
VORAVIT CHITTITAVORNVORAVIT CHITTITAVORN
CARDIOVASCULAR THORACIC.
DEPARTMENT OF SURGERY.
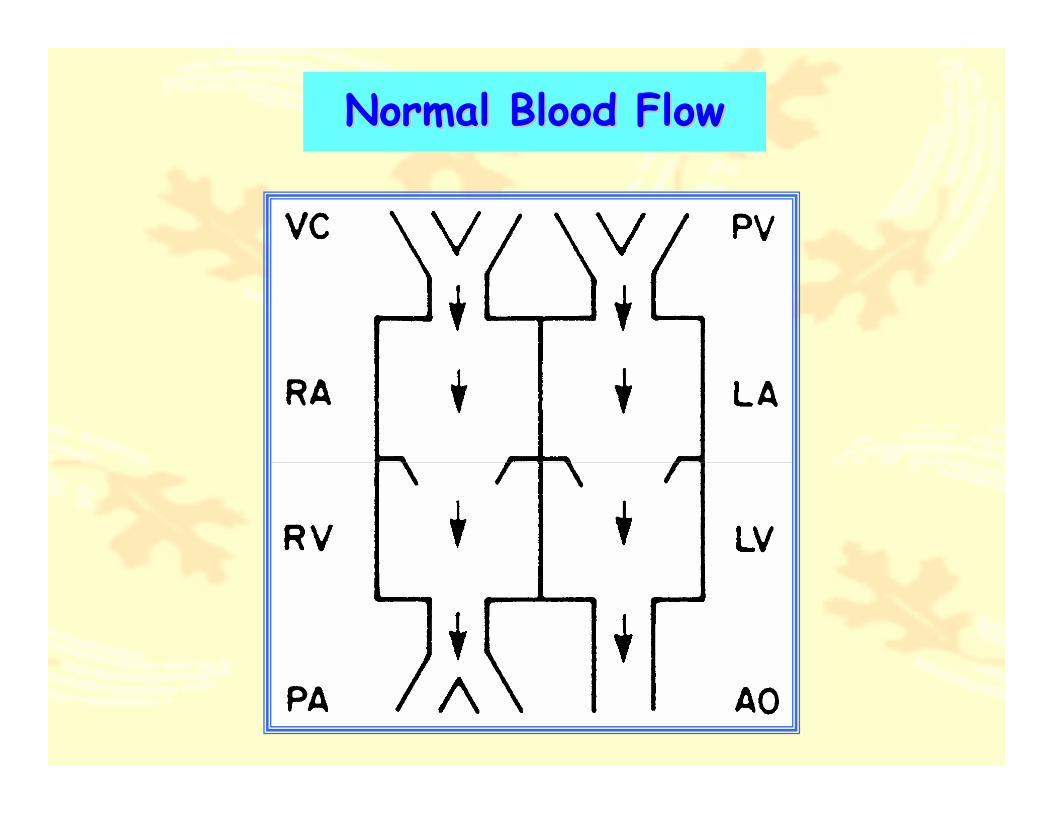
Normal Blood FlowNormal Blood Flow
CONGENITAL HEART DISEASE CONGENITAL HEART DISEASE ((CHDsCHDs))
1.1. Cyanotic Heart DiseaseCyanotic Heart Disease� Increase Pulmonary Blood FlowIncrease Pulmonary Blood Flow
•TGA
•TAPVC
•Tricuspid Atresia (TA)
•Truncus Arteriosus
•HLHS

1.1. Cyanotic Heart DiseaseCyanotic Heart Disease� Decrease Pulmonary Blood FlowDecrease Pulmonary Blood Flow
•Tetralogy of Fallot (TOF)
• Pulmonary Atresia (PA)
•Tricuspid Atresia (TA)
CONGENITAL HEART DISEASE CONGENITAL HEART DISEASE ((CHDsCHDs))
2.2. NonNon--Cyanotic Heart DiseaseCyanotic Heart Disease� Increase Pulmonary Blood FlowIncrease Pulmonary Blood Flow
•Atrial Septal Defect (ASD)
•Ventricular Septal Defect (VSD)
• Patent Ductus Arteriosus (PDA)
•Aortopulmonic Window (APW)
•Endocardial Cushion Defect (ECD)
CONGENITAL HEART DISEASE CONGENITAL HEART DISEASE ((CHDsCHDs))
2.2. NonNon--Cyanotic Heart DiseaseCyanotic Heart Disease�� Normal Pulmonary Blood FlowNormal Pulmonary Blood Flow
•Coarctation of Aorta
•Aortic Stenosis (AS)
•Mitral Stenosis (MS)
CONGENITAL HEART DISEASE CONGENITAL HEART DISEASE ((CHDsCHDs))

DIAGNOSIS FOR CHDsDIAGNOSIS FOR CHDs
1. History
2. Physical Examination
3. Radiographic Study
4. Electrocardiogram (ECG)
5. Echocardiography
6. Cardiac Catheterization
ATRIAL SEPTAL DEFECT (ASD)
• ASD, Isolate anomaly 5 to 10% of all CHDs
• Male : Female = 1 : 2
• Classification to Three Types
1. Secondum Defect (50-70%)
2. Primum Defect (10-15%)
3. Sinus Venosus Defect (10%)

Type of ASDType of ASD

ASD SECONDUMASD SECONDUM
• Usually Asymptomatic in childhood
• Physical Examination
Relative Slender Body
Wide Split and Fixed S2
Systolic Ejection Murmur
• ECG : RAD and/or RBBB
• CXR : Cardiomegaly with Prominent PA

ATRIAL SEPTAL DEFECT (ASD)
ASD SECONDUMASD SECONDUM
• EchocardiographyDiagnostic Tool
Evaluation For1. Size of ASD
2. Flow Direction
3. Estimation of PA and RV pressure
ASD ASD :: NATURAL HISTORYNATURAL HISTORY
• Spontaneous Closure, before 3 months and defect <3 mm, 100% spontaneous closure
• Rare to spontaneous closure, when defect larger than 8 mm
• If untreated ASD, PHT develop in adult 20 to 40 years of life
• IE not associated to ASD, SBE prophylaxis is unnecessary

MANAGEMENT OF ASDMANAGEMENT OF ASD
Medical Treatment
• NOT Exercise restriction
• IE prophylaxis unnecessary
• For CHF
Surgical Treatment
• Pericardial Patch Closure
• Prosthetic Patch Closure
SURGICAL MANAGEMENT OF SURGICAL MANAGEMENT OF ASD SECONDUMASD SECONDUM
Indication For Surgery• Symptomatic ASD Secondum
• Lt. to Rt. shunt flow (Qp:Qs > 1.5:1)
Contraindication For Surgery
• High Pulmonary Vascular Resistant (PVR)more than 10 unit/m2

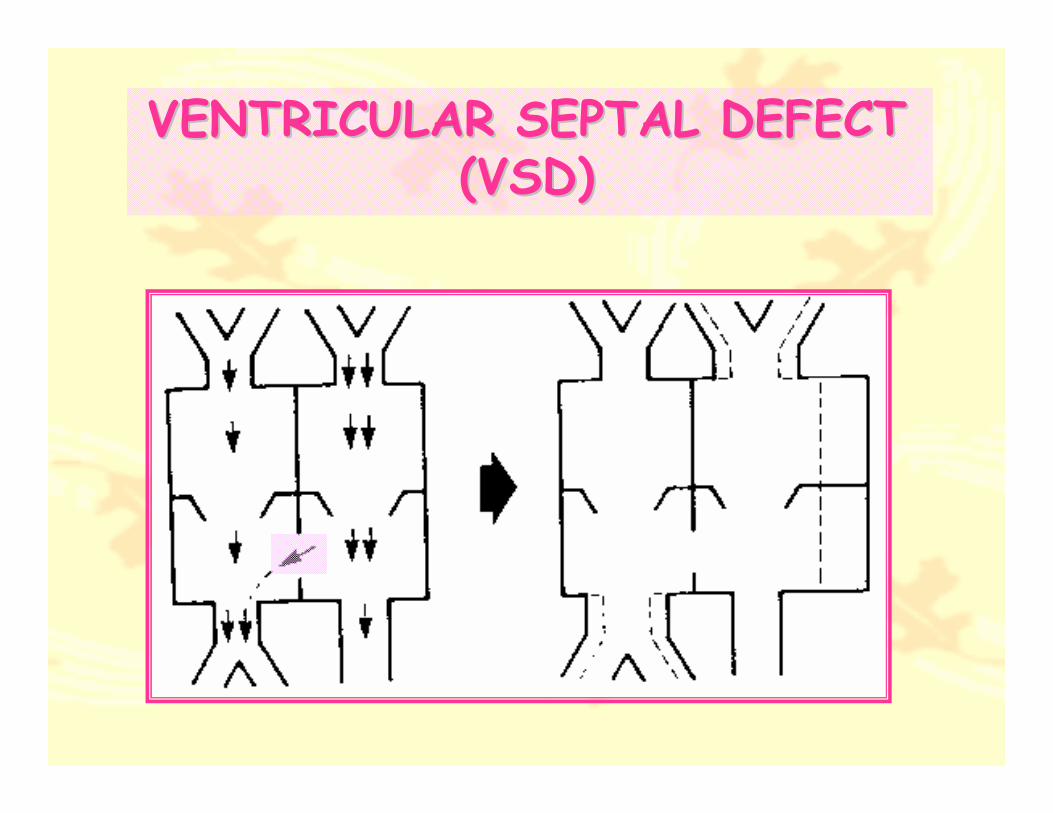
VENTRICULAR SEPTAL DEFECT VENTRICULAR SEPTAL DEFECT ((VSDVSD))
• Most common form of CHDs, 15-20%
• Classification
Perimembranous
Inlet Type
Outlet or Infundibular
Apical Muscular
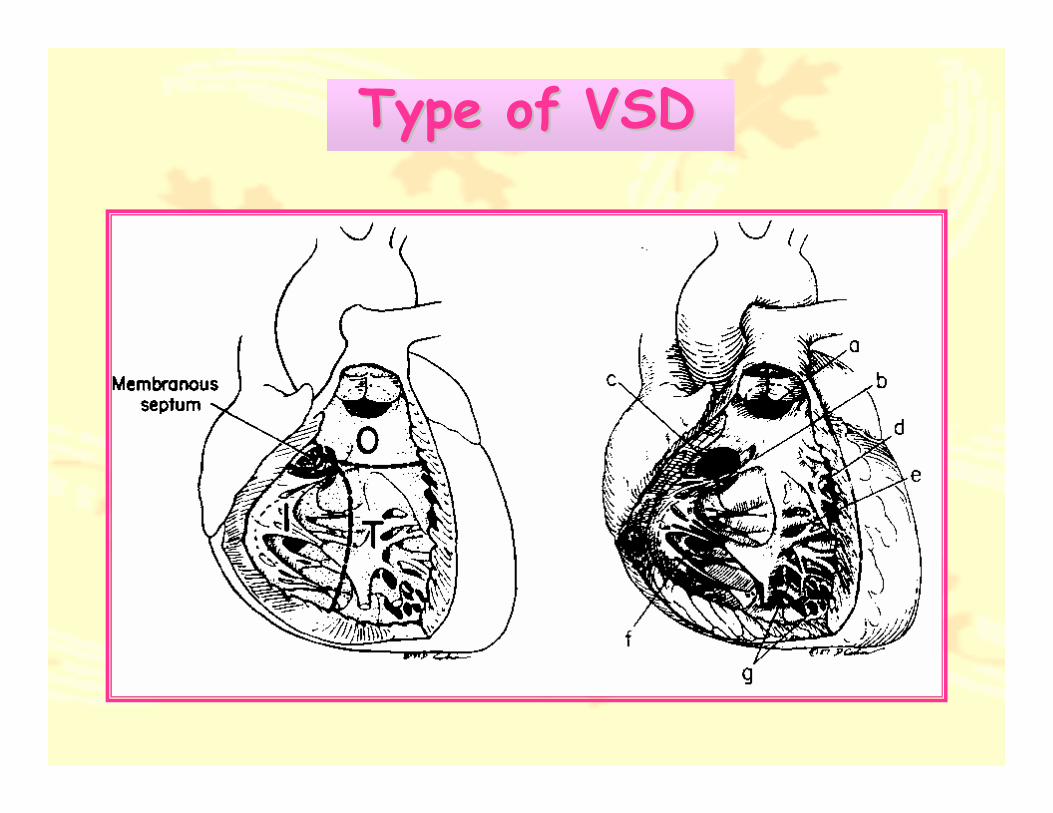
Type of VSDType of VSD
PATHOLOGICAL OF VSDPATHOLOGICAL OF VSD
• The Bundle of His related to Posteroinferior rim of Perimembranous VSD
• Outlet and Apical Trabeculae Type, not associate to the Conduction system
• In Infundibular defect (Subpulmonic or Subaortic VSD), NOT UNCOMMON to associate AR, most by herniate of RCC
VENTRICULAR SEPTAL DEFECT VENTRICULAR SEPTAL DEFECT ((VSDVSD))

CLINICAL MANIFESTATION OF CLINICAL MANIFESTATION OF VSDVSD
• Small VSD, usually asymptomatic
• Moderate to Large VSD, Delayed growth and development,repeated pulmonary infection, CHF and decrease exercise tolerance
• Long standing PHT, reverse shunt Rt. to Lt. shunt may be occurred and cyanosis

PHYSICAL EXAMINATION OF PHYSICAL EXAMINATION OF VSDVSD
• Systolic Thrill or SEM at LLSB
• Precordial bulge and Hyperactivity
• Poor Weight gain
• Signs of CHF

Electrocardiography• Small VSD, Normal ECG
• Moderate or Large VSD, LAD or LVH
• In PVOD, ECG show RVH only
Radiographic Finding• Cardiomegaly, LA and LV enlargement
• Prominent PA trunk
• In PVOD, Hilar MPA enlarge,but!Peripheral lung field oligemic, normal heart size
VSD VSD :: NATURAL HISTORYNATURAL HISTORY
• Spontaneous closure, occur in Perimembranous and Muscular Defect
• Age at 1,3 and 6 months,Spontaneous closure occur 80%,60%and 50%
• EISENMENGER SYNDROME

MANAGEMENT OF VSDMANAGEMENT OF VSD
Medical Treatment• Treatment of CHF with Diuretic and
Digoxin
• Correct of associated Pulmonary infection
Surgical Treatment• Surgical Closure of VSD
SURGICAL TREATMENT FOR SURGICAL TREATMENT FOR VSDVSD
Surgical Indication• Infant with large VSD and CHF,
with failed medical treatment
• After 1 year, Qp:Qs > 1.5:1
• Older infant with large VSD and elevation of PVR

SURGICAL TREATMENT FOR SURGICAL TREATMENT FOR VSDVSD
Surgical Contraindication• Small VSD, with Qp:Qs < 1.5:1
• Irreversible High PVR or PVOD or prominent Rt. to Lt. shunt

PATENT DUCTUS ARTERIOSUS PATENT DUCTUS ARTERIOSUS ((PDAPDA))
• Occur 5-10% of all CHDs
• More common in female
• Result from, Abnormally not regress of dorsal aortic arch 6th
Clinical ManifestationClinical Manifestation• Usually Asymptomatic, when PDA small
• Large PDA, dyspnea and/or pulmonary infection and/or CHF can occurred

PATENT DUCTUS ARTERIOSUS PATENT DUCTUS ARTERIOSUS ((PDAPDA))
PHYSICAL EXAMINATION OF PHYSICAL EXAMINATION OF PDAPDA
• Hyperactive Precordium
• Systolic Thrill at LUSB
• Elevate of SBP and lower DBP
• Normal P2 sound
• Continuous or Machinery Murmur

PDA PDA :: NATURAL HISTORYNATURAL HISTORY
• Definition to classified PDA, When persistent of Ductus until 3 months age
• Chance of spontaneous closure in premature infant more than term infant
• CHF and Recurrent pneumonia, usually occurred in large PDA
• BE more frequent in small PDA than in large PDA

MANAGEMENT OF PDAMANAGEMENT OF PDA
Medical Treatment• NSAID, Indomethacin
• Diuretic and Digitalis
Intervention Non Operative Procedure• Devices Closure
Surgical Treatment• PDA Ligation
• PDA Division and Suture
SURGERY FOR PDASURGERY FOR PDA
Surgical IndicationSurgical Indication
• Anatomic existence, Regardless of size PDA
Surgical ContraindicationSurgical Contraindication
• Presence of PVOD
Surgical ComplicationsSurgical Complications
• Injury To Recurrent Laryngeal Nerve,Lt. phrenic nerve, Chylothorax,Recanalization,Bleeding
COARCTATION OF AORTA COARCTATION OF AORTA ((CoACoA))
• MORE COMMON IN MALE
• Turner Syndrome, 30% ASSOCIATED
• Associated Cardiac Defect:Aortic Hypoplasia
AV abnormality
VSD (50%)
PDA (60%)
MV abnormality

COARCTATION OF AORTA COARCTATION OF AORTA ((CoACoA))
Clinical ManifestationClinical Manifestation• Poor Feeding, Poor Weight Gain
• Acute Circulatory Shock, CHF
Physical ExaminationPhysical Examination• Oliguria, Anuria, Acidemia
• Differential Cyanosis
• Weak Peripheral Pulse
• Signs of CHF
Radiographic FindingRadiographic Finding• Marked Cardiomegaly
• 3 sign picture

COARCTATION OF AORTA COARCTATION OF AORTA ((CoACoA))
MANAGEMENT OF CoA
Medical Treatment• Prostaglandin E1
• Correct CHF and Acidosis
Intervention and Non Operative• Balloon Angioplasty
Surgical Treatment• Coarctectomy with End to End Anastomosis
• Subclavian Flap or Patch Graft Aortoplasty

SURGICAL TREATMENT FOR CoA
Surgical Indication• Symptomatic, CHF or Circulatory Shock
• Asymptomatic, When PG > 20 mmHg
• Associated with VSD
Surgical Complication• Renal Failure
• Residual or Recoarctation
• Necrotizing Mesenteric Arteritis
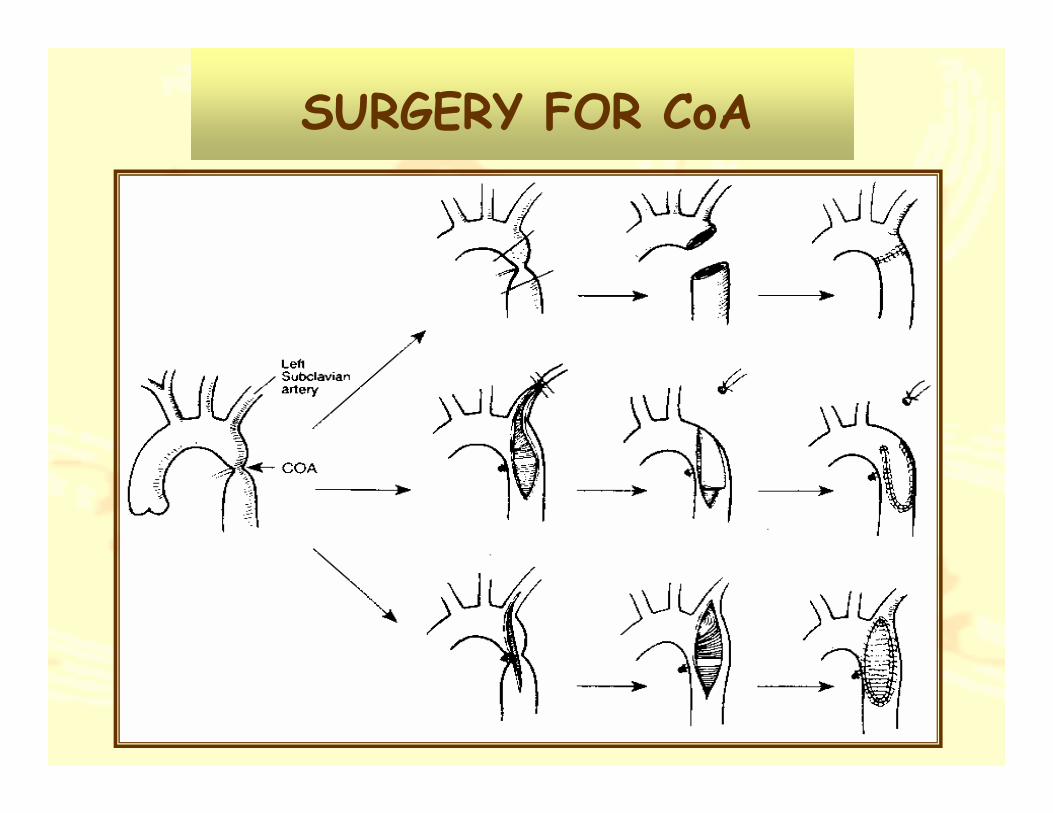
SURGERY FOR CoA

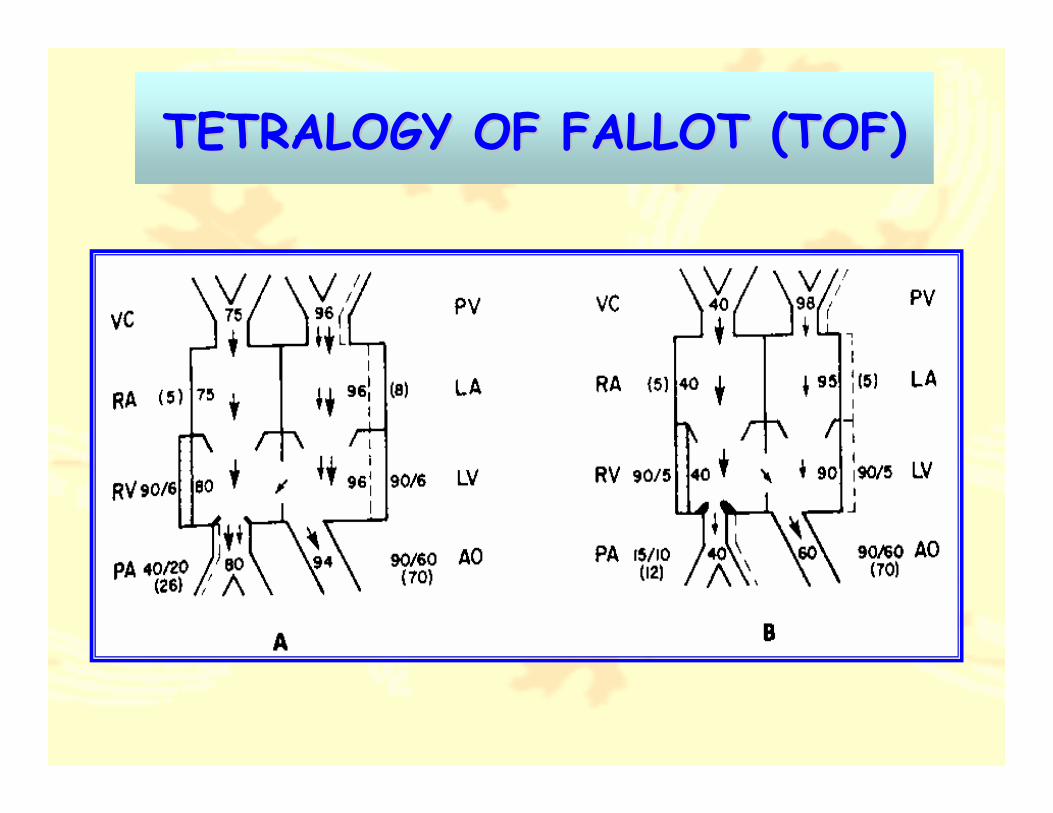
TETRALOGY OF FALLOT TETRALOGY OF FALLOT ((TOFTOF))
• Composed of 4 abnormalities1. Large VSD
2. Right Ventricular Outflow Tract Obstruction (RVOTO)
3. RVH
4. Overriding of Aorta
TETRALOGY OF FALLOT TETRALOGY OF FALLOT ((TOFTOF))

PATHOLOGICAL PATHOLOGICAL :: TOFTOF
• Most VSD in TOF is Perimembranous
• RVOTO, most common at Infundibular stenosis
• PV annulus usually small, Hypoplastic MPA and small PA branch
• RT aortic arch, 25%
• Abnormal coronary artery, LAD from RCA
Clinical Manifestation• Dyspnea on exertion
• Cyanosis
• CHF
• Hypoxic Spell
Physical Examination• Vary degree cyanosis, Tachypnea,
Clubbing
• SEM at LUPSB
Electrocardiography• Cyanotic TOF show RAD
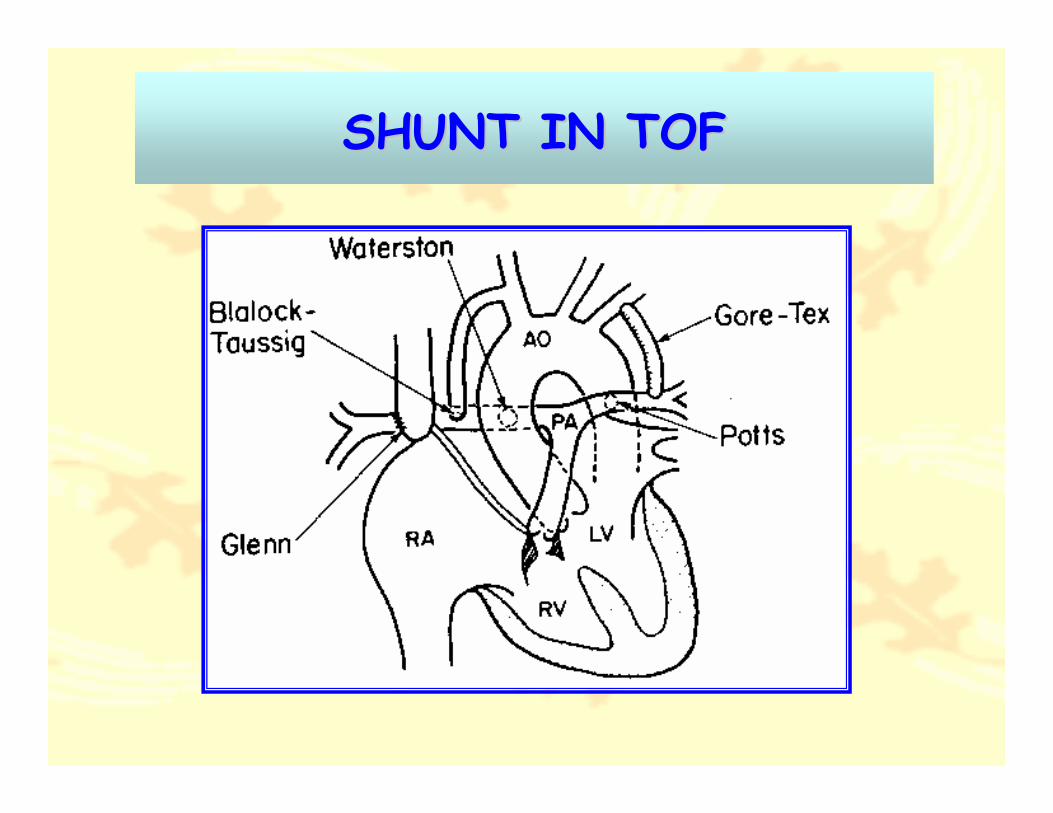
SHUNT IN TOFSHUNT IN TOF

Radiographic Finding• Normal Heart size or smaller
• Decrease Pulmonary Vasculature
• Boot Shaped or Coeur En Sabot
Echocardiography• Diagnostic Tool
• Severity of TOF
• Anomalous of coronary artery
• Associated Anomalies

ECHOCARDIOGRAPHY OF TOFECHOCARDIOGRAPHY OF TOF
TOF TOF :: NATUERAL HISTORYNATUERAL HISTORY
• Progressive Cyanosis and Infundibulum Stenosis
• Growth Retardation
• Polycythemia
• Paradoxical Emboli
• Hypoxic SpellParoxysmal hyperpnea, increase
cyanosis, Decrease intensity of murmur
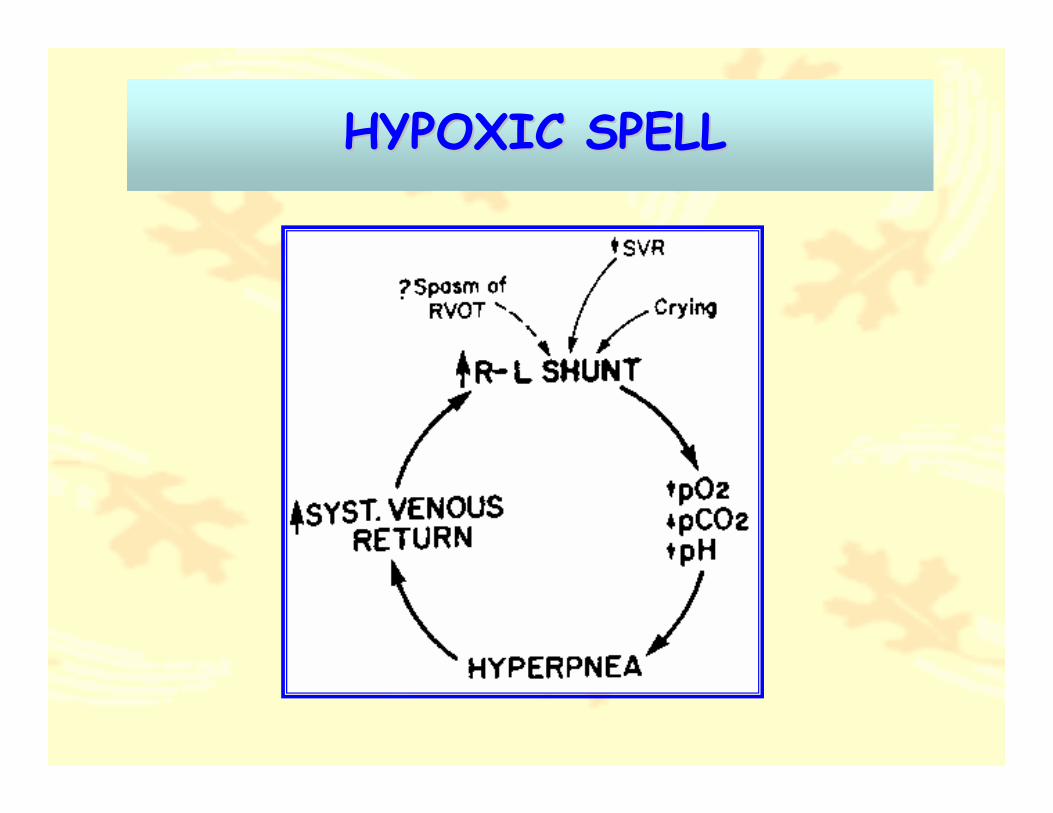
HYPOXIC SPELLHYPOXIC SPELL

MANAGEMENT OF TOFMANAGEMENT OF TOF
Medical Treatment• Recognized and treat Hypoxic Spell
• Maintenance good oral hygiene
• Correct Iron deficiency anemia
Surgical Treatment• Palliative Procedure
• Definitive Surgery
PALLIATIVE SURGERY FOR TOFPALLIATIVE SURGERY FOR TOF
• To Augment Pulmonary Blood Flow
• To Promote Size of PA branches
• Most common shunt used, Modified Blalock-Taussig Shunt (MBTs)
• Indications : Neonate TOF with PA,Infant with small pulmonary annulus,Severe cyanotic infant, Infant with spell,Infant with anomaly coronary artery

DEFINITE SURGERY FOR TOFDEFINITE SURGERY FOR TOF
• Composed of :
1. Correct RVOTO
2. Closure VSD
• Indications: Symptomatic infant with favorable RVOT and PA size, Previously palliative shunt 1 To 2 years
• Complication: Bleeding, PV regurgitation, CHF, RBBB, CHB
TRANSPOSITION GREAT ARTERIES TRANSPOSITION GREAT ARTERIES ((TGATGA))
• Considered to D-TGA
• More common in male (M:F = 3:1)
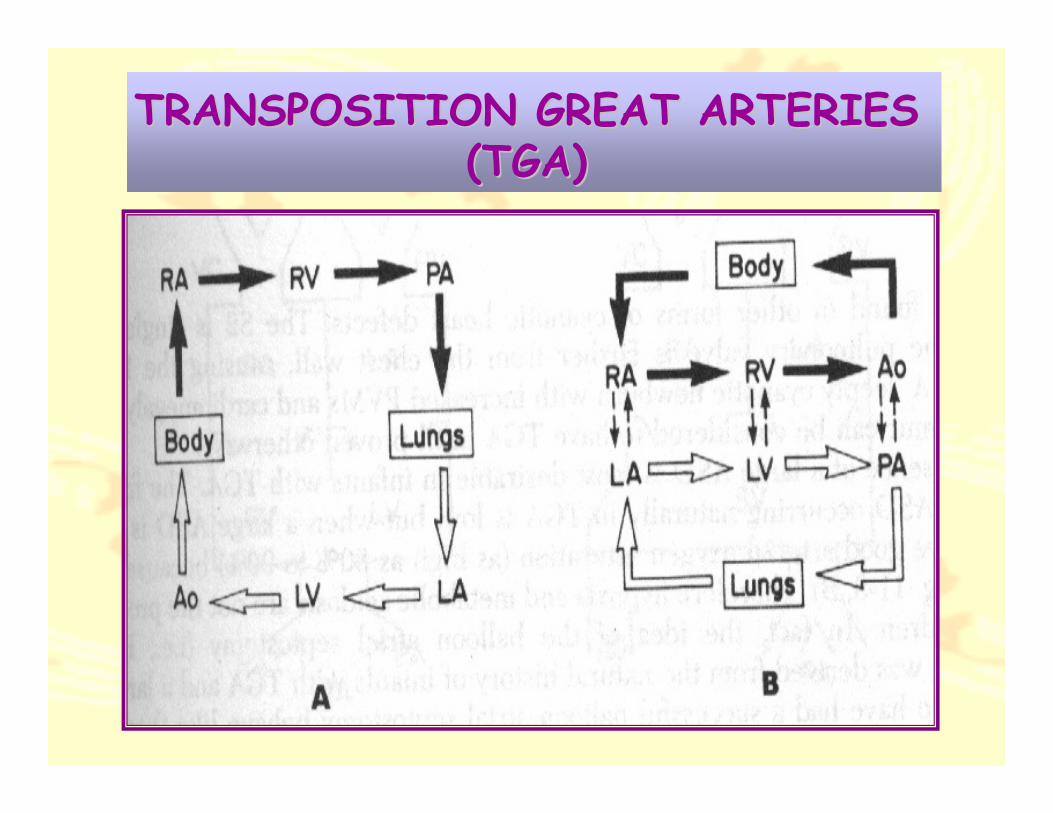
• D-TGA, aorta arise from RV, anterior to PA
• PA arise from LV, posterior to aorta
• Mixing of two circulations at ASD, or VSD, or PDA necessary for survival
• VSD, occur 30 to 40%, anywhere in IVS
TRANSPOSITION GREAT ARTERIES TRANSPOSITION GREAT ARTERIES ((TGATGA))
Clinical Manifestation• Cyanosis at birth
• CHF during newborn
Physical Examination• Moderate to Severe cyanosis
• TGA intact IVS, no murmur
• Severe hypoxemia not response to oxygen
ECG : RAD, RVH, LVH (TGA,VSD)
CXR : Cardiomegaly, Increase PBF
Egg Shape, narrow superior mediastinum

TGA TGA :: NATURALNATURAL HISTORYHISTORY
• Progressive Hypoxemia and Acidosis
• Progressive CHF
• Without surgical intervention, 90% death occur before 6 months of life
• TGA IVS, progress of incompatible LV
• TGA VSD, prone to develop CHF, PVOD
MANAGEMENT OF TGAMANAGEMENT OF TGA
Medical Treatment• Correct Metabolic acidosis
• Prostaglandin E1
• CHF : Diuretic or Digoxin
Surgical Treatment• Palliative Surgical Treatment
• Definite Surgical Treatment
PALLIATIVE SURGERY FOR TGAPALLIATIVE SURGERY FOR TGA
1. For Mixing Blood at Atrium levelBalloon Atrial Septostomy
Operation for Atrial Septectomy
2. For Training LV pressure and LVmuscle to expose the systemic
pressure by the method of PA Banding
DEFINITE SURGERY FOR TGA
To Switch Rt and Lt side blood
for Desaturated blood to Pulmonary circulation and Oxygenated blood to Systemic
circulation, can be done at three levels
1.Atrial Level (Mustard,Senning Operation)
2.Ventricular Level (Rastelli Operation)
3.Great Artery Level (Arterial Switch Op)
AIMAIM::

VORAVIT CHITTITAVORNVORAVIT CHITTITAVORN
CARDIOVASCULAR THORACIC.
DEPARTMENT OF SURGERY.
ACQUIRED HEART DISEASEACQUIRED HEART DISEASE
SPECTRUM OF DISEASESPECTRUM OF DISEASE
1. VALVULAR DISEASE
2. MYOCARDIAL DISEASE
3. CORONARY ARTERY DISEASE
4. GREAT THORACIC VASCULAR
DISEASE

CONTENT
�� VALVULAR HEART DISEASEVALVULAR HEART DISEASE
�� CORONARY ARTERY CORONARY ARTERY DISEASEDISEASE
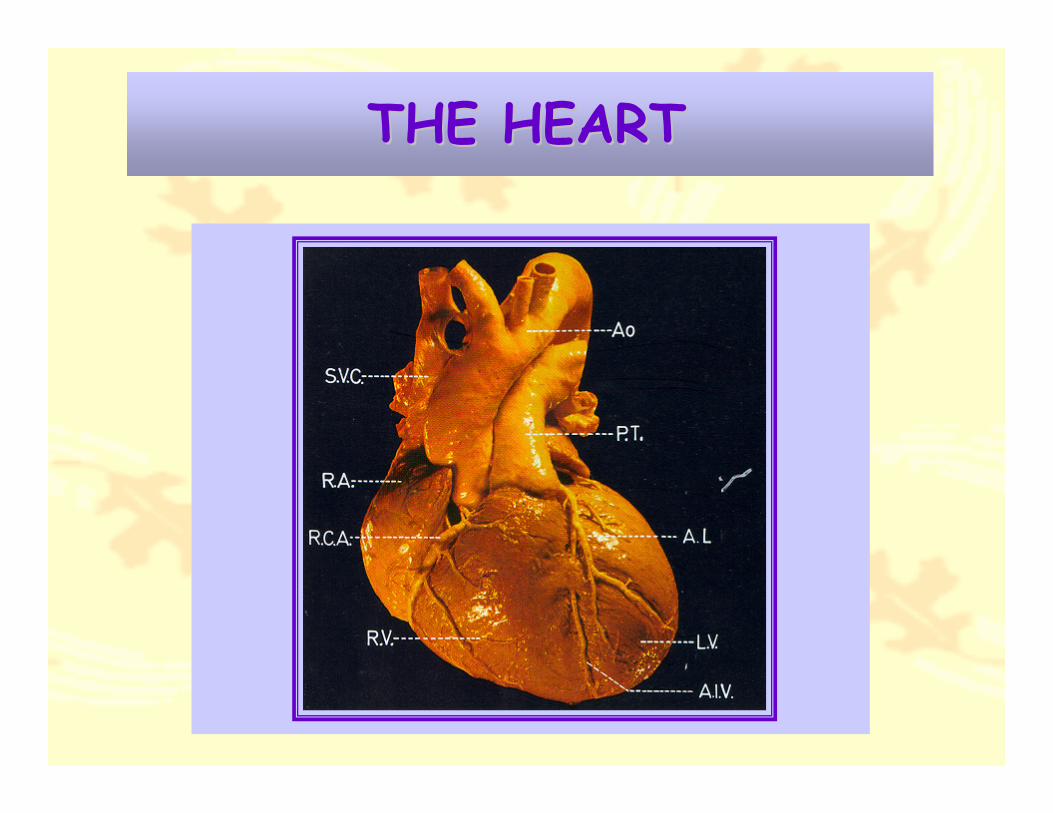
THE HEARTTHE HEART
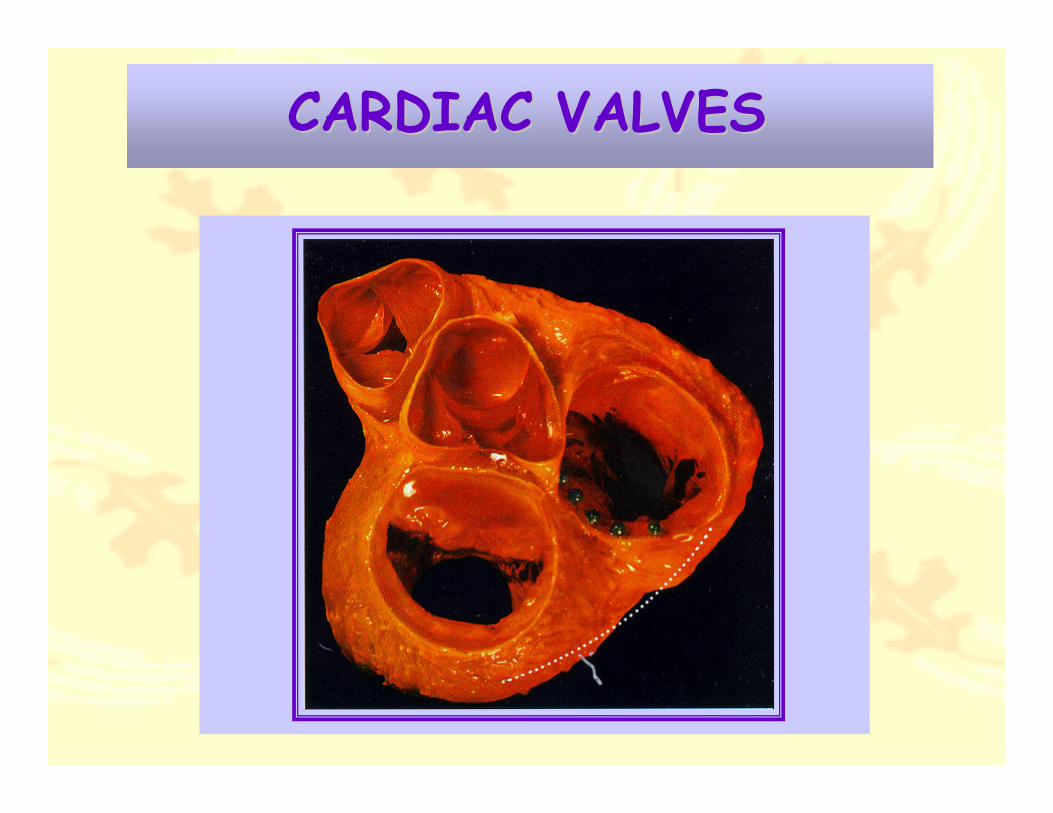
CARDIAC VALVESCARDIAC VALVES
ACQUIRED DISEASE OF THEACQUIRED DISEASE OF THETRICUSPID VALVETRICUSPID VALVE
ANATOMYANATOMY
1. The largest of all cardiac valve
2. In normal adult, TV orifice area 8-10 cm2
3. Composed of three leaflets:
• Anterior leaflet
• Posterior leaflet
• Septal leaflet
4. Related anatomical to conduction system

TRICUSPID VALVETRICUSPID VALVE
PATHOLOGY AND PATHOLOGY AND CLASSIFICATIONCLASSIFICATION
� FUNCTIONAL TV DISEASEFUNCTIONAL TV DISEASE
� ORGANIC TV DISEASEORGANIC TV DISEASE
– TV STENOSIS (TS)
– TV REGURGITATION (TR)

PATHOLOGICAL OF TV
• In Tricuspid Stenosis
RHD is the most common cause
Almost Always, associated MV disease
• In Tricuspid Regurgitation
Most common from Functional TR
Related to Lt. sided heart pressure
PATHOPHYSIOLOGY
TRICUSPID STENOSISTRICUSPID STENOSIS
• Reduced blood flow to pulmonary
circulation
• Decreased preload
• Decreased LV stroke volume
• Causing Salt And Water Retention
Renin-Aldosterone-Angiotensin

PATHOPHYSIOLOGY
TRICUSPID REGURGITATIONTRICUSPID REGURGITATION
• Limit preload to Lt. side heart
• Chronic volume overload to the RV
• Increased intensity of murmur with inspiration
• Hepatojugular Reflux only seen in TR
Diagnosis Study• Echocardiography
• Cardiac Catheterization
Clinical Manifestation
• Tricuspid Stenosis
Prominent jugular “ a - Wave “
AF and RA enlargement
• Tricuspid Regurgitation
Prominent jugular “ v - Wave “
Ascites, Edema, Pulsatile Hepatomegaly
MANAGEMENT OF TV DISEASE
Medical Therapy• Limited role in TS or TR
• Use follow through the clinical sequence
“ Regardless Organic TV disease, Lt. side pathology is the most determinant in planning of management “
Surgical therapy• Surgical Repaired or Replacement
SURGICAL INDICATION
• Evidence of TS or TR with NYHA FC III or IV
• Moderate to Severe TR or Structural TR
• When pressure gradient across TV more than 4 mmHg in TS
ACQUIRED DISEASE OF THE ACQUIRED DISEASE OF THE MITRAL VALVEMITRAL VALVE
Surgical Anatomy• Valvular Leaflet
• Valve Annulus
• Chordae Tendinae
• Papillary Muscle
• LV wall
Normal MV orifice area = 4 to 6 cm2

MITRAL VALVEMITRAL VALVE

PATHOLOGICAL DISEASE OF PATHOLOGICAL DISEASE OF THE MITRAL VALVE THE MITRAL VALVE
� Mitral Stenosis ( MS )
� Mitral Regurgitation ( MR )
MITRAL STENOSISMITRAL STENOSIS
• Only known cause from RF
• Rheumatic Valvulitis
Fusion of Commissure
Fusion and Shortening Chordaes
Fibrosis and Calcification Leaflets
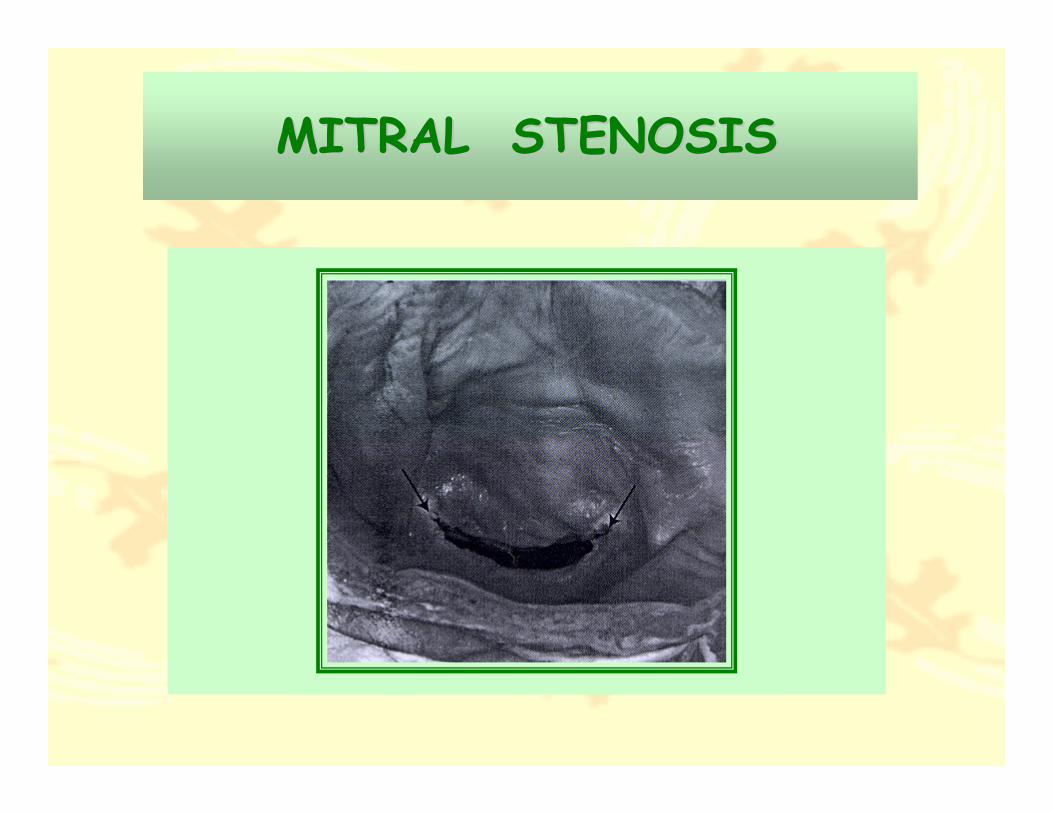
MITRAL STENOSISMITRAL STENOSIS

CLINICAL MANIFESTATION OF MSCLINICAL MANIFESTATION OF MS
• Dyspnea on exertion
• Symptom of Pulmonary Congestion
• Atrial Fibrillation
• Stroke or Arterial Occlusion
• Auscultatory Finding
Apical Diastolic Rumble Murmur
Increase First Heart Sound
Opening Snap

MITRAL STENOSISMITRAL STENOSIS

DIAGNOSIS OF MSDIAGNOSIS OF MS
• EchocardiographySevere MS, when MV orifice < 1 cm2
• Cardiac Catheterization
Significant MS, when pressure gradient more than 5 mmHg
Severe MS, when pressure gradient more than 10 mmHg

MANAGEMENT OF MS MANAGEMENT OF MS
Medical TreatmentMedical Treatment• Symptomatic mild MS, Diuretic and Digitalis
• Associated AF, Anticoagulation drug
• Asymptomatic MS, NOT needed treatment
Percutaneous Transmitral CommissurotomyPercutaneous Transmitral Commissurotomy
(( PTMC PTMC ))
• Contraindication for MS with LA thrombus and MS with moderate MR

SURGICAL TREATMENT FOR MSSURGICAL TREATMENT FOR MS
Surgical Options• Mitral Commissurotomy
• Mitral Valve Replacement ( MVR )
Surgical Indications• Asymptomatic Severe MS
• MS with NYHA FC III or IV
• MS with new onset AF

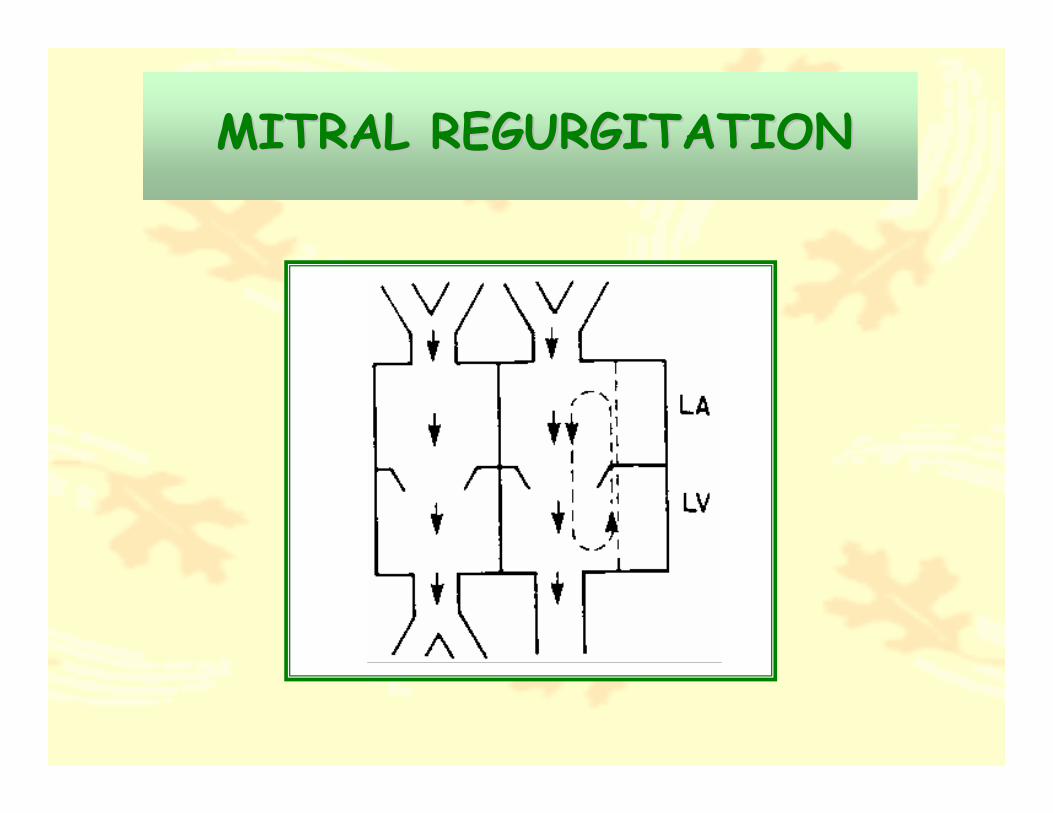
MITRAL REGURGITATION MITRAL REGURGITATION ((MRMR))
ETIOLOGYETIOLOGY
• Myxomatous Degeneration
• Rheumatic Process
• Mitral Valve Prolapse
• Rupture Chordae Tendinae
• Ischemic Mitral Regurgitation

CLINICAL MANIFESTATION CLINICAL MANIFESTATION OF MROF MR
• Asymptomatic
• Dyspnea on exertion
• Palpitation
• Congestive Heart Failure
Timing and Onset of clinical manifestation,depend on the cause of MR

Physical Examination• Holosystolic Murmur or PSM at apex
radiate to the axilla
• Signs of Pulmonary Congestion
• Possible AF
Radiographic Finding
• LA enlargement ( unlike to MS )
• LV enlargement
• Pulmonary Venous Congestion
MITRAL REGURGITATIONMITRAL REGURGITATION

MANAGEMENT OF MRMANAGEMENT OF MR
Medical Treatment• Diuretic and Digitalis
• Afterload Reduction
Surgical Treatment Options• MV Repaired
• MV Replacement ( MVR )

SURGICAL INDICATION OF MRSURGICAL INDICATION OF MR
• Acute Symptomatic MR
• Enlargement of LA more than 4.5cm with recent onset of AF
• Progressive enlargement LVEDD more than 6 cm
• Symptomatic or Asymptomatic with LV Dysfunction
ACQUIRED DISEASE OF THE ACQUIRED DISEASE OF THE AORTIC VALVEAORTIC VALVE
Surgical Anatomy
• Tricuspid Leaflets
Left coronary cusp ( LCC )
Right coronary cusp ( RCC )
Non coronary cusp ( NCC )
• AV Conduction system pass beneath the junction between RCC and NCC
• Normal AV orifice area = 2 to 4 cm2
PATHOLOGICAL DISEASE PATHOLOGICAL DISEASE OF AVOF AV
• AORTIC STENOSIS ( AS )
• AORTIC REGURGITATION ( AR )
AORTIC STENOSIS AORTIC STENOSIS (( AS AS ))
• Most Common Cause from Degenerative Calcification
• AS, Subsequent to LVH, Progression of LVH is mechanism for normalized ventricular wall stress By Increase Wall Thickness
• AFTERLOAD MISMATCH, chronic elevation of LV wall stress from insufficient LVH

Physical ExaminationPhysical Examination• Systolic Ejection Murmur ( SEM )
• Delayed Carotid Upstroke
Clinical ManifestationClinical Manifestation• Syncope
• Angina
• CHF or Arrhythmia
Radiographic FindingRadiographic Finding• Normal to Mild LV enlargement
• Poststenotic Ascending Aortic Enlargement
SEVERE ASSEVERE AS
• AV ORIFICE AREA
LESS THAN 0.8 cm2
• MEAN AV PRESSURE GRADIENT
MORE THAN 50 mmHg

MANAGEMENT OF ASMANAGEMENT OF AS
Medical Treatment• Limited role in symptomatic AS
• Afterload Reduction therapy is relative contraindication
Percutaneous Balloon Valvuloplasty, limited role in adult, But! Good result in child

SURGICAL TREATMENT FOR ASSURGICAL TREATMENT FOR AS
Surgical Options• AV Repaired
• AV Replacement ( AVR )
Surgical Indication• Symptomatic AS
• Asymptomatic AS withAV area less than 0.8 cm2, or PPG over 50 mmHg, or LVESD more than 50 mm, LVEDD > 65 mm
AORTIC REGURGITATION AORTIC REGURGITATION ((ARAR))
ETIOLOGYETIOLOGY
• Degenerative AV
• RHD
• Congenital Bicuspid AV
• Annuloaortic Ectasia (e.g.Marfan Syndrome)
• Aortic Dissection
• Ascending Aortic Aneurysm
• Bacterial Endocarditis
• Trauma
PATHOPHYSIOLOGY OF ARPATHOPHYSIOLOGY OF AR
• Represent volume overload of LV
• Increase Diastolic Filling Pressure
• Raising of LVEDV
• Increase Diastolic Wall Stress
• Long term progressive LV dilatation
CLINICAL MANIFESTATION CLINICAL MANIFESTATION OF AROF AR
• CHF
• Dyspnea
• Paroxysmal Nocturnal Dyspnea
• Orthopnea
• Angina
• Syncope

PHYSICAL EXAMINATION PHYSICAL EXAMINATION OF AROF AR
• Lateral displace of LV apical impulse
• Increase systolic stroke volume
• Decrease diastolic aortic pressure
• Diastolic Blowing Murmur
• Pulsatile peripheral pulse
( Water - Hammer Pulse )

Radiographic Finding• LV enlargement
• Ascending Aorta enlargement
• Pulmonary Venous Engorgement
Diagnostic Study
• Echocardiography
• Cardiac Catheterization

AORTIC REGURGITATIONAORTIC REGURGITATION

MANAGEMENT OF AR MANAGEMENT OF AR
Medical Treatment• Use in Asymptomatic AR with normal LV
function
• Diuretic and Afterload reduction
Surgical Treatment Options
• AV Repaired
• AV Replacement ( AVR )
SURGICAL INDICATIONSURGICAL INDICATIONFOR ARFOR AR
• Symptomatic AR with NYHA FC III or more
• AR with impaired LV function ( LVESD over 55 mm and LVEDD over 65 mm )
• Severe acute AR with CHF
• AV Endocarditis with moderate to severe AR

CORONARY ARTERY DISEASE CORONARY ARTERY DISEASE ((CADCAD))
DEFINITION• Narrowing of one or more coronary
artery from atherosclerotic disease which limit myocardium blood flow
• Significant Stenosis define as diameter
reducing 50%, which equal to
crossectional area reduction 75%

LtLt coronary systemcoronary system• Lt main artery (LM)
• Lt anterior descending
artery (LAD)
: Septal Perforator branch
: Diagonal branch (DG)
• Lt circumflex artery (LCx)
: Obtuse Marginal branch (OM)
RtRt coronary systemcoronary system• Conus branch
• Sinus node artery
• AV nodal artery
• Bifurcation 2 major branches
: Posterolateralbranch (PL)
: Posterodescending(PDA)
CORONARY ARTERY ANATOMYCORONARY ARTERY ANATOMY
RISK FACTORS FOR CADRISK FACTORS FOR CAD
• Old Aging
• Diabetes
• Hypertension
• Smoking
• Hyperlipidemia
• COPD
• Chronic Renal Disease
CLINICAL MANIFESTATION CLINICAL MANIFESTATION OF CADOF CAD
• Acute Myocardial Infarction
• Stable Angina
• Unstable Angina
• Atypical Angina
• CHF
• Clinical of MR or VSD
• Miscellaneous symptoms
MANAGEMENT OF CADMANAGEMENT OF CAD
Medical Treatment• Control of HT, DM and Hyperlipidemia
• Vasodilator Drug (e.g.Nitrate)
• Beta Blocker in selected patients
• Antiplatelet Drugs
• Diuretic, or Calcium Channel Blocker
• Thrombolytic Therapy (e.g.Streptokinase)

INTERVENTION AND NONINTERVENTION AND NON--OPERATIVE TREATMENT FOR OPERATIVE TREATMENT FOR
CADCAD
• Percutaneous Transcoronary Angioplasty
( PTCA )
• Photodynamic Therapy
• Laser Therapy
SURGICAL TREATMENT SURGICAL TREATMENT FOR CADFOR CAD
Surgical Options• Coronary Endaterctomy
• Coronary Artery Bypass Graft (CABG)
Conventional CABG (On CPB)
Off Pump CABG (OPCABG)
• Cardiac Transplantation
INDICATION FOR SURGICAL INDICATION FOR SURGICAL REVASCULARIZATION REVASCULARIZATION ((CABGCABG))
• Failure of medical therapy
• Unstable Angina
• LM Disease
• Symptomatic Triple vessel CAD with LV Dysfunction
• Postinfarction Angina
INDICATION FOR SURGICAL INDICATION FOR SURGICAL REVASCULARIZATION REVASCULARIZATION ((CABGCABG))
• Double vessel disease with proximal disease of LAD
• Acute MI with cardiogenic shock
• Failed PTCA
• Reoperation for recurrent symptom
• Kawasaki Disease
• Congenital Coronary Anomalies
Recommended

















