Embed Size (px)
Citation preview

Author(s): Rebecca W. Van Dyke, M.D., 2012
License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution – Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. The citation key on the following slide provides information about how you may share and adapt this material.
Copyright holders of content included in this material should contact [email protected] with any questions, corrections, or clarification regarding the use of content.
For more information about how to cite these materials visit http://open.umich.edu/education/about/terms-of-use.
Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition.
Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers.

Attribution Keyfor more information see: http://open.umich.edu/wiki/AttributionPolicy
Use + Share + Adapt
Make Your Own Assessment
Creative Commons – Attribution License
Creative Commons – Attribution Share Alike License
Creative Commons – Attribution Noncommercial License
Creative Commons – Attribution Noncommercial Share Alike License
GNU – Free Documentation License
Creative Commons – Zero Waiver
Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in your jurisdiction may differ
Public Domain – Expired: Works that are no longer protected due to an expired copyright term.
Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105)
Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain.
Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ
Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair.
To use this content you should do your own independent analysis to determine whether or not your use will be Fair.
{ Content the copyright holder, author, or law permits you to use, share and adapt. }
{ Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. }
{ Content Open.Michigan has used under a Fair Use determination. }

M2 GI Sequence
Cholestatic Liver Diseases
Rebecca W. Van Dyke, MD
Winter 2012

Learning Objectives
• At the end of this lecture the student should be able to:
• • 1. Define cholestatic and hepatocellular liver disease, provide examples of both
and be able to interpret panels of liver tests.• • 2. Define the difference between intrahepatic and extrahepatic cholestasis and
outline approaches to distinguishing them.• • 3. Define the pathophysiology of representative cholestatic diseases, including
drug-induced cholestasis, primary biliary cirrhosis, primary sclerosing cholangitis and bile duct obstruction.
• • 4. Outline an approach to the evaluation of the jaundiced patient.• • 5. Define acute and chronic hepatocellular liver disease and provide
representative examples.

Industry Relationship Disclosures
Industry Supported Research and Outside Relationships
• None

Common Types of Liver Disease
Hepatocellular: Injury to hepatocytes (necrosis/apoptosis) Consequences:
decreased synthetic/metabolic activityrelease of intracellular contents (AST/ALT)
Cholestasis: Impaired bile formation (hepatocytes)Impaired bile flow (bile ducts/ductules) Consequences:
build up in blood of substances normally excreted in bile (bilirubin, bile acids)
synthesis/release of apical membrane proteins (AP)

Cholestasis =impaired bileflow
Structuresinvolved insecretion andpassage of bile

Cholestatic Liver Disease
Classification of cholestatic diseases:
1. A functional impairment in bile formation at the level of the hepatocyte.
2. A structural interference with normal bile secretion and flow at the level of small intrahepatic bile ducts.
3. A structural interference with normal bile flow at the level of large and extrahepatic bile ducts.

Cholestatic Liver Disease
Biochemical cholestasis: increased serum bilirubinincreased serum alkaline phosphatase
Clinical cholestasis: jaundicedark urine/clay-colored fecespruritus
Pathological cholestasis: bile plugs in dilated canaliculiincreased bile pigment in hepatocytesbile lakes/bile infarctsbiliary infection (acute cholangitis)

Tests for Evaluating Cholestasis
• Screening tests that suggest cholestasis– Color change in skin/sclerae/stool/urine– Laboratory biochemical tests (Alk Phos, Bilirubin)
• Diagnostic tests to establish proof of disease– Liver biopsy– Indirect visualization of dilated bile ducts and/or masses
compressing bile ducts/stones (CT, U/S)– Direct visualization of lumen of bile ducts allowing
identification of plumbing problems • ERCP - endoscopic retrograde cholangiopancreatography• MRCP - magnetic resonance cholangiopancreatography

Jaundice: Consequence of Cholestasis

Hypercarotenemia (hand on the right) – the only other potential disease in the
differential diagnosis of yellow skin

Clinical Consequences of Severe Cholestasis: 1. Clay-colored stools 2. Bilirubin in urine

Cholestasis: Specific Examples
1. Intrahepatic cholestasis due to decreased bile formation:SepsisEstrogens
2. Intrahepatic cholestasis due to diseases that alter intrahepatic bile ducts:
Primary biliary cirrhosisInfiltration of liver with tumor/granulomas
3. Intrahepatic cholestasis due to any severe liver disease:Viral hepatitis
4. Extrahepatic bile duct obstruction:Tumor, gallstones, duct stricturesPrimary sclerosing cholangitis

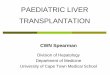
Cholestasis:Specific Abnormalities in Bile Formation
Transporters involved in uptake and biliary secretion of bilirubin and/or bile acids may be inhibited by various agents, leading to cholestasis and jaundice.
Examples: EstrogensEndotoxin/tumor necrosis factor

Intrahepatic Cholestasis: Retained bile pigments/bilirubin in hepatocytes
Retained bile

ATP
ADPBile acids
ATPA
DP
Bilirubin conjugates Glutathione S-conjugates other organic anions
Bile Canaliculus
Hepatocyte Sinusoidal Blood
Na+
Bile Acid
Transporters Inhibited by Estrogens

Intrahepatic Cholestasis
Intrahepatic cholestasis due to diseases thatcompress and/or destroy intrahepatic bile ducts:
Primary Biliary Cirrhosis
Infiltration of liver with tumor/granulomas

Primary Biliary Cirrhosis• Chronic, slowly evolving cholestatic
disorder
• Primarily affects middle-aged women
• Primary lesion:– T cell mediated destruction of intrahepatic bile
ducts– Slow progression to cirrhosis
• Relative sparing of hepatocytes with relative preservation of liver function

Primary Biliary Cirrhosis (PBC)Typical laboratory abnormalities:
Alk Phos 1050 IU/l (nl 50-110)
Bilirubin 1.0-2.0 mg/dl (nl 0.4-1.0)
AST/ALT 75-150 IU/l (nl 25-60)
Albumin 3.7 gm/dl (nl 3.5-4.5)
Prothrombin time 11 seconds (nl 8-12)
Cholesterol 420 mg/dl (nl 110-200)
Antimitochondrial antibody:positive in 95%
Liver copper: may be elevated due to chronic cholestasis

Early lesion of Primary Biliary Cirrhosis

Bile duct

Primary Biliary Cirrhosis (PBC)
Clinical Findings:
Jaundice
Pruritus (related to retention of bile acidsand other substances)
Xanthomas/xanthalasmas (cholesterol deposits in skin)

Jaundice

Skin lesions onthe back fromscratching dueto pruritus inPrimary BiliaryCirrhosis

PBC: xanthalasmas

PBC: xanthomas

Infiltrative/Granulomatous Diseases
Often present with cholestasis:elevated alkaline phosphatasewith or without jaundice
Increased alk phos due to compression of smallintrahepatic bile ducts by expandinggranulomas
Examples: tuberculosissarcoidosis

Hepatic Granulomas/Sarcoidosis

Hepatic Sarcoidosis: granulomas and giant cells

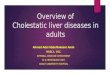
Extrahepatic Biliary Obstruction

Intrahepatic
Perihilar
Distalextrahepatic
Duodenum
AmpullaOf Vater
Commonbile duct
Gallbladder
Commonhepatic duct
LiverExtra-HepaticBileDucts
Obstruction ofthe bile ductsat any pointoutside theliver can cause cholestasis by blocking bile flow.
Adapted from Gordon Flynn, Wikimedia Commons

ERCP (normal)Endoscopic Retrograde CholangioPancreatography

Intrahepatic
Perihilar
Distalextrahepatic
Duodenum
AmpullaOf Vater
Commonbile duct
Gallbladder
Commonhepatic duct
Liver
Does obstructionof the cystic ductor gallbladdercause jaundice?
Adapted from Gordon Flynn, Wikimedia Commons

Subsets of Extrahepatic Biliary Obstruction
Intrinsic Obstruction Extrinsic Obstruction
Gallstones Tumor:Biliary Strictures pancreatic postsurgical cholangiocarcinomaPrimary sclerosing cholangitis periampullary lymphomaWorms/parasites or metastatic tumorBlood clot/hemobilia Acute/chronic pancreatitis
(edema/fibrosis in head of
pancreas)Congenital disease:
biliary atresia choledochal cyst

Primary Sclerosing Cholangitis• Slowly evolving disease with fibrosis, stricturing and
inflammation around extrahepatic bile ducts.– May also affect intrahepatic ducts
• Primarily affects middle-aged men– Associated with ulcerative colitis.
• Complications include complete duct obstruction, jaundice, biliary infection (cholangitis), pruritus.
• Relative preservation of hepatocytes.

Primary Sclerosing Cholangitis
Typical laboratory abnormalities:
Alk Phos 875 IU/l (nl 50-110)
Bilirubin 2.0-5.0 mg/dl (nl 0.4-1.0)
AST/ALT 75-150 IU/l (nl 25-60)
Albumin 3.5 gm/dl (nl 3.5-4.5)
Prothrombin time 11 seconds (nl 8-12)

Primary Sclerosing Cholangitis
Typical Clinical Findings:
Bile duct obstruction: best seen on direct imaging
Jaundice and dilated bile ducts if complete obstruction of major duct occurs.
Bile plugs/bile lakes/bile infarcts on liver biopsy
Biliary infection (cholangitis) - acute bacterialinfection of stagnant bile.
Cirrhosis

Sclerosing Cholangitis:“onion-skinning fibrosis” around bile ducts
very thickenedbile duct walldecreases luminaldiameter


Biliary obstruction
• When bile ducts are obstructed, what happens to the bile?
• What happens to the bile duct upstream of the obstruction?


Evidence of Bile Duct Obstruction: Dilated ducts upstream of the obstruction
Bile-filled dilated bile ducts are large dark gray tubularstructures that runparallel to the portalveins (white arrows).
Portal veins are whitedue to IV contrast.liver parenchyma islight gray due to IVcontrast.

Dilated bile ducts and gallbladder
Gallbladder
Dilated bile ducts
Mass in head ofthe pancreas

Bile Duct Obstruction: Bile Plugs in Bile Ducts
Portal vein
HA

More canalicular cholestasis

Acute Cholangitis: PMNs in Bile Duct
HA

Other Causes of Extra-hepatic Biliary Obstruction

High grade cholangiocarcinoma at the hilum

High grade bilateral obstruction from metastatic rectal carcinoma

Biliary stricture due to cholangiocarcinoma
Alk phos = 669 IUBili = 17.5 mg/dlAST = 68 IUALT = 38 IU

More permanent metal mesh stent placed
A plastic stent bridgesthe stenosis

Bile ductobstructionfrom chronicpancreatitis

Biliary Obstruction:
Multiple stonesin biliary tree

Large ducts nearhilum massivelydilated
Small peripheralducts also enlargedand visible
Bile Duct Dilation due to Obstruction

An unusualcause of biliary obstruction
Radio-opaque dye injected through T-tubefills common bile ductand intrahepatic bileducts.
Dark linear structures are ascariasislocated in biliary system (black arrows).

Ascaris emerging from common bile duct as seen endoscopically

Consequences of Cholestasis
• Secondary liver damage– Bile acid-induced hepatocyte injury– Secondary biliary cirrhosis
• Failure of substances secreted in bile to reach intestine– Bile acid deficiency in gut– Fat malabsorption/fat-soluble vitamin
malabsorption

SUMMARY: EVALUATION OF CHOLESTASIS AND/OR JAUNDICE
1. Suspect cholestasis based on history, physical exam, lab tests.
2. Look for clues to mechanical obstruction of ducts and/or mass lesions (radiologic studies).
3. Visualize, diagnose and treat mechanical obstruction.
4. Consider intrahepatic cholestasis, obtain liver biopsy.
See algorithms in syllabus and in textbook

Additional Source Informationfor more information see: http://open.umich.edu/wiki/CitationPolicy
Slide 32 & 34: Adapted from Gordon Flynn, Wikimedia Commons, http://commons.wikimedia.org/wiki/File:Digestive_system_with_liver.png, CC:BY-SA, http://creativecommons.org/licenses/by-sa/2.5/deed.en