VTEprophylaxisandproceduralanticoagulation:FocusonOrthopedicsurgeries
SaraMahmoud,BPharm,PharmDcand,BCCCS,RPh
ClinicalPharmacist,AlWakra Hospital
CPDofficecoordinator,HamadMedicalCorporation

LearningObjectives:
• ListtheavailableanticoagulantsinHMCformulary
• ComparedifferentpharmacologicalagentsusedforVTEprophylaxisandtherapy
• ReviewCHESTandAAOSguidelinesinpreventingVTEinorthopedicsurgery
• Outlinetheguidelinesforinterruptinganticoagulationandbridgingtherapyinsurgicalpatients

PharmacologicalagentsusedforVTEprophylaxisandtherapy
Shortacting Maintenance therapyagents (long)
Onsetofaction Rapid Variable(warfarin: 5-7days)
Duration(Halflife) Short Long
Examples LMWH,UFH Warfarin,NOAC/DOAC

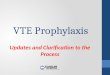
Coagulationcascade
LMWH
UFH

ShortactingEnoxaparin Dalteparin Unfractionated
Heparin(UFH)Mechanismof
actionInhibitfactorXa Inhibitantithrombin
III+factorXa
DosingProphylacticTherapeutic
40unitsOD SC1mg/kgBIDSC1.5mg/kgODSC
5000unitsOD SC120u/kgBIDSC200u/kgODSC
5000uBIDorTID80u/kgbolus
followed by18u/kgMonitoring Anti-factorXa aPTT q6hours
Pharmacokinetics Renalimpairment:reducedoseby50%
Lessaccumilated inrenalimpairment
Safeinrenalimpairment&
dialysis

MaintenancetherapyWarfarin Dabigatran Rivaroxaban
Mechanismofaction
Competes withVitaminKreceptorsonthelivertoformclottingfactors
Directthrombininhibitor
Direct FactorXainhibitor
Dosing ⋍ 5mg 150mgBID 15mgBID 21daysThen,20mgOD
Monitoring INR NA NATimetopeak 5-7days 1hr,(delayedbyfood
2hrs)2-4hrs
Halflifeelimination
20-60hours 12-17Hrs(elderly:14-17hrs)
5-9Hrs(Elderly:11-13hrs)
Prolongedbyrenalimpairment

Q:FACTORMYTH?
• ApatientistobestartedononeoftheNovelAnticoagulants(NOAC)today.ThepatientneedshortactingLMWHorbridgingtherapysuchasinwarfarin
cases?FACT/MYTH
MYTH!
Novelanticoagulantsexerttheireffectimmediatelywithoutrequirementofbridgingtherapy

VTEProphylaxis

VTEinsurgery
• VenousThrombo-embolism(VTE)isacommoncomplicationofsurgery
• PEisthemostcommoncauseofpreventabledeathinhospitalizedpatientsinsurgery
• PostoperativeDVTisoftenasymptomatic
• ItissuggestedthatroutinescreeningforDVThaslowsensitivity
• VTEoccursinabout3%ofpatientsundergoingorthopedicsurgerydespiteprophylaxis (highestintotalkneeandhipsurgeries)
• IncidenceofclinicallyevidentDVTis2-5%

VTEprevalenceaftermajororthopedicsurgeryinabsenceofprophylaxis
Procedure DVTTotal PE(Fatal)
Hiparthroplasty 42-57% 0.9-28%(0.1-2%)
Kneearthroplasty 31-85% 1.5-10% (0.1-1.7%)
Hipfracturesurgery 46-60% 3-11%(2.5-7.5%)
Answer:Pleasenotethatthesenumbersarebeforetheneweraofearlyambulationofsurgicalpatients

RiskfactorclassificationforVTEformationRisklevel CalfDVT Proximal
DVTClinical PE FatalPE
LowriskMinorSurgeryinpt <40yrs noriskfactors
2% 0.4% 0.2% <0.01%
ModerateriskMinorsurgeryinpatient +additionalriskfactors40-60yr oldpatient+NOriskfactors
1—20% 2-4% 1-2% 0.1-0.4%
HighriskSurgeryin>60yr old+additionalriskfactor
20-40% 4-8% 2-4% 0.4-1%
HighestriskSurgeryinpt >40yrsmultipleriskfactorsHip/Kneearthroplasty,hipfracturesurgery
40-80% 10-20% 4-10% 0.2-5%

RiskfactorsforVTEActivecancerPreviousVTE(except superficialveinthrombosis)Reducedmobility(3foldincrease)Elderly (>70yrs)Heart FailureoranyformofrespiratoryfailureAcutemyocardialinfarctionorischemicstrokeAcute infectionorrheumatological disorderObesity(BMI>30)
Ongoinghormonal therapy(oralcontraceptive)*
Criticalillness

Othersuggestedriskfactors- SIGNNHS
FamilyHistoryofVTEVaricoseveins
Raolixifene orTamoxifene (breastcancer)
Pregnancy(10foldincrease),Puerperium(post-partum:25foldincrease)
CentralVenousCatheter(11.5foldincrease)

ProphylaxisKeypoints
• Totalhip/kneereplacementsurgeryshouldbeplacedonDVTprophylaxis• Considerextendedprophylaxisinmajorsurgeries• Allothersurgeries:basedonclinicalappraisalofthepatient’sindividualriskfactors• AspirinisnotrecommendedforDVTprophylaxis• Inpatientswithincreasedriskofbleeding:usemechanicalprophylaxis• Somearticlesrecommendedacombinationofmechanicalandpharmacological
prophylaxis• TheAustralian&NewZealandworkingpartyonthemanagementofVTErecommend
toprescribeVTEprophylaxisexceptiftherearecontraindications(thrombocytopenia,elevatedINR,hepaticdisease,activebleeding,highriskofbleeding)

AgentsusedforVTEprophylaxisEnoxaparin Dalteparin Unfractionated
Heparin(UFH)Mechanismof
actionInhibitfactorXa Inhibitantithrombin
III+factorXa
Dosing 40unitsOD SC(obese)
5000unitsOD SC 5000uBIDorTID
Monitoring Nomonitoringrequired
Pharmacokinetics Renalimpairment:30mgdailySC
Lessaccumulatedinrenalimpairment
Safeinrenalimpairment&
dialysis
MechanicalVTEprophylaxis

Q:FACTORMYTH?
• ElasticstockingisequivalenttomechanicalcompressionsinDVTprophylaxis
MYTH!
ElasticstockingsshouldNOT beusedtopreventVTE,theyareinferiortomechanicalcompressions

GUIDELINESACCP,AAOS

CHESTguidelinesrecommendationsIndication Totalhip/kneearthroplasty orHipfracturesurgery
Recommendation
VTEprophylaxisforminimum10-14days
Agents Preferredagent:LMWH, UFHLessfavored:Fondaparinux,Dabigatran,Apixaban,Warfarin(INR2.5)- increasedriskofbleedingNostrongevidence:Aspirin,Pneumaticcompression
Pneumaticcompressions
Highriskofbleeding(previousmajor bleeding,renalfailure,antiplateletagent,surgicalbleedingrisk)Compliance shouldbefor18hrsperday
Timing ForLMWH,initiate12hoursbeforesurgeryResume12-24hourspostsurgery(lessriskofbleeding)

CHESTguidelinesrecommendations
Indication Majororthopedicsurgery
Recommendation VTEprophylaxisfor35daysvs10-14days
Agents Preferredagent:LMWH, UFHLessfavored:Fondaparinux,Dabigatran,Apixaban,Warfarin(INR2.5)- increasedriskofbleedingNostrongevidence:Aspirin,Pneumaticcompression
Recommendation CombinationofpharmacologicalandmechanicalprophylaxisBasedoncochrane meta-analysis
NoncompliancetoIPCD
Dabigatran/Apixaban
Recommendation DopplerUltrasoundscreeningforpatientspostmajororthopedicsurgery

QUESTION:WHATISTHEPREFERREDVTEPROPHYLAXISAGENTBASEDONTHEGUIDELINES?
• LowMolecularWeight(Enoxaparin/Dalteparin)
• UnfractionatedHeparin
• Apixaban
• Dabigatran
• Aspirin
• Warfarin
• Fondaparinux
• Rivaroxaban
• Pneumaticcompression
Answer:LowMolecularWeightHeparin
20%reductioninDVTin favorofLMWH
Equivalent,notenoughdataaboutbleeding
Equivalent,butusedhigherdoseDab.
Comparedveryhighdose,moreDVT
LessasymptomaticDVTwithLMWH
IncreasedbleedingeFond.
Inc.riskofmajorbleeding
LessbleedingwithIPCD,non-inferior

DOSINGOFNOAC INORTHOPEDICSURGERY
Kneereplacement Hipreplacement
Dabigatran 110mggiven1-4hoursaftersurgery
110mggiven1-4hrsaftercompleting
surgeryRivaroxaban 10mgdaily
10-14 daysUpto35days
10mgdaily10-14days
upto35days

NoProphylaxis
Indication Isolatedlower leginjurythatrequiresimmobilization
Indication KneearthroscopywithnohistoryofpriorDVT

Therapeuticanticoagulationandproceduralguidelines

ANTICOAGULATION
• Anticoagulationistheprocessofbloodthinning.Thisisusedtopreventclotformationincertaindiseasessuchasatrialfibrillation,valvereplacement,thrombosis.Itisalsousedtotreatcertainconditionssuchasacutedeepvein
thrombosis,pulmonaryembolismoranyformofthrombosis.

INDICATIONSFORANTICOAGULATION
• Non-Valvular Atrialfibrillation*
• Valvular heartdiseaseandprostheticheartvalves
• Mechanicalvalvevstissuevalve
• Venousthromboembolism(DVT,PE,Otherthrombosis…)
• Inheriteddisease(proteinC,Sdeficiency)
• Autoimmunediseasesrelatedtoincreasedthromboticrisk(antiphospholipidsyndrome)

DOALLPATIENTSWITHAFREQUIREANTICOGAULATION?
• No

DECISIONTOANTICOAGULATION
RiskofthrombosisCHAD-VAS2score
RiskofbleedingHASBLEDscore

CHA2DS2-VASCSCORE
C Congestive heartfailureH Hypertension(>140/90orontherapy)A2 Age>75yearsD DiabetesS2 Priorstroke orTIAV Vasculardisease(PAD,MI,…)A Age65-75Sc Gender (Sexcategory):Female

RISKOFTHROMBOSISBASEDONCHAD2VASC2
0 01 1.3%2 2.2%3 4%5 6.7%6 9.8%7 9.6%8 12.5%9 15.2%

HAS-BLEDSCORE
H Hypertension (SBP>160) 1
A Abnormal renalfunctionAbnormalhepaticfunction
11
S Stroke: priorhistoryofstroke 1
B Bleeding:priorhistoryofmajor bleeding 1
L LabileINR(unstable)
E Elderly>65 1
D Prioralcohol,medsthancanpredisposebleeding(NSAIDs,antiplatelets)
11

INTERRUPTIONOFANTICOAGULATIONANDBRIDGINGINSURGERY
Riskofbleedinginthesurgicalprocedure Riskofthrombosis
High(especiallymechanicalvalve)*
LowHighLow
Donotinterruptanticoagulation
Interruptanticoagulation Bridging Nobridging

WARNING!
• Epiduralanaesthesia:DoNOTuseanyoftheNOACbecauseoftheincreasedriskofspinalorepiduralhematoma• Resume24hoursafterremovalofepiduralcatheter

INTERRUPTION- WARFARIN
Agent INR>3(abovetarget)*
INR2-3(therapeutic)
INR<2(sub-
therapeutic)Warfarin Discontinue>5
daysbeforesurgery
Discontinue5daysbeforesurgery
Discontinue 3-4daysbefore
surgery
CheckINR24hoursbeforesurgery

INTERRUPTION- DOAC
Agent Lowbleedingrisk(surgery) Intermediate orhighbleedingrisk(surgery)
Dabigatran Cl >80:>24hrsCl50-79:>36hrsCl30-49:>48hrsCl:15-29:>72hrs
Cl<15:Nodata>96hrs*
Cl>80:>48hrsCl50-79: >72hrsCl:30-49:>96hrsCl:15-29:>120Cl<15:Nodata
Rivaroxaban Cl>30: >24hrsCl15-29:>36hrsCl<15:Nodata,
Consideranti-Xa level
Cl>30:>48hrsCl<30:Nodata
Surgerybleedingrisk
Renalfunction

EMERGENCYSITUATION

BRIDGING


AGENTSUSEDINBRIDGING
Lowmolecularweightheparin Unfractionatedheparin
MoreconvenientMaynotrequiremonitoring Safestoptioninrenalimpairment
Monitoring:aPTT q6hrs thenq12whendoseisdetermined
RenalImpairment+Obese:MonitorantiFactorXa levels

DOSING
Enoxaparin Dalteparin UFH
Dose 1mg/kg BIDOR1.5mg/kgdaily
120u/kg BIDOR200u/kgdaily
80u/kg bolusfollowedby18u/kgadjustedbasedonapTT
RenalImpairment Reducedose50%Cl<30:MonitorDialysis: Notapproved
Lessaccumilated SAFE!
Monitoring AntifactorXa aPTT q6hrs

KEYPOINTSINBRIDGING
• WhenINR<2,initiatebridgingtherapy
• NextscheduleddoseNOAC
• HoldUFH4hoursbefore
• HoldLMWH12hrs before
• HeparinInducedthrombocytopenia:Lepirudin
• Neverinitiatewarfarininpaient withHITaslongasPLT<50

RESUMING- POSTSURGERY
• Basedonpostproceduralbleedingrisk:
• Warfarin24-48hours
• Warfarin:Bridgeifrequired(basedonCHADVASandHASBLED)
• UntilINRistherapeutic>2formorethan24hoursorafter5dayswhicheveriscloser
• NOAC:Donotbridge
• ResumeNOAC:24hrs (lowpostproceduralbleedingrisk)
• ResumeNOAC:48-72hours(Highpostproceduralbleedingrisk)

REFERENCES
• G.Agnelli,PreventionofVenousThromboembolisminSurgicalPatients.Circulation.2004;110[supplIV]:IV-4–IV-12
• CHESTguidelinesVTEprophylaxisinorthopedicsurgery2012
• AAOSguidelinesVTEprophylaxis
• ACCguidelinesforbridgingtherapyinnon-valvular AFpatients2017
• CHESTguidelinesforpreandpostproceduralanticoagulation
Recommended