Embed Size (px)
Citation preview
X-RAYSX-RAYS
By
Prof Dr IBRAHIM DAWOUD
Prof of Surgery
Mansoura University

How to read
Urology UTP (Urinary Tract Plain). IVU (Intravenous Urography). MRU. Urethrography. Ascending Cystography. CT scan. US. Fistula: Fistulography.



Plain X-ray abdomen ( Rt hypochondrium). The patient is more or less well prepared. It revealed * A radio-opaque shadow in the Rt hypochondrium. Diagnosis
Radio-opaque Shadow in the Rt hypochondrium for DD most probably
RT Renal Stone
How to read
DD of radio-opaque shadow {1} Gall stone -----shape of the stone
------ in lat view in front of the spine
{2} Renal stone -- ---- Cholecystography or IVU
{3} Calcified LN
{4} Fecolith or FB in the small intestine
{5} Phlebolith
{6} Atherosclerotic renal artery
{7} Hydatid cyst in the liver
{8} Calcified TB kidney or suprarenal gland
{9} Calcified costal cartilage
{10} Fracture transverse process of lumbar vertebra
Questions

How to readHow to read
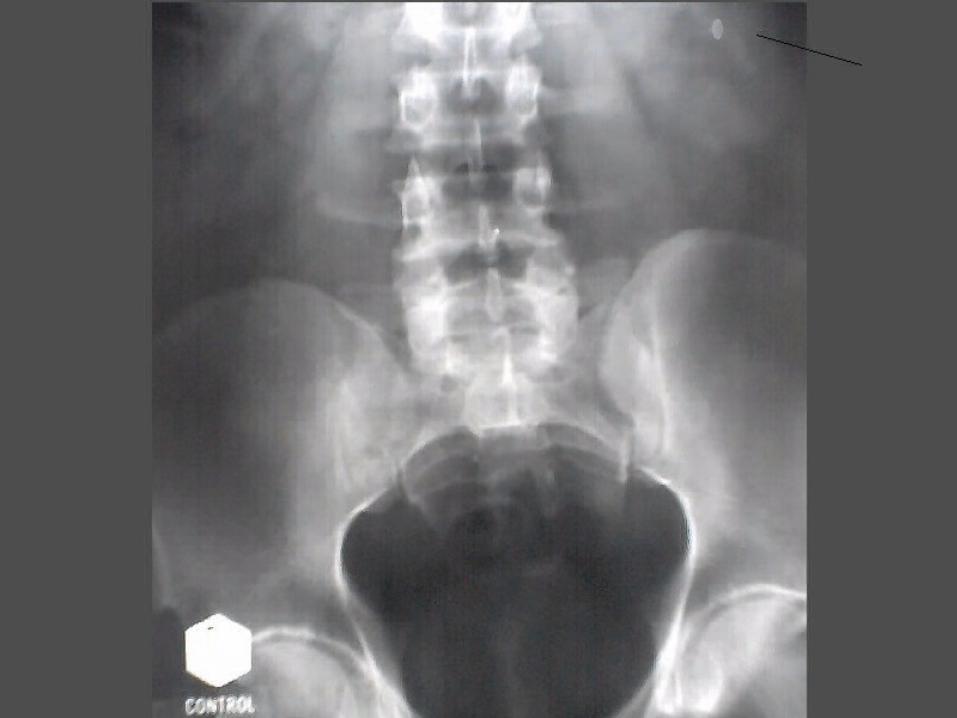
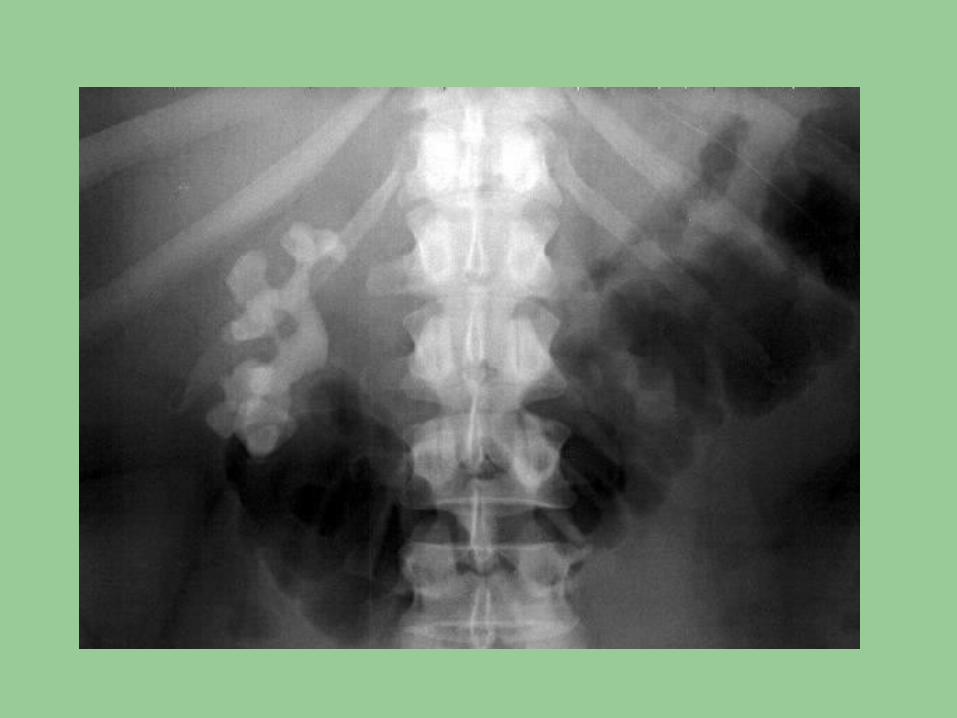
Plain X-ray abdomen ( Lt hypochondrium). The patient is more or less well prepared. It revealed
* A radio-opaque shadow in the Lt hypochondrium.
Diagnosis
Radio-opaque Shadow
in the Lt hypochondrium for DD
most probably
LT Renal Stone

How to readHow to read
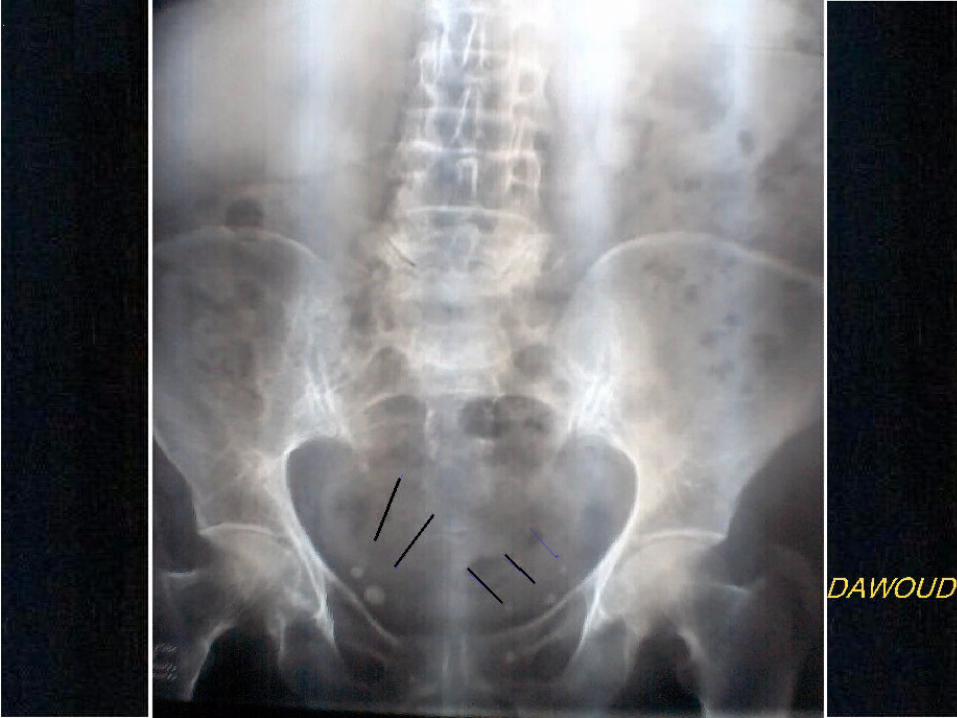
Plain X-ray abdomen. The patient is more or less well prepared. It revealed
* Multiple radio-opaque shadows in the pelvis.
In the course of both pelvic ureters
Diagnosis
Radio-opaque Shadows
in the course of both pelvic ureters
most probably
Ureteric stones



How to readHow to read
Plain X-ray abdomen ( Lt hypochondrium). The patient is more or less well prepared. It revealed
* A radio-opaque shadow in the Lt hypochondrium.
Giving a stag-horn appearance
Diagnosis
Radio-opaque Shadow
in the Lt hypochondrium for DD
most probably
LT Renal Pelvis
Stag-horn Stone

Questions Questions
Pathology Clinical Picture Investigations Treatment
Stones of the Urinary System Stones of the Urinary System



How to readHow to read
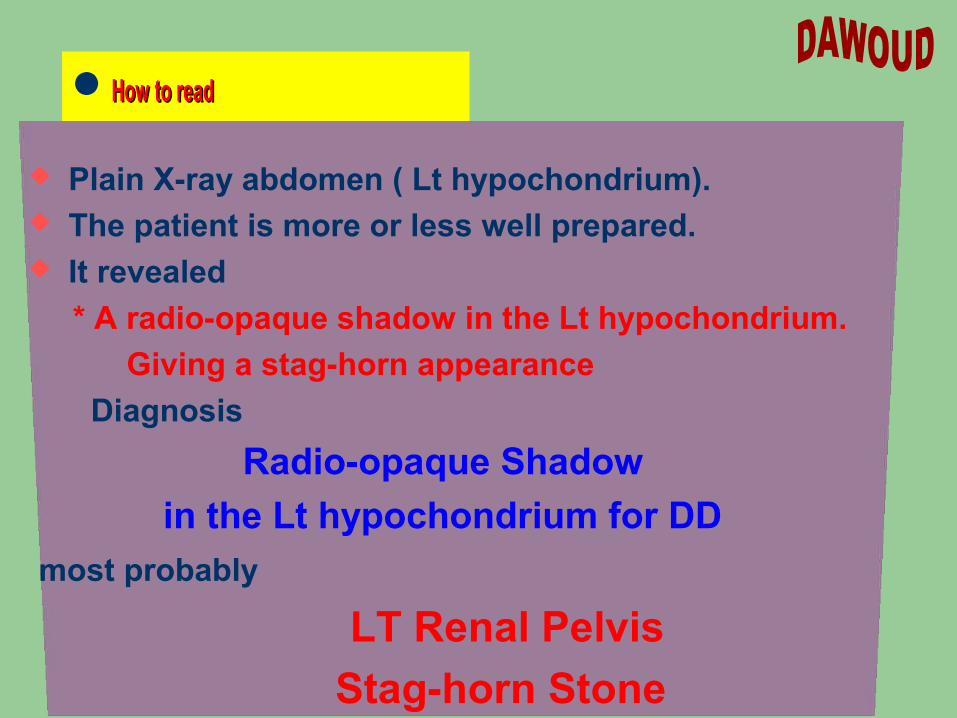
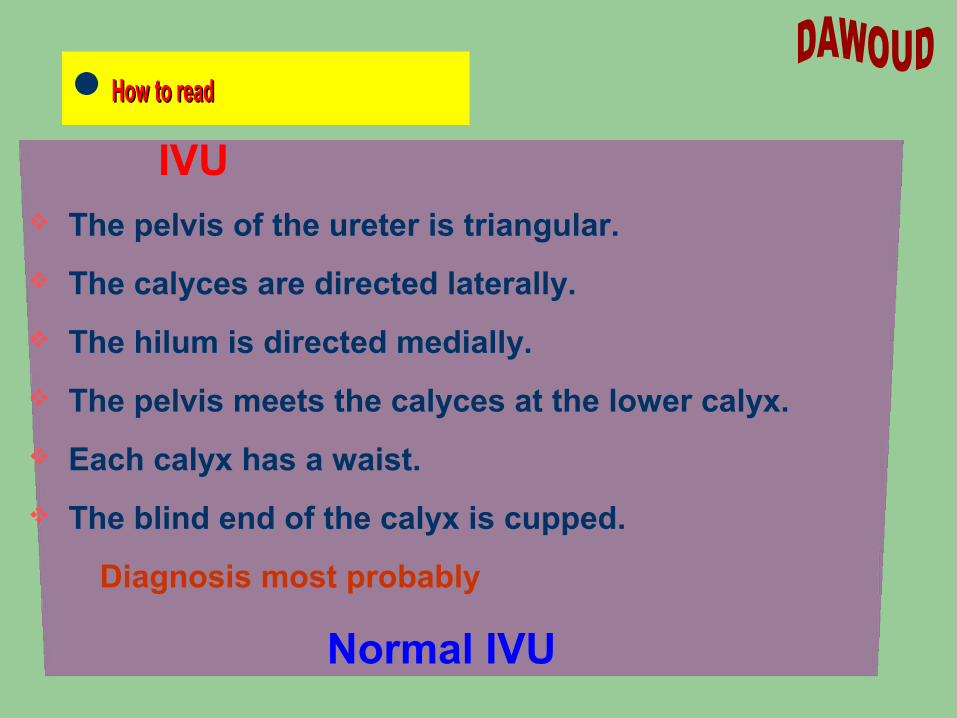
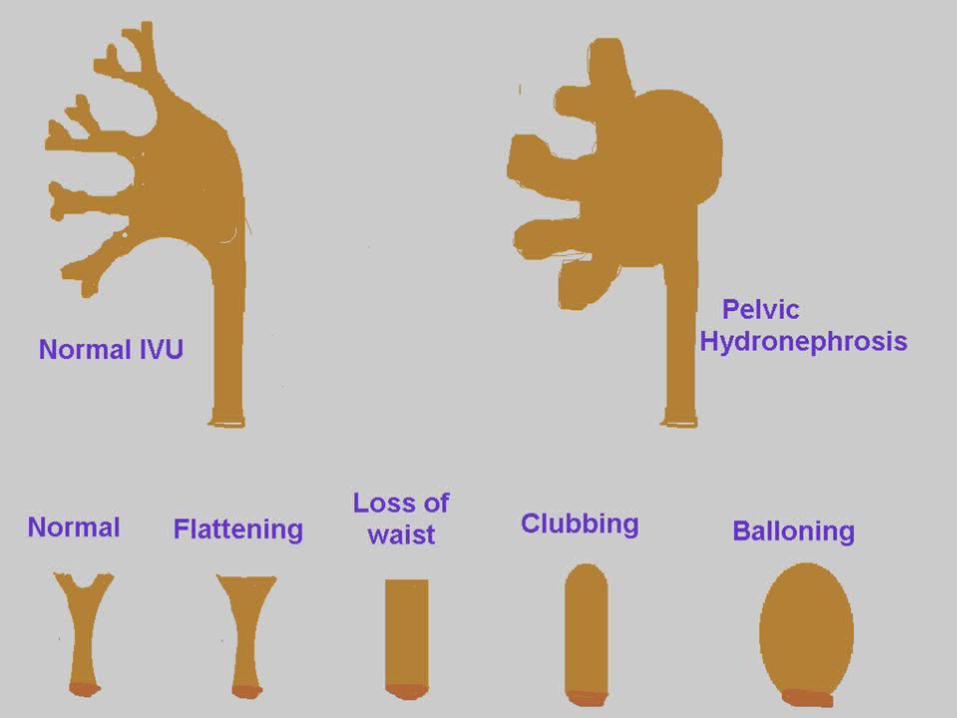
IVU The pelvis of the ureter is triangular.
The calyces are directed laterally.
The hilum is directed medially.
The pelvis meets the calyces at the lower calyx.
Each calyx has a waist.
The blind end of the calyx is cupped.
Diagnosis most probably
Normal IVU



How to readHow to read
IVU The Lt kidney and ureter have normal appearance.
The RT kidney.
- The pelvis shows mild dilatation.
- The calyces revealed signs of hydronephrosis
(flattening- loss of waist- clubbing- ballooning).
- No definite site of distal obstruction appeared in the film.
Diagnosis most probably
Right Hydronephrotic Kidney

How to readHow to read IVU The Lt kidney and ureter have normal appearance.
The right kidney.
- The pelvis shows severe dilatation.
- The calyces revealed signs of hydronephrosis
(flattening- loss of waist- clubbing- ballooning).
- The upper 1/3 of the ureter revealed dilatation
with stricture at the junction bet upper and middle 1/3.
- The UB is normal
Diagnosis most probably
Right Hydronephrotic Kidney
with Hydroureter


How to readHow to read
IVU Both kidneys.
- The Rt pelvis shows mild dilatation and the Lt is severe.
- The calyces revealed signs of hydronephrosis (ballooning).
Rt ureter: - revealed stricture at the lower 1/3.
Lt ureter:- revealed double strictures
(at the pelvi-ureteric junction and at the lower 1/3 with Hydroureter).
UB: Normal
Diagnosis most probably
Bilateral Hydronephrotic Kidney
With stricture ureters

How to readHow to read
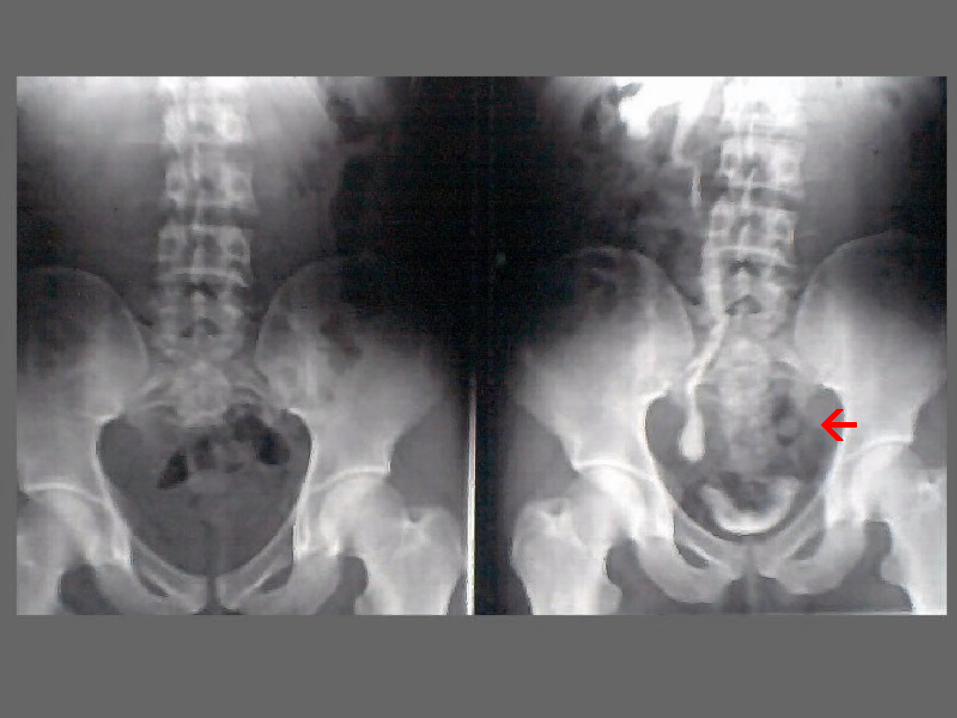
IVU The Rt kidney and ureter have normal appearance.
The left side.
- No visualization of dye.
- A radio-opaque shadow is seen in the course
of the Lt lumbar ureter.
Diagnosis
Non visualized Lt Kidney
most probably due to obstruction by a stone
in the Lt lumbar ureter

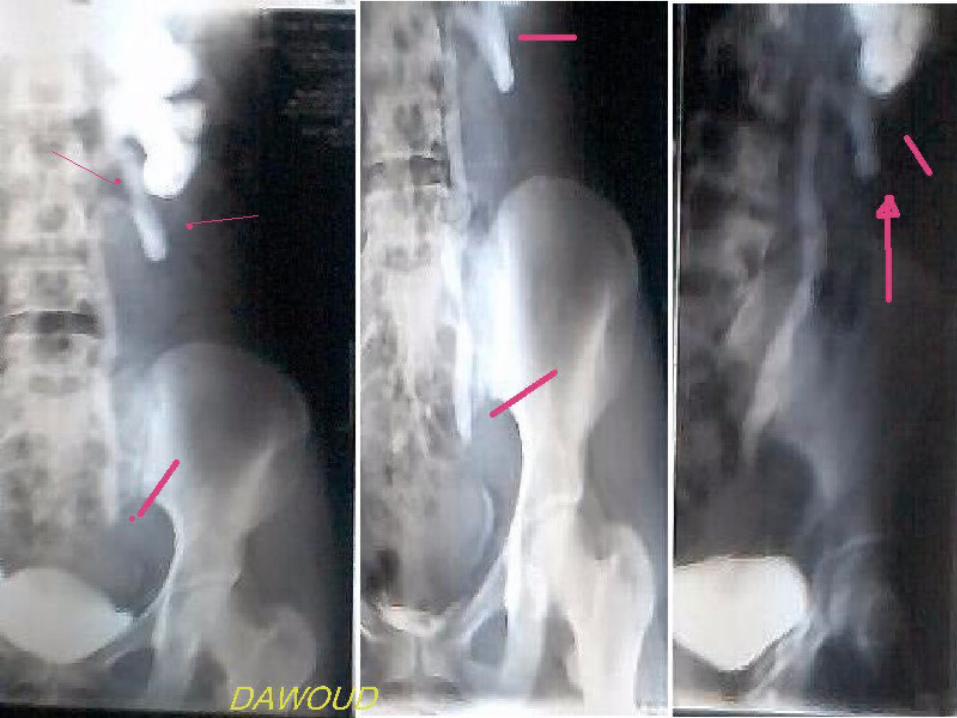
How to readHow to read IVU The Rt kidney and ureter show signs of hydronephrosis
and hydroureter, with stricture at the pelvic ureter.
The left side.
- No visualization of dye.
- A radio-opaque shadow is seen in the course of the Lt pelvic ureter.
Diagnosis
Rt Hydronephrosis and hydroureter
With stricture pelvic ureter
Non visualized Lt Kidney
most probably due to obstruction by a stone
in the Lt pelvic ureter

How to readHow to readIVU The Lt kidney and ureter show signs of
hydronephrosis and hydroureter, with stricture at the pelvic ureter.
The right side.
- normal secretion.
The UB:
- normal.
Diagnosis
Lt Hydronephrosis and hydroureter
With stricture pelvic ureter
Normal Rt kidney


How to readHow to read
IVU The Lt kidney and ureter have normal appearance.
The right side.
- No visualization of dye.
- Multiple radio-opaque shadows are seen in the course
of the right pelvis and ureter .
Diagnosis
Non visualized Rt Kidney
most probably due to obstruction by stones
in the Rt ureter



How to readHow to read
IVU The Rt kidney shows double pelvis.
The Rt kidney and ureter show signs of hydronephrosis and hydroureter, with stricture at the middle 1/3 ureter.
The left side.
- No visualization of dye.
UB: normal
Diagnosis
Rt Hydronephrosis and hydroureter
Double pelvis with stricture middle 1/3 ureter
Non visualized Lt Kidney


How to readHow to read
IVU The Lt kidney and ureter have normal appearance.
The right side.
- Normal secretory function.
- Double pelvis and 2 ureters united at the lower end of the upper 1/3.
Diagnosis
Normal Lt Kidney
Bifid Rt ureter


How to readHow to read
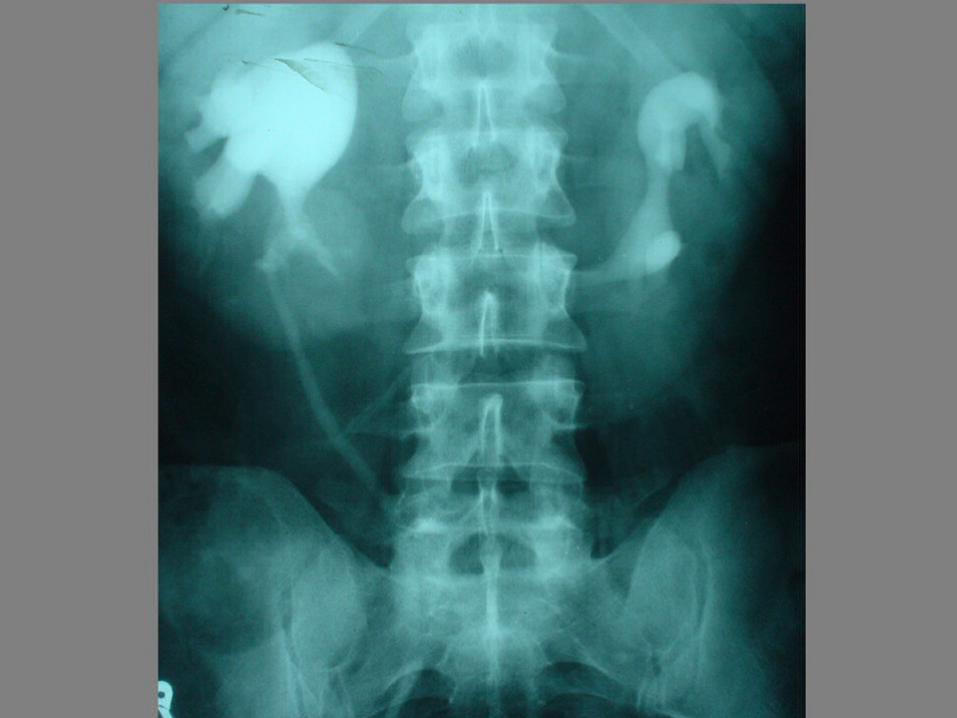
IVU in an infant The Rt kidney and ureter have normal appearance.
The Left side.
- Mild hydonephrosis.
- The left kidney is descended downward and rotated outward.
Dropped Lilly sign
The UB
- Free .
Diagnosis most probably
Neuroblastoma
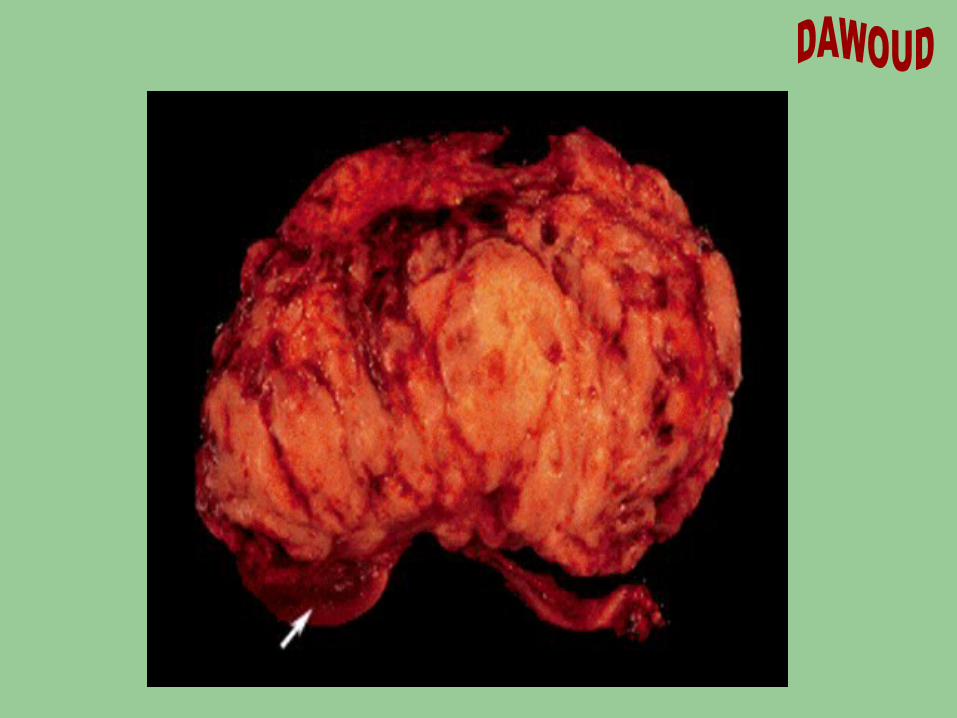

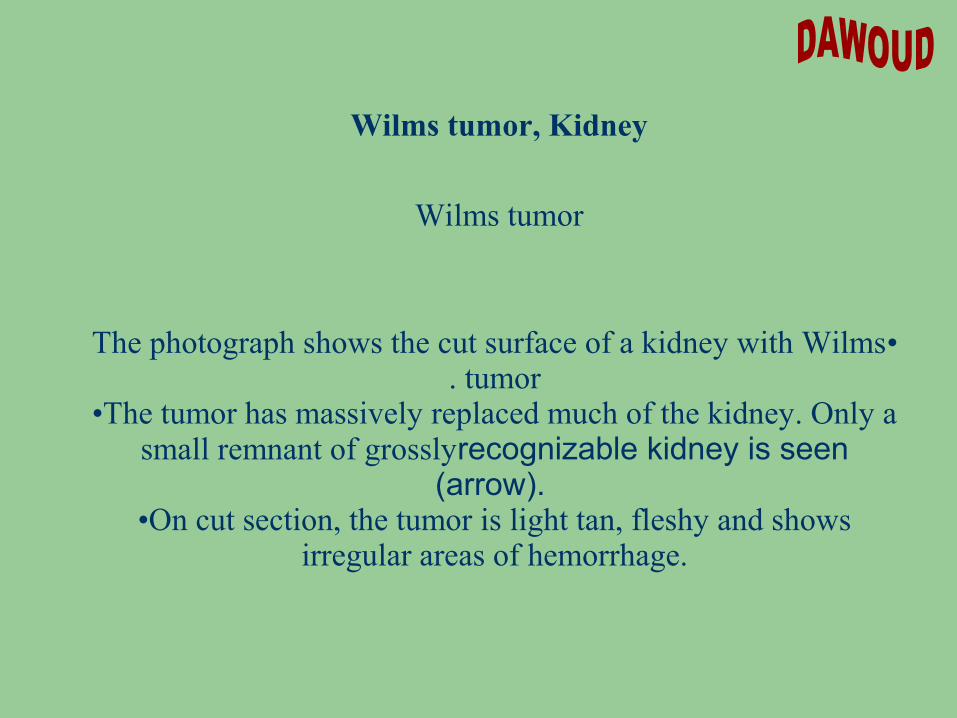
Wilms tumor, Kidney
Wilms tumor
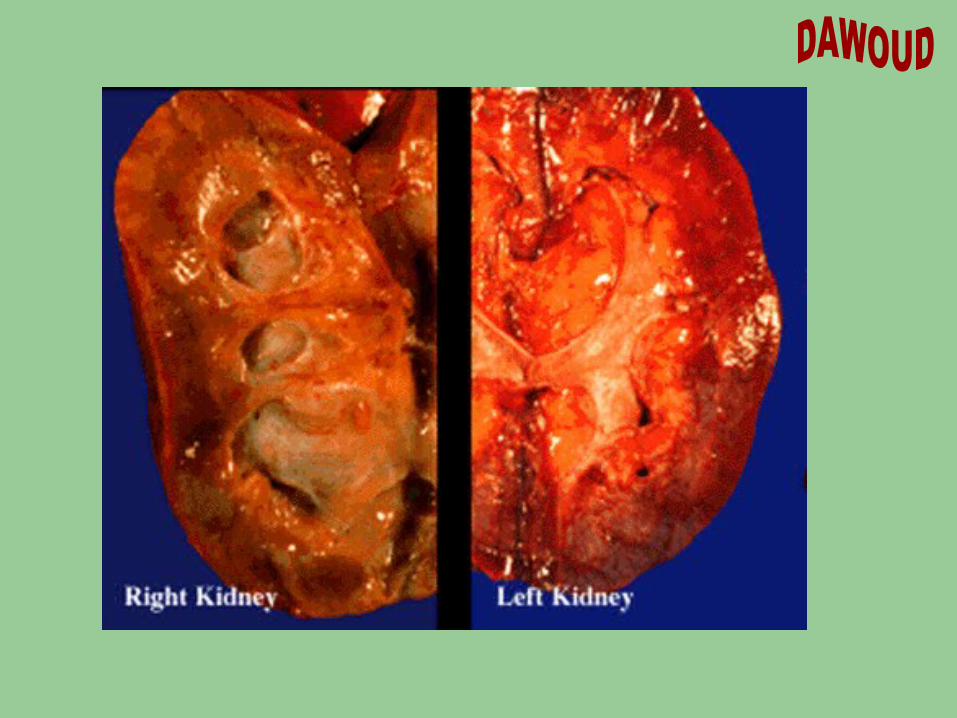
•The photograph shows the cut surface of a kidney with Wilms tumor.
•The tumor has massively replaced much of the kidney. Only a small remnant of grosslyrecognizable kidney is seen
(arrow). •On cut section, the tumor is light tan, fleshy and shows
irregular areas of hemorrhage.



How to readHow to read
IVU The 2 kidneys lie at a lower level and closer to the middle
line.
The lower poles are nearer to each others than the upper.
Their pelves lie anteriorly.
Some calyces are directed medially and others laterally.
The ureters converge slightly over the isthmus and then diverge gradually in a characteristic
Flower vase
The U B - Free .
Diagnosis most probably
Horse-shoe kidney

How to readHow to read
IVU The Rt kidney lie at a lower level.
The Rt pelvis lies anteriorly.
The calyces are directed medially.
A fistulus track connecting the lower calyx to outside
The left kidney non visualized
The UB -- normal
Diagnosis most probably
Horse-shoe kidney with Rt urinary fistula
Non visualized lt kidney (nephrectomy)



How to readHow to read
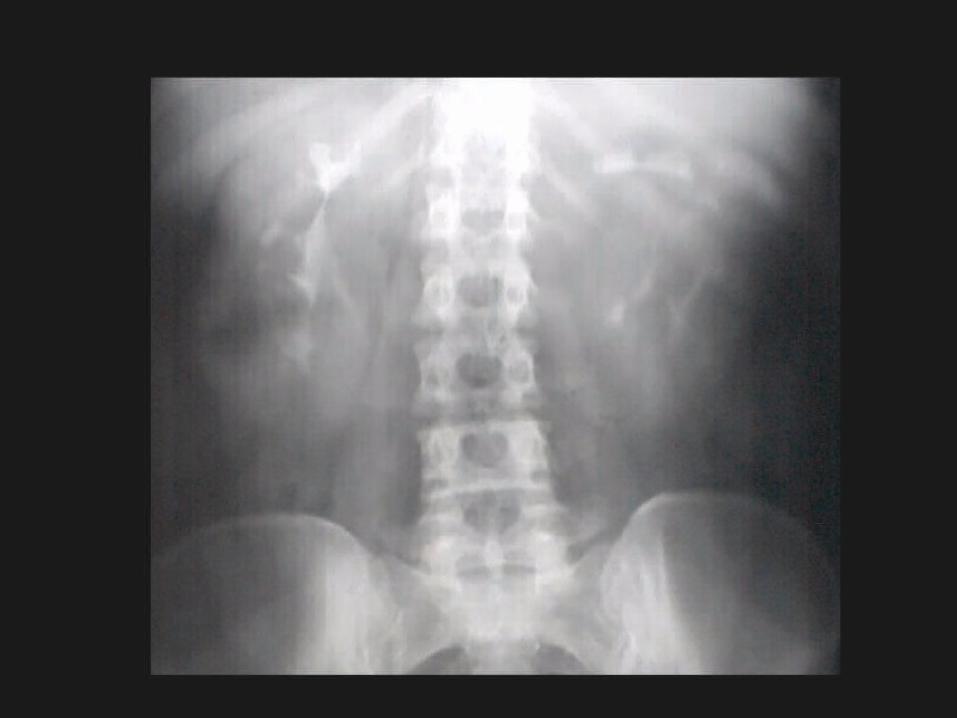
IVU The pelvicalyceal system show elongation,
attenuation and wide separation
Smooth Spider leg appearance The U B Free
Diagnosis most probably
Polycystic kidney
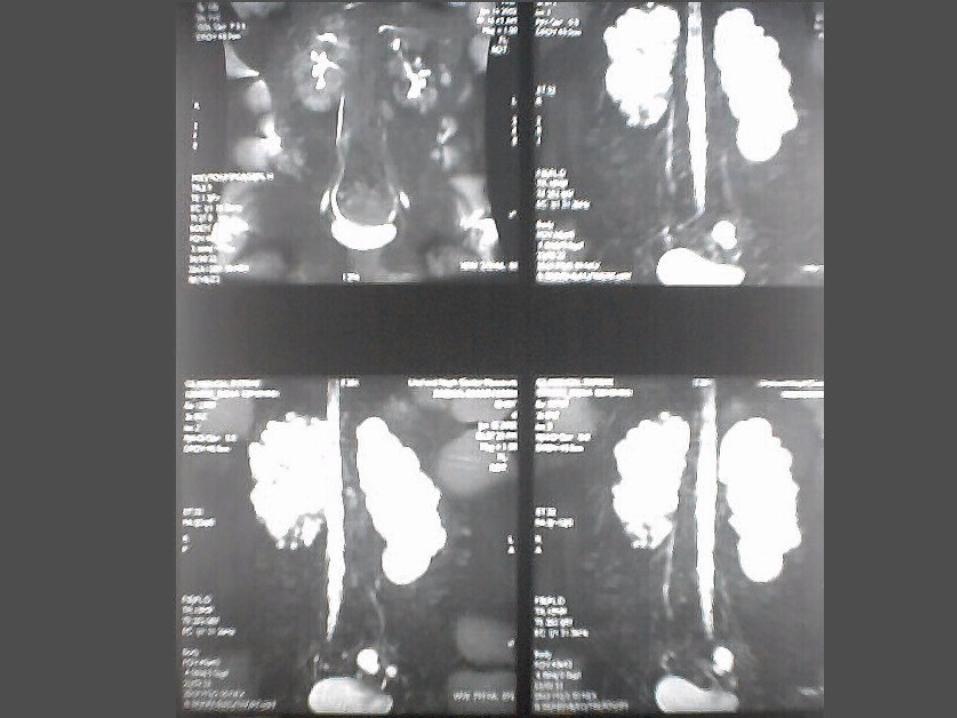
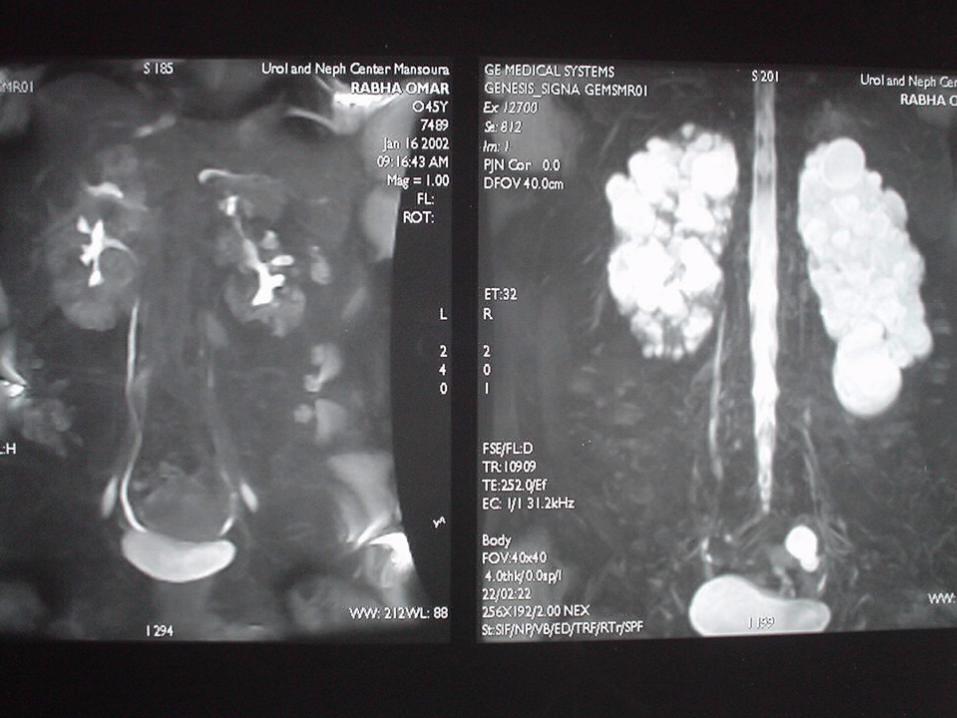
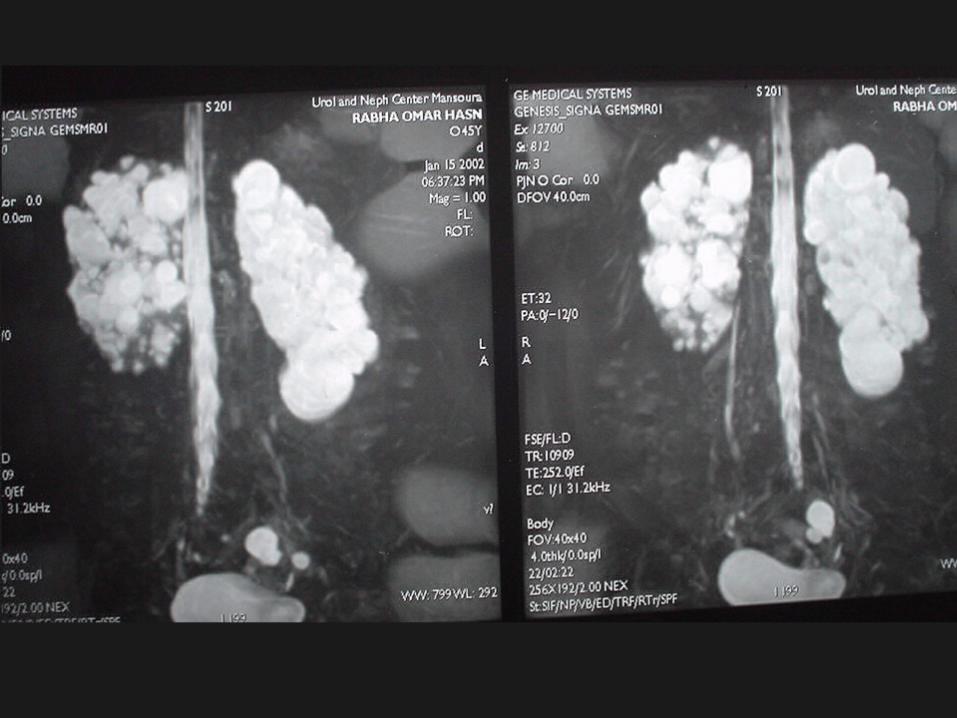
How to readHow to read
MRU The pelvicalyceal system show elongation,
attenuation and wide separation
Smooth Spider leg appearance
Multiple cysts ocuppying the whole kidney
and not communicating with each other.
The U B Free
Diagnosis most probably
Polycystic kidney

How to readHow to read
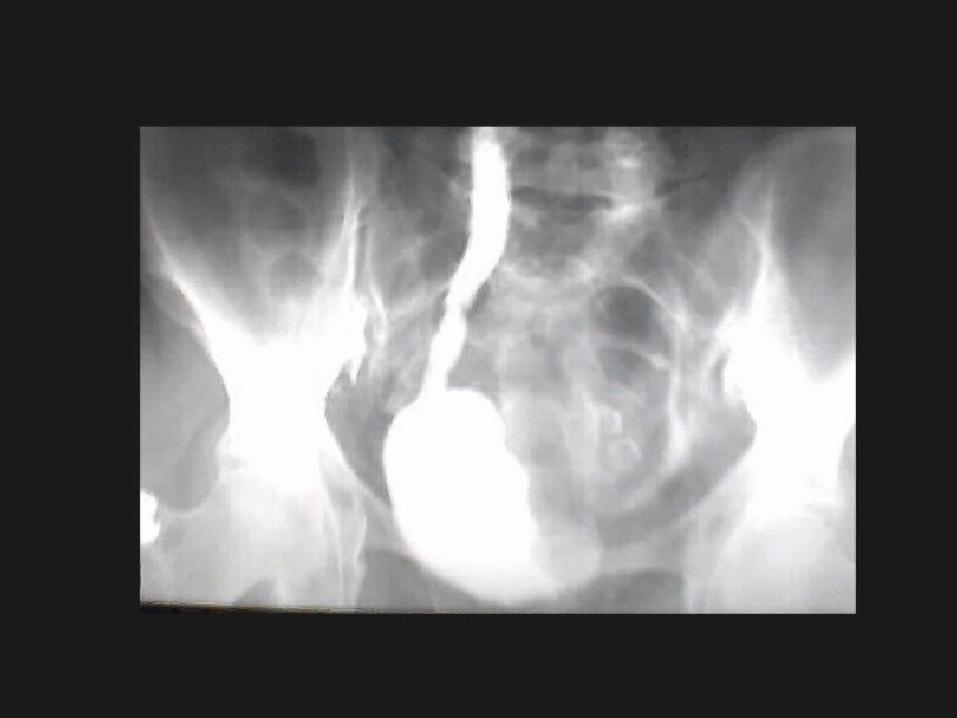
IVU The 2 kidneys and ureters show mild hydroureter and
hydronephrosis
The lower end of the left ureter is shifted laterally
The UB
A large irregular filling defect occupying
the left side of the UB with moth-eaten appearance
Diagnosis most probably
Cancer UB

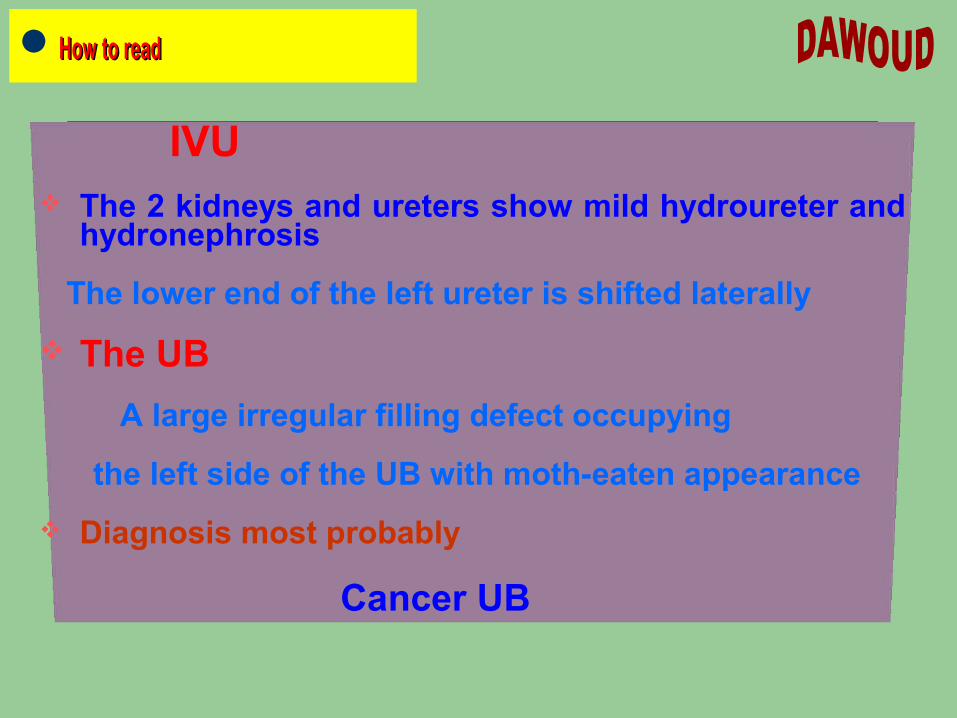
ADENOCARCINOMA
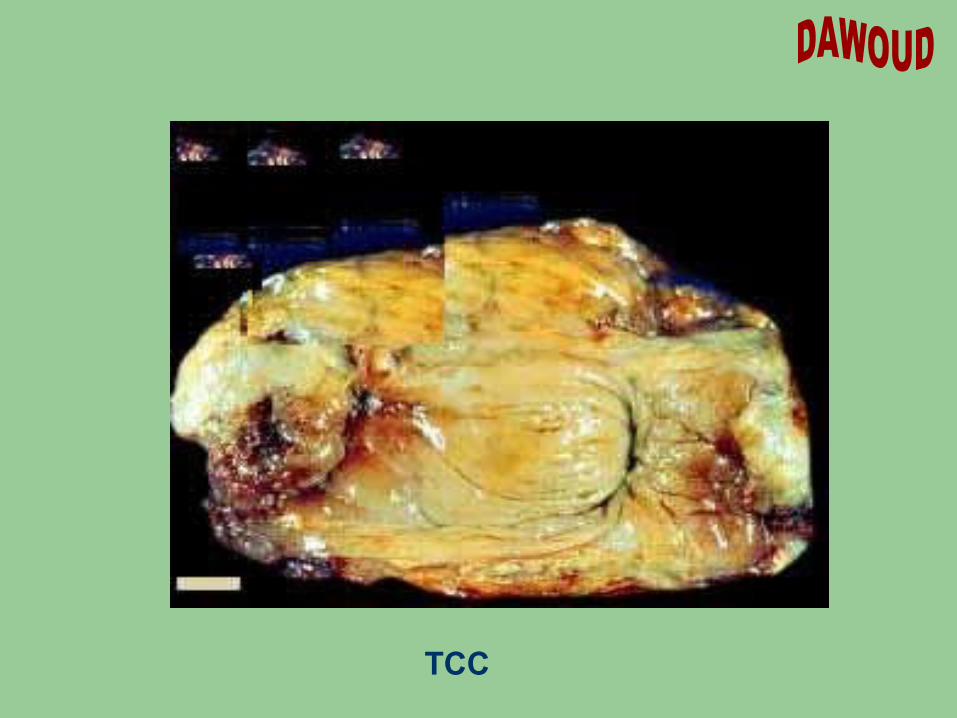
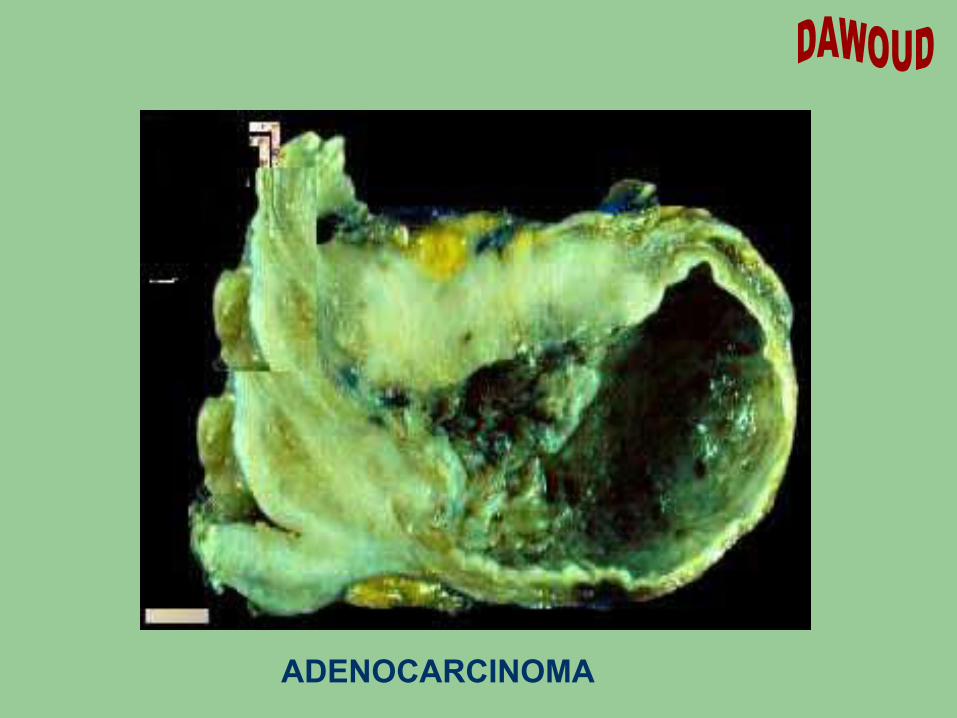
TCC
How to readHow to read
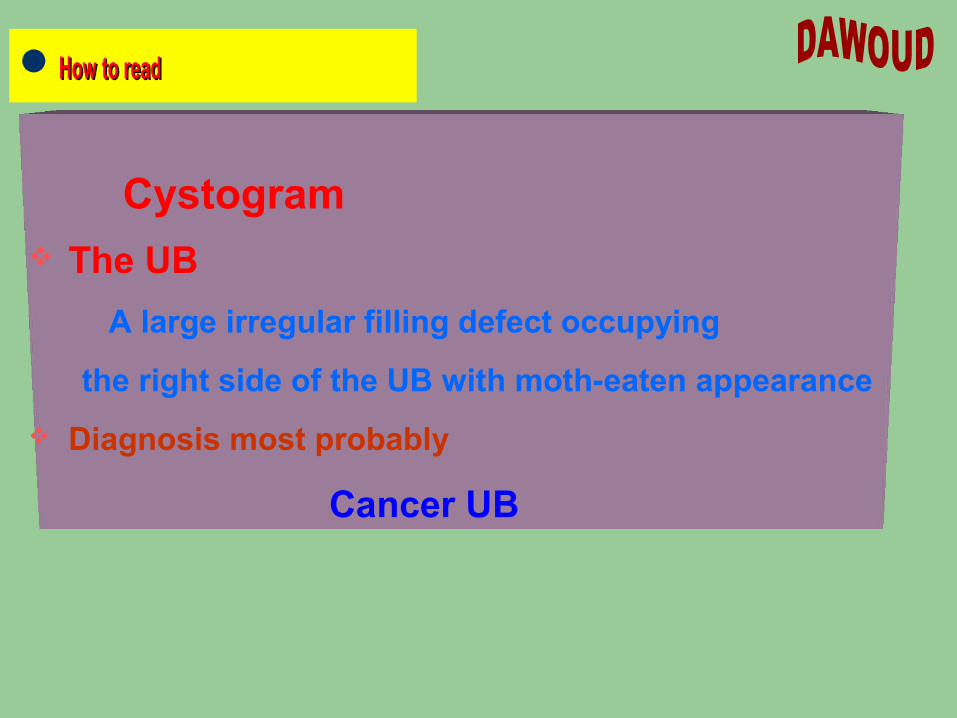
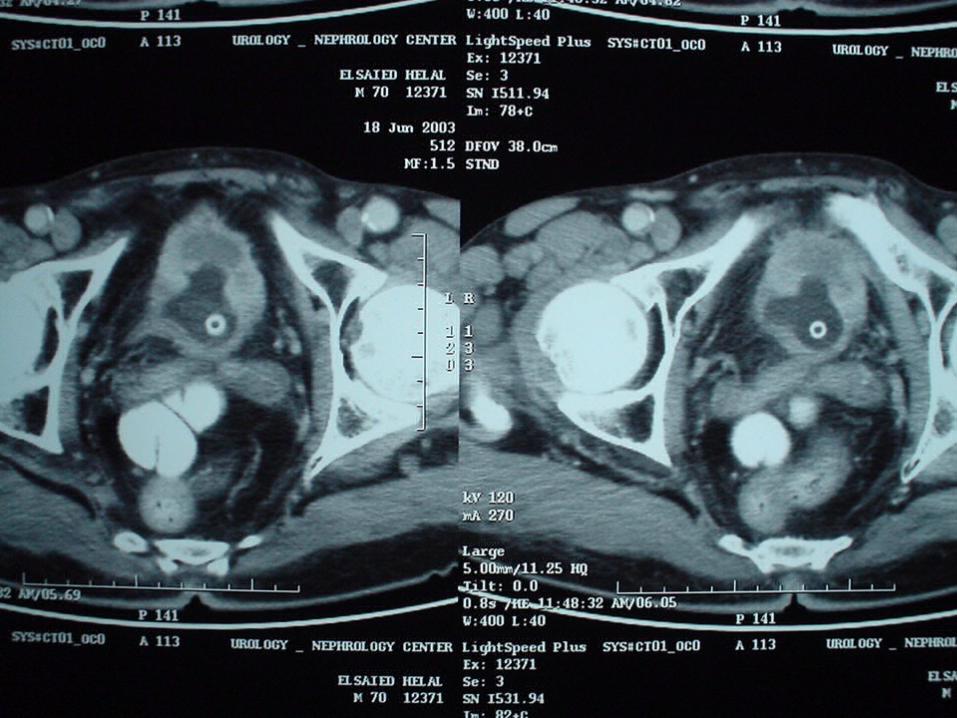
Cystogram The UB
A large irregular filling defect occupying
the right side of the UB with moth-eaten appearance
Diagnosis most probably
Cancer UB

How to readHow to read
Cancer Bladder

How to readHow to read
Cystogram The UB
A diverticulum is senn outpouching between
the junction of the UB and Rt ureter
Diagnosis most probably
UB diverticulum
or Uretrocele


How to readHow to read
Urethrogram The male urethra
A stricture is seen between the prostatic urethra and membranous part
Diagnosis most probably
Urethral stricture

How to readHow to read
Plain X-ray abdomen . The patient is more or less well prepared. A catheter is introduced in the Rt ureter. It revealed
* A large radio-opaque shadow
in the Lt hypochondrium.
Diagnosis
Radio-opaque Shadow
in the Lt hypochondrium for DD
most probably
LT Renal Stone
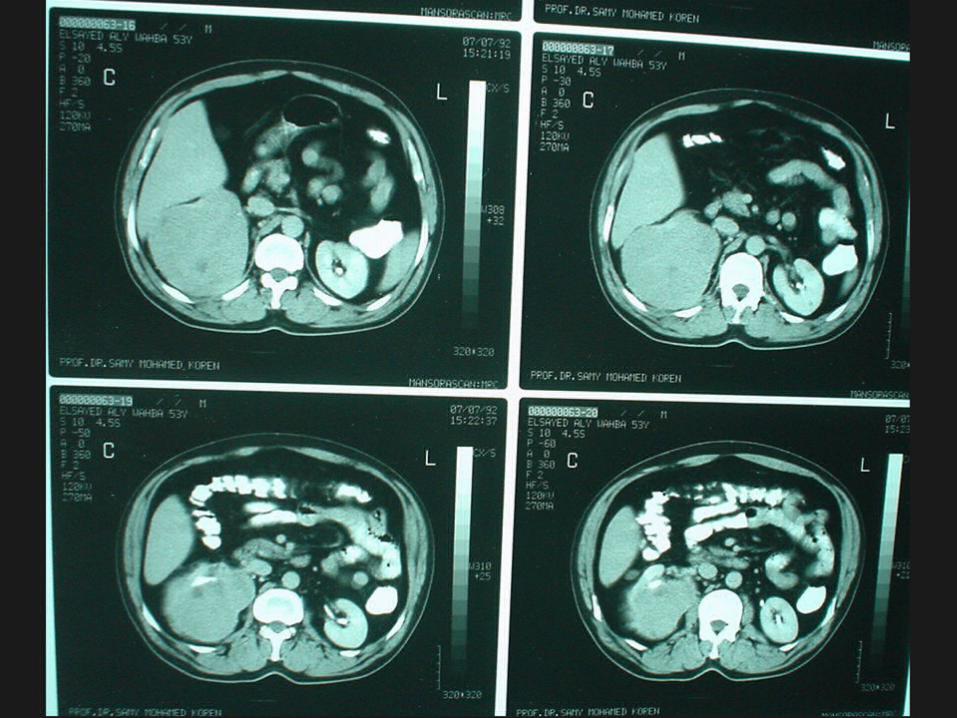
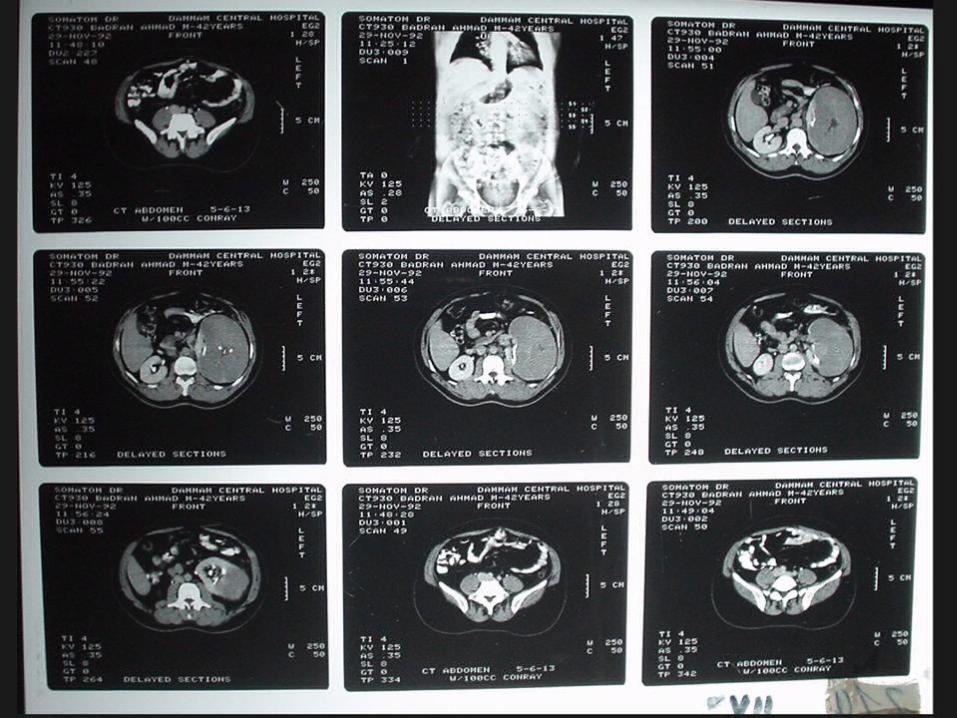
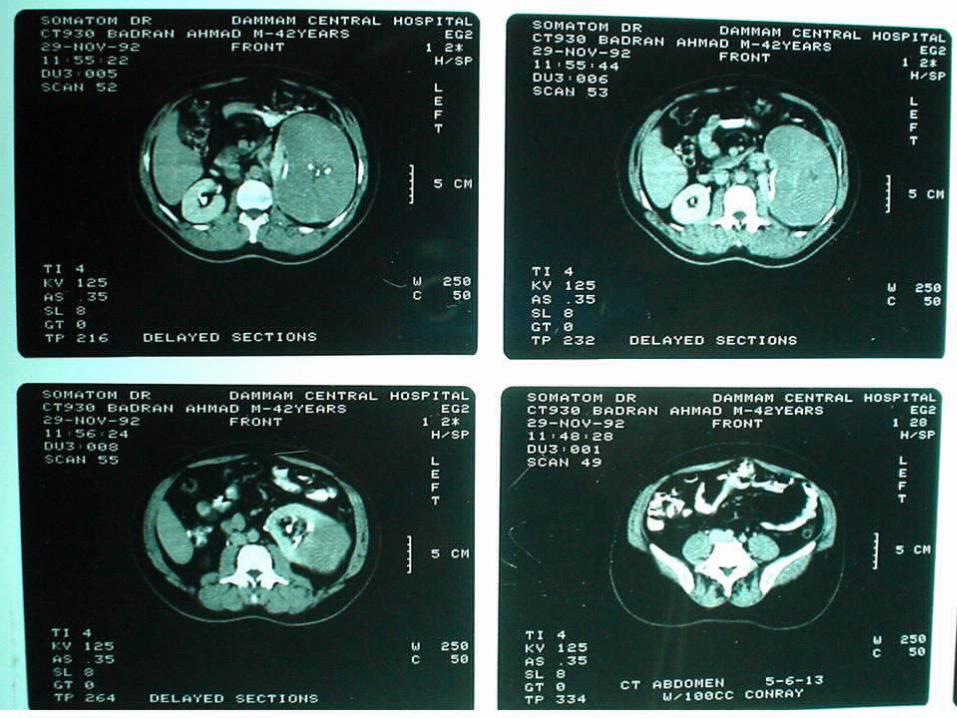
How to readHow to read
Right Renal Cell Carcinoma
How to readHow to read
Left Renal Cell Carcinoma
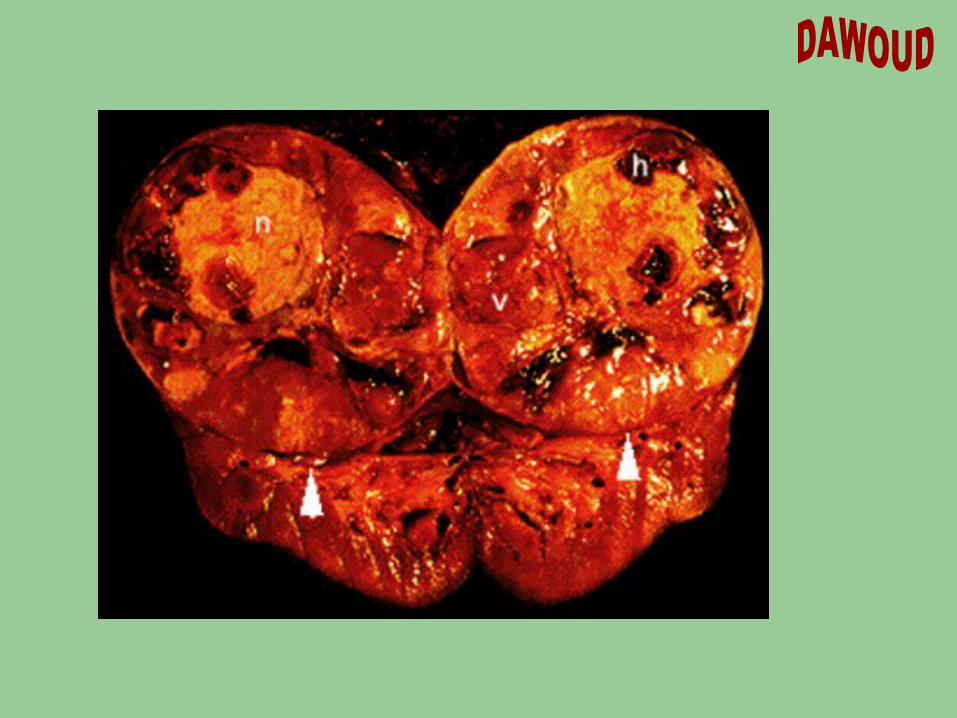
Renal cell adenocarcinoma, Kidney
Renal Cell Adenocarcinoma
•The kidney has been bivalved to show the cut surface of a large spherical tumor involving the upperpole (arrowheads).
•The tumor has sharply defined borders and show a variegated cut surface. Areas of grossly viable
tumor (v) are seen with areas of necrosis (n) and hemorrhage (h).

How to readHow to read
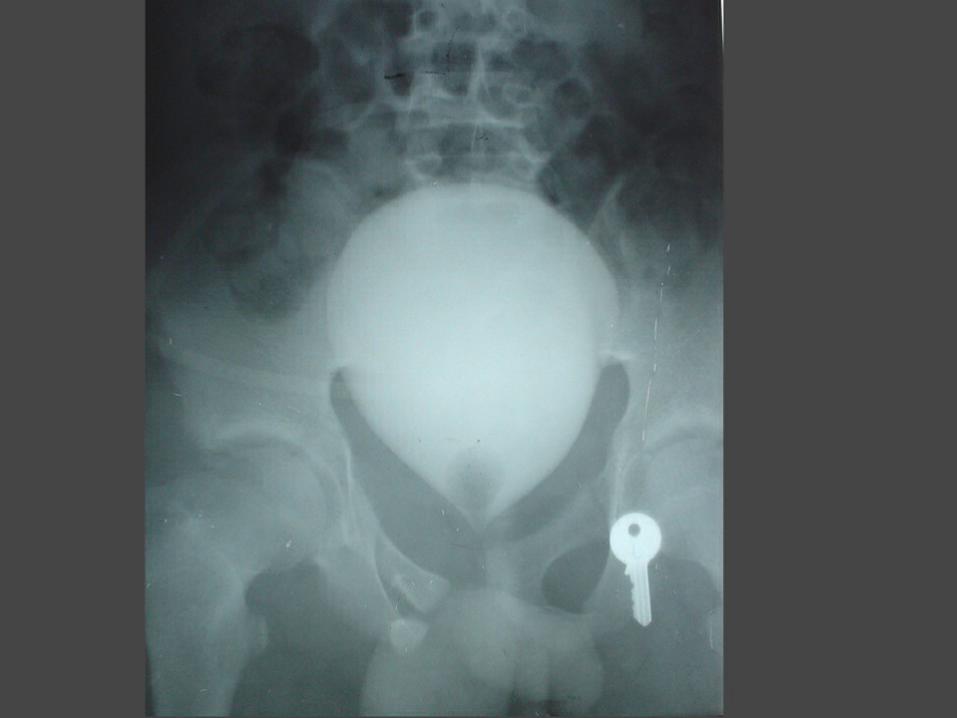
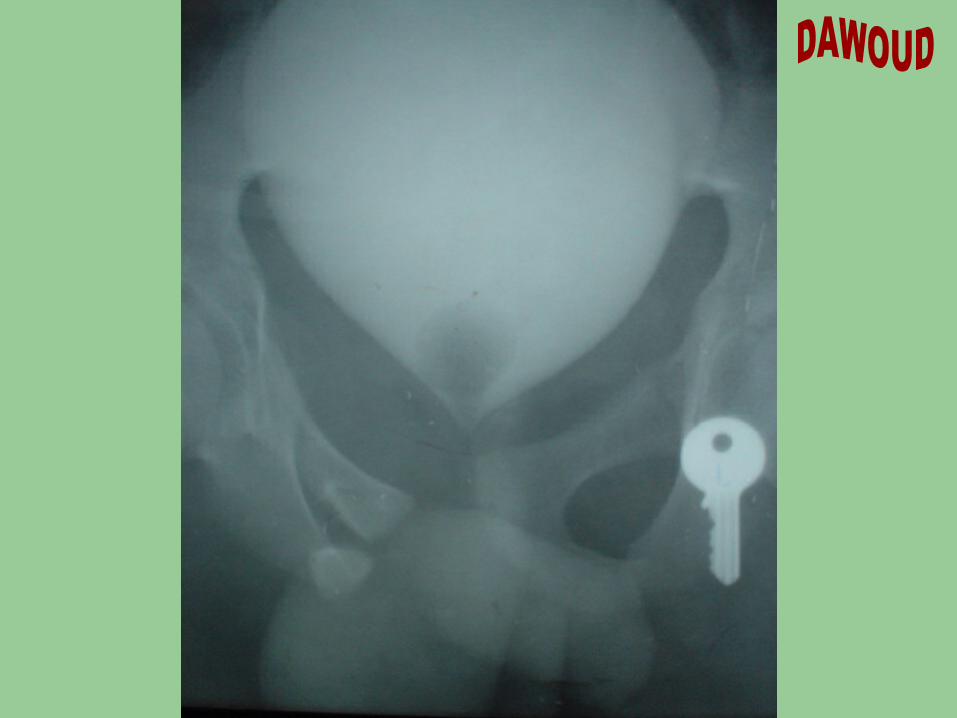
Ascending Cystography Fracture pelvis
Intact UB
Types of Rupture Bladder
(1) Intraperitoneal rupture bladder
(2) Extraperitoneal rupture bladder

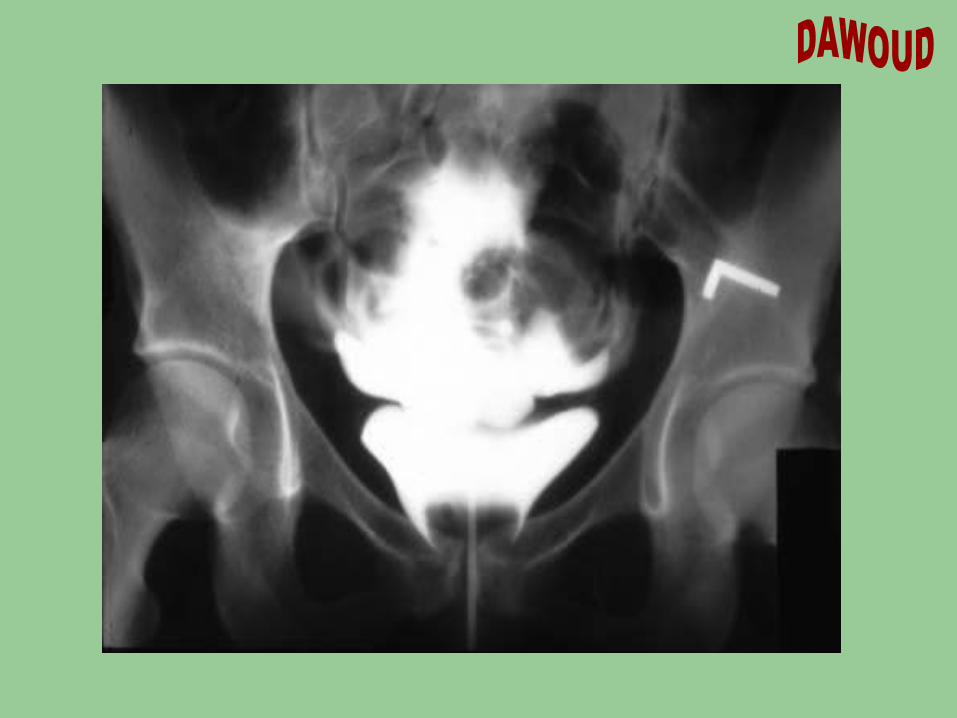
Cystogram of Extraperitoneal bladder rupture.
Note the fractured pelvis and contrast extravasation into the space of Retzius
Cystogram of Intraperitoneal bladder rupture.
The contrast enters the intraperitoneal cavity
and outlines loops of bowel(Fluffy Cotton Appearance)
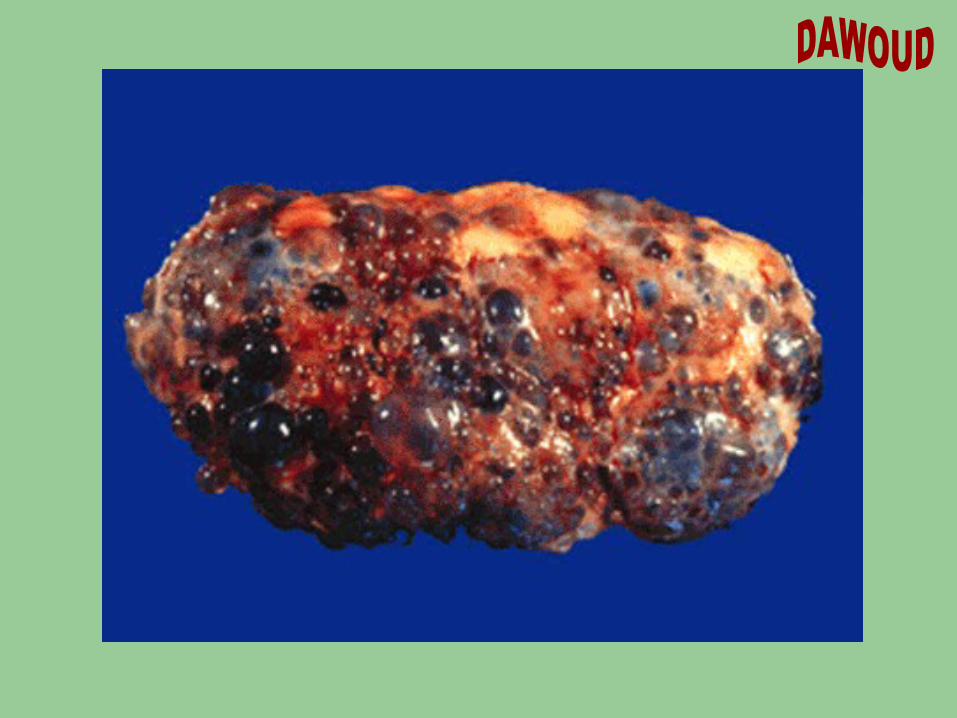
Adult polycystic kidney disease, Kidney
Adult Polycystic Kidney Disease
•This is the external surface of one kidney. •Both the right and left kidneys of this patient had the same
appearance. •Note the numerous intact, unruptured cysts on the surface.

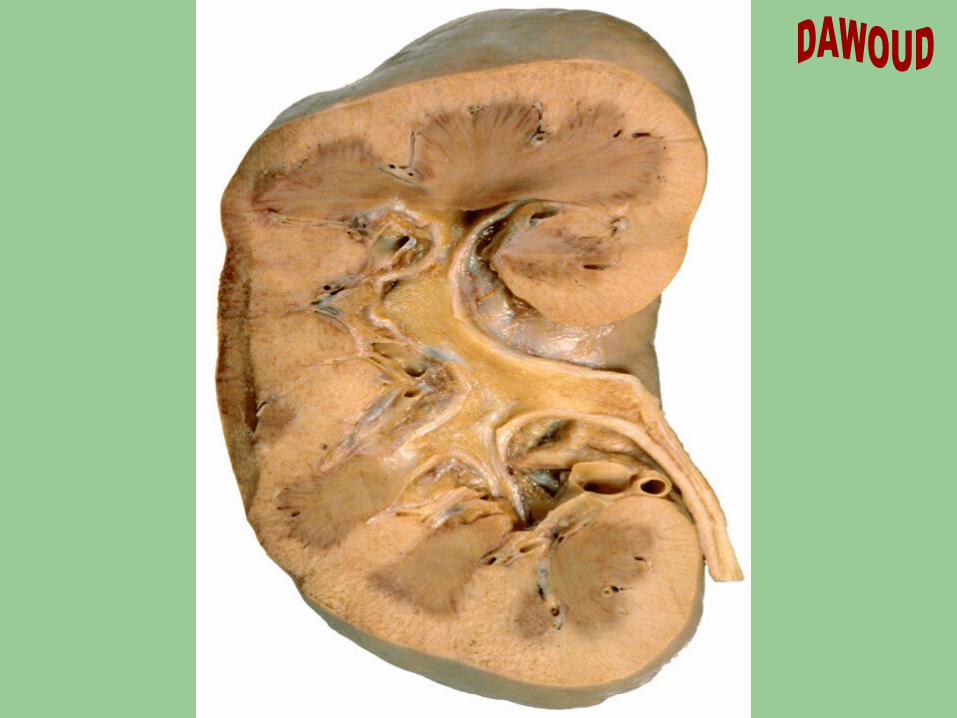
Adult polycystic kidney disease, Kidney
Adult Polycystic Kidney Disease
•This is a cut section of an adult polycystic kidney •Cysts of varying sizes are present throughout the renal parenchyma.
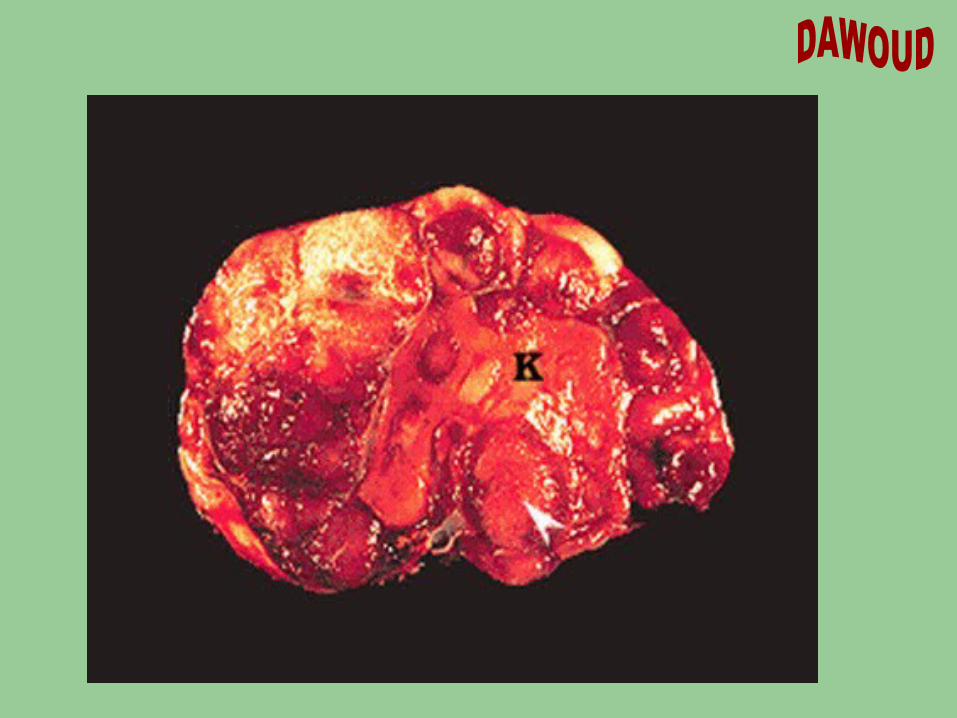
Neuroblastoma, Kidney
Neuroblastoma encasing kidney
• The tissue mass is an adrenal neuroblastoma. The tumor has completely encased the kidney (K(.
• The tumor has entered and expanded the renal sinus (arrowhead(.
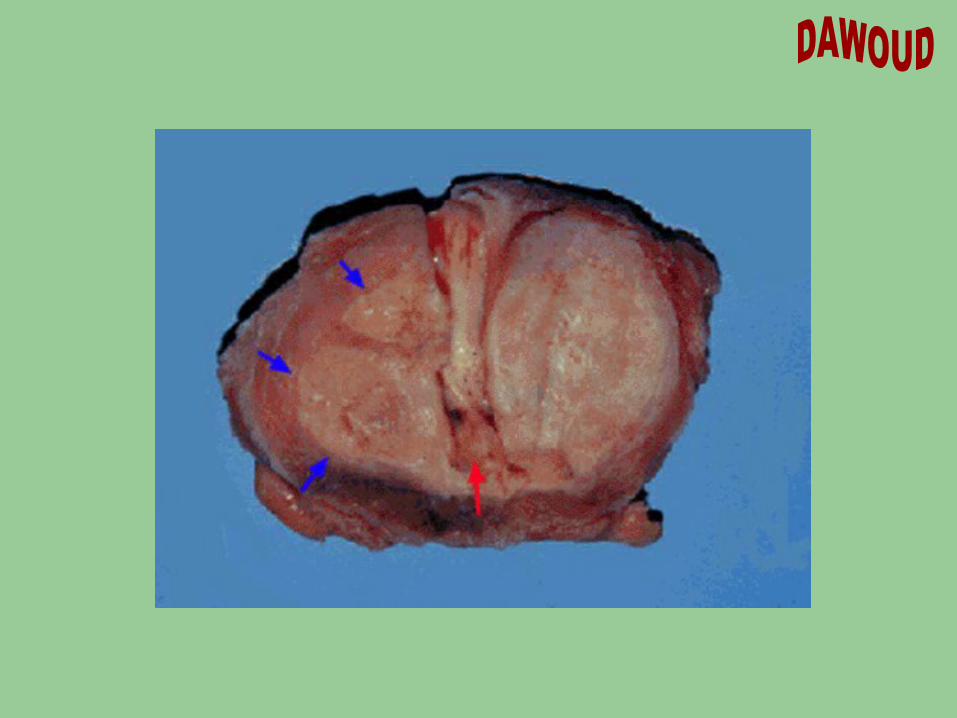
Adenocarcinoma, Prostate
Prostate Adenocarcinoma
• The blue arrows point to the margins of two nodules of tan adenocarcinoma. The other lobe shows hyperplasia.
• The red arrow points to the urethra. • The black staining at the periphery is ink applied to the
specimen to identify the margins of resection.
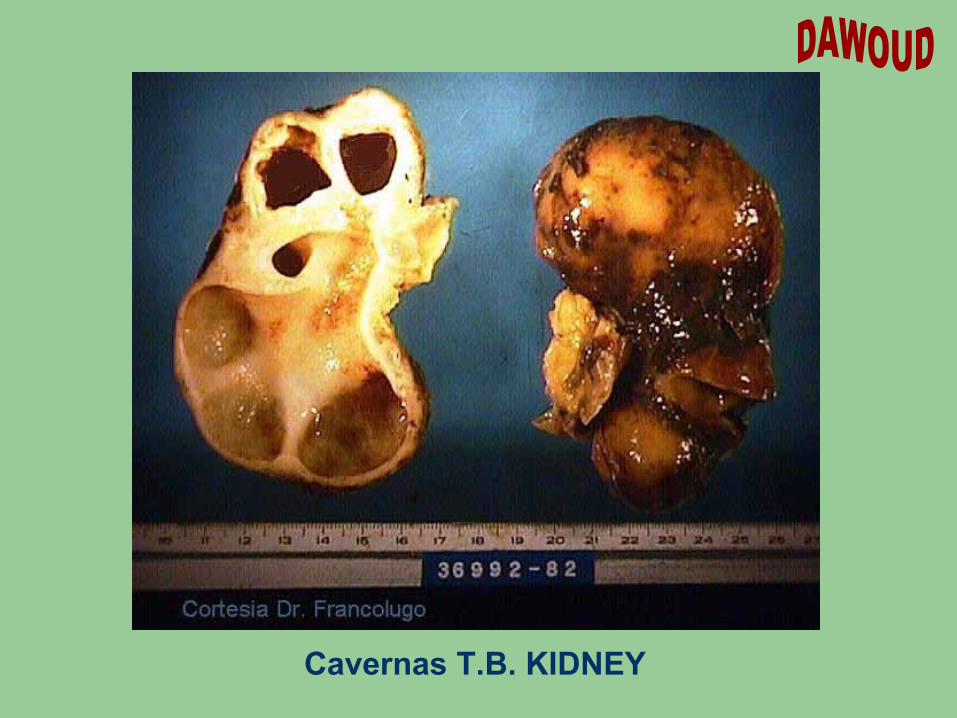
Cavernas T.B. KIDNEY

X-RAYSX-RAYS
By
Prof Dr IBRAHIM DAWOUD
Prof of Surgery
Mansoura University
How to read
X-RAY with dye
Vascular Plain X-Ray. Venography (Phlebography) Arteriography. DVI ( Digital Venous Image). DSA ( Digital Subtraction Angiography). CT scan. Duplex US. MRA.

How to readHow to read
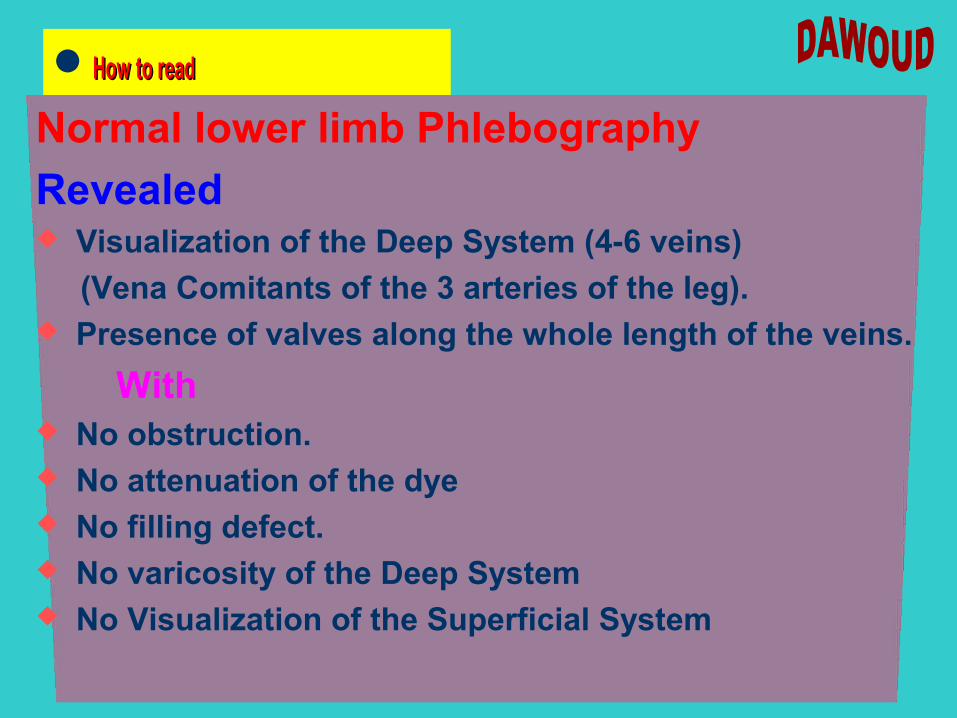
Normal lower limb Phlebography
Revealed Visualization of the Deep System (4-6 veins)
(Vena Comitants of the 3 arteries of the leg). Presence of valves along the whole length of the veins.
With No obstruction. No attenuation of the dye No filling defect. No varicosity of the Deep System No Visualization of the Superficial System




How to readHow to read
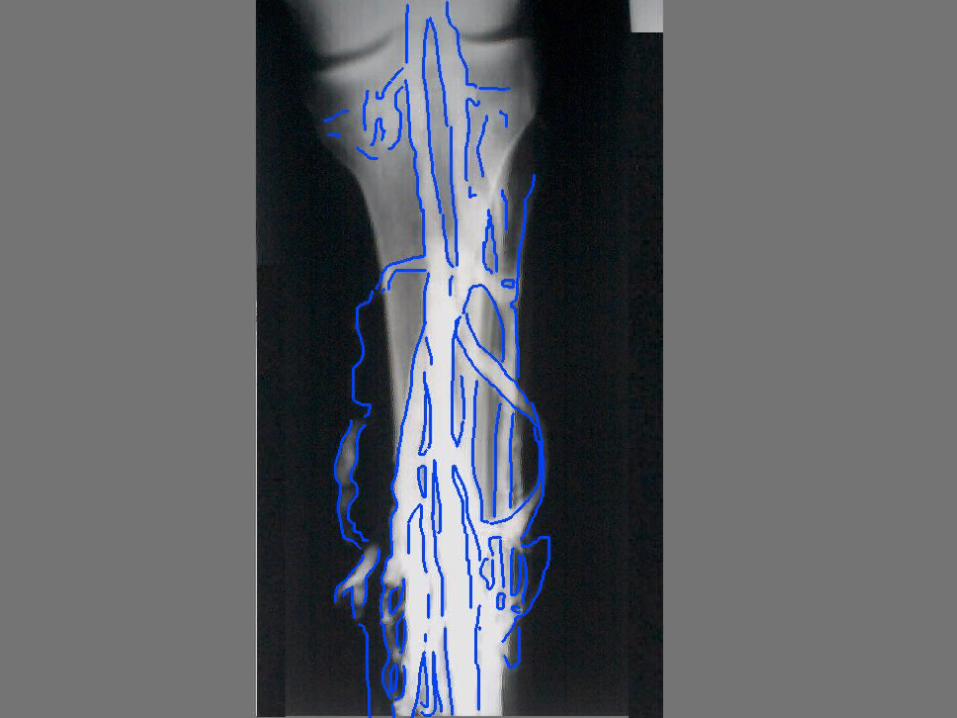
lower limb Phlebography
Revealed Visualization of the Deep System (4-6 veins)
With No obstruction. No attenuation of the dye No filling defect. No varicosity of the Deep System Visualization of the Superficial System, with varicosity
and Incompetent SF Valve
Primary Varicose Vein LSS of the LL
With Incompetent SFV

How to readHow to read
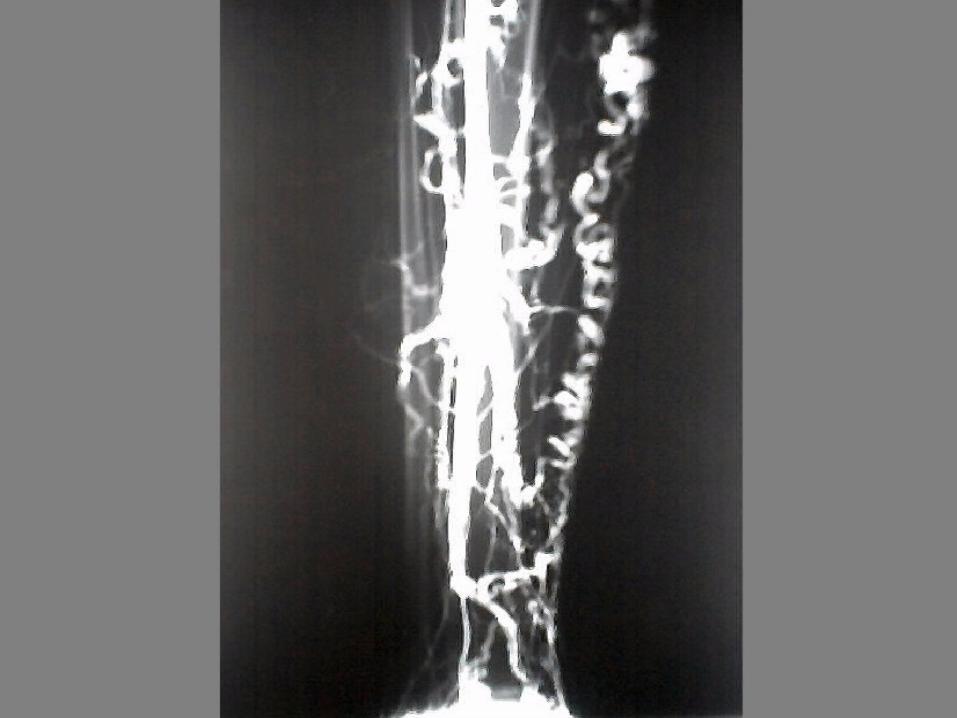
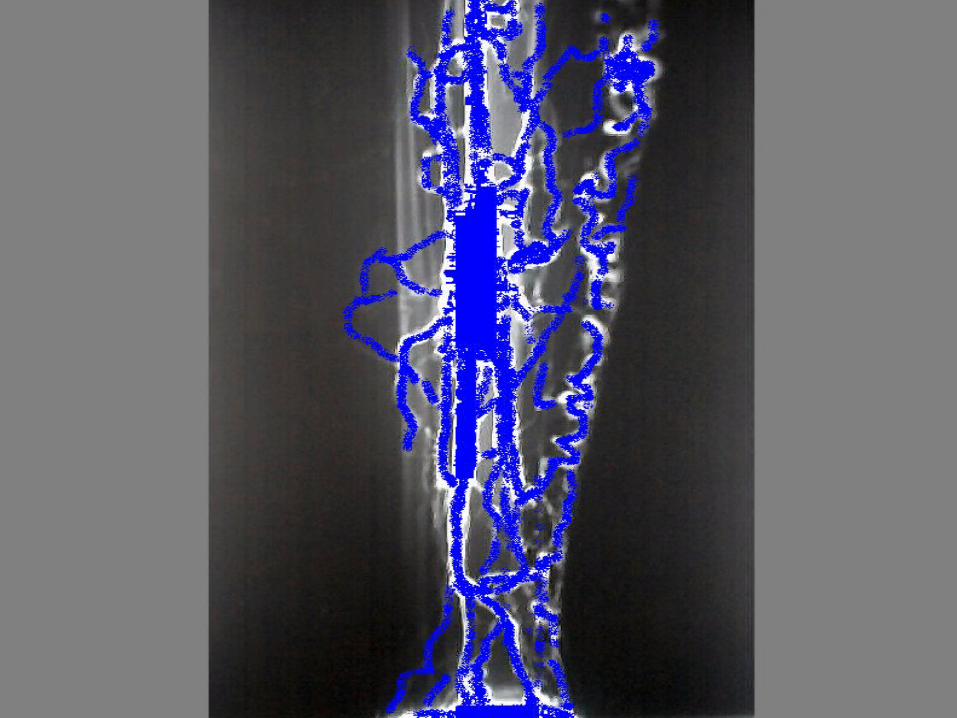
lower limb Phlebography
Revealed Visualization of some the Deep System (2 veins)
With Attenuation of the dye Varicosity of the Deep System Visualization of the Superficial System, with varicosity
and Incompetent SF Valve And With Incompetent Perforators
Secondary Varicose Veins
With Incompetent Leg Perforators


How to readHow to read
lower limb Phlebography
Revealed Visualization of some the Deep System (2 veins)
With Attenuation of the dye Varicosity of the Deep System Visualization of the Superficial System, with varicosity
and Incompetent SF Valve
AND With Incompetent Perforators
Secondary Varicose Veins
With Incompetent Leg Perforators


How to readHow to read
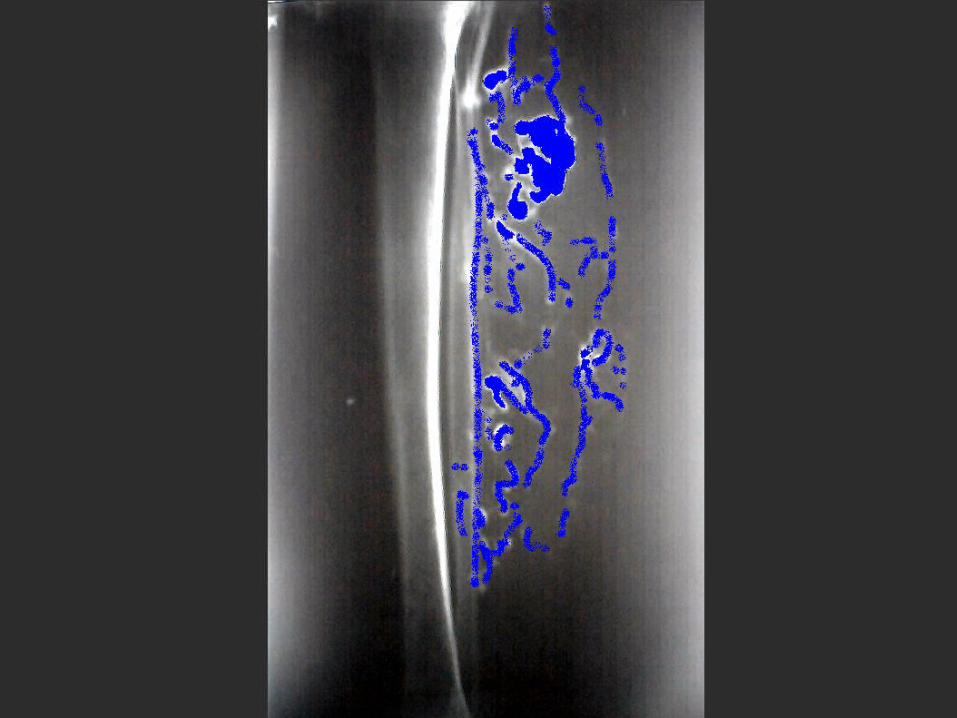
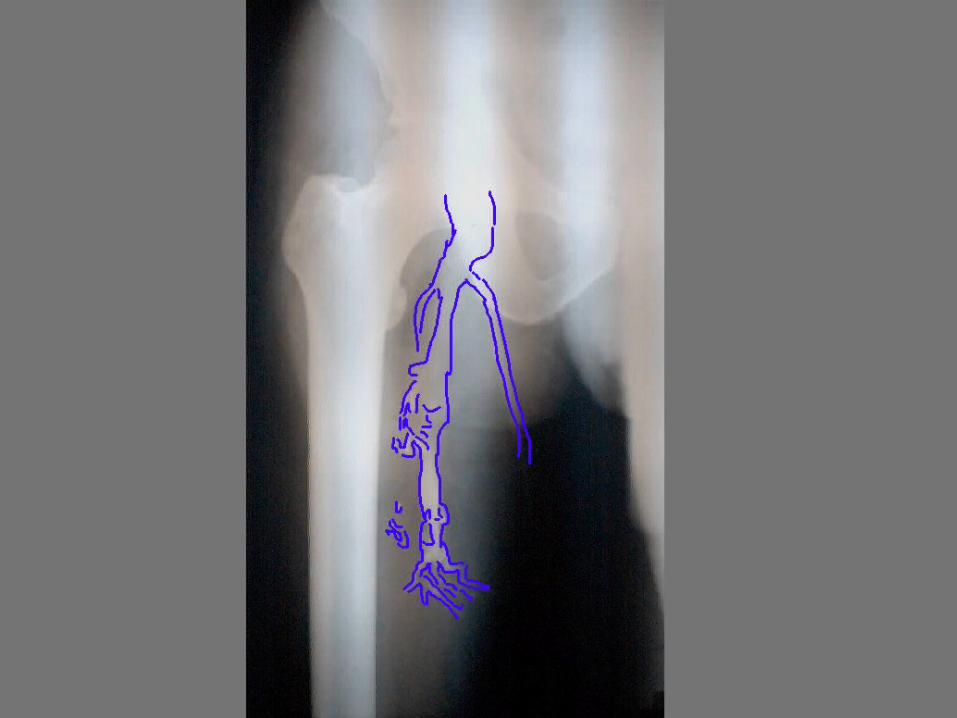
lower limb Phlebography
Revealed Failure of Visualization of some the Deep System apart
from the upper part of Femoral Vein.
With Attenuation of the dye Varicosity of the Femoral vein with no valves. Visualization of the Superficial System, with varicosity
and Incompetent SF Valve
Secondary Varicose Veins
With Deep Venous Obstruction
QUESTIONSQUESTIONS
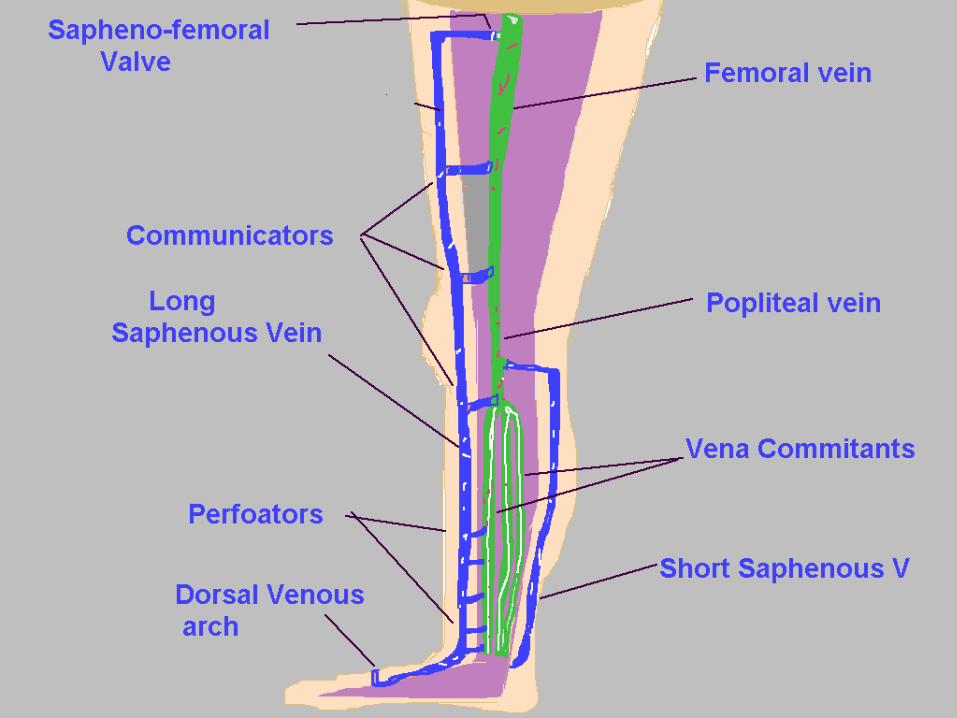
Anatomy of the Venous System of the lower limb. Etiology of Varicose Veins. Pathology of V.V. D.D. between Varicose ulcer and Postphlebitic ulcer. Clinical picture. Other investigations. Treatment.
1ry VV 2ry VV


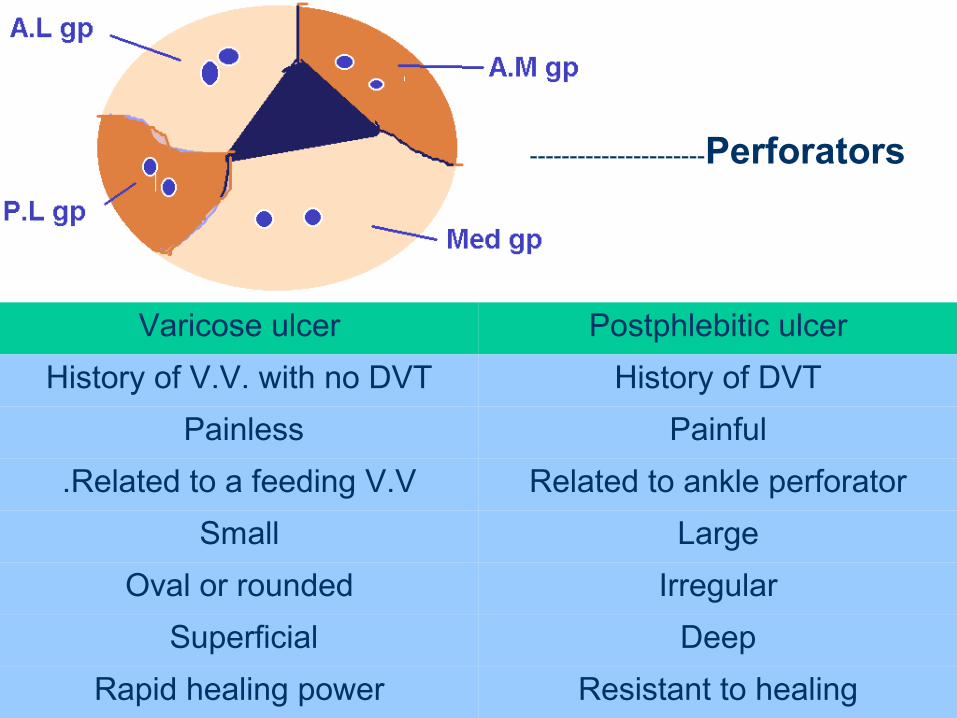
Varicose ulcer Postphlebitic ulcer
History of V.V. with no DVT History of DVT
Painless Painful
Related to a feeding V.V. Related to ankle perforator
Small Large
Oval or rounded Irregular
Superficial Deep
Rapid healing power Resistant to healing
----------------------Perforators
Treatment
1ry V.V.1- Conservative 4- Triple ligation
2- Injection sclerotherapy 5- Trendlenberg op
3- Localized stripping 6- Trendlenberg & Stripping
2ry V.V.
1- 2ry to DVT A- Actual DVT treatment of DVT
B- Postphlebitic leg
D.V. Insufficiency D.V. Obstruction
C- Perforators without ulcer
D- Perforators with ulcer
2- 2ry to other causes

How to readHow to read
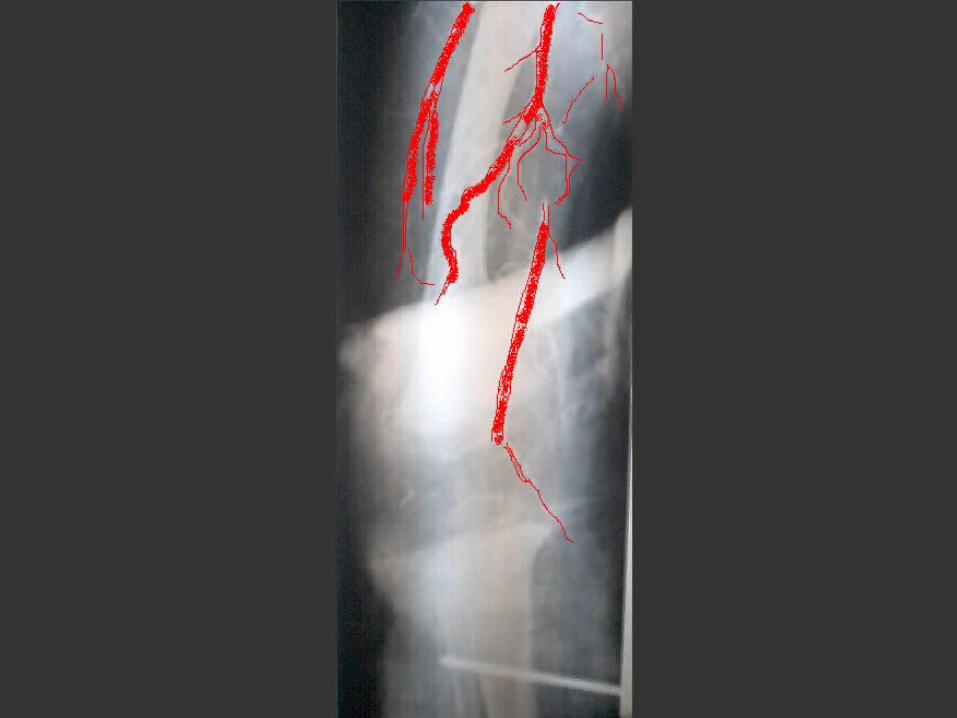
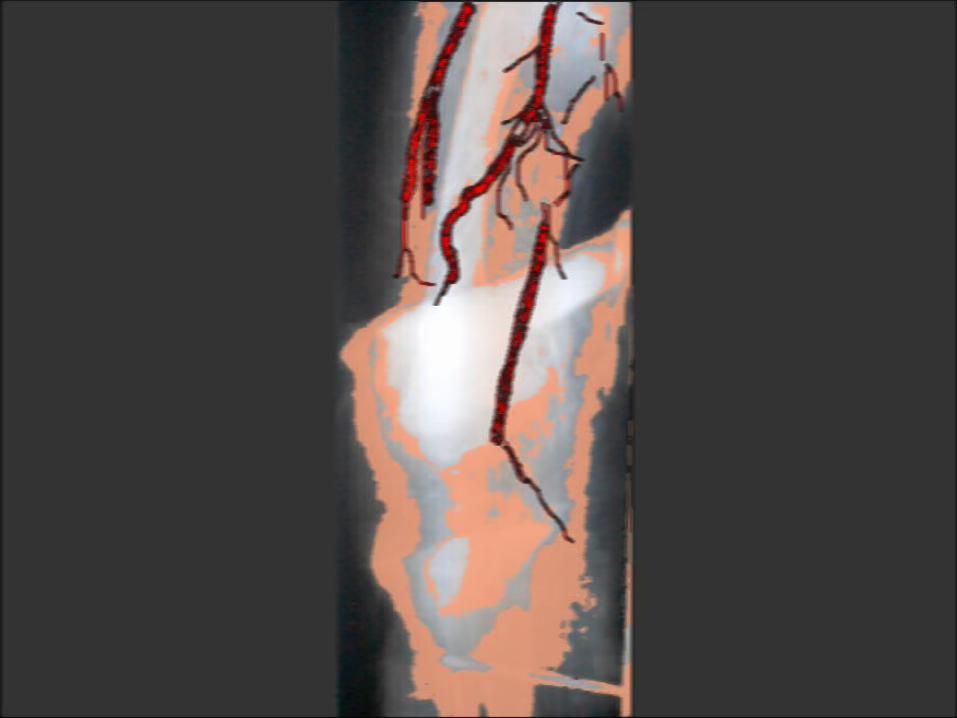
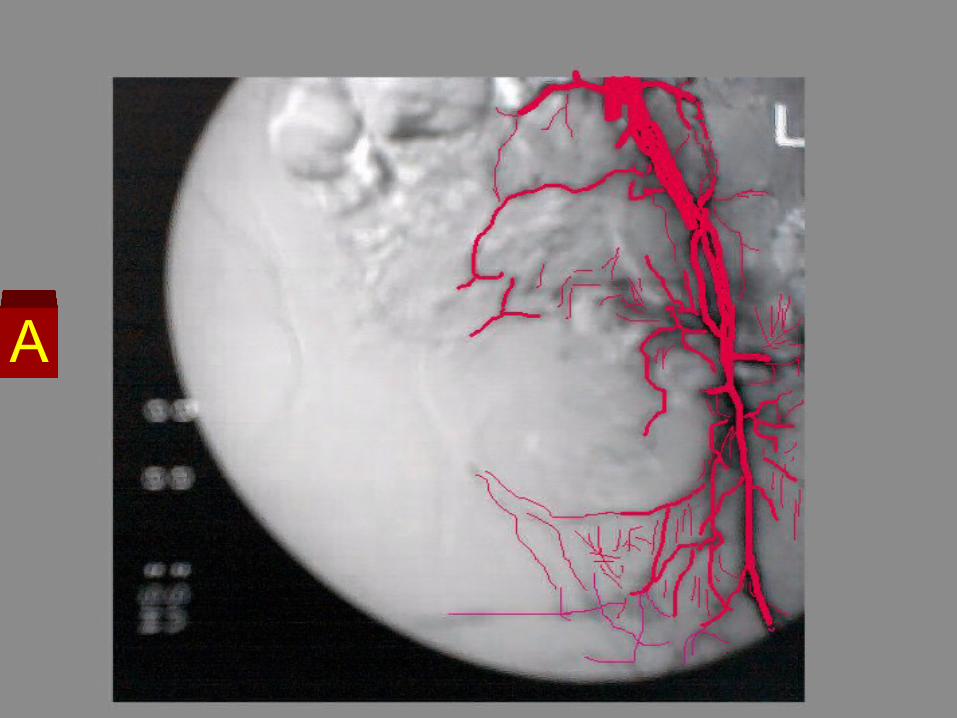
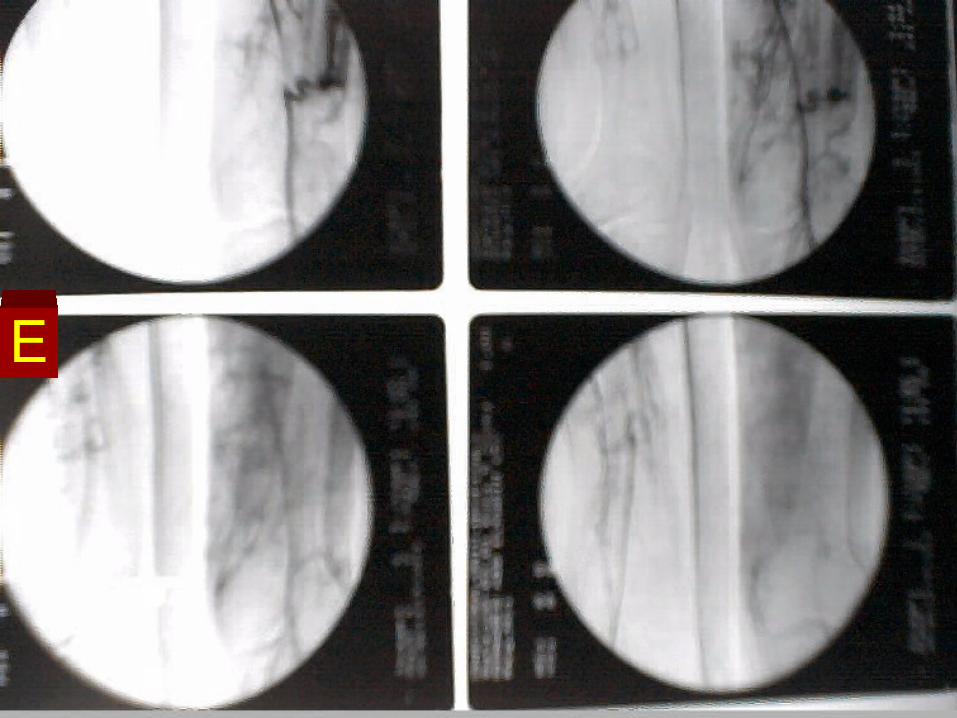
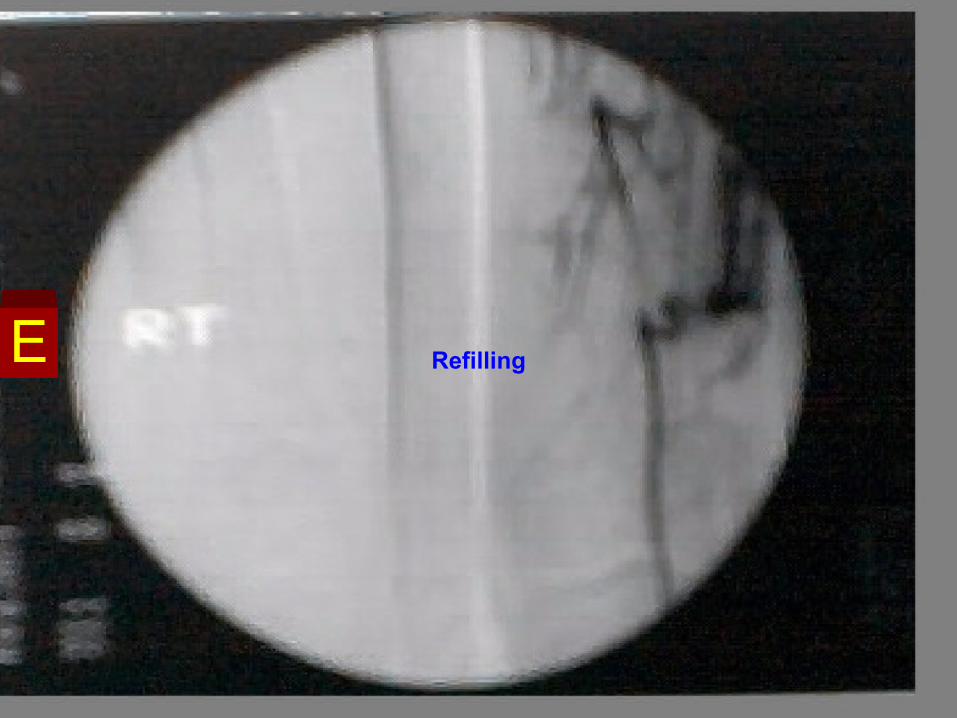
Femoral Angiography
Revealed Total occlusion of the Superficial Femoral Artery just
at its origin. Hypertrophied Deep Femoral Artery. Distal refilling of the middle third of the Deep Femoral
artery through collaterals. Total occlusion of the supragenicular portion of the
Popliteal artery with no distal run off. No distal run off or opacification of the leg arteries. Fracture of the lower end femur with nail fixation.
Acute Ischemia ( post traumatic)
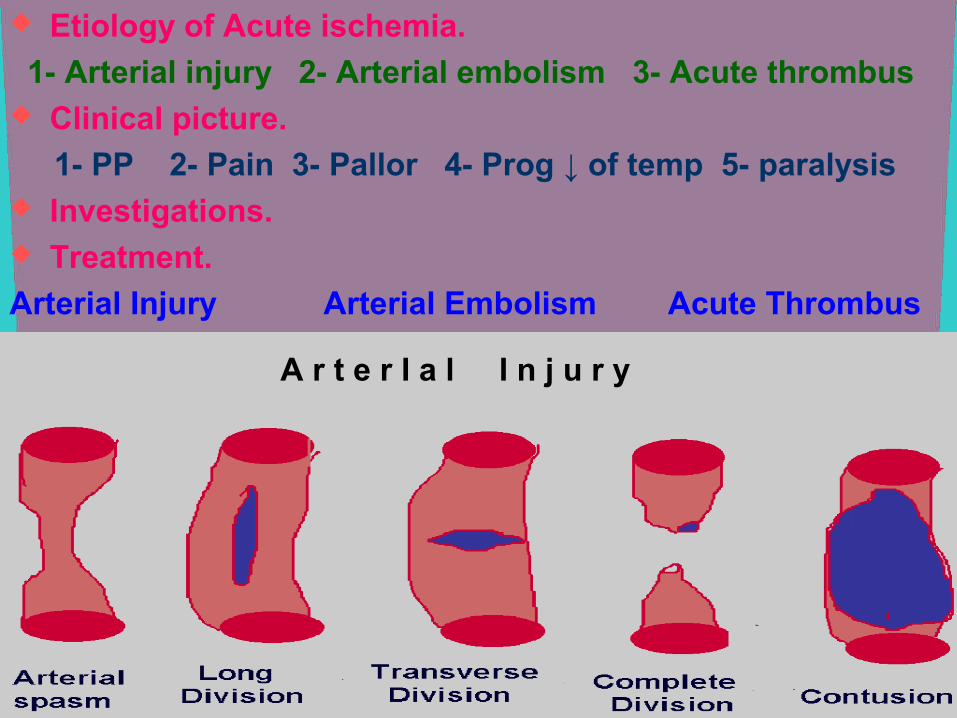
Etiology of Acute ischemia.
1- Arterial injury 2- Arterial embolism 3- Acute thrombus Clinical picture.
1- PP 2- Pain 3- Pallor 4- Prog ↓ of temp 5- paralysis Investigations. Treatment.
Arterial Injury Arterial Embolism Acute Thrombus
A r t e r I a l I n j u r y
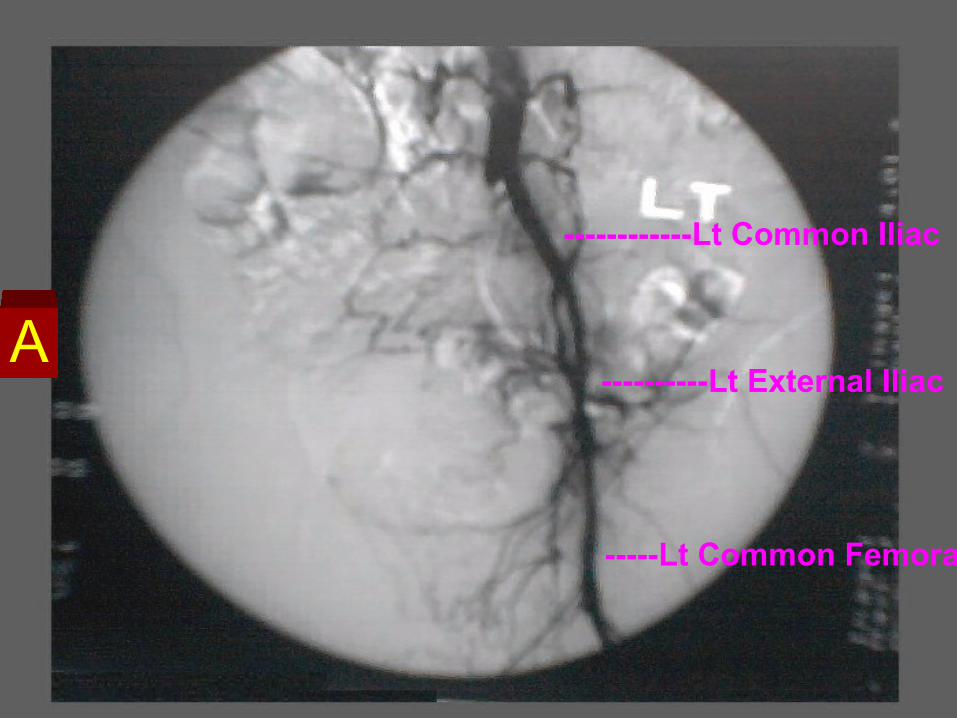
------------Lt Common Iliac
----------Lt External Iliac
-----Lt Common Femoral
A
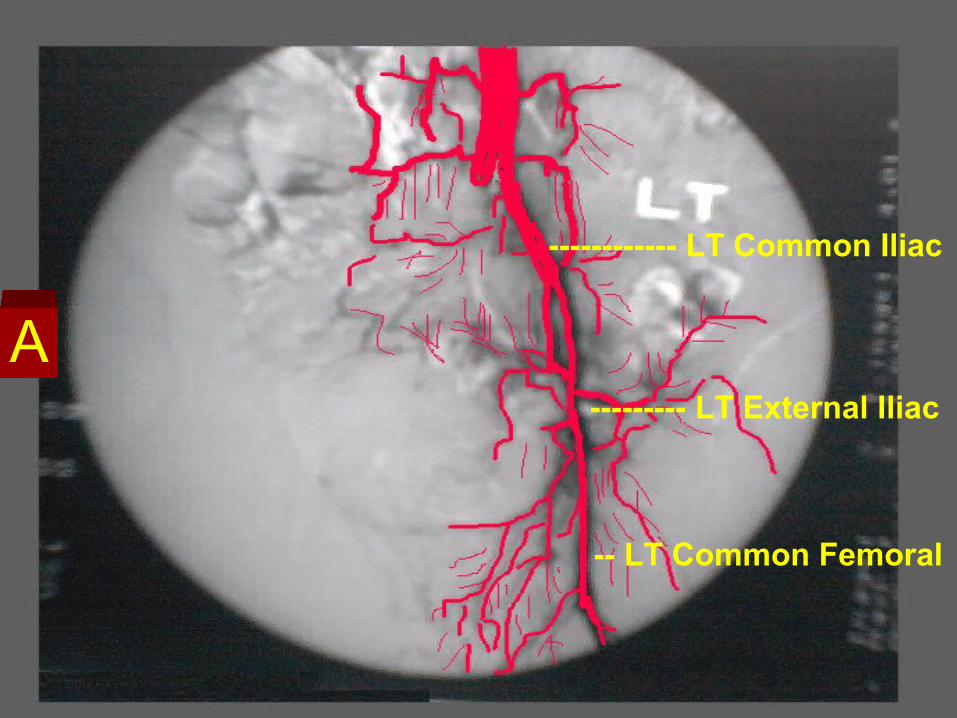
------------ LT Common Iliac
--------- LT External Iliac
-- LT Common Femoral
A
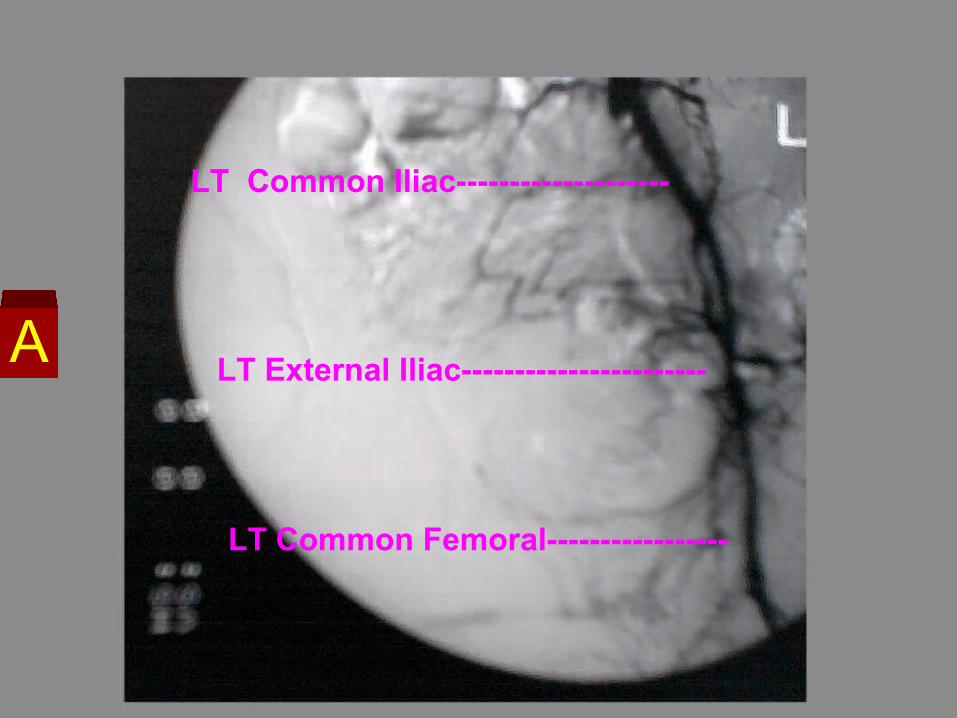
LT Common Iliac--------------------
LT External Iliac-----------------------
LT Common Femoral-----------------
A
A
B
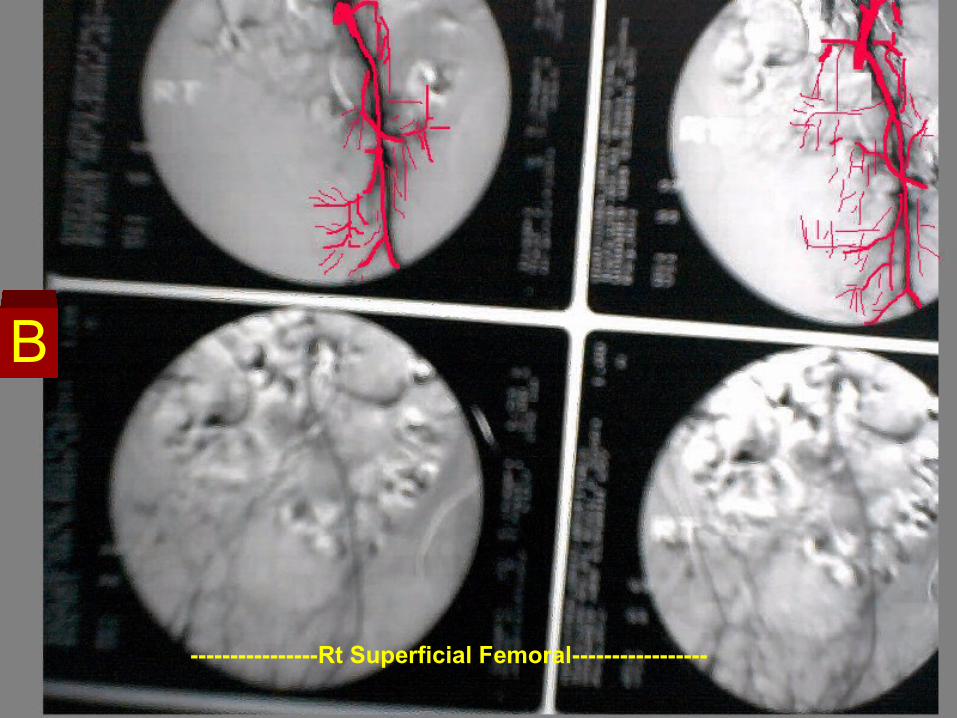
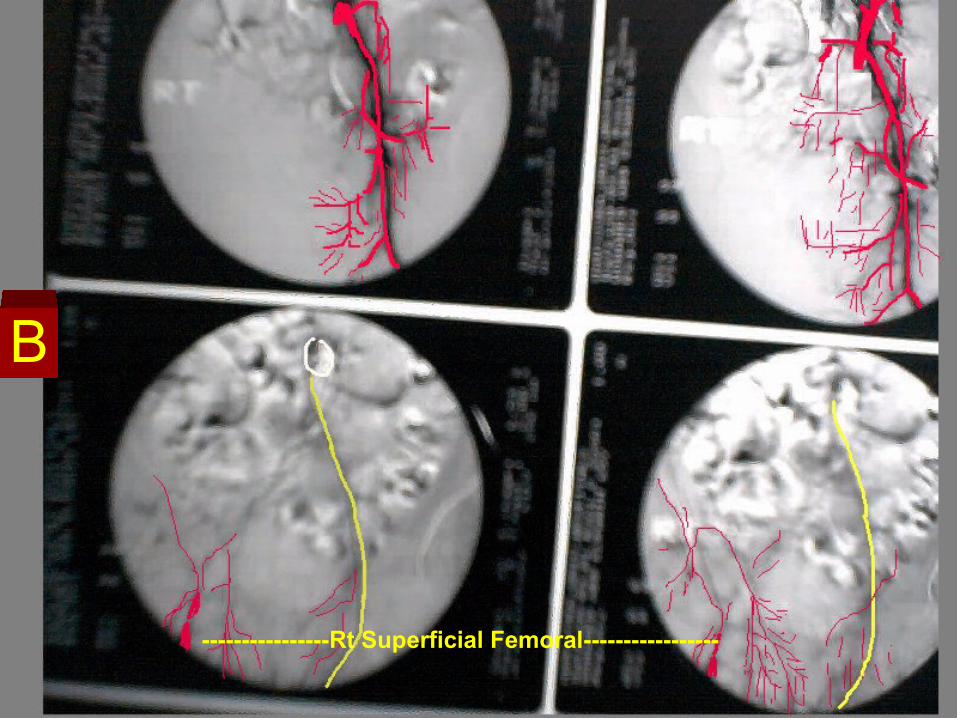
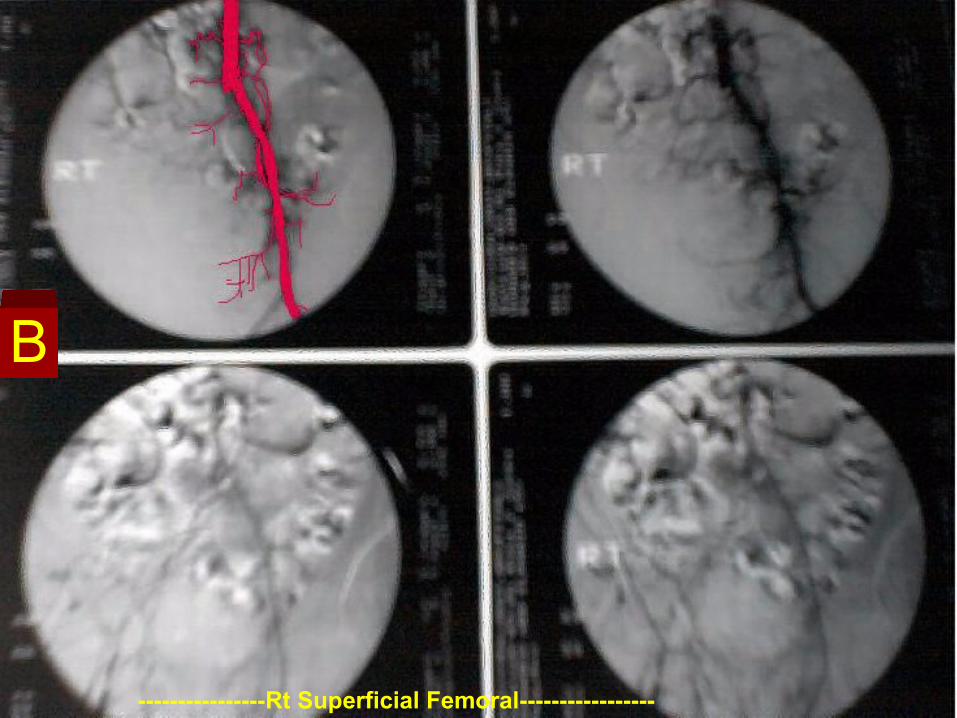
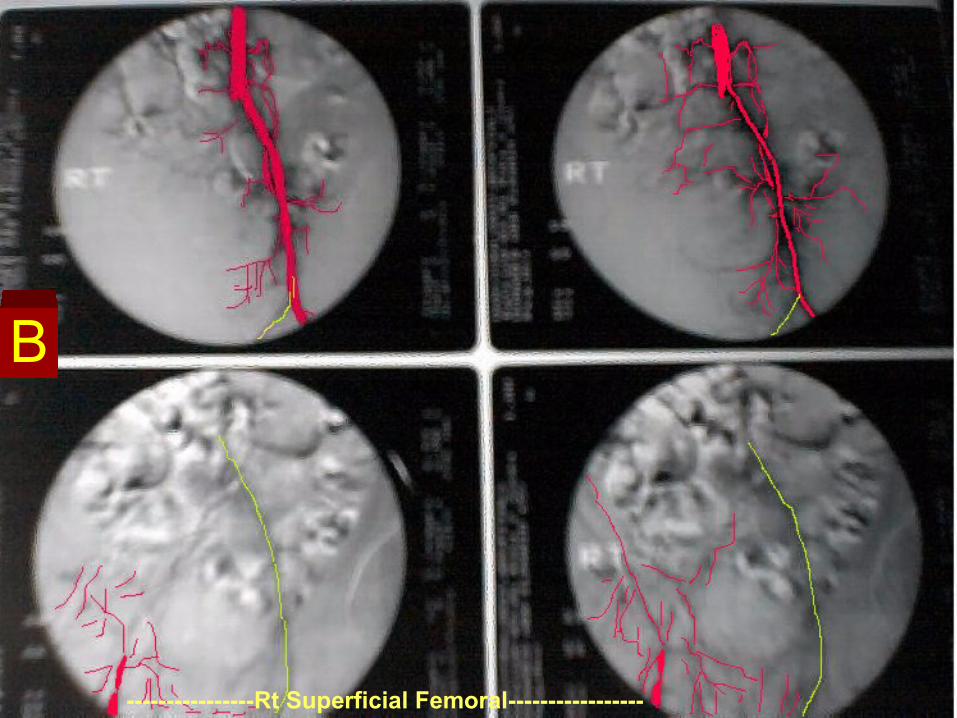
----------------Rt Superficial Femoral-----------------
B
----------------Rt Superficial Femoral-----------------
B
B
----------------Rt Superficial Femoral-----------------
B
----------------Rt Superficial Femoral-----------------
B
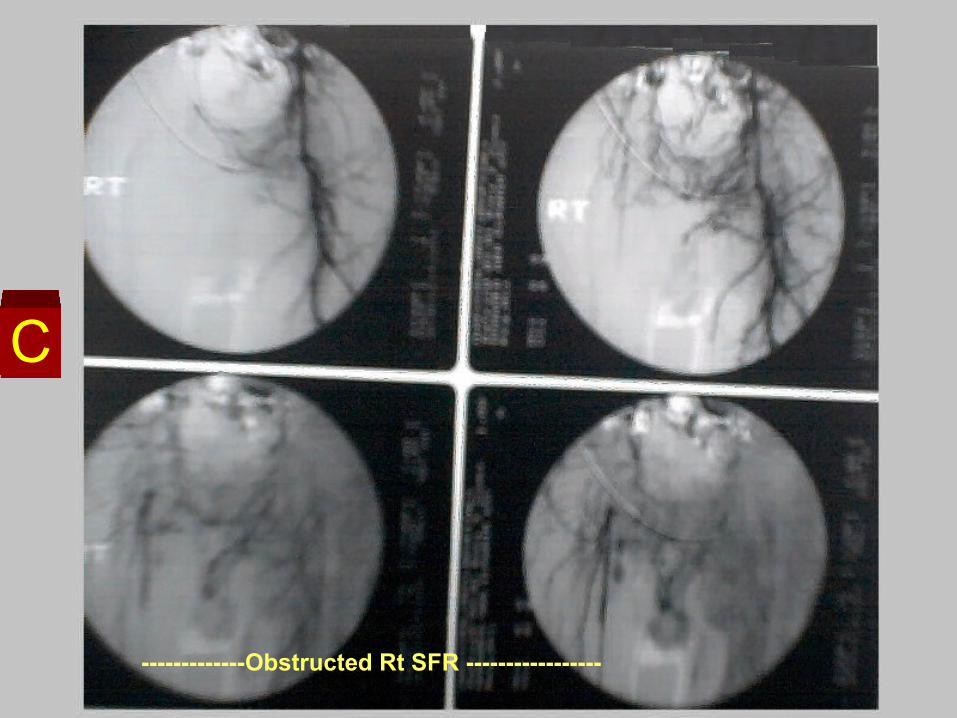
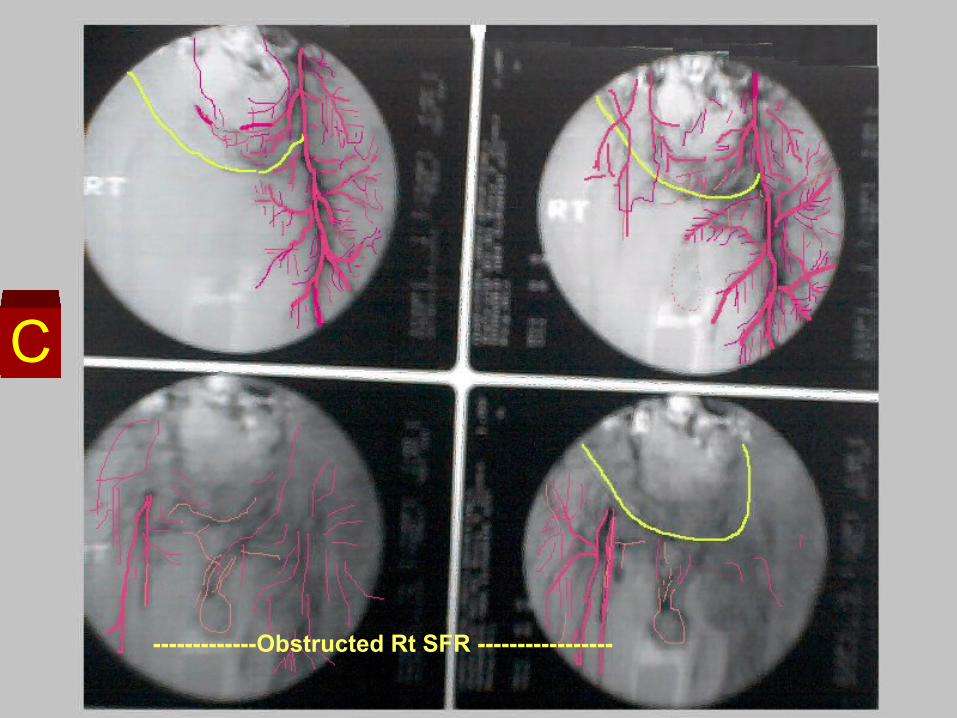
-------------Obstructed Rt SFR -----------------
C
-------------Obstructed Rt SFR -----------------
C
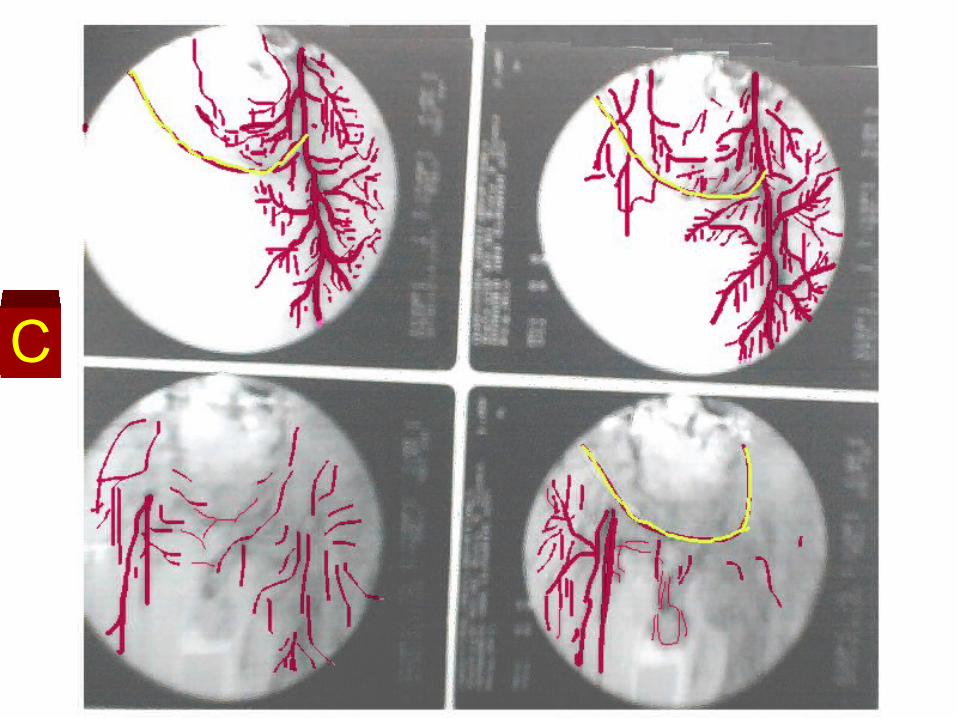
C
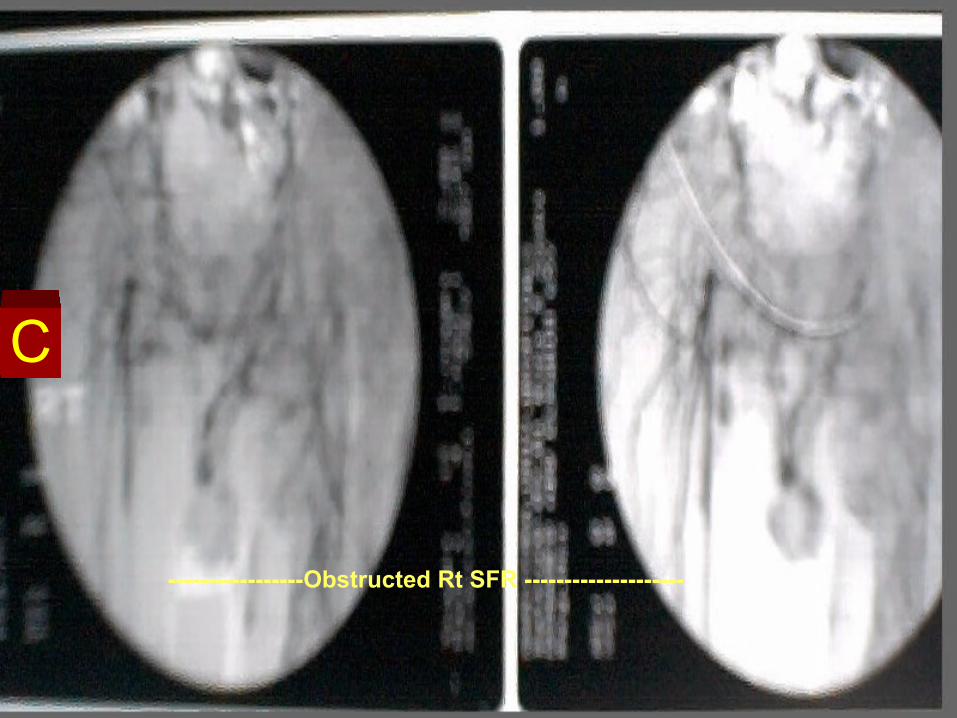
-----------------Obstructed Rt SFR --------------------
C
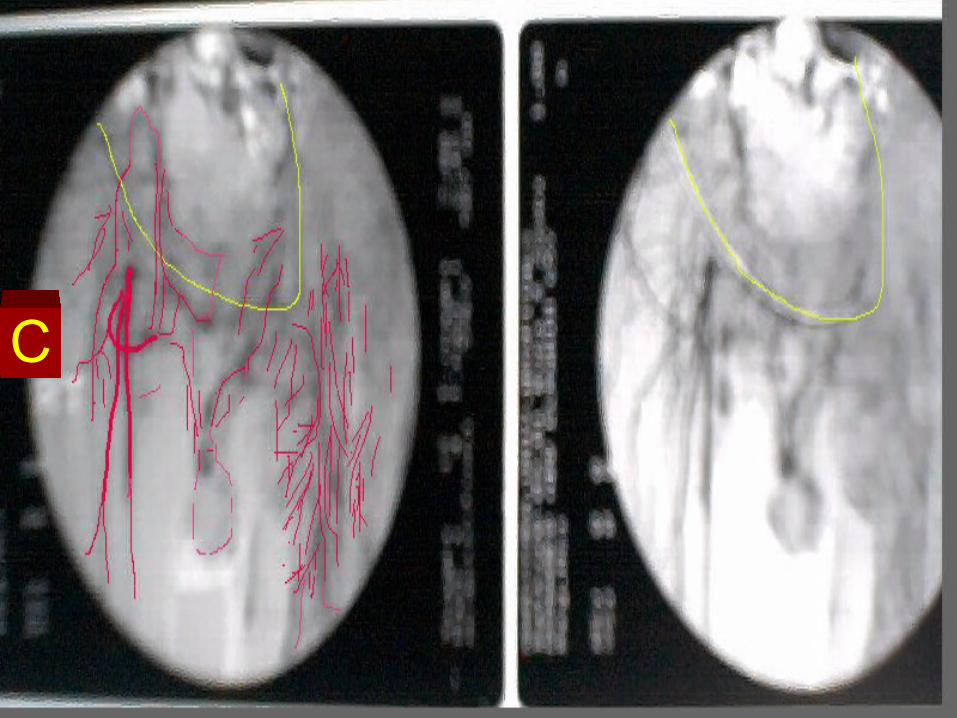
C
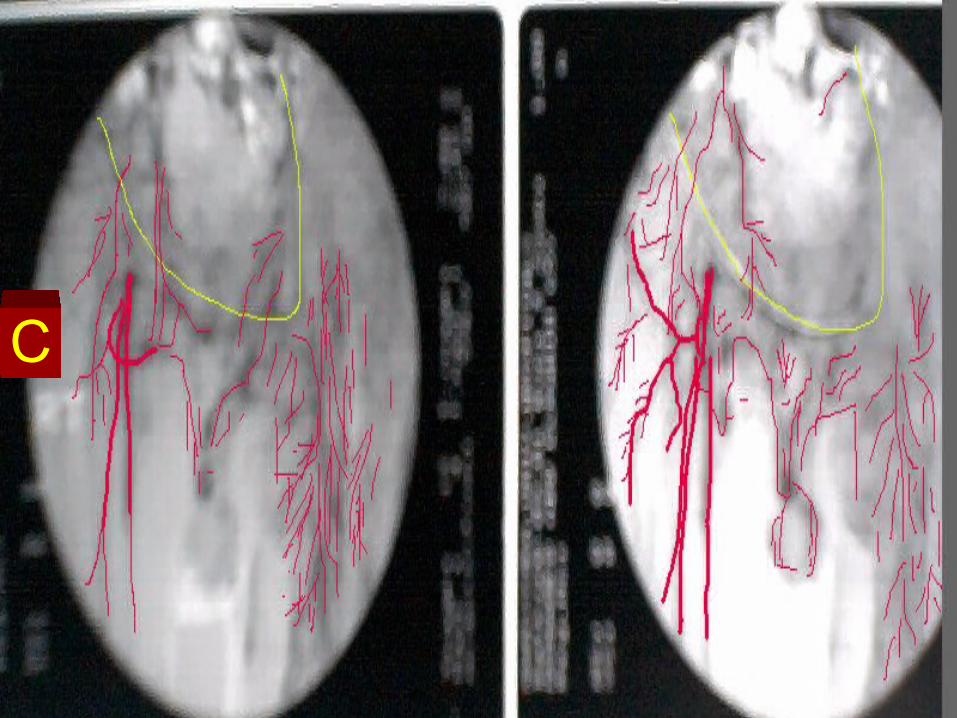
C
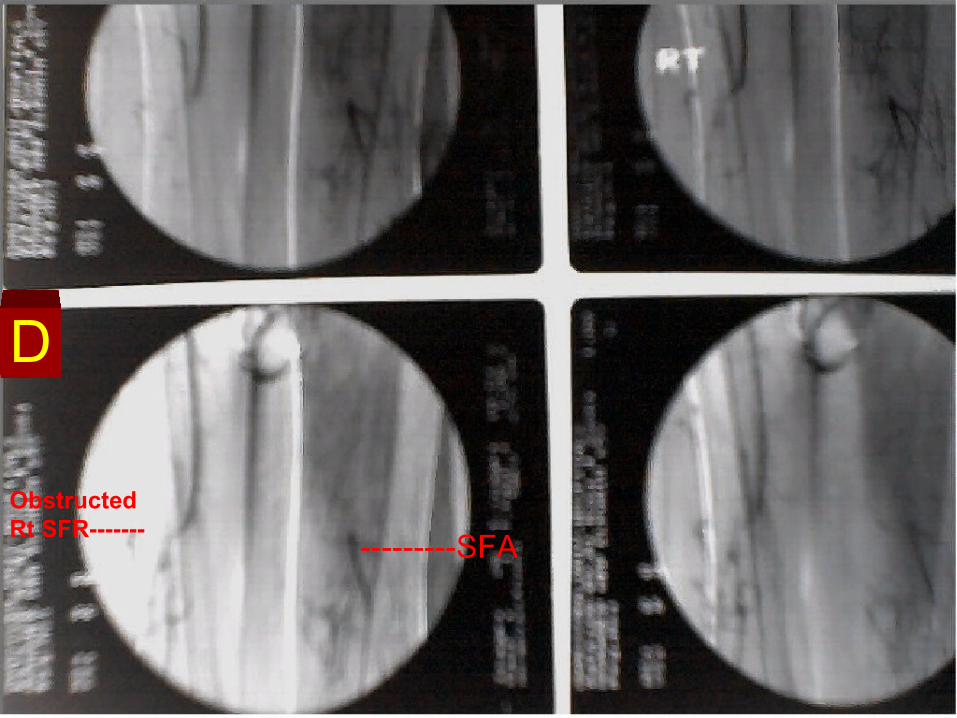
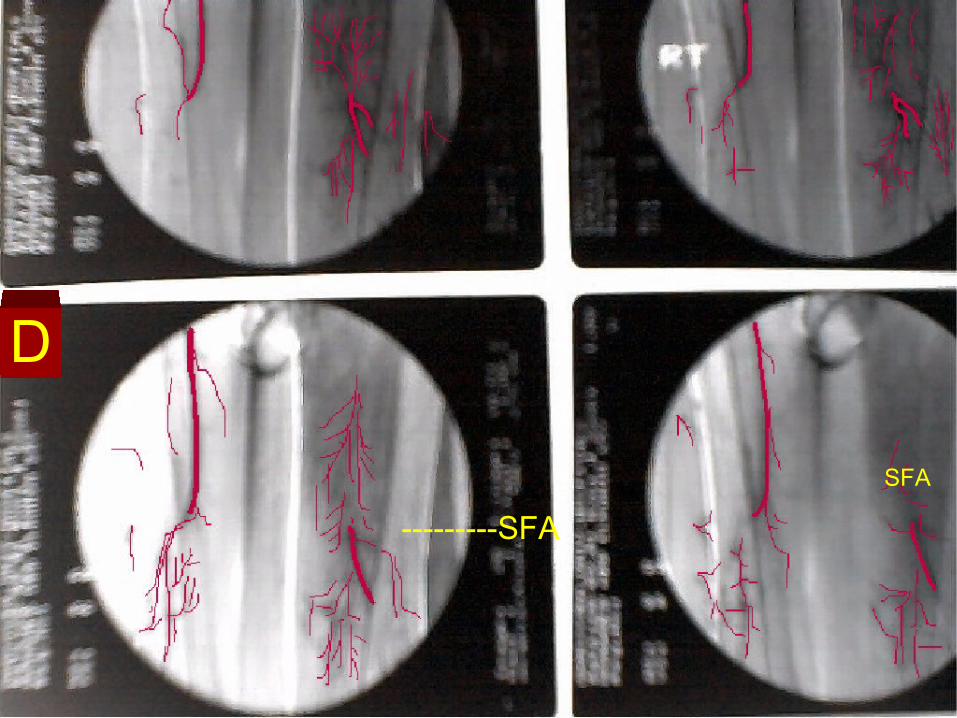
Obstructed Rt SFR-------
---------SFA
D
---------SFA
SFA
D
D
SFASFA
D
E
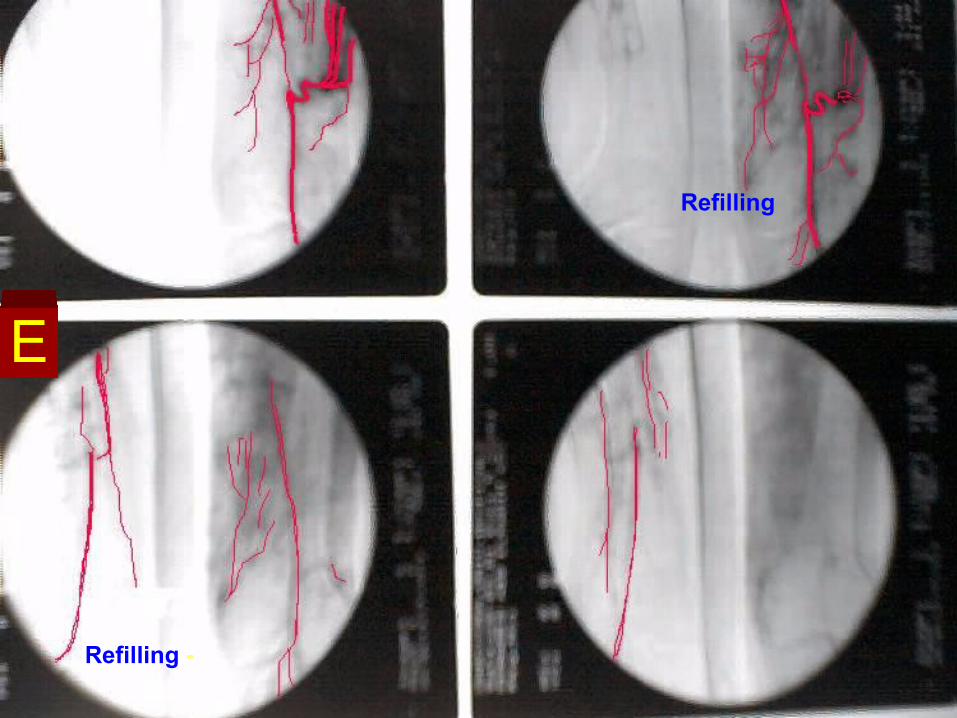
Refilling -
Refilling
E
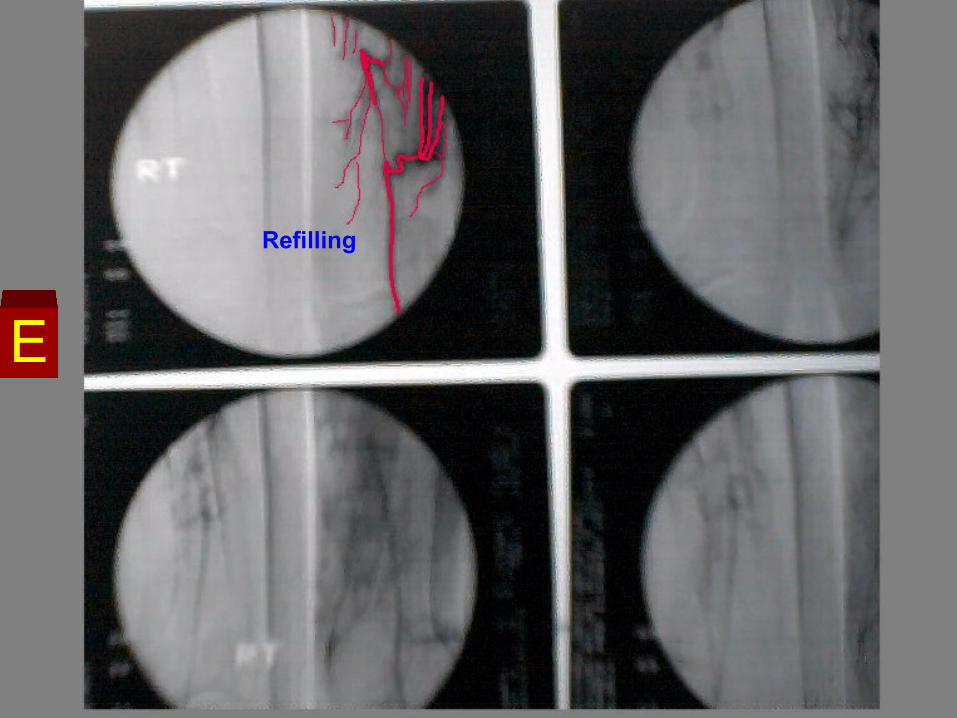
Refilling
E
RefillingE
RefillingE
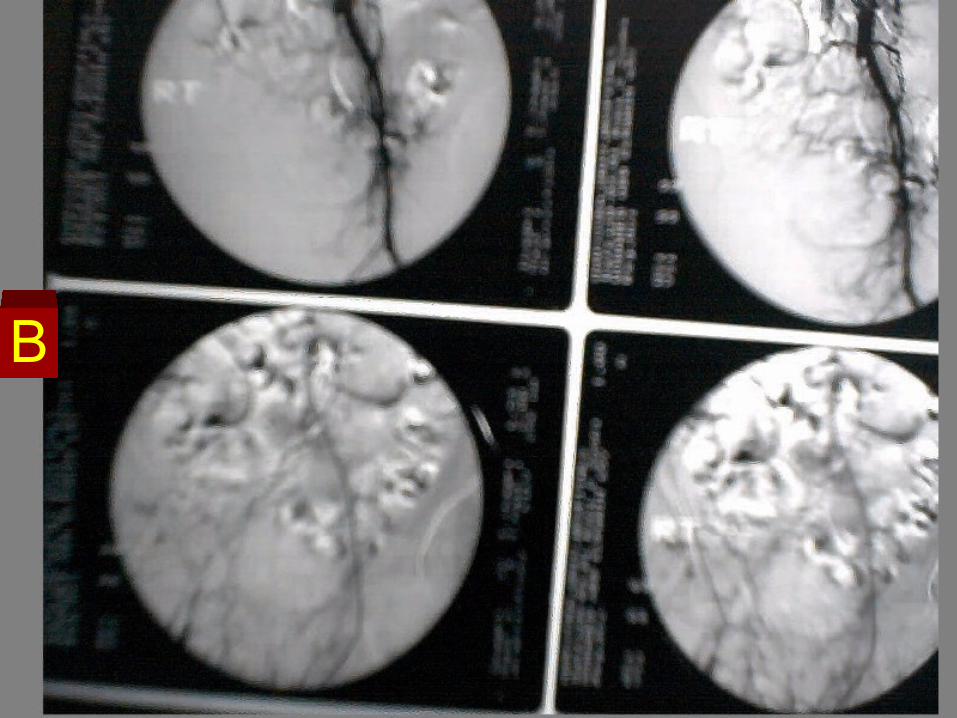
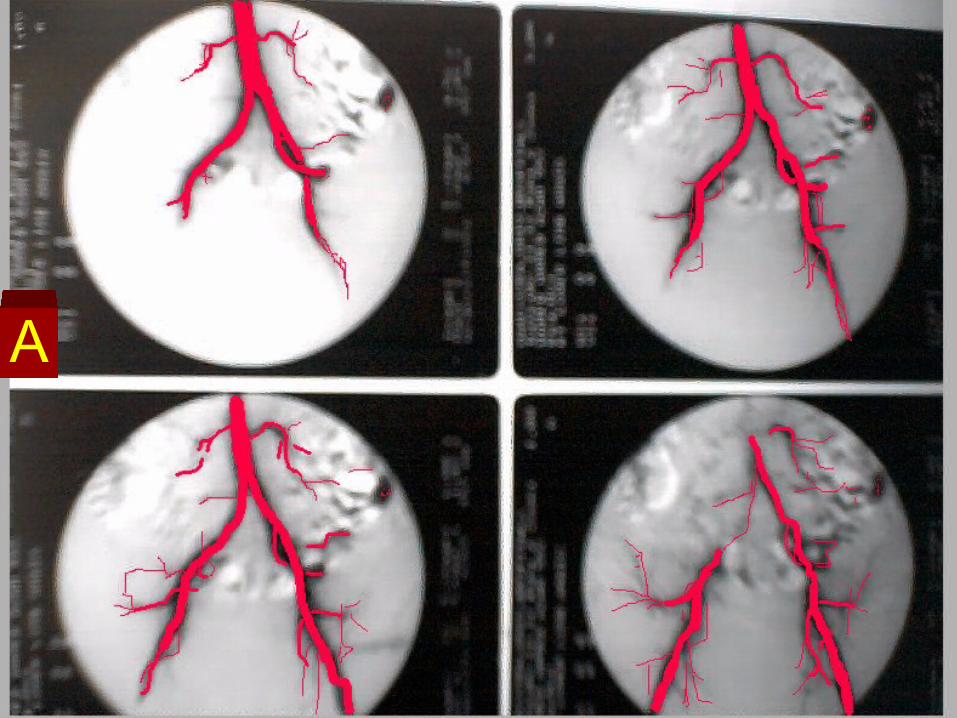
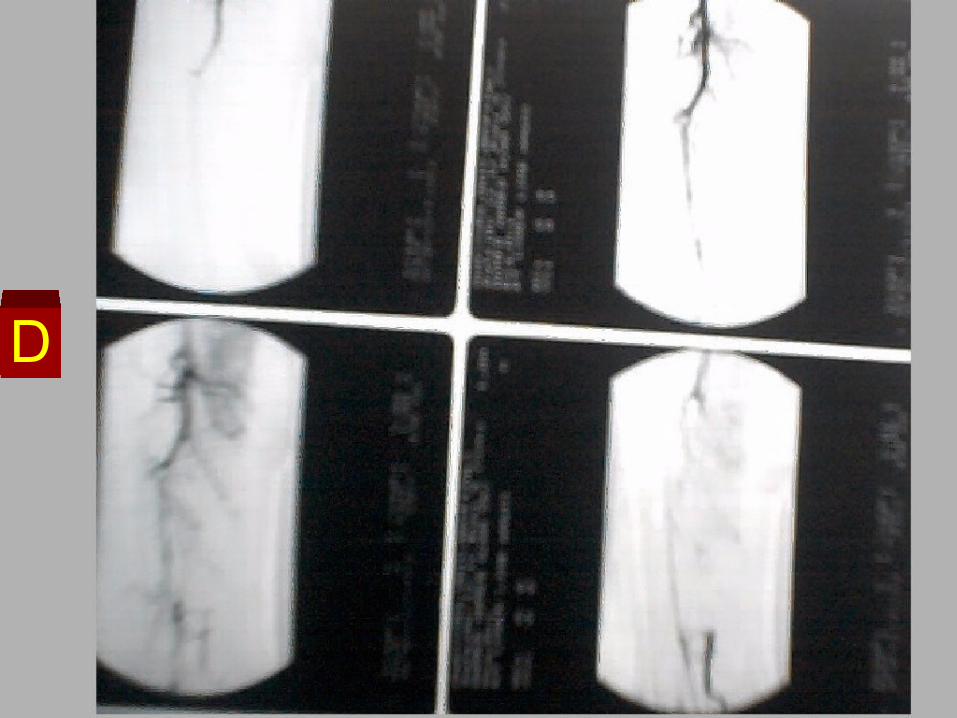
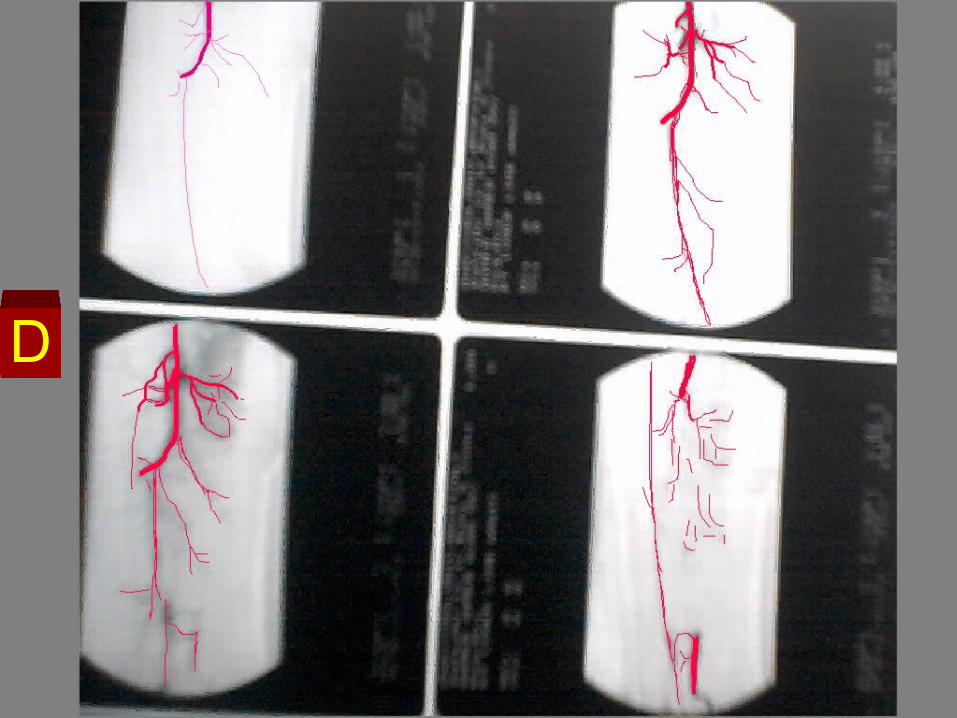
How to readHow to read
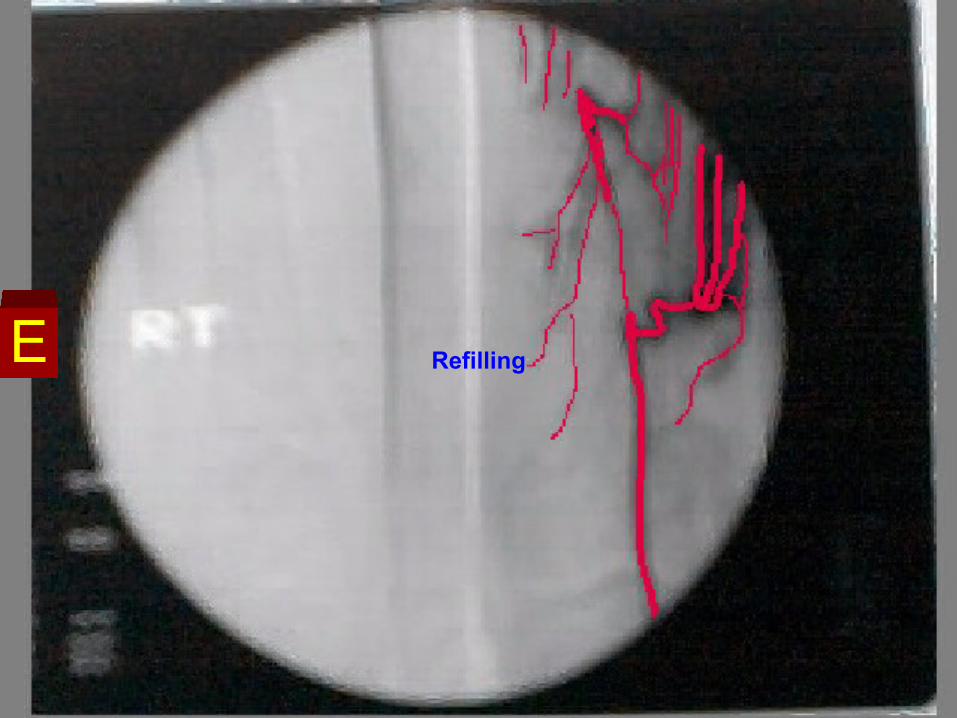
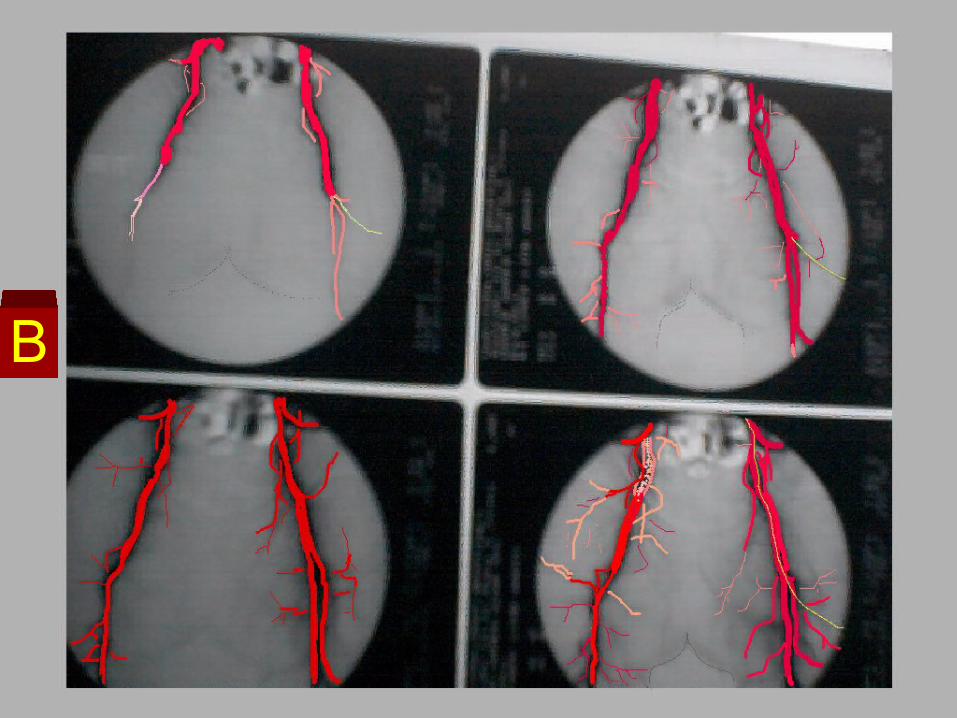
Bilateral lower limb Angiography
Right L.L
Total occlusion of the Rt Common iliac artery, External Iliac artery, and Common Femoral Artery.
The Rt Superficial Femoral Artery is seen refilled through collaterals.
With obstruction of its lower part at the Adductor canal.
Distal refilling of the Rt Popliteal artery through collaterals
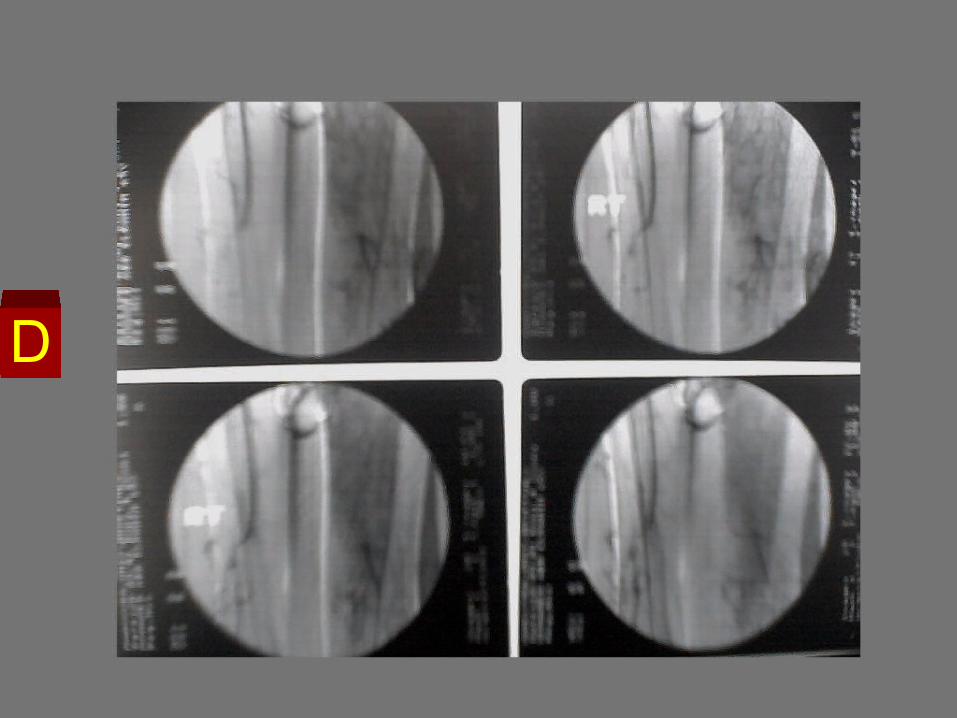
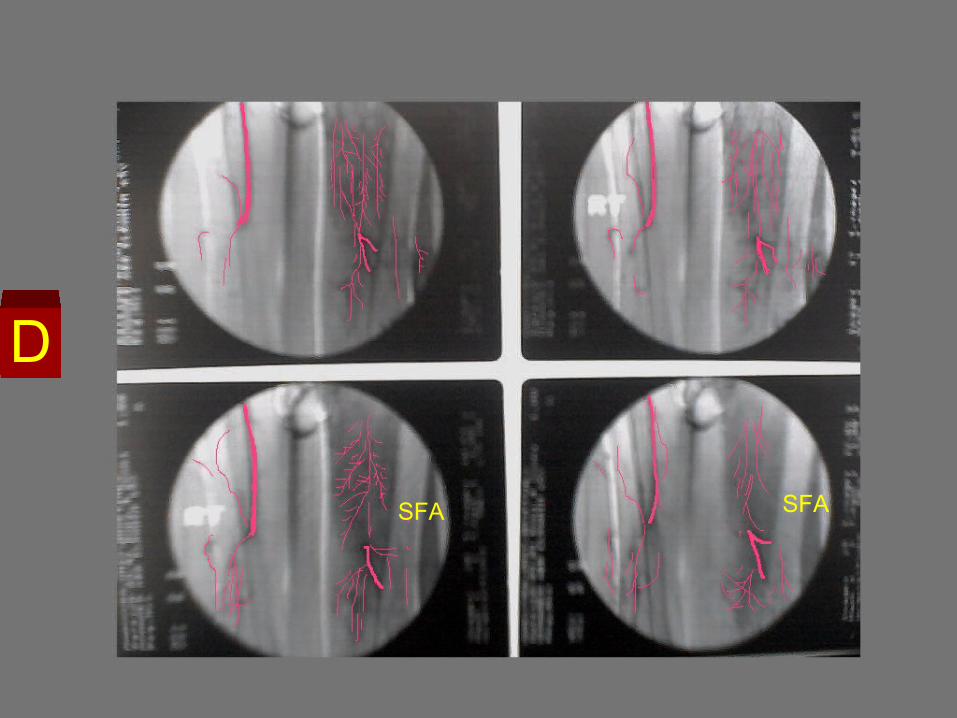
Bilateral lower limb Angiography
Left L.L
Normal Left Common Iliac, Left External Iliac, and Left Common Femoral Arteries.
Total Occlusion of the Left SFA, at its origin from the Lt CFA.
Refilling of the SFA at the mid thigh from collaterals.
Opacified left Popliteal artery.
A
A
A
A
B
B
C
C
C
D
D
D
D
E
E
F
F
G
G
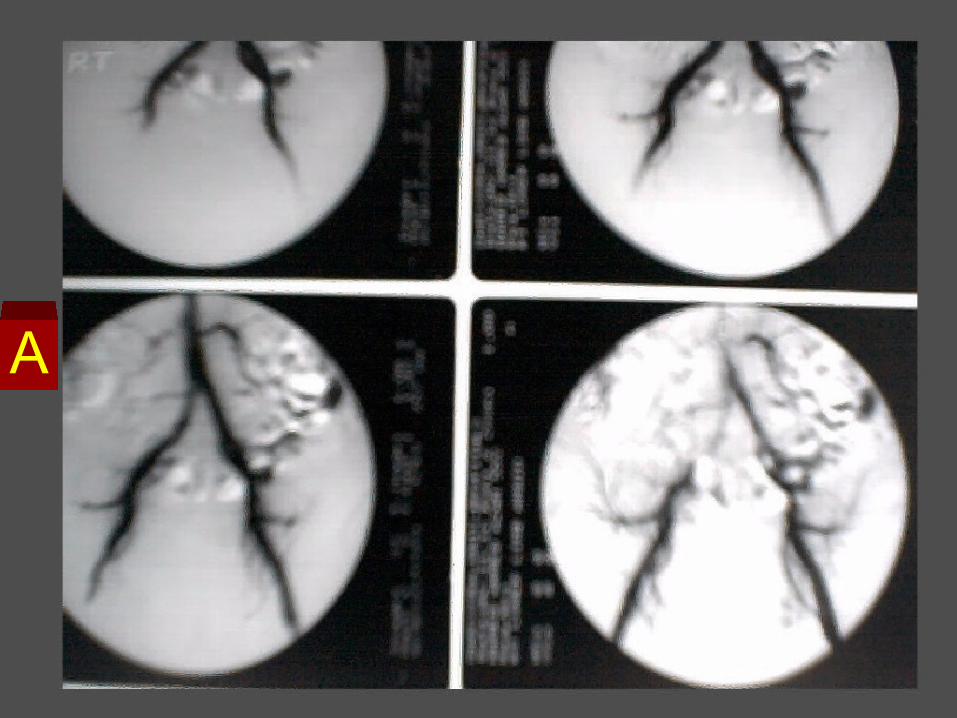
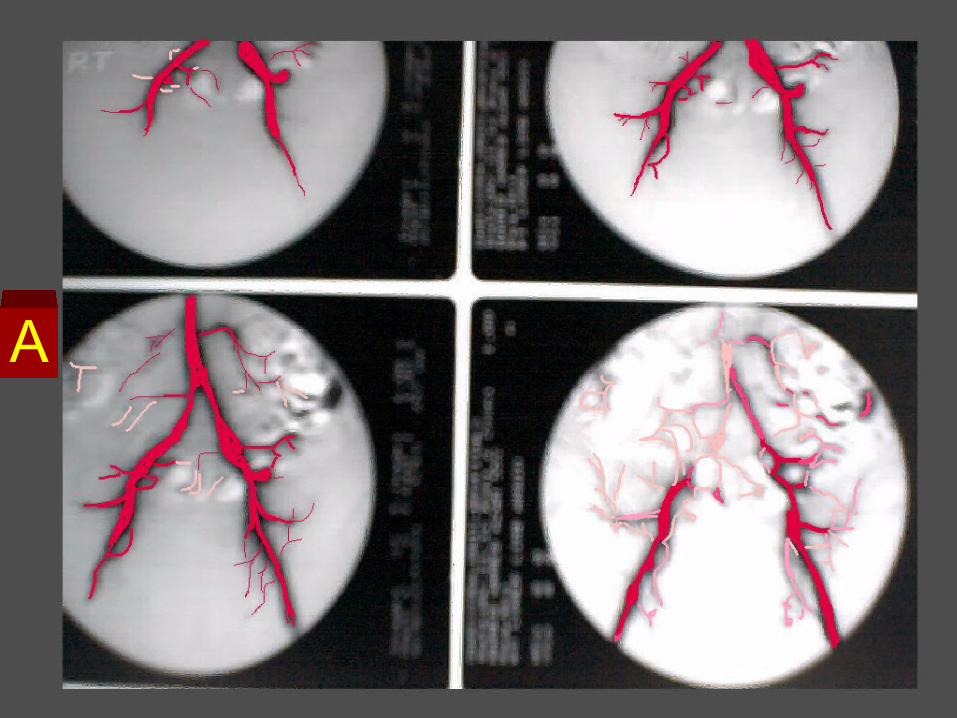
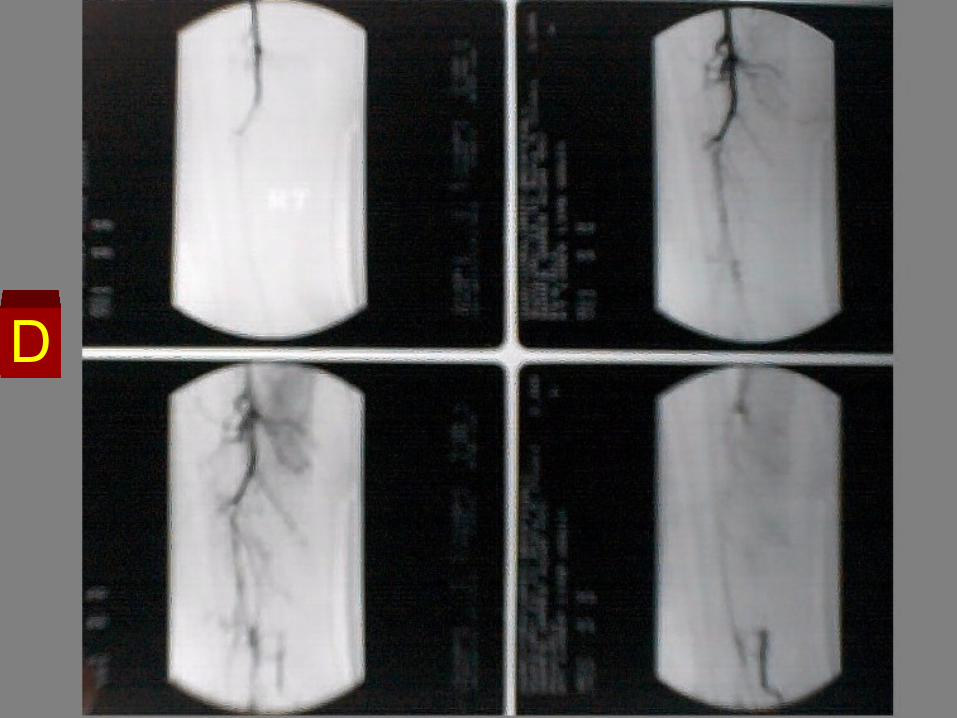
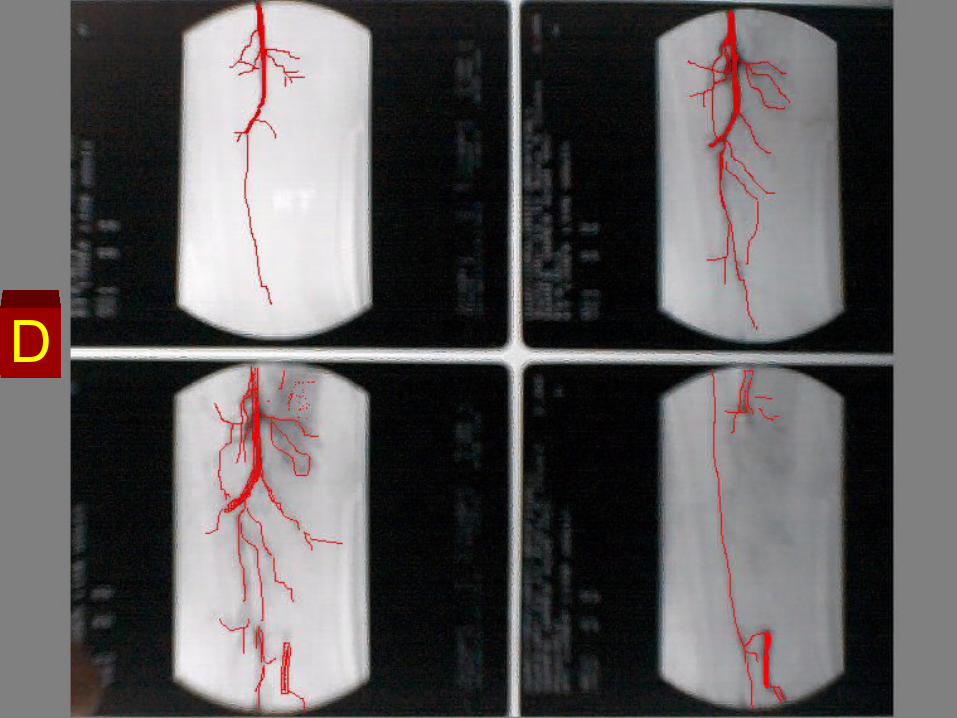
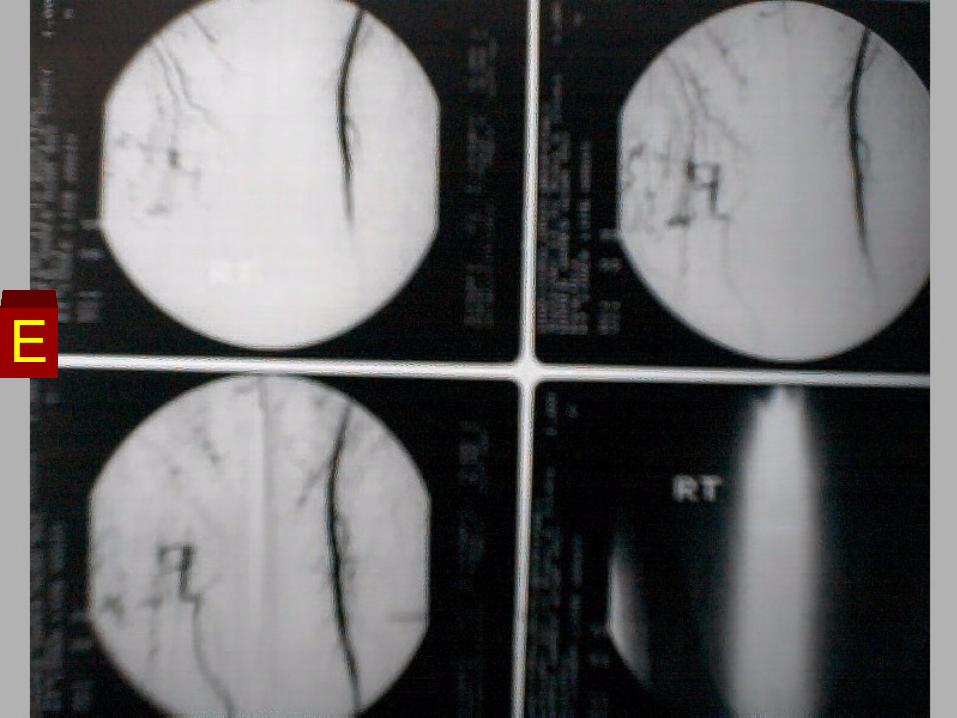
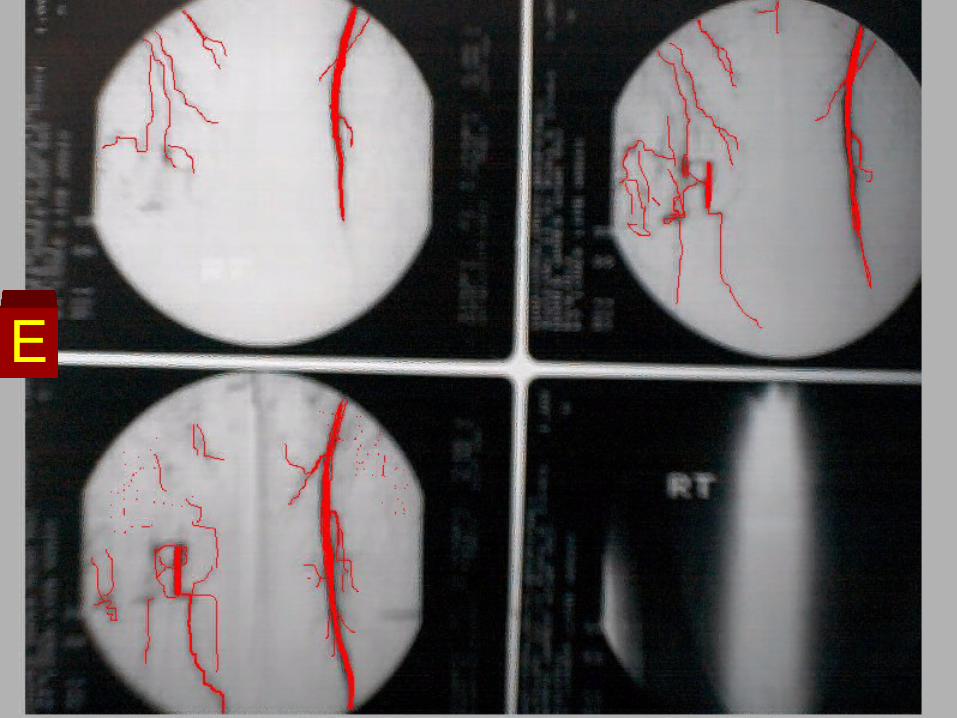
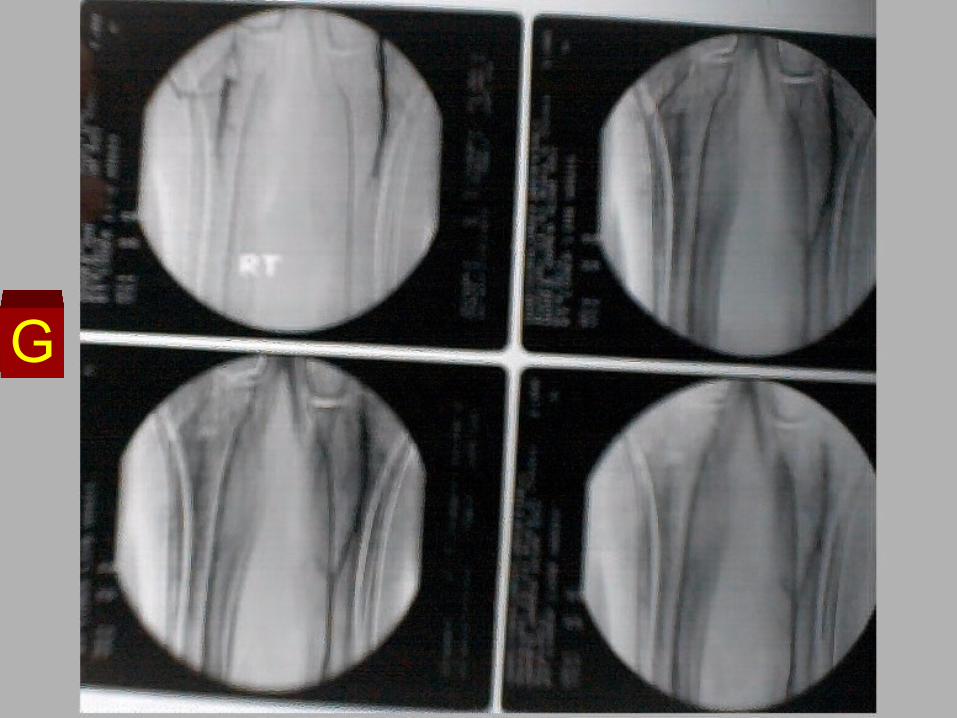
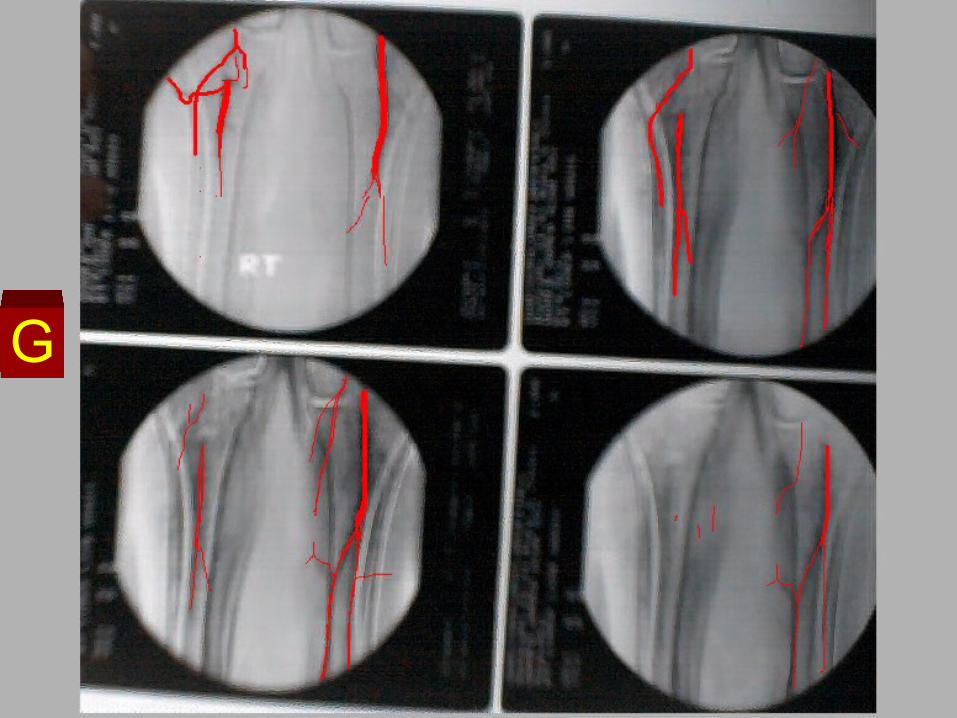
How to readHow to read
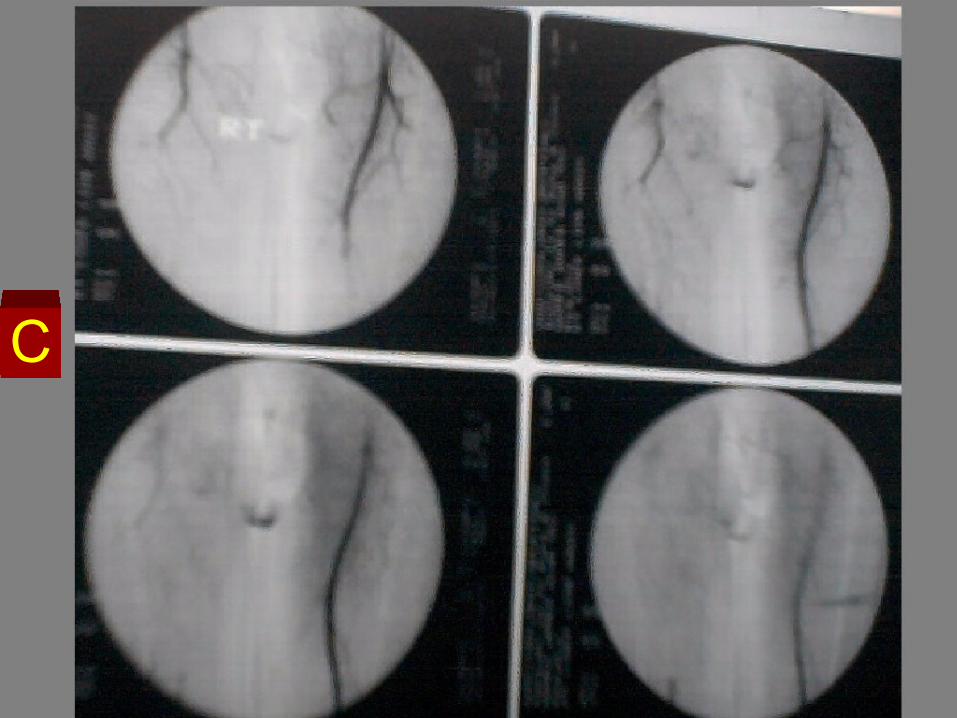
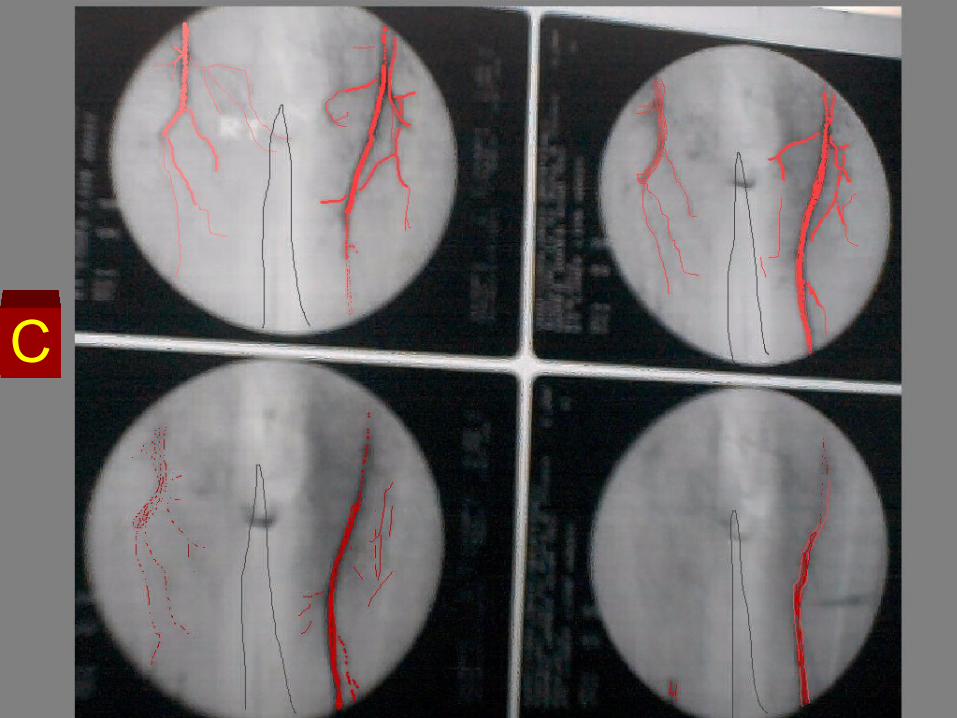
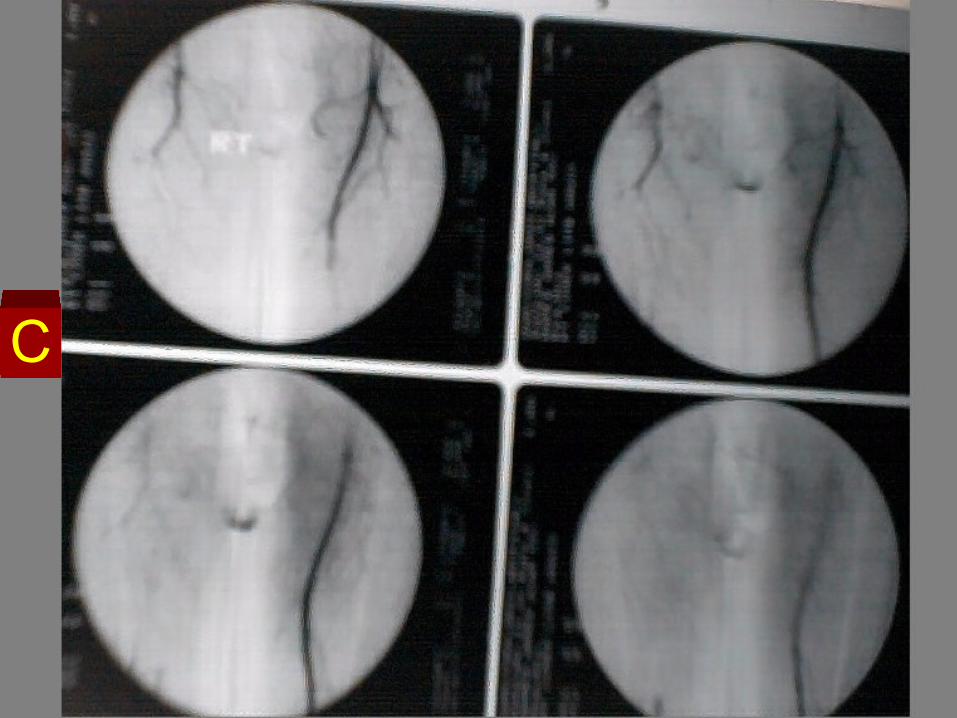
Bilateral lower limb Angiography
Right L.L Normal opacified Rt Common iliac artery, External
Iliac artery, and Common Femoral Artery. Total Occlusion of the Left SFA, at its origin from
the Lt CFA. The Rt Superficial Femoral Artery is seen refilled
through collaterals. Total occlusion of the Rt Popliteal artery. Distal refilling of the inferogenicular portion of Rt
Popliteal artery through collaterals. Opacified Rt Anterior and posterior tibial arteries
down to the Rt ankle joint.
Bilateral lower limb Angiography
Left L.L
Normal opacified Left Common Iliac artery, Left External Iliac, and Left Common Femoral Arteries, Left SFA, left Popliteal artery, and left leg arteries down to the left ankle joint
A

A
B
B
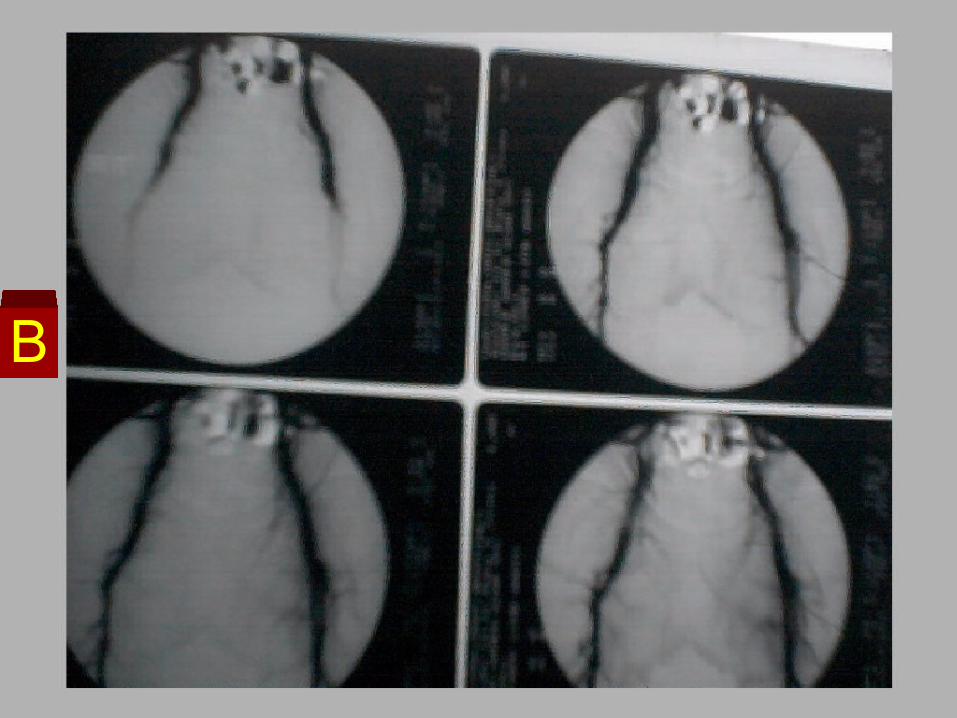
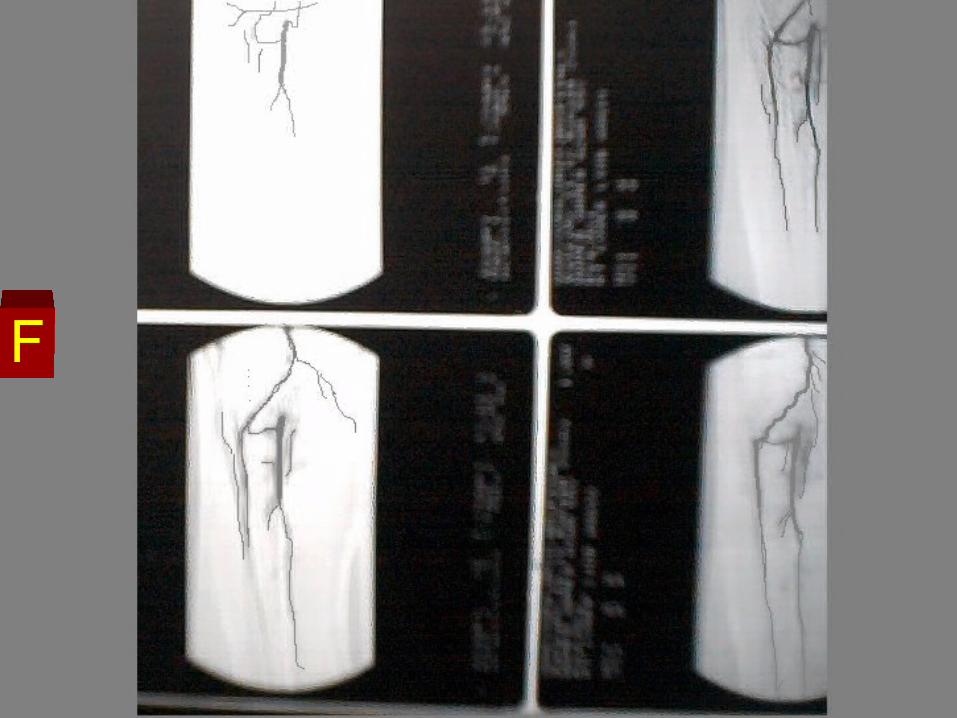
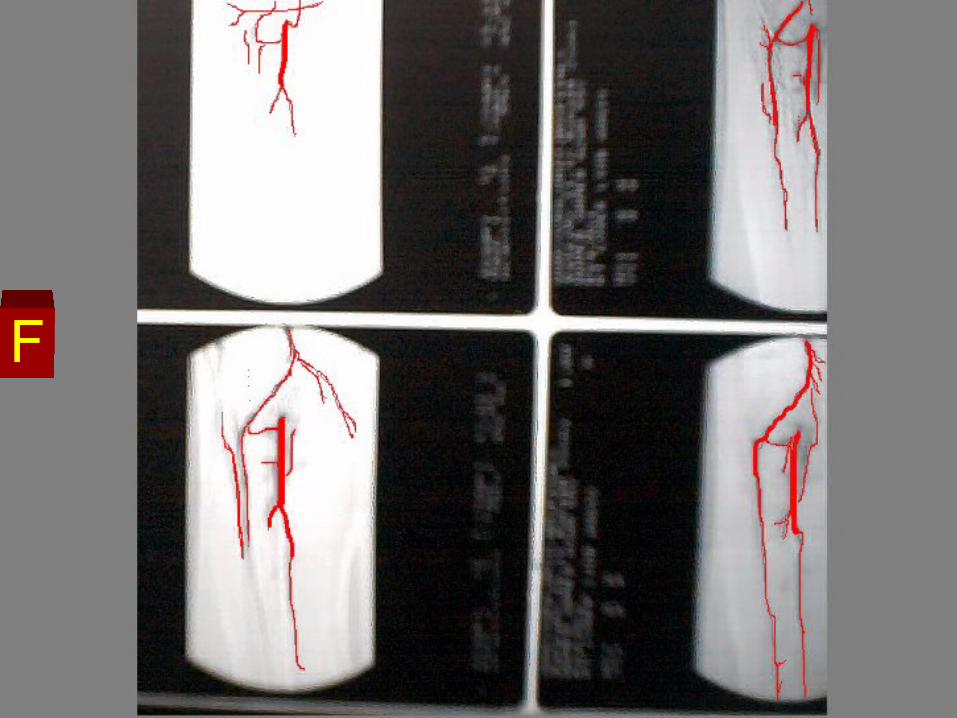
How to readHow to read
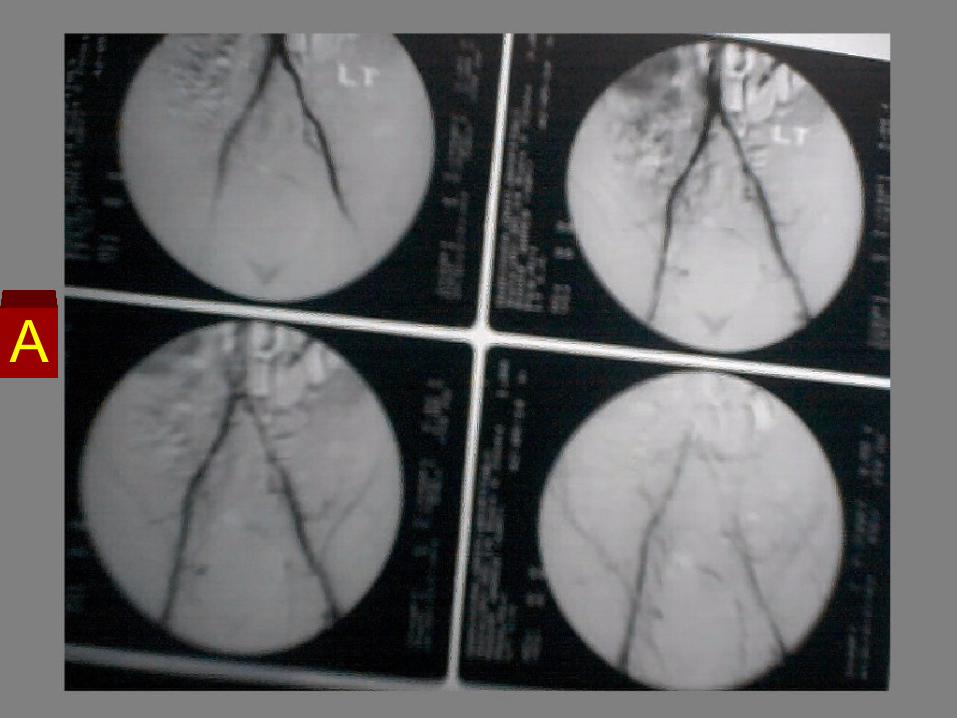
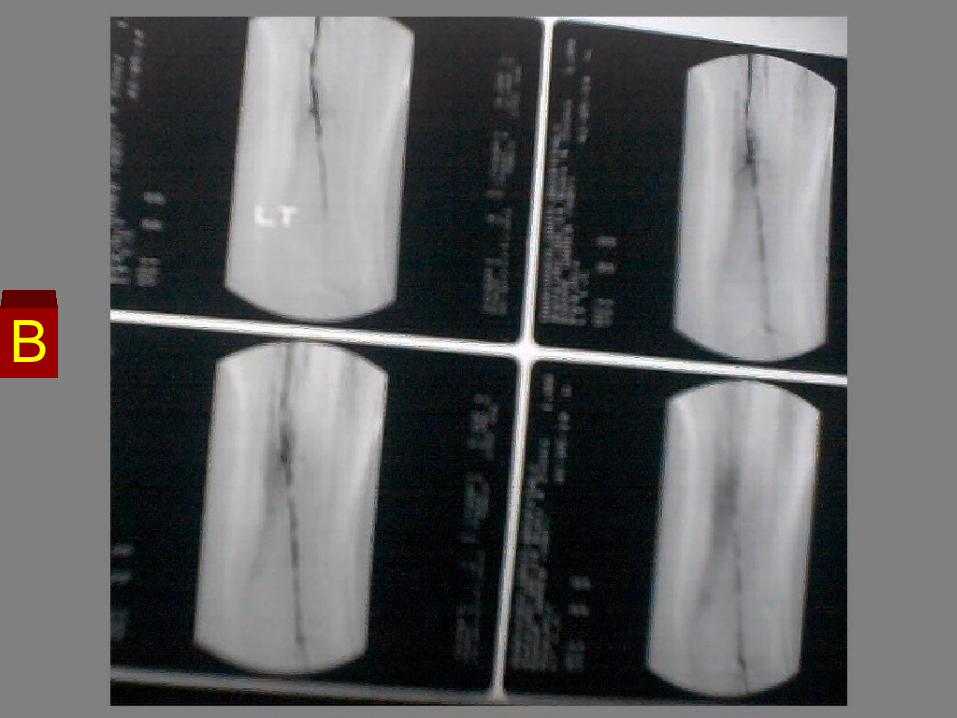
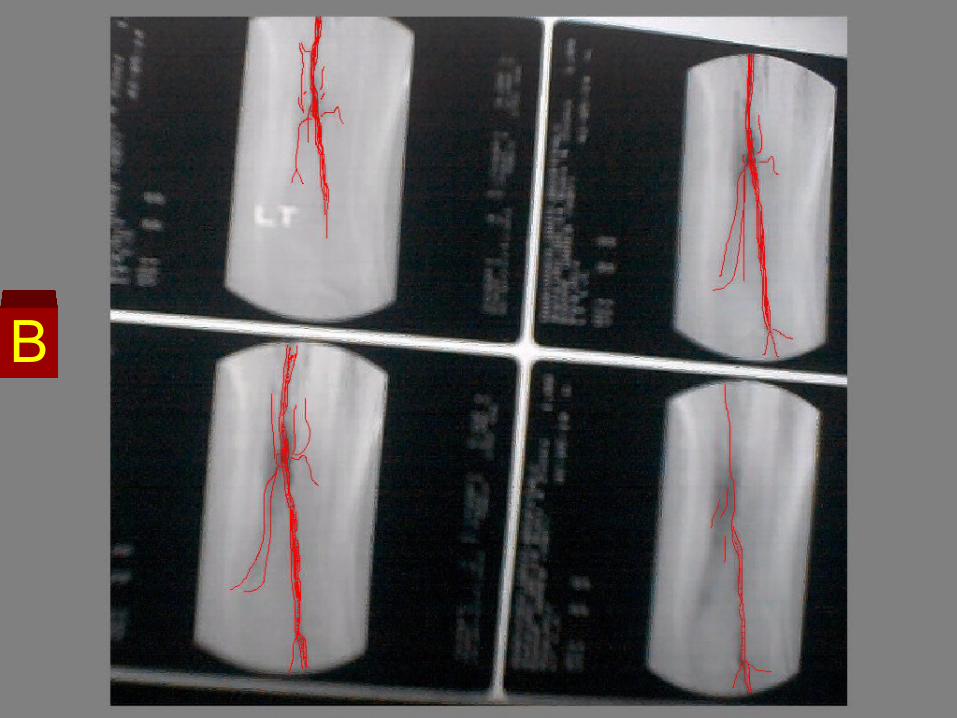
Digital Subtraction Imaging Angiography
Left L.L
Marked irregularity of the wall of the Left Common Iliac, Superficial Femoral, and Popliteal arteries.
With multiple short stenotic areas. Suggestive of marked atherosclerotic changes


How to readHow to read
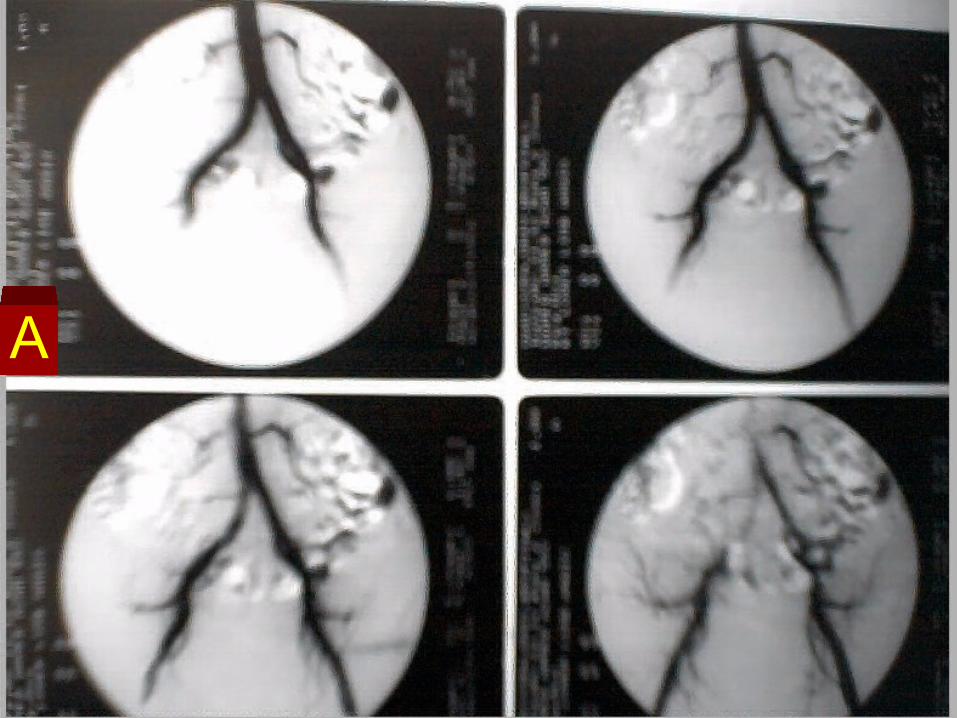
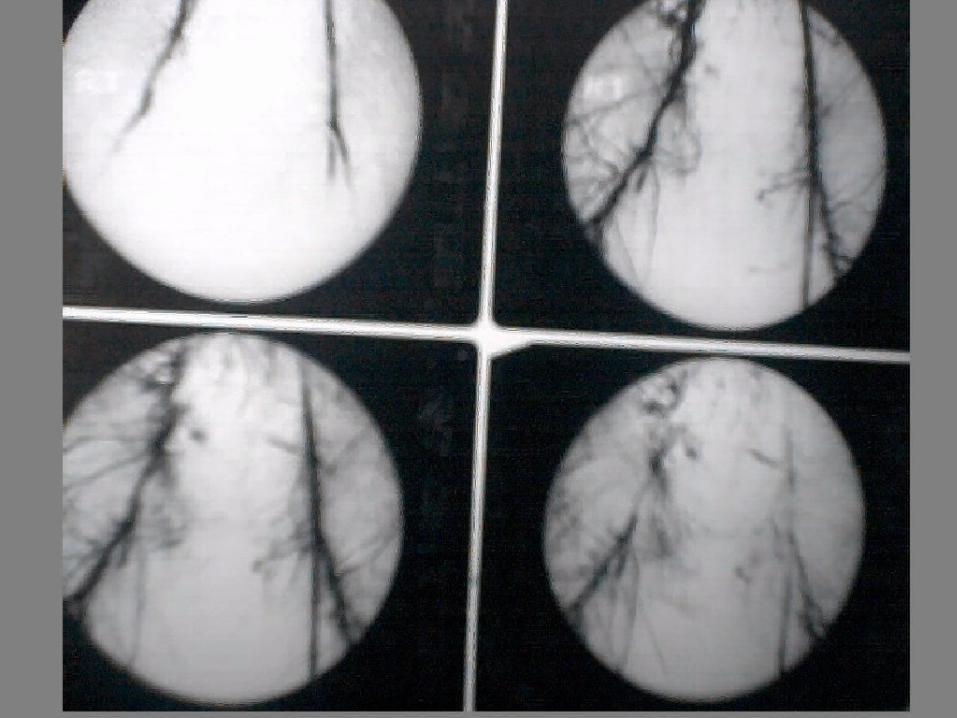
Bilateral lower limb Angiography
Atherosclerotic changes of the Left Common Femoral artery with multiple small marginal defects.
Total occlusion of the Rt Common Femoral Artery with multiple collaterals.
Distal refilling of the Rt superficial femoral and Rt Deep Femoral arteries.
How to readHow to read
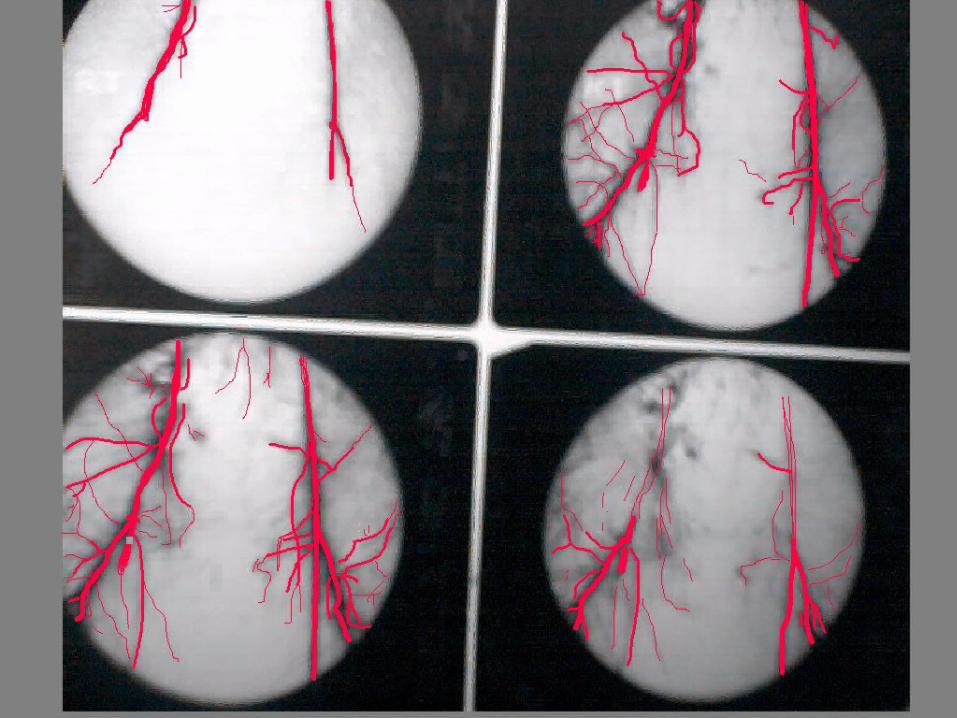
Bilateral lower limb Angiography
Normal course and caliber of the opacified Iliac Arteries.
Normal course of both Common Femoral arteries
and left SFA. Total occlusion of the Rt SFA, high up at its origin
With short markedly stenotic segment above the obstruction.
Etiology of Chronic ischemia. Clinical picture. 1- Pain 2- Color changes
3- Paraesthesia 4- Trophic changes
Investigations. Treatment. 1- Conservative treatment
2- Arterial reconstruction
A- Thromb-end arterectomy
B- Bypass Grafting
3- Balloon Angioplasty.
4- Catheter fibrinolysis
5- Sympathectomy
6- Amputation and rehabilitation
How to readHow to read
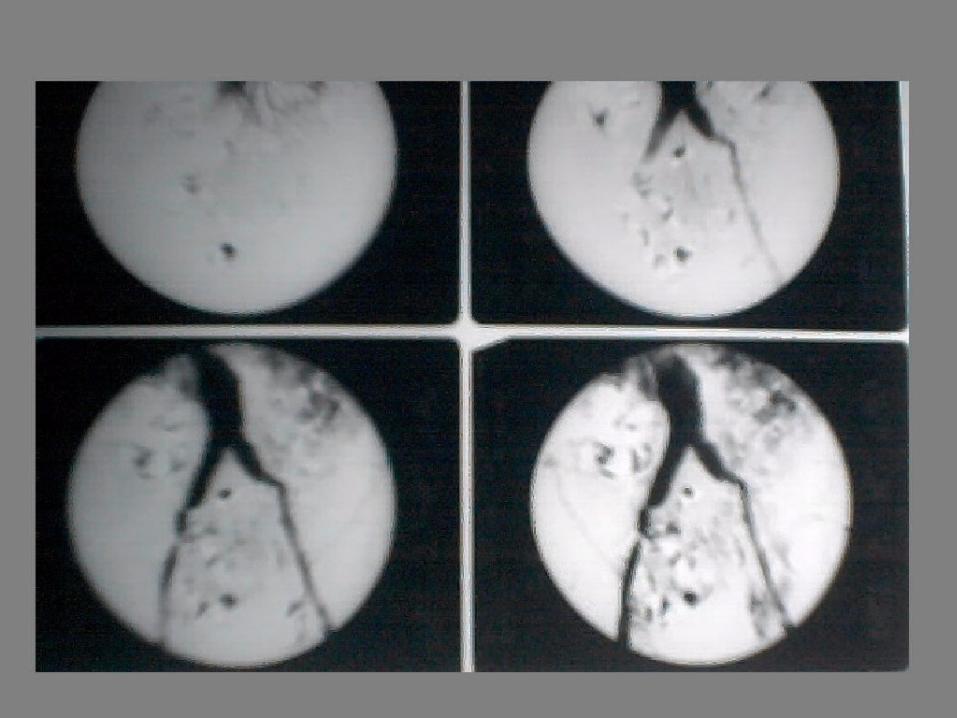
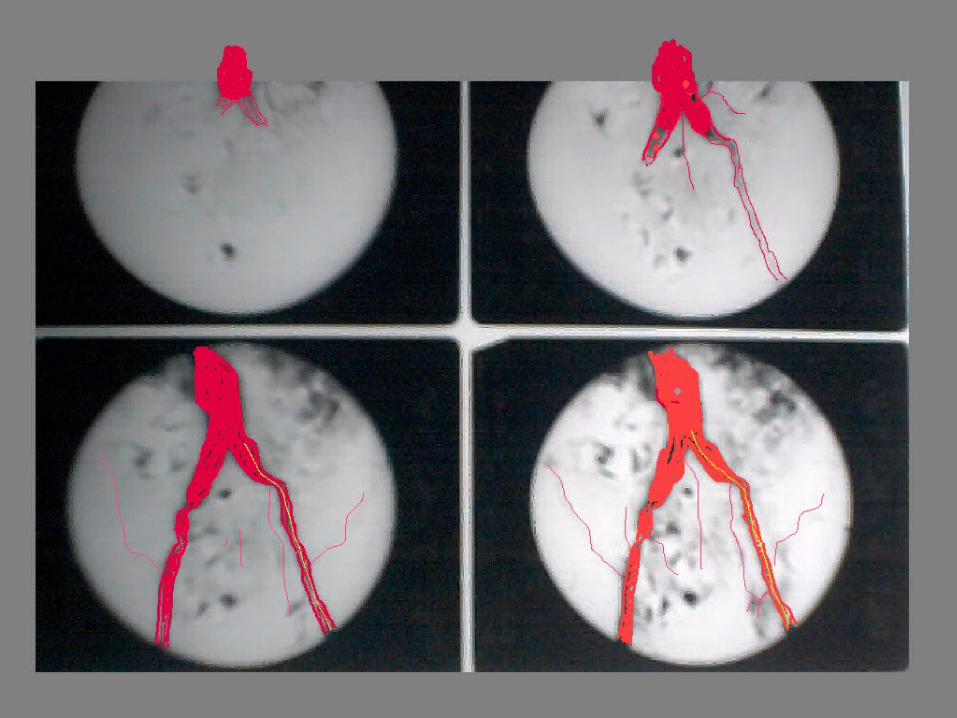
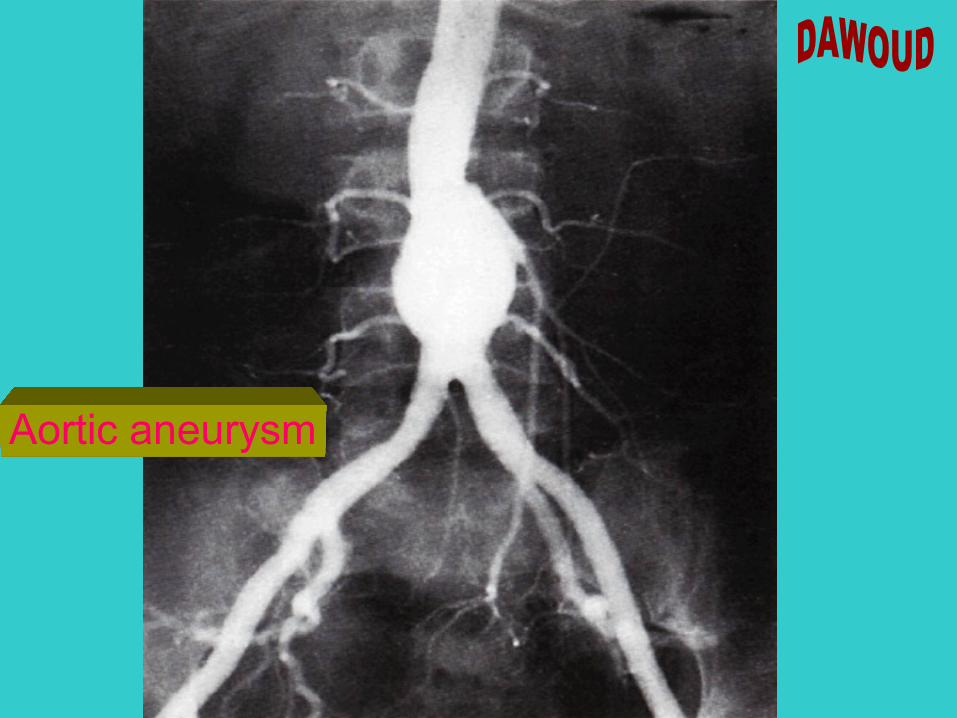
Flush Aortogram
Fusiform Aneurysm of the lower Abdominal Aorta and the Iliac Arteries.
Atherosclerotic changes of the Left Common Iliac Artery with multiple marginal defects ( Atheromas).
Short stenotic segment at the junction of Rt Common and External Iliac arteries
Non opacified Internal Iliac Arteries on both sides

Aortic aneurysm
Aortic aneurysm
How to readHow to read
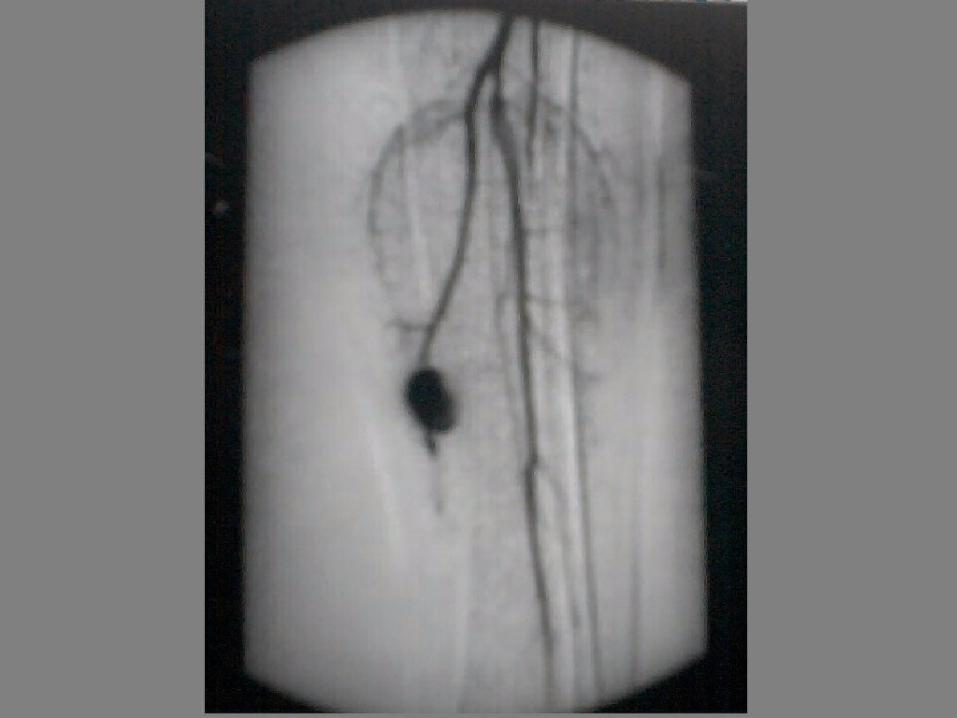
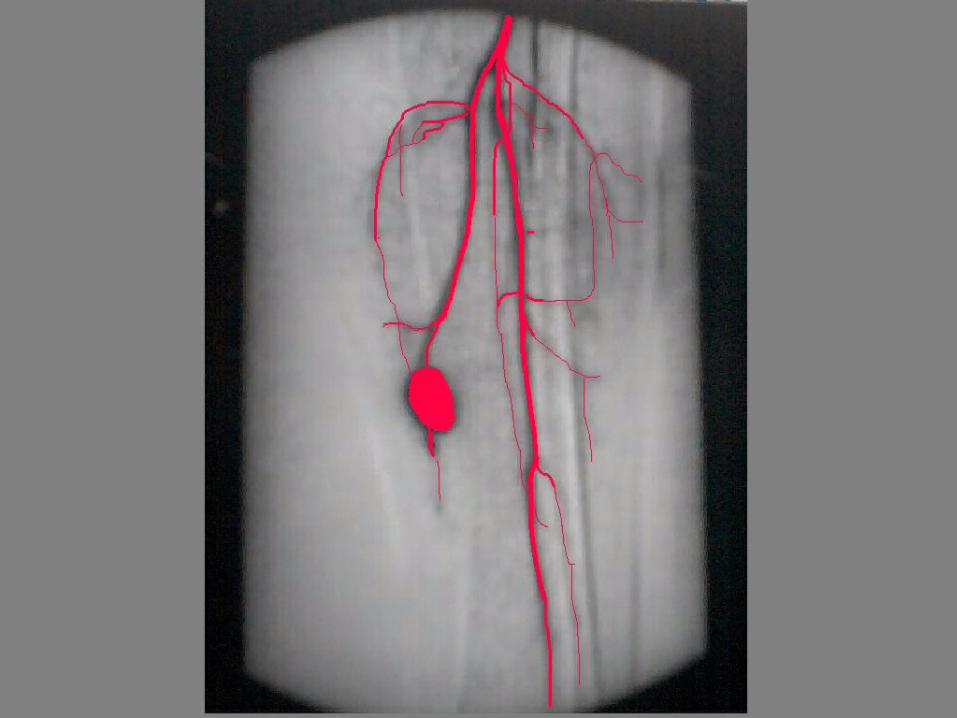
Popliteal and leg Angiography
A small pseudoaneurysm is seen related to the upper part of the left anterior tibial artery.
Likely post-traumatic
Etiology Congenial Traumatic Pathological
Pathology Types ( Fusiform - Saccular - Dissecting)
Sequelae ( Cure - Rupture - Suppuration)
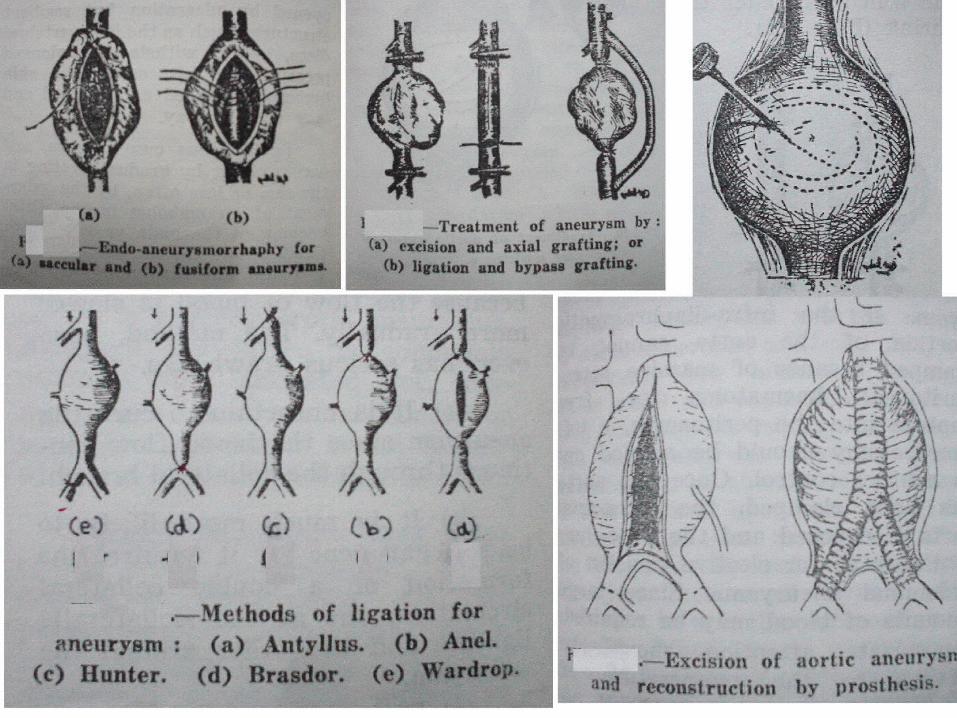
Clinical picture Treatment 1- Endo-aneurysmorrhaphy
2- Arterial reconstruction
3- Excision and ligation
4- Simple ligation
5- Introduction of foreign material

Superior Vena Cava Obstruction





























