Embed Size (px)
Citation preview

THEME: PROTECTING THE VULNERABLE
Providing Social welfare to Informal sector workers
SHRAMIK SURAKSHA YOJNA
Medical cum Life Insurance scheme
Kushagra Tiwari Pratyush Pandey Anshuman Tripathi Saurabh Biyani Alok Ratre
INDIAN INSTITUTE OF TECHNOLOGY, ROORKEE

UNORGANISED SECTOR Characteristics about the Unorganized sector: Contributions to National Product and Net Domestic Product: • 92 % of the total work force
in the country are employed in the unorganized sector.
• 370 million form the workforce of the unorganized sector.
• Over 60 % share as per current price in NDP.
• Contribute significantly to national product.
Contribution to savings and capital formation: • Sharing of only household
sector in total gross domestic saving mainly unorganized sector is about three-fourth.
• More than 30 % of the national income comes from unorganized sector.
What can be done for this sector: • Government has formed national
commission to address peculiar issues of this sector.
• Mainly working on Social Security-recently approved 1000 cr. for this.
• Adopted a concept of growth pole to link this sector with organized sector.
• Availability of capital for this sector. • Introduction of Health Insurance
AIM:
To propose an umbrella legislation for workers in the unorganised sector that will assure at least a minimum protection and welfare to workers in the unorganised sector.
Causes of problem: • There is a total lack of job security and social
security benefits.
• The areas of exploitation are high, resulting in long hours, unsatisfactory work conditions, and occupational health hazards.
• They are Daily wage earners, piece-rate workers who are engaged in a variety of occupations or employments, victims of invisibility, themselves are un- conscious of the laws, risking of finance capital by self migrants.
• NO effective means to implement, monitor and provide quick redress.
0
50
100
150Organized vs Unorganized
Sector
Unorganized Sector Organized Sector
1

Scheme for Rag Picker
Over 5 million people in India engaged in waste collection
• Waste picking • Sorting • Recycling • Door to door collection
DIRTY PICTURE Rag pickers are individuals with no rights. They have a difficult life, working hard to clean the cities. They recycle wastes that they collect. They are mostly ignored by the government and are harassed by the police, even being put into jail for no reason.
REASON FOR SELECTING THIS SECTION • We must recognize the useful
role played by the scrap collectors both in helping recycling activities as well as in maintaining Civic hygiene.
• Most of the employed workers are women and children .
• It is, therefore, essential that they should be protected from insecurity of various forms.
RAG PICKERS (50 LAKH) 2

INNOVATIVE SOLUTION
Providing medical cum life insurance against the occupational hazards, associated with work (lets start with ragpickers).
Medical cum life insurance.
Implementation model
Advantage over existing system
• Low cost insurance. • Covers occupational diseases stated by the National Institute Of Occupational
Health (NIOH). • Money transferred to account connected with smart card.
• Beneficiaries are identified by Municipal Corporation. • Biometric enabled smart card issued by the Post Office. • Nodal body of the scheme is National Association for Enterprises in unorganized
Sector. • Empanelment of hospitals as decided by nodal body and insurance company. • Claim settlement by the insurance company delivered by Post Office.
• Nothing substantial existing before the scheme. • Use of technology to ensure easy, fast and transparent
transfer of benefits. 3

PUBLIC-PRIVATE PARTNERSHIP
VALUE PROPOSITON
ACCESS
TECHNOLOGY PLATFORM
State Nodal Agencies (SNAs) facilitate the implementation and
monitoring of scheme
The insurance company provides
provides the outpatient benefits
Providers are empanelled according
to Geographical area to ascertain their
accessibility
Development of the outpatient specific
software that works online or offline mode
Government platform with specific tasks being managed by
private parties
Risk pooling is through health
insurance for outpatient care
Beneficiaries can exercise choice to visit any of the empanelled
hospital or medical shops
For authentication and verification of the
enrolled Smart card to enable cashless treatments
Implementation of the solution
4
Basic Features of Scheme
Identification Enrolment
Utilisation of Services
Claim settlement
By municipal corporation by issuing certificate/bonafide.
Issue biometric enabled smart card by post office by conducting camps and collecting fee.
• By utilising the participating hospitals and receive medical aid upon diagnosis.
• Annual health care checkup.
Life insurance claim could be collected through post office upon production of death certificate and submission of smart card.

Stakeholders
4
Government NAEUS Municipal Corporation
Post Office Insurance Company
Healthcare Providers
Rationale for choosing the group
• Basic Funding Agency
• Nodal agency
• Occupation Data
• Ward level worker
• Large network
• Experience • Postman
can help deliver message
• Provides health cover bearing risks.
• Network of hospitals
• Group of hospitals, dispensaries and medical shops.
Work • Provide funds
• Manage data bank
• Overall functionality
• Issue certificate/bonafide to identify
• Issue smart card
• Deals with money transactions
• Provide Insurance product
• Bear risk and claims
Provide health care facility.
Benefits to players
• Achieves goal of social security
• Gets data
• Creates data bank and gets actual number of workers, trends of shifts in jobs
• Additional funding to run offices, as revenues are already crunched
• Additional funding
• Rejuvenates postal bank services suffering from onset of LPG
• Profit making
• Revenue • Job
satisfaction
5

Insurance Company
State Nodal Agency
Health Care Providers
MUNICIPAL CORP.
Beneficiaries
Government of India
POST OFFICE
4. Selection through tendering
7. In
form
ation
an
d c
erification
12. Submission of data and bill
13. Payment to Insurer
6
13
. L
ife
In
su
ran
ce
Cla
im P
roce
ss
Organisation Flow Chart
Awareness Health Camps
8. Enrollment
14. Life Insurance Claim
3. Assistance
Call Center
DATA

Setting Up of Nodal Agency
– Develop a full time team for State Nodal Agency with some experts in Data Analysis ,IT etc
– Strengthen capacity of Post Office and Municipal corp. by training
– Hire District Coordinators eg. NGOs
– Establishing Grievances Redressal system
Primary Stage Role of Nodal Agency
• Setting of State Server require for storing data
• Get the data of eligible candidates from Census and related agencies
• Provide Training to the field officers involved in the process.
• Receive data of other eligible categories from field-officers and NGOs
• Process and analyse Data .
Basic Role of Nodal Agency
• Empanelment of Insurance Agency
• Receive enrolment data from Insurer and OPD data directly from the Health Providers
• Analyse this data on a regular basis
• Prepare monthly report based on data analysis.
• Monitoring- Fraud Detection and Control
Empanelment of
Insurance Agency
– Selection Through Competitive Bidding
– Strengthen capacity of Post Office and Municipal corp. by training
– Hire District Coordinators eg. NGOs
Primary Stage Role of Insurance Agency
Empanel the Healthcare Providers (hospitals, clinics and medical shops) and sign MoUs
Upload their details and providing them with necessary hardware
Train all providers with the new software
Basic Role of Insurance Agency
• Organise Awareness Campaign
• Receive data directly from the Health Providers and provide claim
• Provide Call Center Fascility
• Monitoring- Fraud Detection and Control
Required Resources
7
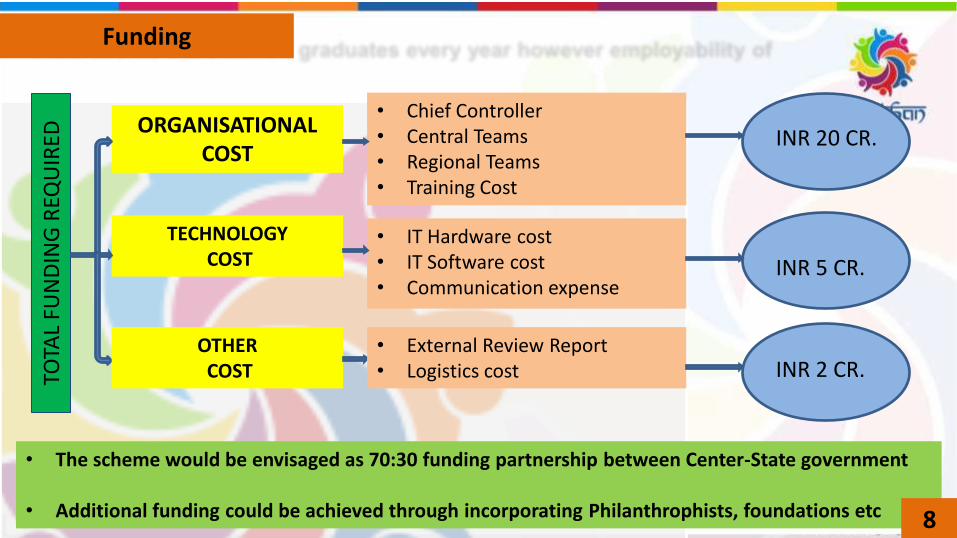
• The scheme would be envisaged as 70:30 funding partnership between Center-State government
• Additional funding could be achieved through incorporating Philanthrophists, foundations etc
Funding
8
TOTA
L FU
ND
ING
REQ
UIR
ED
ORGANISATIONAL COST
TECHNOLOGY COST
• Chief Controller • Central Teams • Regional Teams • Training Cost
• IT Hardware cost • IT Software cost • Communication expense
OTHER COST
• External Review Report • Logistics cost
INR 5 CR.
INR 2 CR.
INR 20 CR.

Measurement
Quantitative and Qualitative study covering all stake holder involved in process.
Inviting reputed organisations/agencies having experience of preparing evaluation studies for government schemes. Responsibility of Research Agency: • Developing Research instruments, after
consulting with nodal agency • Selection of experienced field workers. • Providing adequate training to its field
workers by providing complete background ,topic areas, protocols.
• Data collection and Data Management • Quality Assurance data monitoring on
daily basis on field and during compilation of raw data.
• Data analysis and Report Writing
Impact of solution Scalability
Total Number of Beneficiaries is 50 lakh. Additional 20 lakh if labourers in scrap establishments and reprocessing units included PHASE 1: PUNE (5,000) PHASE 2: DELHI (1,50,000) PHASE 3: Pan India (50,00,000)
Sustainability • These preventive health care measures can
reduce the possibility of disease and lead to fewer future medication.
• Gradually including the people of upper strata in this segment(kabadis,thailawala) risk pooling can be greatly increased to make the system sustainable.
• Another alternative is to offer lifelong insurance coverage, so inter-temporal risk pooling would take place thereby, low incidences of diseases at a young age would be offset by high incidences at an older age.
Monitoring and Fraud Detection - Control
State Nodal Agency • Analyse the data on a regular basis • Visit to the hospitals based on data
analysis • Provide support to the Insurance
Company as and when needed for this purpose
Insurance Company • Daily transaction data from hospitals
should be monitored very closely to identify patterns/ trends
• Triggers/ filters etc. shall be built into software for early detection
• Strict action should be taken against errant hospitals however, good hospitals should be nurtured
• Steps to be taken after de-empanelment are defined in revised advisory for de-empanelment
• SNA should be kept in confidence for actions against hospitals
9

Action area • Provider
activation
• Technology
• Awareness
• Availability and cost of drugs
• Reviews • Claims and
Reimbursement
Issues and Challenges o Lack of co-ordination among the local authorities o not actively claiming public facilities; inadequate
provider density
o Evaluating technology platform to make it user-friendly for smooth functioning
o Ocurrence of technology issues eg. Compatibility of softwares
o Misconception among beneficiaries
o Addressing the high incidence of cost for drugs prescribed
o Need for improving communication between various partners
o Challenges in settlement with providers
Implementing Steps
Extensive field visits to gain first-hand understanding of the ground realities and identification of gaps
Meetings held with the nodal agency
Regular upgrades required based on the feedback Troubleshooting support ( reinstallation of software
and ensuring it is operational) Hands-on training on the software
Interaction held with beneficiaries/community
through participation sector-level meetings Other activities for generating mass awareness
Supply and storage of Janaushadhi medicines Field teams trying to encourage prescription of
Janaushadhi medicines
Follow up visits undertaken to share developments and issues for resolution
Better documentation of terms and conditions Providers directed to deduct tax at source
Challenges and Risks
10
• Report of National Commission on Labour 2(Chapter 7 unorganised sector Part A)
• National Commission on Self-Employed Women, 1988 under the Chairpersonship of Smt. Ela R. Bhatt, included in their terms of reference, the women workers in the unorganised sector SHRAMSHAKTI REPORT):
• NCAER-SEWA (National Council for Applied Economic Research and Self-Employed Women’s Association) workshop March-April 1997
• Brazilian ragpickers by M C da Silva, A G Fassa, C E Siqueira, D Kriebel , Federal University of Pelotas, Brazil
• Report on Child Rag-pickers by NGO PRATHAM
References



![Pensacola Journal. (Pensacola, Florida) 1907-05-09 [p 2].ufdcimages.uflib.ufl.edu/UF/00/07/59/11/00846/00300.pdf · odawater1JJarfJCl BlueRibbon iHizt TRAMIVIELLS Gerunna FRANCHISE](https://img.pdfslide.net/doc/110x75/5e86fbe35f34d64de858df6f/pensacola-journal-pensacola-florida-1907-05-09-p-2-odawater1jjarfjcl-blueribbon.jpg)



