
What’sNewinAllergyandImmunology
SamuelGubernick,DO,FAAAAI,FACAAI,FAAP
Interpretation of Laboratory Tests
• Positive skin prick test or food-specific IgE• Indicates presence of IgE antibody and not clinical
allergy• ~90% sensitivity; ~50% specificity• ~50% asymptomatic sensitization• Larger skin tests or higher sIgE levels correlate with
increased likelihood of allergy but not the severity• Negative skin prick test or food-specific IgE
• Essentially excludes IgE antibody (>95% specific)
SampsonHA,etal.JACI2014;134(5):1016-25.SampsonandHo.JACI1997;100:444-51.SampsonHA,JACI2001;891-96..
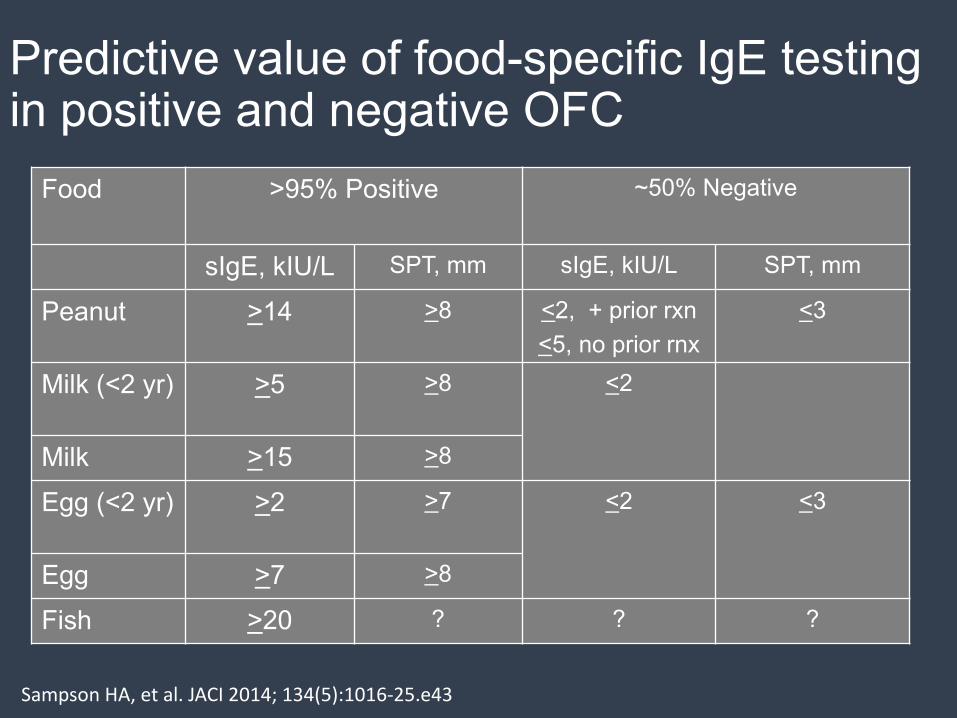
Predictive value of food-specific IgE testing in positive and negative OFC
Food >95% Positive ~50% Negative
sIgE, kIU/L SPT, mm sIgE, kIU/L SPT, mm
Peanut >14 >8 <2, + prior rxn<5, no prior rnx
<3
Milk (<2 yr) >5 >8 <2
Milk >15 >8
Egg (<2 yr) >2 >7 <2 <3
Egg >7 >8
Fish >20 ? ? ?
SampsonHA,etal.JACI2014;134(5):1016-25.e43
Molecular Diagnosis of Food Allergy• Major allergens identified in many foods• For example birch cross-reactive allergens:
• Ara h 8 in peanut and Cor a 1 in hazelnut are associated with mild oral symptoms or no symptoms at all upon ingestion.
• Storage seed proteins: • Ara h 1, 2, 3 in peanut and Cor a 9 and 14 in
hazelnut are associated with systemic reactions.
Sicherer SH,WoodRA.JACIinPractice2013;1:1-13.SampsonHA,etal.JACI2014;134(5):1016-25.e43


Egg
Ovomucoid Gald1 Heat-stableandhighlyallergenicRiskforreactiontoallformsofeggHighlevelsindicatepersistentallergy
Ovalbumin Gald2 Heat-labileMostabundanteggwhiteproteinRiskforclinicalreactiontoraworslightlyheatedegg
Conalbumin Gald3 Heat-labileRiskforclinicalreactiontoraworslightlyheatedegg
Lysozyme Gald4 RiskforclinicalreactiontoraworslightlyheatedeggLysozymeisusedasanadditiveincertainpharmaceuticalproductsandfoods
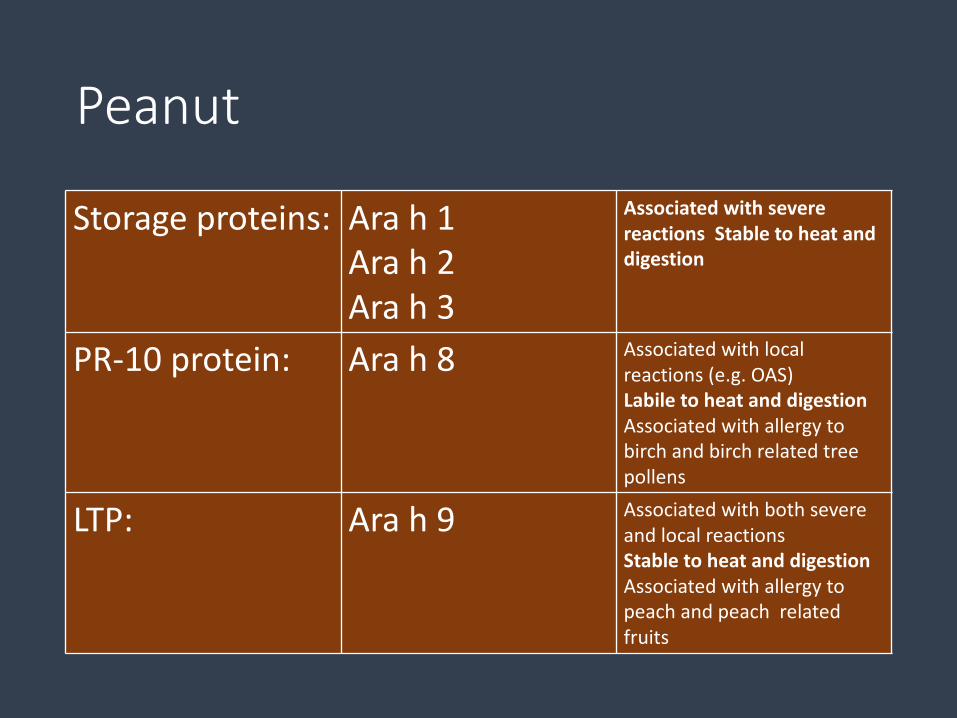
Peanut
Storageproteins: Arah1Arah2Arah3
AssociatedwithseverereactionsStabletoheatanddigestion
PR-10protein: Arah8 Associatedwithlocalreactions(e.g.OAS)LabiletoheatanddigestionAssociatedwithallergytobirchandbirchrelatedtreepollens
LTP: Arah9 AssociatedwithbothsevereandlocalreactionsStabletoheatanddigestionAssociatedwithallergytopeachandpeachrelatedfruits
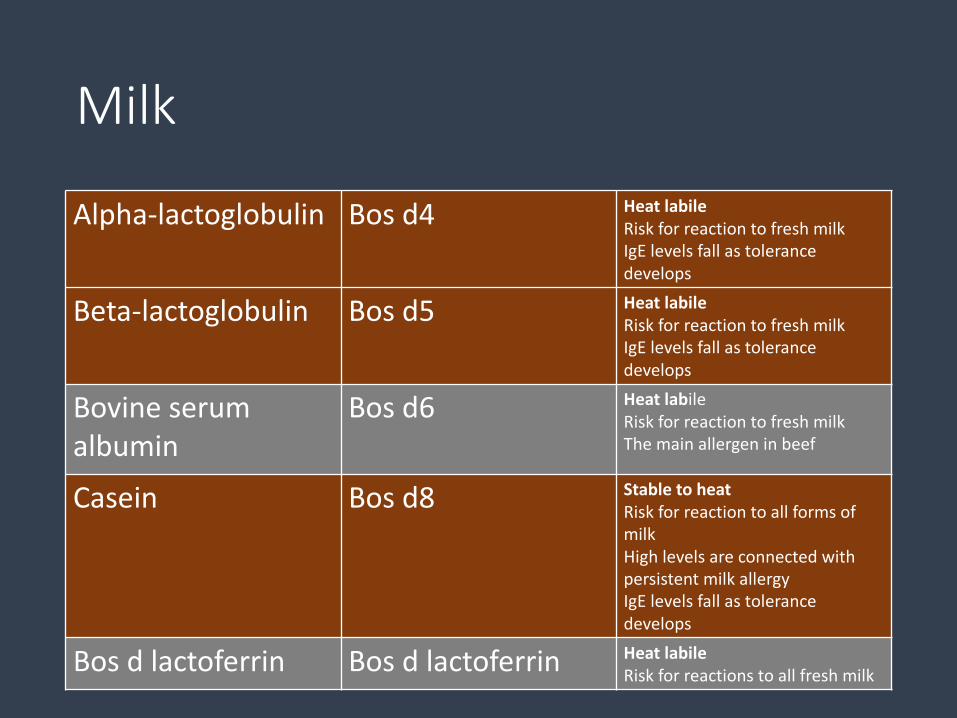
Milk
Alpha-lactoglobulin Bosd4 HeatlabileRiskforreactiontofreshmilkIgElevelsfallastolerancedevelops
Beta-lactoglobulin Bosd5 HeatlabileRiskforreactiontofreshmilkIgElevelsfallastolerancedevelops
Bovineserumalbumin
Bosd6 HeatlabileRiskforreactiontofreshmilkThemainallergeninbeef
Casein Bosd8 StabletoheatRiskforreactiontoallformsofmilkHighlevelsareconnectedwithpersistentmilkallergyIgElevelsfallastolerancedevelops
Bosdlactoferrin Bos dlactoferrin HeatlabileRiskforreactionstoallfreshmilk
RandomizedTrialofPeanutConsumptioninInfantsatRiskfor
PeanutAllergyGeorgeDuToit,M.B.,B.Ch.,GrahamRoberts,D.M.,PeterH.Sayre,M.D.,Ph.D.,HenryT.Bahnson,M.P.H.,Suzana Radulovic,M.D.,AlexandraF.Santos,M.D.,HelenA.Brough,M.B.,B.S.,DeborahPhippard,Ph.D.,MonicaBasting,M.A.,MaryFeeney,M.Sc.,R.D.,VictorTurcanu,M.D.,Ph.D.,MichelleL.Sever,M.S.P.H.,Ph.D.,MargaritaGomezLorenzo,M.D.,MarshallPlaut,M.D.,andGideonLack,M.B.,B.Ch.,for theLEAPStudyTeam*
NEJM 2015; 372:803-813 February 26, 2015
LearningEarlyAboutPeanutAllergy(LEAP)• Prevalenceofpeanutallergyhasdoubledinlast10yearsfrom1.4to3%.
• InIsrael,peanutcontainingfoodsaregiventoinfantsstartingabout7monthsofage.
• IntheUnitedKingdomchildrenarenotgivenpeanutcontainingfoodsduringtheirfirstyearoflife.
• Observationthattheprevalenceofpeanutallergywas10timeshigheramongJewishchildrenintheUKcomparedtoIsraelichildrenofsimilarancestry.
• PurposeofLEAPtrialwastodetermineifearlyintroductionofdietarypeanutcouldserveasaneffectiveprimaryandsecondarystrategyforthepreventionofpeanutallergy.

LEAPtrial
• 640infants4to11monthsoldwithsevereeczema,eggallergyorboth• Skinpricktesttopeanut• Excludedinfantswithlargepositiveskinpricktests• Participantswerestratifiedinto2cohortsbasedonSPT:
• Group1:Nomeasurablewhealaftertesting• Group2:Whealmeasuring1to4mmindiameter
• Groupswerethenrandomizedtoeitherconsumingoravoidingpeanuts• Peanutconsumptiongrouphadanopen-labelpeanutchallenge• Thosewhodidnotreactonoralchallengereceivedatleast6gofpeanutproteinperweek,distributedin3ormoremealsperweek,untiltheyreached60monthsofage.
• Evaluatedforpeanutallergyat60monthsofage
LEAPtrialdefinitions
• Severeeczemadefinedaspersistentorfrequentlyrecurringeczemacovering≥10%BSAwithtypicalmorphologyanddistributionasassessedbyahealthcareproviderandrequiringfrequentneedforprescription-strengthtopicalcorticosteroids,calcineurininhibitorsorotheranti-inflammatoryagentsdespiteappropriateuseofemollients.
• Eggallergyisdefinedasaskinpricktestwhealdiameterof3mmorgreaterwitheggwhiteextractinaninfantwithahistoryofanallergicreactiontoeggorwhohasfailedaneggoralfoodchallenge.
• FYI- 2000mgofpeanutproteinisabout9peanuts

LEAPtrialprimaryoutcome
• 530of542childreninthenegativeSPTgroupwereabletobeevaluated.Prevalenceofpeanutallergyatage5was13.7%intheavoidancegroupand1.9%intheconsumptiongroup.p<0.001,86.1%relativeriskreduction.
• All98childreninthegroupwith1-4mmwhealsontheinitialSPTwereevaluated.Prevalenceofpeanutallergyatage5was35.3%intheavoidancegroupand10.6%intheconsumptiongroup.p<0.004,70%relativeriskreduction.
LEAPConclusion
• Primarypreventiontargetspersonswhoarenotsensitizedtopeanutsandsecondarypreventiontargetsthosewhoaresensitized.
• Inthisstudy,theinterventionwaseffectiveinreducingtheprevalenceofpeanutallergyintermsofbothprimaryprevention(prevalenceof6.0%intheavoidancegroupvs.1.0%intheconsumptiongroup,P=0.008)andsecondaryprevention(33.1%vs.6.8%,P<0.001.

EffectofAvoidanceonPeanutAllergyafterEarlyPeanutConsumption
GeorgeDuToit,M.B.,B.Ch.,PeterH.Sayre,M.D.,Ph.D.,GrahamRoberts,D.M.,MichelleL.Sever,M.S.P.H.,Ph.D.,Kaitie Lawson,M.S.,HenryT.Bahnson,M.P.H.,HelenA.Brough,M.B.,B.S.,Ph.D.,AlexandraF.Santos,M.D.,Ph.D.,KristinaM.Harris,Ph.D.,Suzana Radulovic,M.D.,MonicaBasting,M.A.,VictorTurcanu,M.D.,Ph.D.,MarshallPlaut,M.D.,andGideonLack,M.B.,B.Ch.,for theImmuneToleranceNetworkLEAP-OnStudyTeam*
NEngl JMed2016;374:1435-1443April12,2016DOI:10.1056/NEJMoa1514209
LEAP-ON
• LEAP-ONevaluatedwhetherparticipantswhohadconsumedpeanutformorethanfouryearswereprotectedlong-termagainstpeanutallergywhentheystoppedeatingpeanut.
• Followed556oftheoriginal640childreninLEAP(bothconsumersandavoiders)foraone-yearperiodofpeanutavoidance.
• Thiscohortincluded274previouspeanutconsumersand282previouspeanutavoiders.
LEAP-ON
• After12monthsofpeanutavoidance,4.8%oftheoriginalpeanutconsumerswerefoundtobeallergic,comparedto18.6%oftheoriginalpeanutavoiders.
• LEAP-ONdemonstratesthatpeanutallergypreventionachievedfromearlypeanutconsumptioninat-riskinfantspersistsafteraone-yearperiodofavoidingpeanut.
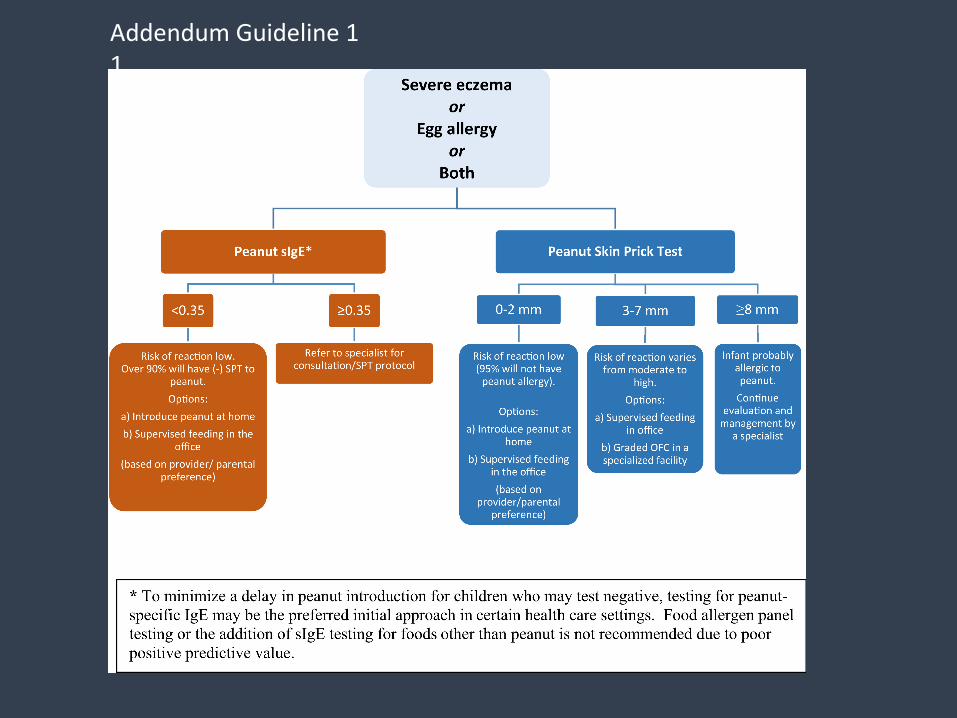
AddendumGuideline11
AddendumGuideline2
• TheEPsuggeststhatinfantswithmildtomoderateeczemashouldhaveintroductionofage-appropriatepeanut-containingfoodasearlyas4-6monthsofage,inaccordancewithfamilypreferencesandculturalpractices,toreducetheriskofpeanutallergy.
• Peanutshouldnotbetheinitialsolidfoodintroducedintoaninfant’sdiet.Othersolidfoodshouldbetriedfirsttoshowtheinfantis developmentallyready.
• TheEPrecommendsthatinfantsinthiscategorymayhavedietarypeanutintroducedathomewithoutanin-officeevaluation.However,theEPrecognizesthatsomecaregiversandhealthcareprovidersmaydesireanin-officeevaluation,inwhichcasethedecisionpointsshowninFigure1shouldapply.
AddendumGuideline3:
• TheEPrecommendsthatinfantswithouteczemaoranyfoodallergyhaveage-appropriatepeanut-containingfoodsfreelyintroducedinthediet,togetherwithothersolidfoods,andinaccordancewithfamilypreferencesandculturalpractices.
•
TheGlobalBurdenofAsthma
• 334millionpeoplehaveasthma• Annualworldwidedeathsduetoasthmahavebeenestimatedat250,000
• 14%ofworld’schildrenexperienceasthmasymptoms• 8.6%ofyoungadults(18to45yearsofage)experienceasthmasymptoms
• 4.5%ofyoungadultshavebeendiagnosedwithasthmaand/oraretakingtreatmentforasthma
• Theburdenofasthmaisgreatestforchildren10to14yearsofageandtheelderly75to79yearsofage
• Asthmaisthe14th mostimportantdisorderintheworldintermsoftheextentanddurationofdisability
GINA
AsthmaDefinitionGINA2016
• “Asthmaisaheterogeneousdisease,usuallycharacterizedbychronicairwayinflammation.Itisdefinedbythehistoryofrespiratorysymptomssuchaswheeze,shortnessofbreath,chesttightnessandcoughthatvaryovertimeandinintensity,togetherwithvariableexpiratoryairflowlimitation.”
• Clinicaldefinitionthatdoesnottakeintoaccounttheclinicalpresentationortheindividualresponsetotreatment

Thenewparadigm
• Asthmaisaheterogeneousdiseasewithmultiplephenotypesthathavevariableriskfactorsandresponsestotreatment.
• Whilemild-to-moderateasthmausuallyrespondstotraditionalmedications,severeasthmaisoftenrefractorytoICSs,LABAs,andLRAs.
• Phenotypingofasthmapatientsnowpartofthediagnosticworkupofallpatientsnotrespondingtostandardtherapy.
• Biomarkershelpdefinethespecificpathophysiologyofdifferentasthmaphenotypesandidentifypotentialtherapeutictargets.
• Anunderstandingofpatientphenotypesandendotypes andthebiologicalsusedtotargetspecificclassesofasthmaallowsforpersonalizedcaretoasthmaticpatients.
Phenotype
• Phenotype isanorganism'sexpressedphysicaltraits.• Phenotype isdeterminedbyanindividual'sgenotypeandexpressedgenes,randomgeneticvariation,andenvironmentalinfluences.
• Examplesofanindividual's phenotype includetraitssuchascolor,height,size,shape,andbehavior.
• Phenotypesalsoincludeobservablecharacteristicsthatcanbemeasuredinthelaboratory,suchaslevelsofenzymes,hormones,bloodcells,andinflammatorymediators.
Endotypes
• Newapproachtoasthmaclassificationbasedonendotypesthatrepresentspecificcellularpatternsalongwithclinicalcharacteristicswithineachpatientsubgroup.
• Analysisofinducedsputumsamplesallowsfordeterminationofinflammatoryendotypesaccordingtogranulocyticcomposition- eosinophilic,neutrophilic,mixedgranulocytic,orpaucigranulocytic.
• Patientswithsevereadult-onsetasthmacanbedividedintoaneutrophilicinflammatoryphenotypeorhaveeosinophilicinflammationthatisunresponsivetohigh-dosesteroids.
T-helpertype2-driveninflammationdefinesmajorsubphenotypes ofasthma.
WoodruffPG,Modrek B,ChoyDF,AbbasAR,Koth LL,ArronJR,Fahy JV
AmJRespir Crit Care Med.2009Sep 1;180(5):388-95
• T2asthmamediatedbyIL-4,IL-5andIL-13.• HalfofpatientswithpersistentasthmahaveT2inflammation.• MicroarrayandPCFRanalysesofairwayepithelialbrushingsfrom42patientswithmild-to-moderateasthmaand28healthycontrols.
• ClassifiedsubjectswithasthmabasedonhighorlowexpressionofIL-13-induciblegenes.
• Analyzedcytokineexpressioninbronchialbiopsies,markersofinflammationandremodeling,andresponsivenesstoICSs.
• FEV1measuredatbaseline,after4and8 weeksofdailyfluticasone(500 mgtwicedaily),and1 weekafterthestoppingfluticasone.
• FEV1responsetoICSisgreaterinType2asthmaandlittle/noneoccursinType1asthma
BiomarkersinAsthma
• FeNO values,peripheralbloodeosinophilcounts,andperiostin levelsreflectaT2inflammatoryresponse.
• Obviousoverlapbetweentheseindividualbiomarkers.• Instudiestoevaluatemepolizumab andlebrikizumab,forexample,therewereincreasesinFeNO,eosinophilcountsandperiostin levels.
• ThesemarkershaveageneralabsenceofspecificityforcomponentsofT2inflammationandarenotpreciseindefiningwhichtreatmentchoicewillbemosteffective.

FeNO
• NitricoxideisgeneratedbyairwayepitheliumandisamarkerofT2inflammation.
• Fractionalexhalednitricoxide(FeNO)measuredduringexhalationcanaidthediagnosisandmonitoringofT2asthma,differentialdiagnosisofeosinophilicasthma,predictionofresponsivenesstoICStherapy,anddifferentiatingnonadherencefrompoorresponders.
• Approximately50%ofasthmaattributedtoeosinophilicinflammation.• ThistypeofasthmaissensitivetotreatmentwithcorticosteroidsandismoststronglyassociatedwithelevatedlevelsofNO.
• Incontrast,inflammationassociatedwithneutrophilsisrelativelyresistanttocorticosteroidsandisnotassociatedwithelevatedlevelsofNO.
FeNO
• FeNO hasmanyconfoundingfactors.• TobaccosmokedecreasesFeNO values.• FeNO generallyhigherininatopicdiseasewithorwithoutasthma.• ObesehavelowerFeNO,andweightlosscanincreaseFeNO.• DemographicvariationsinFeNO.• ChildrenhavelowerFeNO valuesthanadults.• Maleshave25%higherFeNO thanfemales.• TheuseofFeNO asabiomarkerinasthmaisstillbeingevaluated.

Periostin
• Periostin involvedinmanyaspectsofallergicinflammation,suchaseosinophilrecruitment,airwayremodeling,developmentofT2phenotype,andincreasedexpressionofinflammatorymediators.
• PeriostinisinducedbyIL-13,aT2cytokine.• Serumperiostin levelssignificantlyhigherinasthmaticpatientswithevidenceofeosinophilicairwayinflammationcomparedtothosewithminimaleosinophilicairwayinflammation.
• SubsetsofasthmaticpatientshaveincreasedIL-13levelsintheirairwaysandperiostin canbeusedtoanddefineT2phenotypes.
• Lebrikizumab,amAb againstIL-13demonstratedsignificantimprovementinFEV1inpatientswithincreasedperiostin levelsandminimalimprovementinthosewithlowperiostin levels.
AllergicAsthma
• Mostcommonphenotype• 45-88%ofasthmaticpatientsinrecentstudies• Youngerpatientsandonsetatearlieragethannon-allergic• Higherprevalenceinchildren,but60-75%prevalenceinelderlyintworecentstudies
• Definedbasedonsensitizationandclinicalcorrelation• Morecommoninmales• Familyhistoryofallergiescommon• Seasonalvariationmorecommonthannon-allergicasthma• Exercise-symptomsmorefrequent/severethannon-allergic

PersistentSevereAsthma> 6y/o
Asthmarequiringtreatmentwithhighdoseinhaledcorticosteroidsplusasecondcontrollerand/orsystemiccorticosteroidsforatleast50%ofthepreviousyeartopreventitfrombecominguncontrollableorasthmathatremainsuncontrollabledespitethistherapy.
Eur Resp J2014;43-343-73
EosinophilicAsthma
• Pathologicstudiesledtothedescriptionofsubgroupsofsevereasthmaticsbasedonthepresenceorabsenceofeosinophils.
• Majorityofsevereasthmaticshadelevatedairwayeosinophilsdespitechronicuseofhigh-doseoralsteroids.
• Farfewerpatientswhodevelopedasthmaearlyinlifedemonstratedtissueeosinophilia,ascomparedwiththosewithlate-onsetasthma(36%versus63%)
• Inducedsputumeosinophilsarehigherinpatientswithmoresevereairflowobstructionandmethacholinereactivity.
SevereEosinophilicasthma
• Associatedwithincreasedseverity,lowerlungfunction,poorasthmacontrol,late-onsetdisease,exacerbationsinICSandsteroidrefractoriness.
• Oftenassociatedwithsinusitis,nasalpolypsandsometimesAERD,• Oftenlackofclinicalallergydespitepositiveskintestsin~75%.• “Fixed”airflowobstruction,reducedFVCandincreasedRV.• Inducedsputumcellcount(1%to3%invariousstudies)isthegoldstandardforidentifyingeosinophilicinflammation.
• Severalnoninvasivebiomarkers,includingperipheralbloodeosinophils,FeNO,andperiostin,arepotentialsurrogates.
• Normalizationofinducedsputumeosinophilcountsisaneffectivestrategyforpreventingsevereasthmaexacerbationsandhospitalizations.
Diagnosticevaluationofeosinophilicasthma–Peripheralbloodeosinophils
• Peripheralbloodeosinophilcountsareeasilyobtainedandwidelyavailable,butlackbothspecificityandsensitivity.
• Inasthmaticswithperipheraleosinophilia,thereisasuggestedcorrelationwithseverityofasthmasymptomsandaninversecorrelationinpulmonaryfunctionasmeasuredbyFEV1.
• HastieevaluatedmultiplevariablesincludingFeNO,FEV1,lIgE,andbloodeosinophilcountsinpredictingasthmaphenotype.• Peripheralbloodeosinophils>300/μL hadapoorpositivepredictivevalueinidentifyinganeosinophilicasthmaphenotypebasedonsputumeosinophilsof>2%.
• Peripheralbloodeosinophiliamaybeamarkerofdiseaseseverityinasthma,butdoesnotcorrelateconsistentlywithsputumeosinophilia.
HastieATetal.JACI,2013Jul;132(1):72-80

Diagnosticevaluationofeosinophilicasthma-IgE
• EosinophilicasthmacanbeassociatedwithT2-mediatedallergicdiseaseandallergensensitization,especiallyinearlieronsetdisease.
• LackofcorrelationbetweentotalIgE levelsandthepresenceofeosinophilsinBALfluidorbiopsyspecimens.
• TotalIgE haslittleutilityinevaluationofmostpatientswithasthma.
Diagnosticevaluationofeosinophilicasthma• Usingalogisticregressionmodelincludingage,sex,bodymassindex,IgE levels,bloodeosinophils,FeNO levels,andserumperiostin levelsin59patientswithsevereasthma,Jiaetalfoundserumperiostin wasthebestpredictorofairwayeosinophilia.
• Aserumperiostin level>25ng/mLhadapositivepredictivevalueof93%andanegativepredictivevalueof37%forsputumeosinophils(>3%)ortissueeosinophilia.
Jia Getal.JACI, 2012Sep;130(3):647-654.
Omalizumab
• RecombinantChinesehamsterovarycell-derivedhumanizedIgG1kmonoclonalantibody.
• BindscirculatingIgEregardlessofIgE specificity.
• PreventsbindingofIgEtoFceRI,thehighaffinityIgEreceptoronmastcellsandbasophils.
• Doesnotbindcell-boundIgEandthereforeshouldnotactivatemastcellsorbasophils.
• GivenSQ,dosebyweight,every2or4weeks
Omalizumab
• Efficacyinmoderate-severeasthma• Reductioninsymptomscores• Reductioninrescuealbuterol• Reductioninoralcorticosteroidbursts• Reductionin#exacerbations• ImprovedAMPEFR

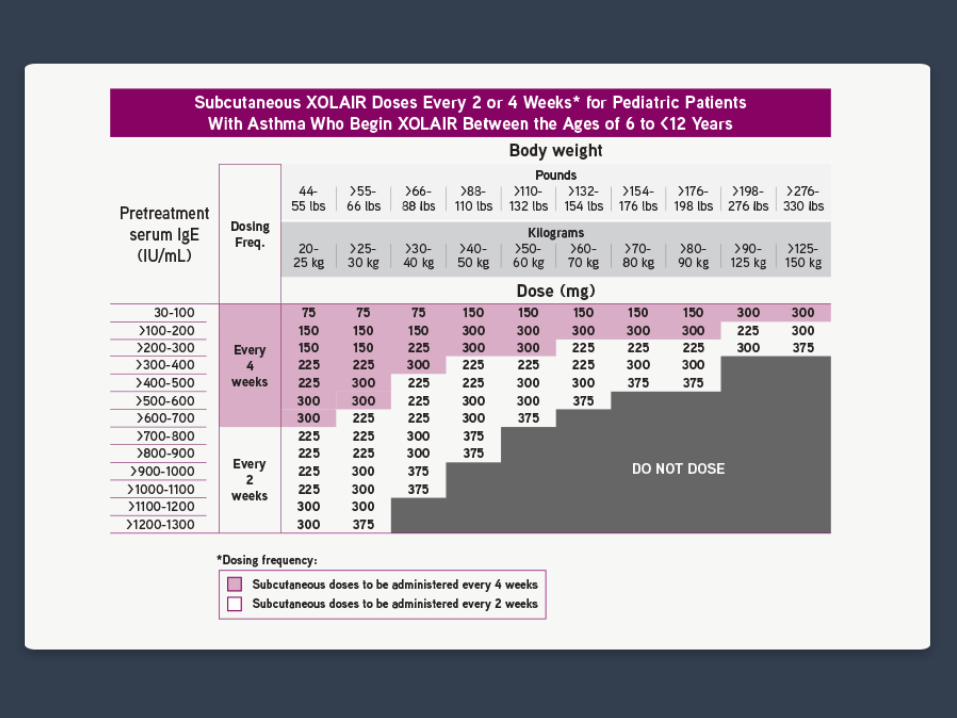
AppropriateCandidatesforAnti-IgE Therapy
• Adultsandadolescents6yearsandabove• Moderatetosevereasthma• PositiveskintestorsIgE toaperennialaeroallergen• IgEbetween30-700IU/mL• Symptomsareinadequatelycontrolledwithinhaledcorticosteroids

Pre-treatmentSerumIgE
BodyWeight
30−60kg >60−70kg >70−90kg >90−150kg ≥30−100IU/mL 150mg 150mg 150mg 300mg
>100−200IU/mL 300mg 300mg 300mg
>200−300IU/mL 300mg
>300−400IU/mL SEETABLE2
>400−500IU/mL
>500−600IU/mL
Table 1. Subcutaneous Omalizumab Dosing Every 4 Weeks for Patients 12 Years of Age and Older with Asthma
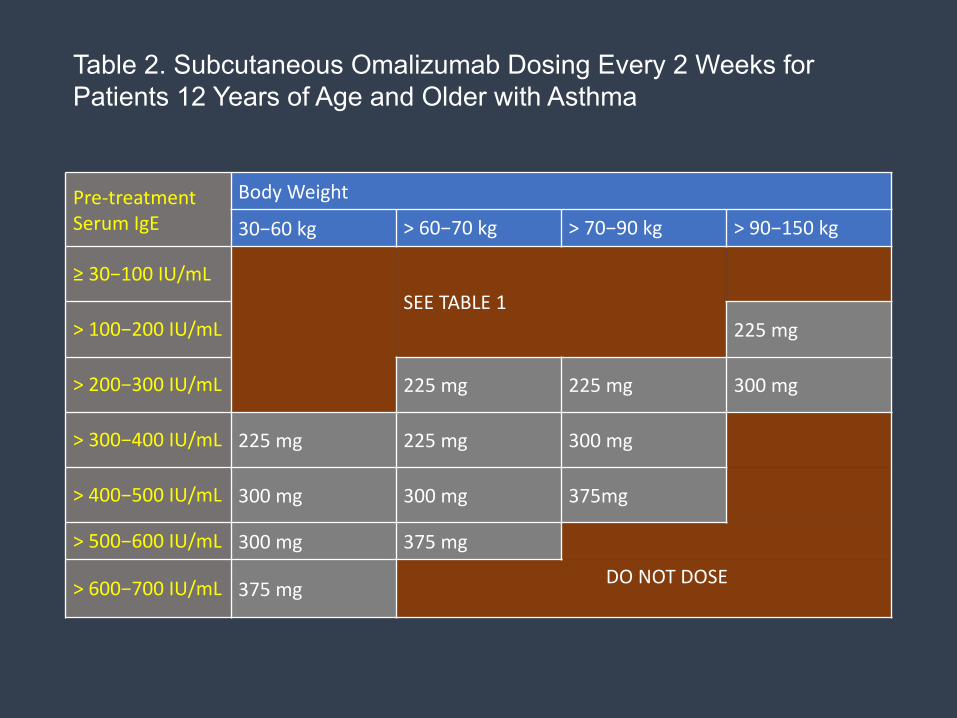
Pre-treatmentSerumIgE
BodyWeight
30−60kg >60−70kg >70−90kg >90−150kg
≥30−100IU/mL SEETABLE1
>100−200IU/mL 225mg
>200−300IU/mL 225mg 225mg 300mg
>300−400IU/mL 225mg 225mg 300mg
>400−500IU/mL 300mg 300mg 375mg
>500−600IU/mL 300mg 375mg
>600−700IU/mL 375mg DONOTDOSE
Table 2. Subcutaneous Omalizumab Dosing Every 2 Weeks for Patients 12 Years of Age and Older with Asthma

Warnings
• Anaphylaxisestimatedtobe0.1%andatleast0.2%.• AnaphylaxisoccurredwiththefirstdoseofXOLAIRin2patientsandwiththefourthdosein1patient.
• Thetimetoonsetofanaphylaxiswas90minutesafteradministrationin2patientsand2hoursafteradministrationin1patient.
• Malignantneoplasmswereobservedin20of4127(0.5%)XOLAIR-treatedpatientscomparedwith5of2236(0.2%)controlpatientsininitialstudies.
• Asubsequent5-yearobservationalstudyof5007XOLAIR-treatedand2829non- XOLAIR-treatedadolescentandadultpatientsfoundthattheincidenceratesofprimarymalignancies(per1000patientyears)weresimilarinbothgroups(12.3vs13.0).
XolairAdversereactions
• Inpatients≥12yearsofage,themostcommonlyobservedadversereactionswere:arthralgia(8%),pain(general)(7%),legpain(4%),fatigue(3%),dizziness(3%),fracture(2%),armpain(2%),pruritus(2%),dermatitis(2%),andearache(2%).
• Inpediatricpatients6to<12yearsofage,themostcommonlyobservedadversereactionswere:nasopharyngitis,headache,fever,upperabdominalpain,streptococcalpharyngitis,otitismedia,viralgastroenteritis,arthropodbite,andepistaxis.
IL-5
• Recruitment,granulematuration,andsurvivalofeosinophilsintheairwaysarepromotedbyIL-3,GM-CSF,andespeciallyIL-5.
• IL-5isproducedbyCD4+Th2cells,mastcells,eosinophils,andbasophils.
• MainbiologicalroleofIL-5istocontrolproliferation,differentiation,andactivationofeosinophils.
• ItalsostimulatesthefinaldifferentiationofactivatedBcellsintoantibody-formingcells.
• RepresentafunctionallinkbetweenT-cellactivationandinflammatoryresponsesmediatedbyeosinophils.
EosinophilFunctions
• Antiparasitic - especiallyagainsthelminthsinthelarvalstage• Antiviral• Antibacterial- actsasAPC,generationofcytokinesandchemokinesandphagocytosisofintracellularbacteriasuchasmycobacterium
• Eosinophilscanbeefficientinhostdefenseagainstgram-negativebacteriaandoxygen-dependentkilling,i.e.,superoxideactinginconjunctionwithEPO,maybethemostimportantbactericidaleffectorfunctionofthesecells.Importantatmucosalinterfacesandinthemucosaof,forexample,thelargeintestine,wheretheconditionsareaerobic.
• Staphaureus,E.coli,Pseudomonas

Mepolizumab
• Mepolizumabwasthefirstanti-IL-5moleculedesignedandtestedinforeosinophilicasthma.
• Nucala (mepolizumab)isahumanizedIgG1kappamonoclonalantibodywhichbindstosolubleinterleukin-5(IL-5),preventingitsbindingtothealphachainoftheIL-5receptorcomplexexpressedontheeosinophilcellsurface.
Mepolizumab
• Indication:• Asadd-onmaintenancetreatmentofadultpatientswithsevereeosinophilicasthmawhoareinadequatelycontrolledwithhigh-doseinhaledcorticosteroidsandanadditionalasthmacontroller,andhaveabloodeosinophilcountof≥150cells/μL atinitiationoftreatmentwithmepolizumab OR≥300cells/μL inthepast12months.
• Dosage:• Afixeddoseof100mgmepolizumab (Nucala™)bysubcutaneousinjectionevery4weeks.
MepolizumabTreatmentinPatientswithSevereEosinophilicAsthma
HectorG.Ortega,M.D.,Sc.D.,MarkC.Liu,M.D.,IanD.Pavord,D.M.,GuyG.Brusselle,M.D.,J.MarkFitzGerald,M.D.,AlfredoChetta,M.D.,MarcHumbert,M.D.,Ph.D.,LynnE.Katz,Pharm.D.,OliverN.Keene,M.Sc.,StevenW.Yancey,M.Sc.,andPascalChanez,M.D.,Ph.D.,for theMENSAInvestigators*
NEngl JMed2014;371:1198-1207

ClinicalTrials:ExacerbationStudy(MENSA)
• A32-week,multicenter,randomized,DBPCparallel-groupstudyevaluatingtheefficacyandsafetyofmepolizumab100 mgSCandmepolizumab 75mgIVvsplacebointheadd-ontreatmentofsevereeosinophilicasthma(N=576).
• Primaryendpoint:• Annualizedfrequencyofclinicallysignificantexacerbations.
• Secondary endpoints:• AnnualizedfrequencyofexacerbationsrequiringhospitalizationorERvisit
• Changefrombaselineinlungfunctionatweek32.• Changefrombaselineinhealth-relatedQOLatweek32.
MENSA
• Inclusioncriteria:• Historyof≥2asthmaexacerbationsinthepastyear• Peripheralbloodeosinophils≥150cells/µLwithin6weeksoffirstdose,or≥300 cells/µLwithinpastyear
• Regularuseofhigh-doseICSplusanadditionalcontrollerwithorwithoutOCS
• Backgroundtherapy:• Allpatientsreceivedmaintenancetherapypriortoandduringthestudy,whichconsistedofhigh-doseICSplusadditionalcontroller(s),withorwithoutOCS

Results
• Efficacyresults: Exacerbations• Mepolizumab100mgSCsignificantlyreducedthefrequencyofclinicallysignificantexacerbationsvs.placebo.
• Mepolizumab100mgSCalsosignificantlyreducedthefrequencyofclinicallysignificantexacerbationsrequiringhospitalizationsand/orERvisitsby61% vs.placebo.
• Themeanchangefrombaselineinpre-bronchodilatorFEV1was183mLwithmepolizumab vs.86mLwithplaceboatweek32.
• Resultsfromclusteranalysis• Largermepolizumab treatmentresponseinclusterswithbloodeosinophillevelsof150cells/μl orgreater,withthelargesttreatmentresponseseeninobesepatientswithmorecomorbiditiesandairwayreversibility.

ClusterAnalysisandCharacterizationofResponsetoMepolizumab.AStepClosertoPersonalizedMedicineforPatientswithSevereAsthma
HectorOrtega,Hao Li,RobertSuruki,FrankAlbers,DavidGordonandStevenYancey
AnnAmThorac Soc Vol 11,No7,pp 1011–1017,Sep 2014
• ExamineddatasetfromtheDoseRangingEfficacyAndsafetywithMepolizumab(DREAM)studywiththespecificobjectiveofidentifyingclustersofdataassociatedwithexacerbationratesasobtainedbymepolizumab treatment.
• Baselinecovariatesconsideredforinclusionwereregion,sex,age,weight,numberofexacerbationsintheyearbeforethestudy,useofmaintenanceoralcorticosteroids,percentpredictedFEV1,airwayreversibility,bloodeosinophilcount,andIgE levels.

• Higherlevelsofbloodeosinophilsandgreaternumberofpreviousexacerbationsatbaselineledtogreaterreductioninexacerbationswithmepolizumab.
• Forthemajorityofpatientswithelevatedeosinophils,bloodeosinophilcountisthebiomarkerofchoiceforpredictingtreatmentoutcomewithmepolizumab insevereasthma.
• Therewasalargermepolizumab treatmentresponseinclusterswithbloodeosinophillevelsof150cells/μl orgreater,withthelargesttreatmentresponseseeninobesepatientswithmorecomorbiditiesandairwayreversibility.
Oralglucocorticoid-sparingeffectofmepolizumab ineosinophilicasthma
BelEH,WenzelSE,ThompsonPJ,Prazma CM,KeeneON,YanceySW,OrtegaHG,Pavord ID;SIRIUSInvestigators.
NEngl JMed.2014Sep 25;371(13):1189-97
ClinicalTrials:OralCorticosteroidReductionStudy(SIRIUS)
• A24-week,multicenter,randomized,DBPCparallel-groupstudythatevaluatedtheefficacyandsafetyofmepolizumab vs.placeboonreducingtherequirementformaintenanceoralcorticosteroids,whilemaintainingasthmacontrol,inpatientswithsevereeosinophilicasthma(N=135).
• PrimaryEndpoint• PercentreductionofOCSdoseoverWeeks20-24comparedwiththedoseofOCSestablishedduringtherun-in/optimizationphase.
SIRIUS
• Selectinclusioncriteria:• Peripheralbloodeosinophil≥150cells/uL inthe6weekspriortofirstdose,or≥300cells/uL intheprevious12months
• Regularuseofhigh-doseICSplusadditionalcontroller(s)• RegularmaintenancetreatmentwithOCS
• Backgroundtherapy:• Priortothestudy,patientswereonhigh-doseICSplusanadditionalcontroller(s)withOCS(5-35mg/dayprednisoneorequivalent)
• Duringa3- to8-weekrun-inphase,theOCSdosewasadjustedweeklytoestablishthelowestpossibleOCSdoserequiredtomaintainasthmacontrol.
• Afterrandomization,theOCSdosewasreducedevery4 weeksbetweenWeeks4-20untilzero,orthelowestdoserequiredtomaintainasthmacontrol.NofurtherOCSdoseadjustmentsweremadeafterWeek20.

AtWeek20-24(secondaryendpoints):
• 54%(37/69)ofmepolizumab patientsachieveda ≥50%reductioninthedailyOCSdose vs.33%(22/66)onplacebo.
• 54%(37/69)ofmepolizumab patientsachieveda reductioninthedailyOCSdoseto≤5mg vs.32%(21/66)onplacebo.
• 14% (10/69)ofpatientsonmepolizumab 100 mgSCachieveda total(100%)reduction indailyOCSdoseto0mgvs.8%(5/66)onplacebo.
Mepolizumab AdverseReactions
• Headache,pharyngitis,lowerrespiratorytractinfection,urinarytractinfection,nasalcongestion,upperabdominalpain,eczema,backpain,pyrexiaandinjectionsitereactions
• Acuteanddelayedsystemicreactions,includinghypersensitivityreactions
• Parasiticinfections• HerpesZoster- considervaricellavaccination

Reslizumab
• Reslizumab (Cinqair)isaninterleukin-5antagonistmonoclonalantibody(IgG4kappa)indicatedforadd-onmaintenancetreatmentofpatientswithsevereasthmaaged18yearsandolder,andwithaneosinophilicphenotype.
• Reslizumab bindstoIL-5inhibitingthebioactivityofIL-5byblockingitsbindingtothealphachainoftheIL-5receptorcomplexexpressedontheeosinophilsurface.
ReslizumabDosing
• Reslizumab (CINQAIR)isforintravenousinfusiononly.
• Reslizumab (CINQAIR)shouldbeadministeredinahealthcaresettingbyahealthcareprofessionalpreparedtomanageanaphylaxis
• Recommendeddosageregimenis3mg/kgevery4weeksbyIVinfusionover20-50minutes

ReslizumabforInadequatelyControlledAsthmaWithElevatedBloodEosinophilLevels :A
RandomizedPhase3Study
LeifBjermer,CatherineLemiere,JorgeMaspero,SivanWeiss,JamesZangrilli,MatthewGerminaro
ChestVolume150,Issue4,October2016,Pages789–798
Rezlizumab
• Patientsaged12to75yearswithasthmainadequatelycontrolledbyatleastamedium-doseICSandwithabloodeosinophilcount> 400.
• Of1,025screenedpatients,315wererandomlyassignedtotreatmentand265completedthestudy.
• Randomizedtoreceivereslizumab 0.3mg/kgor3.0mg/kgorplaceboadministeredonceevery4weeksfor16weeks.
• Primaryendpointwaschangefrombaselineinpre-bronchodilatorFEV1over16weeks.
• SecondaryendpointsincludedFVC,FEF25%-75%,patient-reportedcontrolofasthmasymptoms,SABAuse,bloodeosinophillevels,andsafety.
• ReslizumabsignificantlyimprovedFEV1inthetreatmentgroups.115mlinthe0.3mg/kggroupand160mlinthe3.0mg/kggroup.
• IncreasesinFVC(130mL)andFEF25%-75%(233mL/s)wereobservedwithreslizumab 3.0mg/kg.
• ReslizumabimprovedscoresontheAsthmaControlQuestionnaire(ACQ)andAsthmaQualityofLifeQuestionnaire(AQLQ)vsplacebo.
• SABAusedecreasedwithreslizumab.• 3.0-mg/kgdoseofreslizumab providedgreaterimprovementsinasthmaoutcomesvsthe0.3-mg/kgdose,withcomparablesafety.
• Mostcommonadverseeventswereworseningofasthma,headache,andnasopharyngitis.
Reslizumabforinadequatelycontrolledasthmawithelevatedbloodeosinophilcounts: resultsfromtwomulticentre,parallel,double-blind,randomised,
placebo-controlled,phase3trials.
MarioCastro,JamesZangrill,MichaelWechsler,EricDBateman,GuyGBrusselle,PhilipBarden,KevinMurphy,JorgeFMaspero,ChristopherO’Brien,StephanieKorn
LancetRespir Med, 2015May;3(5):355-66
Reslizumab
• Of2597patientsscreened,953wererandomlyassignedtoreceiveeitherreslizumab (n=477orplacebo(n=476).
• Inbothstudies,patientsreceivingreslizumab hadasignificantreductioninthefrequencyofasthmaexacerbations.
• Study1:rateratio[RR]0·50[95%CI0·37-0·67]• Study2:0·41[0·28-0·59]• Bothp<0·0001)comparedtoplacebogroup.
• Commonadverseeventsonreslizumab weresimilartoplacebo.• Themostcommonadverseeventswereworseningasthmasymptoms,URIs,andnasopharyngitis.
• Twopatientsinthereslizumab grouphadanaphylacticreactions.Bothrespondedtostandardtreatment.
Reslizumab (Cinqair)
• Anaphylaxishasbeenobservedin0.3%ofpatientsinplacebo-controlledclinicalstudies.
• Anaphylaxiswasreportedasearlyastheseconddose.• Inplacebo-controlledclinicalstudies,6/1028(0.6%)patientsreceiving3mg/kgCINQAIRhadatleast1malignantneoplasmreportedcomparedto2/730(0.3%)patientsintheplacebogroup.
• Eosinophilsmaybeinvolvedintheimmunologicalresponsetosomeparasitic(helminth)infections.Treatpatientswithpre-existinghelminthinfectionsbeforeinitiatingCINQAIR.IfpatientsbecomeinfectedwhilereceivingtreatmentwithCINQAIRanddonotrespondtoanti-helminthtreatment,discontinuetreatmentwithCINQAIRuntilinfectionresolves.
CPKelevationsandmuscle-relatedadversereactions• ElevatedbaselineCPKwasmorefrequentinpatientsrandomizedtoCINQAIR(14%)versusplacebo(9%).
• TransientCPKelevationsinpatientswithnormalbaselineCPKvalueswereobservedmorefrequentlywithCINQAIR(20%)versusplacebo(18%).
• CPKelevations>10xULNwere0.8%intheCINQAIRgroupcomparedto0.4%intheplacebogroup.
• CPKelevations>10xULNwereasymptomaticanddidnotleadtotreatmentdiscontinuation.
• Myalgiawasreportedin1%(10/1028)ofpatientsintheCINQAIR3mg/kggroupcomparedto0.5%(4/730)ofpatientsintheplacebogroup.
• Onthedayofinfusion,musculoskeletaladversereactionswerereportedin2.2%and1.5%ofpatientstreatedwithCINQAIR3mg/kgandplacebo,respectively.
• Thesereactionsincluded(butwerenotlimitedto)musculoskeletalchestpain,neckpain,musclespasms,extremitypain,musclefatigue,andmusculoskeletalpain.
•
Recommended

















