persons with
decompensated cirrhosis will become
compensated (look normal clinically and by LFT)
after proper treatment

Recommended