Embed Size (px)
Citation preview
20 Pulmonary Disease with Eosinophilia
CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
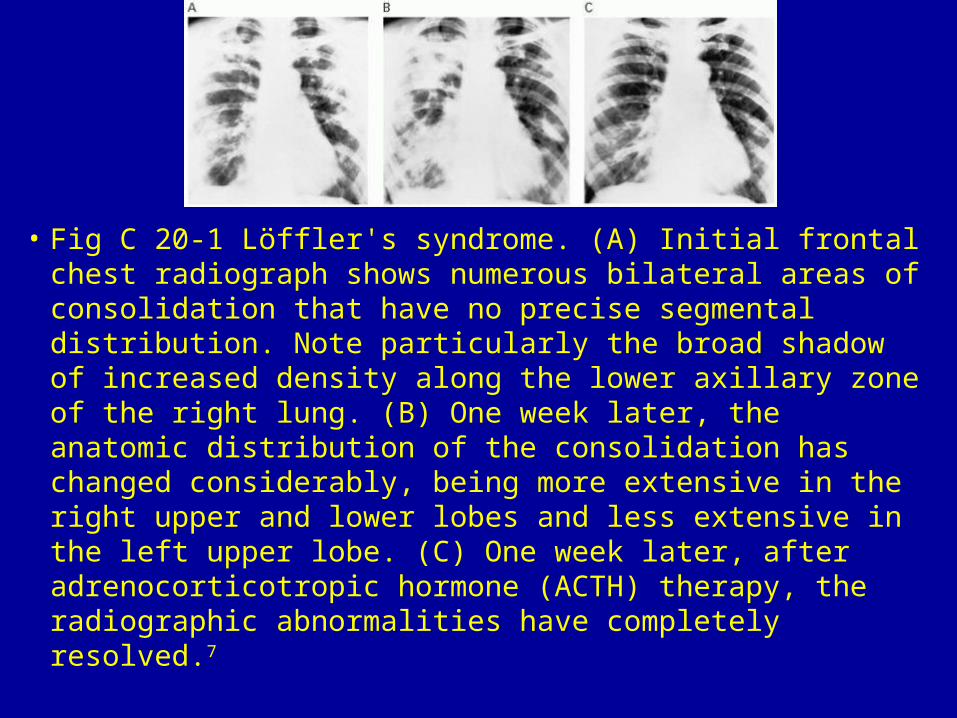
• Fig C 20-1 Löffler's syndrome. (A) Initial frontal chest radiograph shows numerous bilateral areas of consolidation that have no precise segmental distribution. Note particularly the broad shadow of increased density along the lower axillary zone of the right lung. (B) One week later, the anatomic distribution of the consolidation has changed considerably, being more extensive in the right upper and lower lobes and less extensive in the left upper lobe. (C) One week later, after adrenocorticotropic hormone (ACTH) therapy, the radiographic abnormalities have completely resolved.7
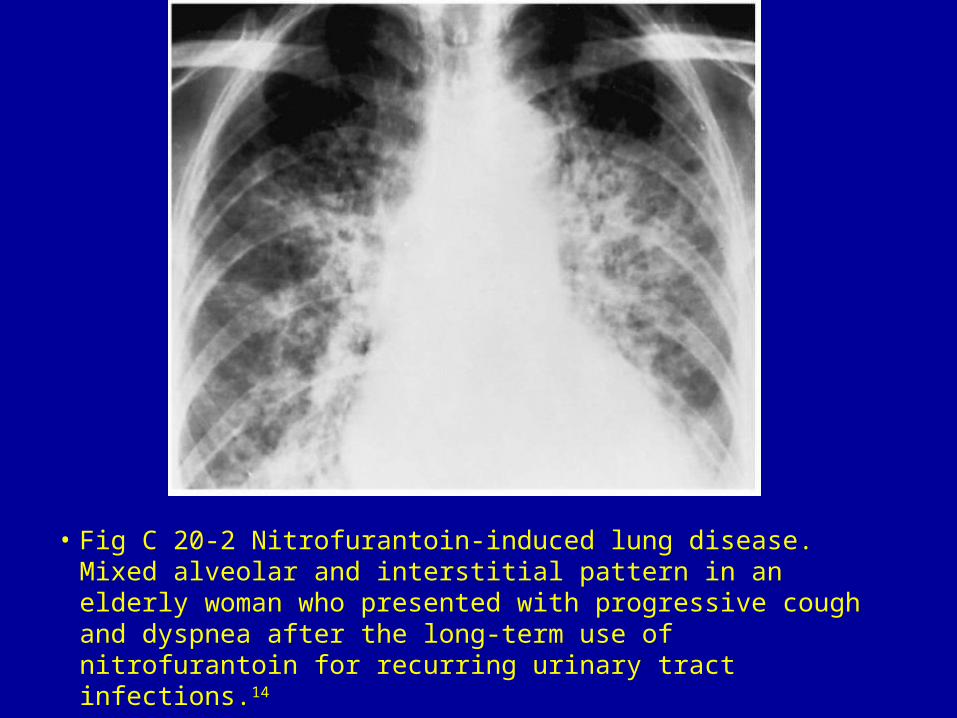
• Fig C 20-2 Nitrofurantoin-induced lung disease. Mixed alveolar and interstitial pattern in an elderly woman who presented with progressive cough and dyspnea after the long-term use of nitrofurantoin for recurring urinary tract infections.14
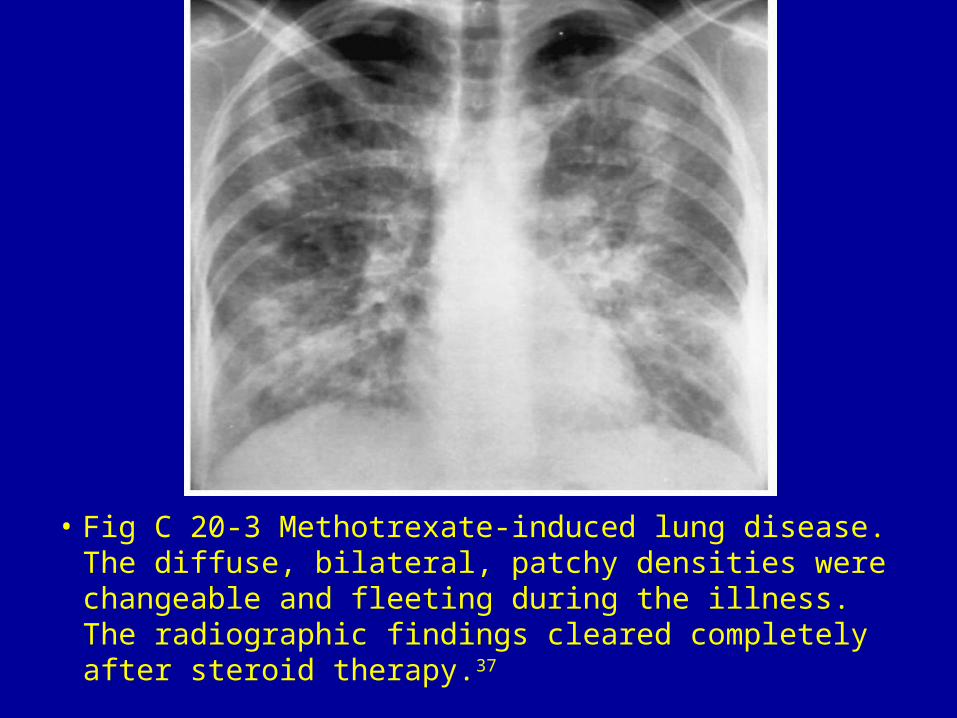
• Fig C 20-3 Methotrexate-induced lung disease. The diffuse, bilateral, patchy densities were changeable and fleeting during the illness. The radiographic findings cleared completely after steroid therapy.37
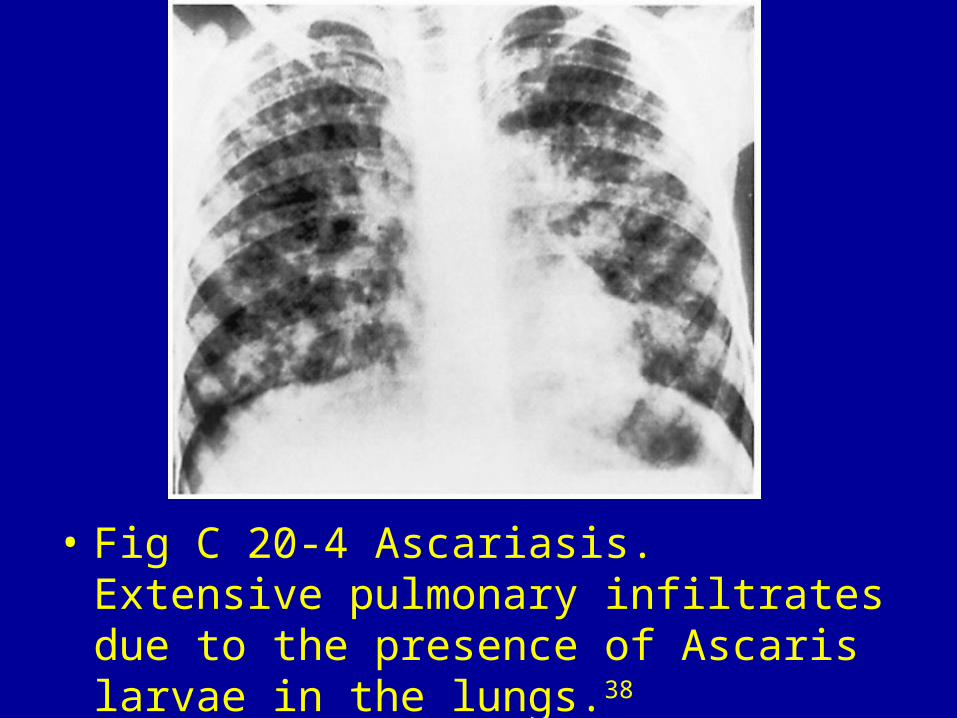
• Fig C 20-4 Ascariasis. Extensive pulmonary infiltrates due to the presence of Ascaris larvae in the lungs.38
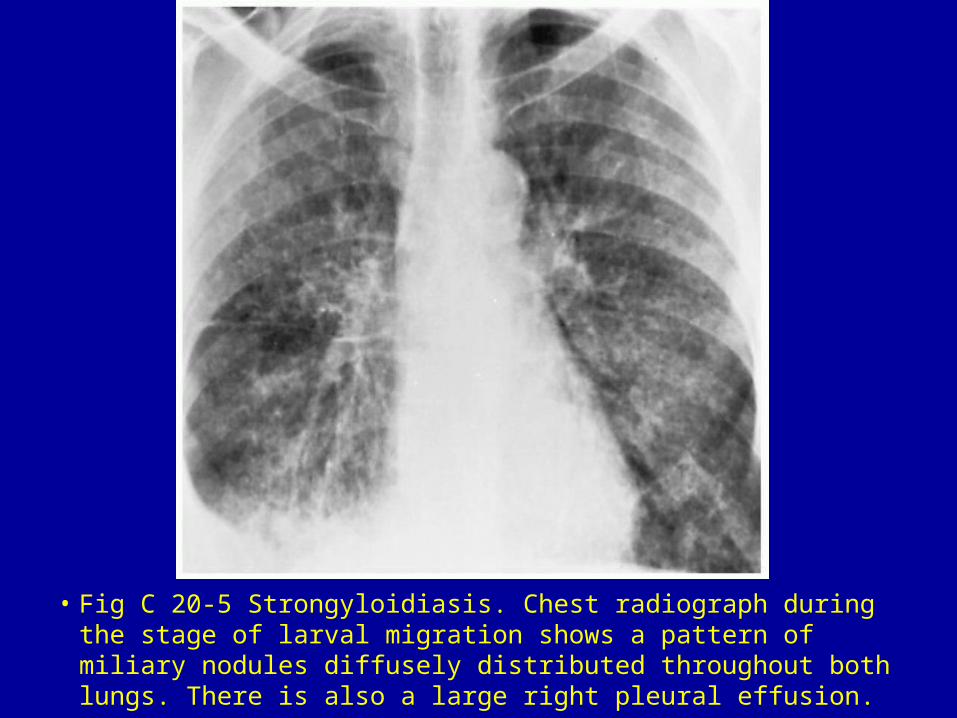
• Fig C 20-5 Strongyloidiasis. Chest radiograph during the stage of larval migration shows a pattern of miliary nodules diffusely distributed throughout both lungs. There is also a large right pleural effusion.
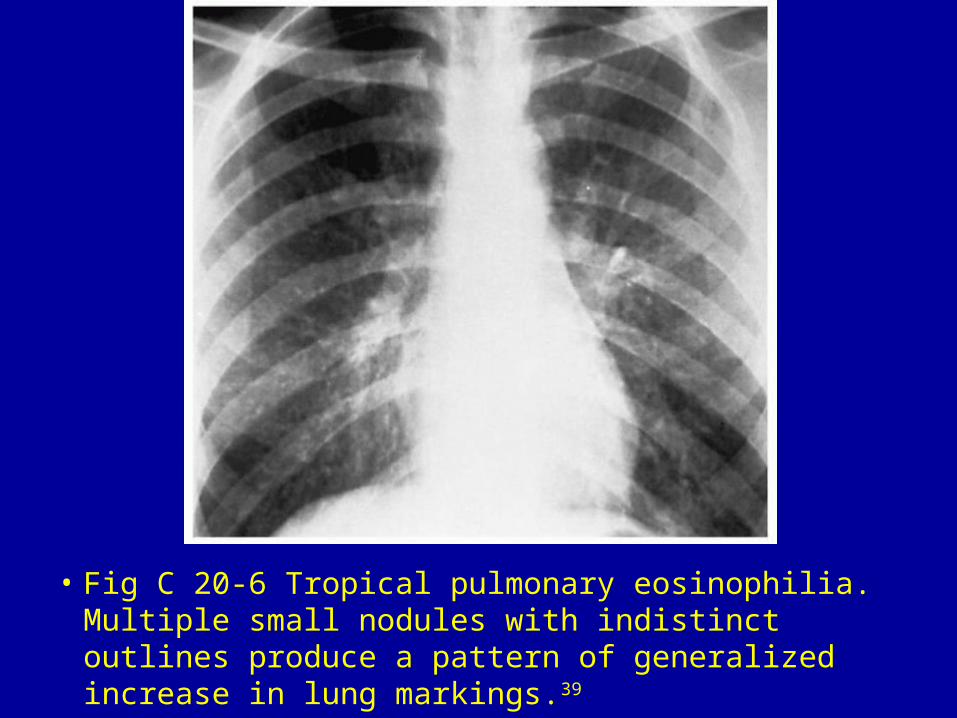
• Fig C 20-6 Tropical pulmonary eosinophilia. Multiple small nodules with indistinct outlines produce a pattern of generalized increase in lung markings.39
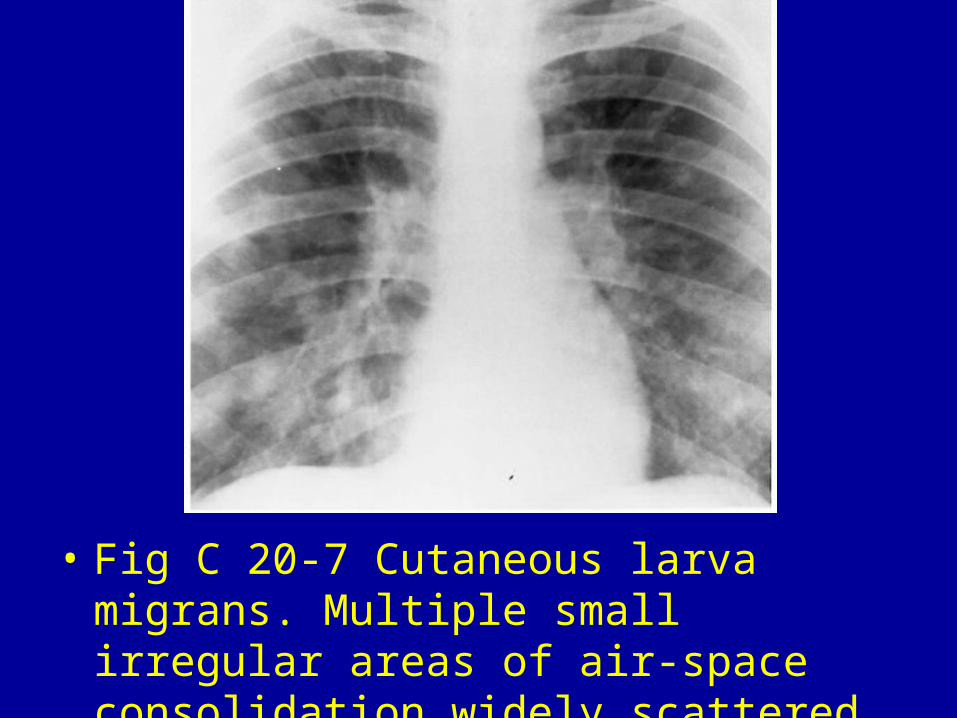
• Fig C 20-7 Cutaneous larva migrans. Multiple small irregular areas of air-space consolidation widely scattered throughout both lungs.40

• Fig C 20-8 Dirofilariasis. Well-circumscribed solitary pulmonary nodule (arrow) that is indistinguishable from a malignant coin lesion.
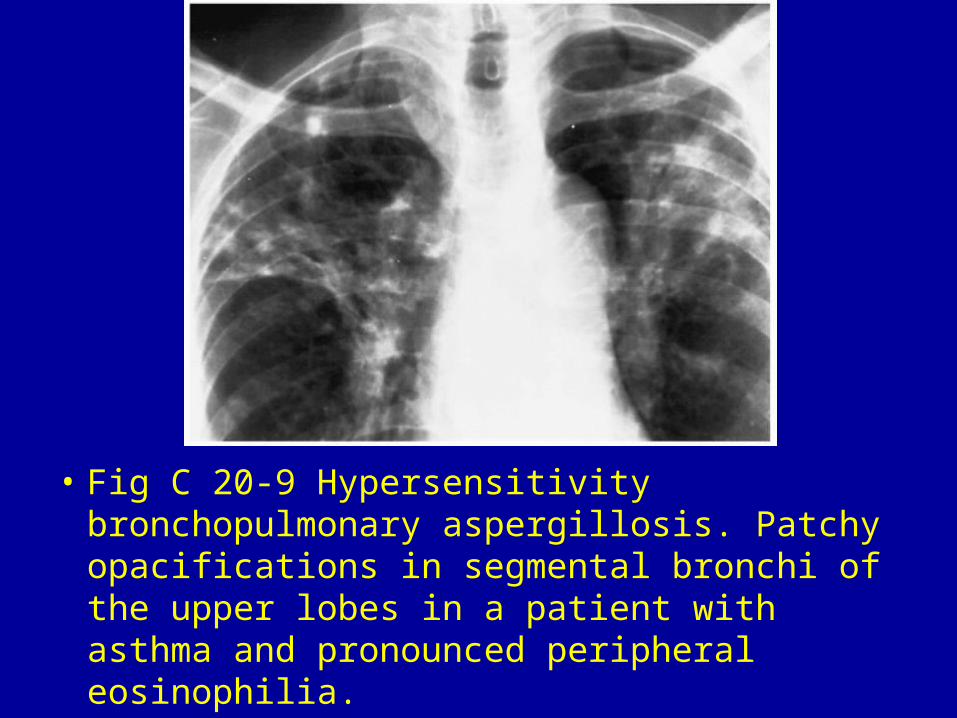
• Fig C 20-9 Hypersensitivity bronchopulmonary aspergillosis. Patchy opacifications in segmental bronchi of the upper lobes in a patient with asthma and pronounced peripheral eosinophilia.
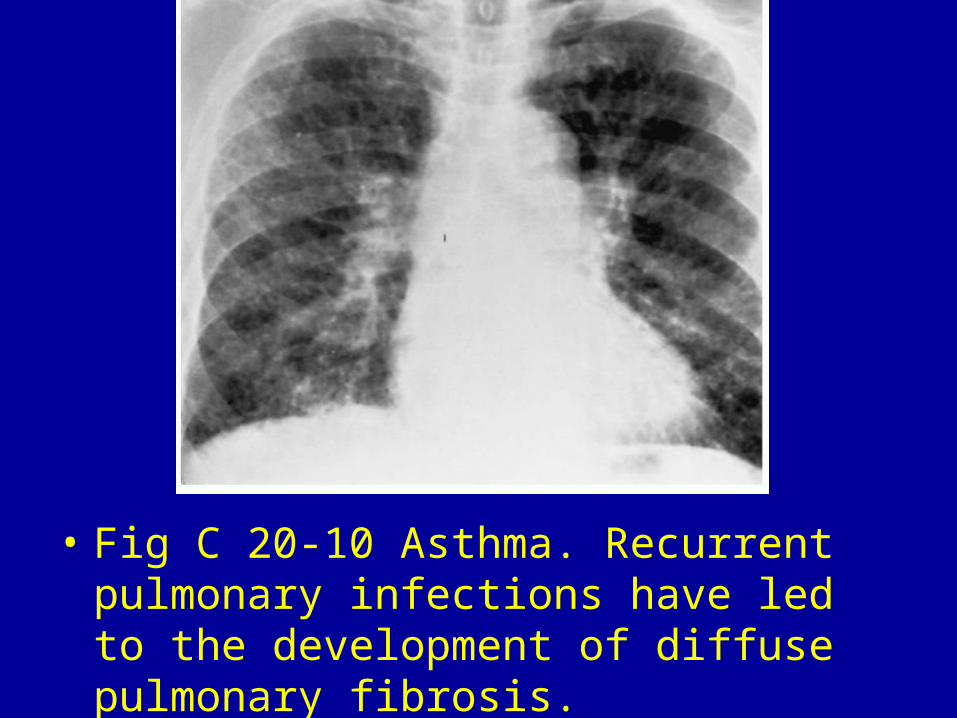
• Fig C 20-10 Asthma. Recurrent pulmonary infections have led to the development of diffuse pulmonary fibrosis.
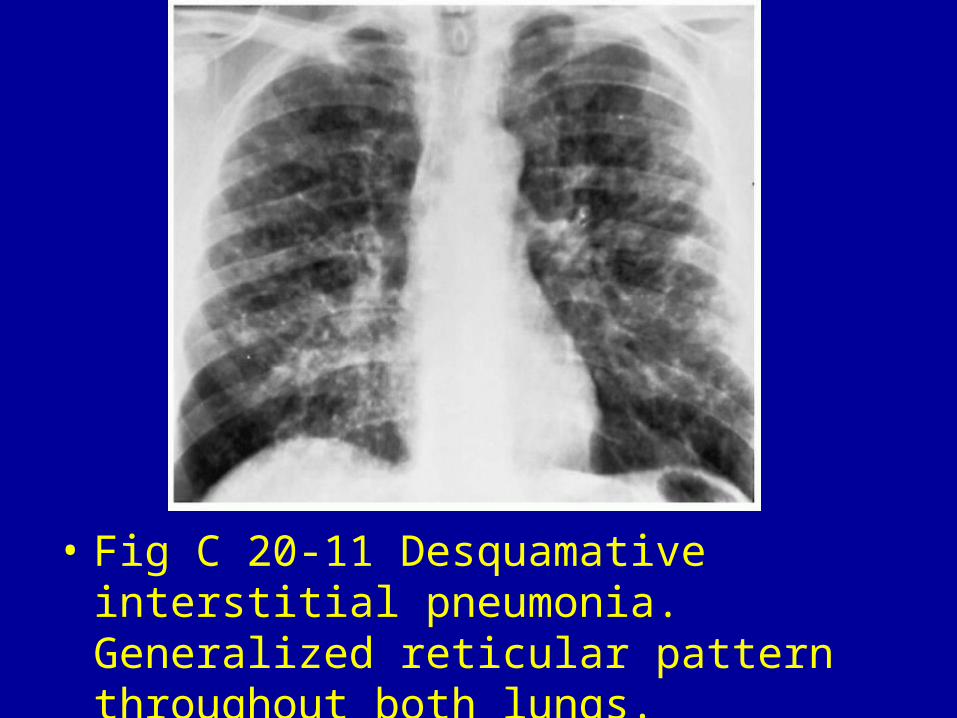
• Fig C 20-11 Desquamative interstitial pneumonia. Generalized reticular pattern throughout both lungs.
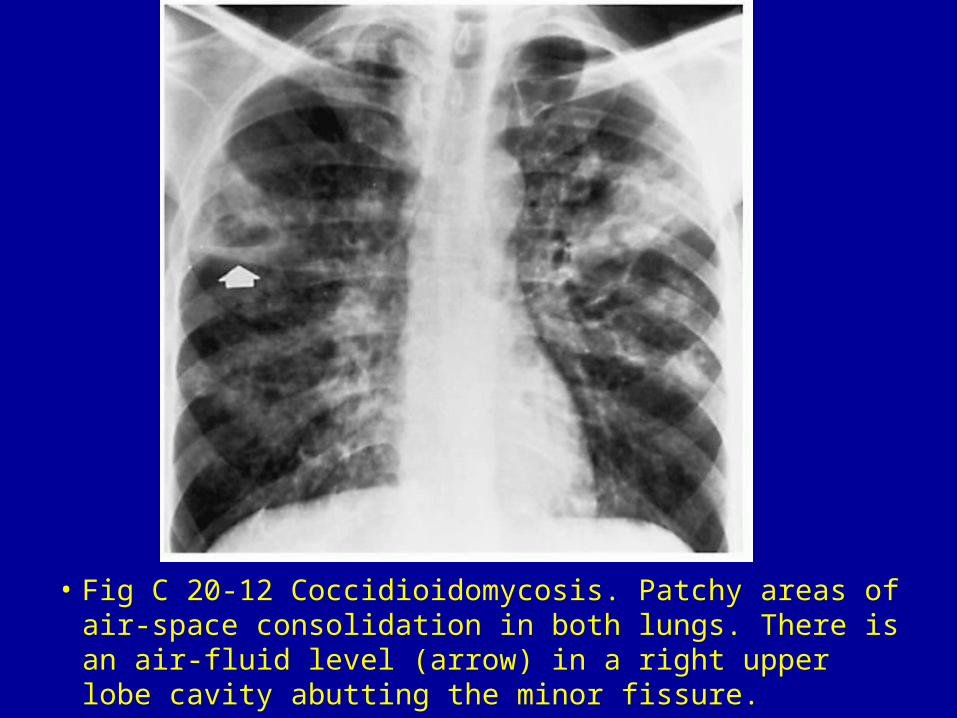
• Fig C 20-12 Coccidioidomycosis. Patchy areas of air-space consolidation in both lungs. There is an air-fluid level (arrow) in a right upper lobe cavity abutting the minor fissure.






























