Embed Size (px)
Citation preview
Breast Surgery Christiane Riedinger, September 2014
Resources: Path notes, Surgical Talk, Lecture Notes in Clin Surgery

TOC● Clinical Assessment● Pathology● Management
Clinical Assessment

History● Symptoms of breast disease
○ Pain■ Cyclical? => Bilat. can depend on diet (caffeine)
Drug Mx: change contraceptive method, danazol, tamoxifen, LHRH analogues
■ Non-cyclical? => Abscess, CA, Tietze’s syndrome*, Herpes Zoster and other chest wall lesions.
○ Discharge■ Clear Intraductal papilloma (benign)■ Milky Galactorrhoea■ Purulent Abscess■ Multi-coloured Duct ectasia (inflammatory)■ Blood Intraductal papilloma, CA, Paget’s
○ Lump
Breast Tumours: How to describe a lump
● she cuts the fish 3x + PER
○ site, size, surface○ colour, contour, consistency, compressability/fluctuancy○ tenderness, temperature, transillumination○ fluid-filled, fixed (tethering vs. fixation, depth), fields (lymphatic drainage)○ pulsatile (e.g. aneurysm)○ expansile○ reducible/relation to skin, muscle, other structures (hernia/breast lesion)
● Difference between tethering (lesion near fibrous septum or ligaments of Astley Cooper, evident upon elevation of the arms or tension of pec major - dimpling) and fixation (tumour attached to muscle and skin? implies more advanced disease)
● ??????

Breast Examination (1) ● Ask about pain● Be ruthless but polite in terms of exposure for inspection
● General observation○ General appearance - cachexia, pallor, SOB○ Signs of previous surgery - wide local excision, mastectomy, reconstruction○ Signs of infection○ Nipples
■ Discharge, e.g. lactation, blood (duct ectasia, intraductal papilloma)■ Rash (e.g. in Paget’s, DCIS underlying nipple, peau d’orange)■ Inversion/retraction of nipples■ Accessory nipples (usually below breast), accessory breast tissue (usually in axilla)
○ Supraclavicular area and axilla - swollen, nodes, veins, muscle wasting
● Continue with patient sitting at 45*
● Inspect breasts ○ Ask if pain when moving arms○ Watch breasts as arms behind head – T4 skin, Astley Cooper* => Tethering?
arms behind back – T4 chest wall pec. major => Fixation?○ = check for invading masses of stage T4○ Ask about discharge and ask patient to demonstrate it

Breast Examination (2)● Continue with patient lying flat with hands behind the head● Cover patient and expose body parts needed
● Check inframammary fold with back of hand○ Say: “I am now examining under the breast”○ Most common finding: intertrigo – chronic thrush under breast
● Palpate 5 areas of the breast and axilla and nodes○ Upper outer quadrant + axilla (most common site of lesions)
Hold pt’s R arm with your R arm then palpate axilla with the other hand. Ask patient to lift arm up, place hand in axilla, lift arm down to rest on yours, then roll fingers down axilla 4 times. Examine the left axilla with the left hand and vice versa. If you feel a lump, feel if it is fixed or not.
○ Upper inner quadrant○ Lower inner quadrant○ Lower outer quadrant○ Areolar complex○ Palpate normal breast first
■ During palpation don’t lift up hand■ Move all around breast
○ Lymph nodes: Axillary (already done), infraclavicular, supraclavicular, neck
● Cover patient

Breast Examination (3)
● PRESENTATION ○ To complete my examination, I’d like to
■ Send off potential discharge for cytology■ Palpate the liver and ausculate the chest for suspected mestastases■ Perform a triple assessment
■ Clinical Hx and Ex => done■ Radiological Mammography and US +/- MRI■ Pathological Fine needle aspiration => cytology and core biopsy■ MRI if younger patient or discrepancy between clinical assessment and
mammography or when planning breast conserving surgery
○ This lady has a non-tender/tender Xcm lump in the X quadrant of the X breast. It has a XX surface and a XX edge, is mobile/immobile and not/attached to XX. There are XXX palpable in the axilla, continue description as above. There are XXX nodes palpable in the supraclavicular fossa / other sites. My differential diagnosis is XXXX based on the age of the patient, the most likely diagnosis is XXXX.

Breast Examination (4) ● Note main DD has 4 choices (Mannequin does not have inflammatory lesion and 2 lumps to palpate, the benign diagnosis depends on age of
patient)○ Fibrocystic lesion
■ Women >30-40■ Changes with cycle
○ Benign neoplasm, e.g. fibroadenoma■ Women <30-40■ Changes with cycle
○ Malignant lesion: Peau d’orange, nipple retraction, tethering, fixation, change in breast size, ulceration, Paget’s■ Painless lump■ More likely in upper outer quadrant?
○ Inflammatory lesion■ Usually painful
● DD of breast discharge○ Ask if spontaneous or on squeezing○ Orange watery fluid from single duct Intraductal papilloma○ Bright red blood from single duct Papilloma or malignancy○ White or green discharge from multiple ducts Benign○ Bilateral milky discharge Galactorrhoea
● Note on axillary nodes○ 25% of palpable node will not contain metastases○ 25% of nodes containing metastases are not palpable

Aids to DD● Have 4 main options for lump (note for exam: mannequin does not have
inflammatory option, has 1 palpable benign or malignant lump. Need to distinguish 2 benign conditions by age of the patient)○ Benign fibroCYSTIC lesion in older women, terminal ducts undergo
apoptosis and terminal lobuloaveolar unit produces fluid => cyst■ Change with cycle■ Most likely if >>30y and up to menopause
○ Benign FIBROADENOMA = STROMA, “breast mice”■ Change with cycle■ Most likely if <~30y!!! Young!!!
○ MALIGNANT tumour■ Painless lump
○ INFLAMMATORY lesion■ PAINFUL, potential purulent discharge

Pathology

Breast Tumours: Risk factors
● Age
● Gender - only 15% of breast CA patients have other risk factors
● Inherited trait
● Oe exposure: early menarche, late menopause, no children, children at age of >35y
● OCP (risk returns back to normal)
● HRT (beyond the age of 55), risk returns to normal 5y post stopping, combined Oe/P HRT is worse than Oe only
● Previous benign breast disease: atypical epithelial hyperplasia (fibrocystic lesion)
● Obesity, alcohol intake, NOT smoking!?! (Acc. to surgical talk)
● Radiation exposure, esp. post lymphoma (mantle radiotherapy)

Breast Tumours: Overview
● While listing the different pathological types of tumours, think of the
different tissues it can originate from
○ Types of breast tissue epithelium (duct vs. lobule)
○ Fibroblasts (stroma)
○ Types of skin epithelium (keratinocytes vs. glands etc..)

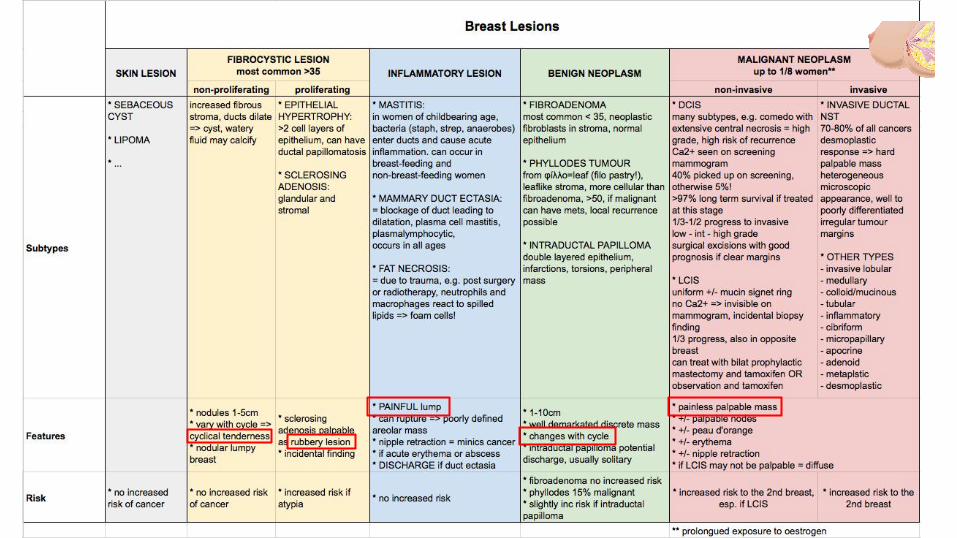
Benign Breast Tumours/Lesions● General: Lipoma, sebaceous cyst, hamartoma, sarcoma (rare), 2* mets● Fibrocystic >>35, perimenopausal, remodelling of breast tissue causing fluid entrapment
○ Non-proliferating cystic changes => cyclical, ASPIRATION AND CYTOLOGY○ Proliferating:
■ Epithelial hypertrophy■ Sclerosing adenosis =>
● Inflammatory○ Mastitis (lactating) => ABX, ABSCESS ASPIRATION AND IV ABX, BREASTFEEDING
CONTINUATION○ Non-lactating: piercings => periductal mastitis, fungal in immunosuppressed,
granulomatous in sarcoidosis or TB, infective in T2DM, RA => TREAT UNDERLYING CAUSE AND CAUSATIVE AGENT
● Benign○ Fibroadenoma <<35 (Breast mice) => EXCISION OR NO Rx○ Phylloides: WLE OR MASTECOMY AS 15% MALIGNANT○ Intraductal papilloma => EXCISION OR NO Rx

Malignant Breast Tumours● DCIS● DCIS near nipple = Paget’s disease● DCIS subtype: comedone● LCIS● Invasive ductal NST● Invasive ductal
○ Lobular○ Medullary○ Colloid/Mucinous○ Tubular○ Inflammatory○ Cibriform○ Micropapillary○ Apocrine○ Adenoid○ Metaplastic
● Invasive LCIS

Breast Tumours: Organisation by site● 50% upper outer
quadrant● 20% central● 4% bilateral 1* or >1 1*
lobular carcinoma
invasive ductal carcinomamucinous carcinomamedullary carcinomaintraductal papillomaPaget’s,
DCIS
lipomasebaceouscyst
stroma:fibrocysticfibroadenomaphylloides

Breast Tumours: Genetic Changes
A HER2 -ve slow growing, responds to tamoxifen but not well to chemo
OeR +ve = luminal B HER2 +ve double +ve, worse, often node involvement
basal-like HER2 -ve, triple -ve, highly aggressive, medullary, BRCA1/2 involved
OeR -ve PR -ve HER2+ve HER2 +ve highly proliferative
● 10% genetic predisposition of which 30% BRCA1/2● RECEPTORS
○ 30% HER2 upregulated (human epidermal GF = Y kinase) => worse prognosis○ Oe R present/absent => if present better prognosis
● PROTEINS○ Ras/Myc upregulated○ pRb/p53 downregulated
● Classification according to receptor involvement:

Management
Screening of Breast Cancer● 47-73 (after 70 voluntary)● Every 3y● 2 view mammogram looking for calcification● Procedure
○ +ve (abnormal) => core biopsy■ B1: Normal => return to screening (if biopsy from wrong area
rebiopsy)■ B2: Benign => reassure, return to screening■ B3: Uncertain malignant potential => excision■ B4: Suspicion of malignancy => rebiopsy or excision■ B5: Malignant => surgical excision (WLE or mastectomy)
● B5a - DCIS● B5b - invasive
○ -ve (normal) => return to screening programme
Ix of Breast Disease● Referral from GP or screening of suspicious lumps or mamogram findings:
● Triple assessment (diagnostic tests)○ Clinical Hx and Ex○ Radiological Mammography and US (useful for Ix of lesions already diagnosed,
not useful for ab initio identification, also US axilla)○ Pathological Fine-needle aspiration FNA cytology and core biopsy
■ FNA: cystic lesion disappears on aspiration => diagnosis■ Core biopsy only performed if suspicion of cancer after FNA
○ MRI if younger patient (high tissue density on mammobraphy) or discrepancy between clinical assessment and mammography or when planning breast conserving surgery
● Other Ix: ○ FBC (potential marrow involvement), LFTs, U&E/CA, CXR, Isotope bone scan,
liver US.
Ix of Breast Disease: Mammography● Views
○ Mediolateral-oblique view MLO○ Craniocaudal view CC○ Lateromedial/mediolateral view?
● Result suspicious of cancer○ White asymmetrical spiculated lesion containing microcalcification○ DCIS: cluster of microcalcification
● Efficiency○ Misses 7% of palpable cancers and 20% in pre-menopausal women○ Lobular carcinoma not well detected
● ADD
Ix of Breast Disease: Staging ● Staging informs on state of progression and guides treatment● Assessment for staging
○ Lymph node biopsy○ CT for metastases○ Bone scan for metastases○ CXR for metastases○ Liver US for metastases○ Blood tests as before: FBC, LFTs, serum calcium, U&E
● TNM○ Tx 1* cannot be assessed○ T0 No evidence of 1*○ Tis In situ○ T1 <2cm○ T2 2-5cm○ T3 >5cm○ T4 Chest wall or skin involvement
● Nx Lymph nodes cannot be assessede.g. if removed
● N0 no involvement● N1 Movable axillary● N2 Fixed axillary● N3 Ipsilateral thoracic nodes● Mx Cannot be assessed● M0 No distant mets● M1 Distant mets
Why Stage and Grade
● Grade = biology/histology differentiation
● Stage = anatomy infiltration
● Prognosis guided by
○ grade (incl. node biopsies)
○ stage
i

Treatment Overview● Management by MDT: surgeon, oncologist, nurse, radiologist, histopathologist, cytologist,
coordinator, +/- plastic surgery, genetics, palliative careBreast care nurse from 1st visit for SUPPORT AND EDUCATION
● Medical○ Tyrosine kinase inhibitors: HER2 antagonists Herceptin○ Endocrine treatment: Oe antagonist Tamoxifen pre-menopausal, Arimidex post
● Surgical○ Excision of the tumour○ Surgery to axilla○ +/- Breast reconstruction
● Radiological ● +/- Adjuvant therapy: hormonal, biological or chemotherapy, neo-adjuvant means prior to
surgery● Know local policies and national guidelines● Consider social circumstances of patient● Breast care nurse from 1st visit for SUPPORT AND EDUCATION

Surgical Treatment of the 1* Tumour● <4cm
○ Breast-conserving surgery: WLE wide local excision and radiotherapy○ OR mastectomy○ Depends on patient choice, 75% chose WLE
● For impalpable tumours○ Stereotactic localisation under mammographic control○ Needle is placed in place of microcalcification ○ Area surrounding the needle is excised○ Excised area X-rayed to confirm it contains the calcifications
● If margins of local excision not clear, re-excision is required● Treatment of axilla is not normally done in DCIS

Treatment of the Axilla● Aim: Prevent cancer spread and establish prognosis (axillary nodes most important prognostic
indicator!)● Procedures:
Sentinel lymph node biopsy SNL1. Pre-op US with FNA2. Sentinel node biopsy
● Pre-op intradermal injection of technetium and methylene blue into tumour / periareolar● Wait 2h● Find first axillary node draining the cancer, excise and examine.● Find hot and blue nodes and excise just these
3. If sentinel node +ve for tumour => axillary clearanceAxillary sampling
1. Remove >4 nodes and analyse histologically, if any +ve then axillary clearance● Grades of axillary clearance
○ Axillary sampling Lower part of axillary fatpad, obsolete○ Level 1 Nodes up to axillary vein○ Level 2 Nodes up to pec minor○ Level 3 Nodes up to 1st rib○ The more, the higher the risk of nerve damage and lymphoedema
● Do NOT perform radiotherapy to a cleared axilla => inc. risk of lymphoedema

Surgical Treatment of Breast CA● Conservation surgery (usually <4cm)
○ Wide local excision WLE, removal of cylinder of breast tissue down to the pectoral muscle○ Limited axillary surgery○ Post-operative radiotherapy
● Total simple mastectomy (usually >4cm or too large in small breast or nipple)○ Removal of breast tissue, nipple and areola +/- axillary surgery
● Skin sparing mastectomy ○ Circular incision around nipple and removal of breast tissue with nipple by diathermy excision
through incision, followed by insertion of drainage tubes +/- implants and closure● Nipple sparing mastectomy with simultaneous reconstruction● Nipple and areola sparing mastectomy ● Most radical treatment - but no increased survival
○ Radical mastectomy with axillary clearance○ Post-operative radiotherapy (if >5cm or close to chest wall)
● +/- chemotherapy, endocrine and antibody therapy

Breast Reconstruction● Immediate● Delayed
○ If significant comorbidity○ or post-operative radiotherapy
● Becker prosthesis○ Prosthesis placed under the pectoralis muscle / implant with potential port○ Simplest procedure
● Autologous reconstruction / tissue flaps, when skin replacement needed○ Latissimus dorsi○ DIEP
■ Deep inferior epigastric perforator (a, anastomosed onto inf. mammary a)■ Only skin and fat flap
○ previously TRAB (now replaced by DIEP)■ Transverse abdominus, ■ Muscle sacrificed
○
Chemotherapy● Overall reduces the risk of (distal) recurrence by 20%● Greatest success in young node + xx● In each case, assess potential benefits against toxicity (RISK Management!)● Combination more effective than single agent (single more palliative)● Six cycles of cytotoxic chemo given 1/m for 6m● FEC: 5-fluorouracil, epirubicin and cyclophosphamide● Scoring of toxicity 0-4, 1 can still work, from 2 on cannot continue work● Side-effects
○ Alopecia (can prevent with scalp cooling)○ Mouth ulcers○ Sterility○ Myelosuppression○ Extravasation: stop infusion don’t remove!○ Lethargy○ Nausea and vomiting○ Teratogenicity○ Specific to individual drugs

Radiotherapy● Reduces (local) recurrence but not mortality● Usually combined with WLE● 50Gy external beam radiotherapy 5d/w for 3w● Side-effects
○ Tiredness○ Skin irritation (~sunburn) from ~week3○ Shrinkage of the irradiated breast
● Reduces risk of recurrence from 30% to 5% in 10y

Adjuvant Therapy● Improves survival by 5-10% over 10y● Oe antagonists / endocrine therapy
○ Usually for 5y if OeR +ve, especially if nodal spread. +/- ovarian ablation○ Also reduce risk of contralateral breast CA, recurrence, death rate, 5%/10% benefit if node
-ve/+ve at 10y○ Side effects: menopausal-type symptoms (less so with arimidex)○ Tamoxifen - actually a mixed agonist/antagonist = SERM selective OeR modulator○ Arimidex = anastrozole - an aromatase inhibitor that blocks peripheral oe production in
fat tissues in post-menopausal women where ovaries no longer produce Oe● Herceptin = Trastuzumab
○ HER2 antibody○ 25% of breast CA HER2 +ve (i.e. with HER2 overexpression?)○ Side-effects: cardiomyopathy and congestive cardiac failure○ Given every 3w for 1y as long as no cardiac problems○ 3-monthly echocardiograms to monitor (see NICE)
● Neo-adjuvant therapy***○ Treat with endocrine and/or cytotoxic drugs prior to surgery to allow shrinkage of the
tumour, followed by radiotherapy post-operatively

Prognosis● Predictive factors
○ Node involvement single best predictor of survival! Nr of nodes ~ p of distant mets!
○ Also: size, grade (differentiation), Nottingham Prognostic Index (size, grade and nodes), vascular invasion, hormone R, HER2 R, histo type.
● DCIS >90% 5y● if recurrence 50% invasive● <1% death risk
● <2cm 90% 5y● node -ve 80% 5y ● 16 nodes 50% 5y ● distant mets 15% 5y, life expectancy 2-3y● metastases to: (LCIS different: CSF, serosal surfaces, GI, ovaries, uterus, bone
marrow)lung liver brain kidneys bone adrenals (prostate in men)

Advanced Disease● Tumour >5cm initial Mx non-surgical: chemotherapy with subsequent surgery +/-
radiotherapy● Sole radiotherapy only if unfit for surgery or very elderly +/- adjuvant● Metastatic disease: systemic therapy = hormonal, chemotherapy for advanced
visceral disease● Treatment of bone mets
○ Radiotherapy○ Bisphosphonates
● Treatment of hypercalcaemia due to bone mets○ Hydration with IV saline○ Diuretics○ Bisphosphonates (inhibit Ras farnesylation and osteoclast proliferation)
● Palliative care○ Treat pain and other symptoms of advanced disease

Additional Infohttps://www.adjuvantonline.com/index.jsp
● Treatment of discharge of the breast○ Hadfield’s procedure: duct excision○ Microdochectomy: removal of the duct by a probe passed into it