Embed Size (px)
DESCRIPTION
Case record...Occipital lobe cavernoma
Citation preview

CLINICAL PICTURE:
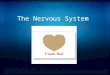
A 30 years old male patient presented clinically with a history of grand mal fits that are occasionally preceded by vivid visual hallucinations.
RADIOLOGICAL FINDINGS:
Figure 1. Type II left occipital cavernoma. Precontrast MRI T1 images. The characteristic MR imaging appearance of cavernomas is a well-defined, lobulated lesion with a reticulated core of heterogenous signal intensity on both T1 and T2 weighted sequences resulting from thrombosis, fibrosis, calcification, and hemorrhage. Extracellular and intracellular methemoglobin and thrombosis are responsible for the high intensity signal within the lesion, while calcifications, fibrosis, and acute and subacute blood are responsible for the low signal areas. The cavernoma in the current case has the classic "popcorn" appearance characteristic of type II cavernomas.
CASE OF THE WEEK
PROFESSOR YASSER METWALLY
CLINICAL PICTURE
RADIOLOGICAL FINDINGS

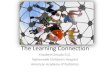
Figure 2. Type II left occipital cavernoma. Precontrast MRI T1 images. The characteristic MR imaging appearance of cavernomas is a well-defined, lobulated lesion with a reticulated core of heterogenous signal intensity on both T1 and T2 weighted sequences resulting from thrombosis, fibrosis, calcification, and hemorrhage. Extracellular and intracellular methemoglobin and thrombosis are responsible for the high intensity signal within the lesion, while calcifications, fibrosis, and acute and subacute blood are responsible for the low signal areas. The cavernoma in the current case has the classic "popcorn" appearance characteristic of type II cavernomas.
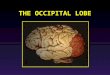
Figure 3. Type II left occipital cavernoma. Precontrast MRI T1 images. The characteristic MR imaging appearance of cavernomas is a well-defined, lobulated lesion with a reticulated core of heterogenous signal intensity on both T1 and T2 weighted sequences resulting from thrombosis, fibrosis, calcification, and hemorrhage. Extracellular and intracellular methemoglobin and thrombosis are responsible for the high intensity signal within the lesion, while calcifications, fibrosis, and acute and subacute blood are responsible for the low signal areas. The cavernoma in the current case has the classic "popcorn" appearance characteristic of type II cavernomas.
Conclusion
MRI picture of occipital cavernoma.

The MRI mixed signal intensity of the precontrast MRI T1 images and the MRI T2 images is due to the presence of altered blood of different ages.
1. The MRI T1 precontrast hyperintensity is due to methemoglobin
2. The MRI T2 hypointensity is due to hemosiderin pigments.
Table 1. Evolution of MR imaging signal characteristics [56]
Table 2. Cavernomas types [56]
DIAGNOSIS: INTRAMEDULLARY CAVERNOMA
DISCUSSION:
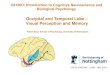
Cavernous malformations (CMs) are one of the four major types of vascular malformations of the central nervous system as classified by McConnick [1]. These lesions are composed of well-circumscribed sinusoidal vascular channels containing blood in various stages of evolution [1 -5]. In the literature, there are a number of synonyms for CMs including cavernomas, cavernous angiomas, angiographically occult vascular malformations, and cavernous hemangiomas [2-15]. In contrast with arteriovenous malformations and developmental venous anomalies, Cavernous malformations have immature blood-vessel wall components, lacking elastin and a significant amount of smooth muscle cells. Originally thought to he rare, CMs are now more commonly discovered because of improvements in neuroimaging techniques. On MR imaging, they are seen as well- circumscribed, reticulated, mixed signal-intensity lesions because of the mixture of oxyhemoglobin, deoxyhemoglobin, extracellular methemoglobin, and intracellular methemoglobin surrounded by an area of hypointensity that corresponds to hemosiderin deposition [6-16] . [Fig. 4]
Phase Time Iron-containing molecule
Iron oxidation
state
Red cell membranes T1 T2 T2*
Hyperacute Hours Oxyhemoglobin Fe2+ Intact Hypointense Hyperintense Acute Hours to
days Deoxyhemoglobin Fe2+ Intact iso/
Hypointense Hypointense Hypointense
Early subacute
Days to 1 week
Methemoglobin Fe2+ Intact Hyperintense Hypointense
Late subacute
1 week to months
Methemoglobin Fe2+ Degraded Hyperintense Hyperintense
Chronic >months Hemosiderin Fe2+ Degraded iso/ Hypointense Hypointense Hypointense
Abbreviations: Fe, iron; iso, isointense relative to normal brain.
Type Neuroimaging characteristics Type I Is a subacute bleed dominated by methemoglobin and therefore homogeneously hyperintense on TI
weighted images (Fig. 10) Type II The lesions have the classic "popcorn" appearance, heterogeneous on both TI and T2 weighted sequences
(Fig. 4, the current case) Type III The lesions are isointense to hypointense on both TI and T2 weighted images because of the predominance
of chronic blood products (Fig. 11) Type IV The lesions are tiny, punctate, foci hypointense on both TI and T2 weighted sequences. These type IV
lesions are often multiple and best seen on gradient echo sequences (Fig. 8). In contrast with telangiectasias, type IV lesions rarely enhance
DIAGNOSIS:
DISCUSSION

Clinically, patients with cavernous malformations are often symptomatic at some point in their lives [7-11,13,17-22]. A significant number of patients are left with neurologic deficits. The recommendations for treatment have varied widely and have ran the entire gamut from operating on the lesions as soon as they are discovered to watchful waiting despite recurrent bleeds. The recommendations for treatment should be based on the existing knowledge of the natural history of the disease.
Patient demographics, lesion location, and presentation
Cavernous malformations affect 0.4-0.9% of the general population according to large autopsy studies [1,13,23]. They constitute 5-16% of all vascular malformations [18,20,24,25]. Most of the lesions are found in the supratentorial compartment (80- 92%), whereas 8-20% are infratentorial [7,18,19,22]. In a study from the University of Toronto Vascular Malformation Study Group in 1997, Porter et al [19] classified lesions into deep and superficial, theorizing that the natural history of lesions in these two locations were significantly different. Deep lesions were those located in the brainstem, cerebellar nuclei, basal ganglia, and the thalamus. Based on this grouping and using a database of 353 patients, approximately 60% of lesions are superficial, 30% are deep, and 3% are within the spinal cord. In terms of specific locations, CMs follow the volume distribution of the neuraxis [7], being most common in the frontal lobe (28%) and followed by the temporal lobe (15.2%). Seventeen to fifty-four percent of patients have multiple lesions [9,19,22,26]. Fifty to eighty- five percent of patients with multiple CMs have a familial type of lesion [9,11,18,22,26,27].
Figure 4. Cavernous malformation (CM): classic morphology. (A) T I weighted MR imaging shows an intra-axial heterogeneous mass (arrow) with pockets of high signal intensity. (B) T2 weighted MR imaging shows a heterogeneous mass (arrow) with a complete rim of hypointensity (hemosiderin) and loculated areas of high signal intensity.
Cavernous malformations appear to have no significant sex predilection. The usual range of age at presentation is from the 2nd to the 5th decades, with the mean usually in the latter 4th decade [ 17,19]. The most common presentation in most series is seizures [7,8,11-13,18]. Seizures were the most common presentation (36%) in the series by Porter et al [19]. The second most common presentation was hemorrhage (25%). Twenty percent presented with focal neurologic deficits without radiographic hemorrhage; 12% were found incidentally; and 6% presented with headaches. In a review of patients with intraventricular CMs (45 cases), Reyns et al [10] found that the common clinical presentations were similar to tumors in the same location (ie, hypothalamic dysfunction, increased intracranial pressure, hydrocephalus). Twenty percent had intraventricular hemorrhage and 16% presented with seizures [10]. In a review of four patients with third ventricular CMs, Sinson et al noted that none of the patients presented with seizures. Their patients presented with hydrocephalus, memory loss, and hypothalamic dysfunction [15].

Figure 5. Radiation induced cavernoma in a patient treated from medulloblastoma with surgery and radiation. A,B immediately following treatment, C,D a year after, and E,F one year later, notice the progressive development of a pontine cavernoma.
The clinical manifestations of supratentorial cavernomas in one study. 55

DE NOVO FORMATION AND FAMILIAL CAVERNOUS MALFORMATIONS
Initially, all cavernous malformations were thought to be congenital. There is now evidence that CMs can arise de novo. Factors associated with de novo formation of CMs are previous irradiation [6,9,21,28,29], genetics in familial cases [22,27], viruses [21], hormonal influences especially in pregnancy [21], and local seeding along a biopsy tract [6,30]. There is a report of a lesion arising de novo in a patient with neither previous irradiation nor a family history [28]. This patient underwent excision of an acoustic neuroma and was subsequently found to have a CM on follow-up imaging.
Cavernous malformations have been shown to arise in patients with previous irradiation (Fig. 5). Studies involving children treated with radiotherapy showed that a "second hit" by irradiation to genetically predisposed tissue may lead to the formation of CMs [6,29,31]. Some authors believe that CMs related to irradiation are more prone to hemorrhage [29]. Once these new lesions are formed, the late radiation effects may lead to growth by mechanisms of angiogenesis, hemorrhage, and thrombosis [9,29].
Familial cases of CMs have been shown to have a 0.2-0.4% incidence per patient per year of de novo lesion formation [22,27,31]. In a recent prospective study involving 33 patients belonging to unrelated French families, 30% of patients were noted to develop new lesions during a two-year follow-up period [32]. The familial type is inherited by autosomal dominant transmission with incomplete penetrance [33]. In Hispanic Americans, the genetic defect responsible for familial lesions, CCM 1, has been localized to chromosome 7q ll-22 [8,22]. Further analysis revealed that KRIT I (a gene at the 7ql 1 -22) mutations are responsible for cerebral CMs [34]. In non-Hispanic Caucasians, two gene loci were identified to be responsible for cerebral CMs: CCM 2 at 7pl3-15 and CCM 3 at 3q25.2-27 [33]. Aside from having a higher rate of de novo formation as compared with sporadic lesions, some authors believe that familial lesions have a higher annual hemorrhage rate [27,32].
Developmental venous anomalies (DVAS) have also been reported to be associated with and possibly play an etiologic role in the formation of CMs [21,23,31,35]. DVAs (previously referred to as venous angiomas) are the most common cerebral vascular malformations, with approximately 4% of the population being affected [36,37]. DVAs simply represent an extreme variant of the normal venous drainage, however. DVAs drain normal brain and must be preserved when CMs are excised [38]. They typically appear on MR imaging as radiating, linear flow-voids (a "caput medusa" pattern) centered on a large collecting vein (Fig. 6). DVAs typically enhance with contrast. According to Dillon et al [39], most DVAs have a collector vein stenosis, and this venous restrictive disease leads to an increased pressure within the capillary bed. This increased venous pressure may cause niicrohemorrhages or red blood cell diapedesis within the parenchyma that in turn leads to angiogenic proliferation. The presence of red blood cells activates a vicious cycle wherein the extruded blood draws fibroblasts that lay down fragile, leaky vessels which in turn leads to more microscopic or gross hemorrhage. Endothelial development in chronic hematomas supports this mode of de novo CM development [35]. In relation to this, a study by Sure et al using immunohistochemical techniques with proliferating cell nuclear antigen (PCNA) and vascular endothelial growth factor (VEGF) showed that CMs have the capacity for endothelial proliferation and neoangiogenesis [40]. A higher concentration of these angiogenic factors in CMs may also explain the development of new cavernous malformations along a biopsy tract. It may be that a small amount of CM tissue transplanted to any point along the biopsy tract may induce the transformation of normal capillaries or the growth of new, fragile vessels. Another explanation is that the
Age of first haemorrhage in 47 cases of supratentorial cavernomas in one study. 55

transplanted CM tissue may become recanalized by nearby parenchymal vessels [30].
HISTOPATHOLOGY
Cavernous malformations are discrete, well-circumscribed lesions composed of thin-walled, dilated vascular channels lined by a single layer of endothelium in a collagenous, fibronectin-rich matrix [7- 9,11,17,33,40,41] (Fig. 7). This conglomeration of sinusoidal vascular channels and its matrix is devoid of elastin, laminin , subendothelial smooth muscle cells, and other mature vascular wall components [9,42]. The surrounding parenchyma contains hemosiderin-laden macrophages and iron-laden glial cells [11]. The lack of intervening brain parenchyma is one of the hallmarks. CMs, however, are not always compact. They may at times be racemose, containing small satellite-like projections into the surrounding brain [9,43]. Grossly, lesions have often been described as mulberry-like in appearance because of the berry-like clusters that contain hemorrhage in various stages of organization [44]. Ultrastructurally, endothelial cells are seen to line the thin cavernous walls that are made up of amorphous, disorganized collagen. Tight junctions and pericytes are noted to be less in number as compared with those in normal blood vessels [41]. The combination of thin walls, composed of amorphous material lacking subendothelial support, and the small number of tight junctions and pericytes predispose to the known propensity of these lesions to leak or bleed [41]. immunohistochemical studies have shown that these lesions do not express laminin, signifying immature and brittle vessels [9]. They stain significantly for fibronectin, consistent with proliferating and leaky vessels [9].
Table 3. Pathological characteristics of cavernomas that differentiate them from arteriovenous malformation
Cavernous angiomas (cavernomas) consist of enlarged capillaries with the following characteristics:
Sinusoidal
Single layer of endothelium
Thin collagenous wall
Lack of smooth muscle fibers and elastic fibers
Capillaries are immediately adjacent to each other, with no intervening neural tissue.
The surrounding parenchyma contains hemosiderin-laden macrophages and iron-laden glial cells.
They typically are not associated with enlarged feeding arteries or draining veins, and blood flow is low or even stagnated (cavernomas are angiographically occult).
Grossly, they may range from soft to hard.
Thrombosis, calcification, or ossification results in a harder lesion.
Adjacent neural tissue may be affected, and small hemorrhages result in hemosiderin staining (iron salts may incite an epileptogenic focus). Tissues also may be gliotic.

Figure 6. Cavernous malformation and associated developmental venous anomaly (DVA). (A)'I'2 weighted MR imaging shows a heterogeneous mass with a hemosiderin ring (arrow). (B) Gadolinium-enhanced Tl weighted MR imaging shows a radiating collection of vessels adjacent to the CM that join one large collecting vein (arrow).
Figure 7a. Histopathology. (A) Microscopic section (trichrome stain) shows a mass of closely apposed vessels of varying size. The vessel walls have a variable thickness, and there is no intervening brain. (B) Whole mount (trichrome stain) of a CM of the third ventricle shows a plexus of vessels with some intervening brain at the periphery.

Figure 7b. Example of cavernomas, notice absence of feeding arteries or draining veins
Figure 7c. Pontine cavernoma, notice absence of feeding arteries or draining veins

Figure 7d. For comparison, an arteriovenous malformation, notice the feeding arteries and the draining veins
IMAGING
Radiographically, high resolution MR imaging is the diagnostic tool of choice for detecting and identifying CMs. On noncontrast CT, CMs frequently appear as focal areas of increased density within the brain often without mass effect (Fig. 8). The increased density either represents calcium, blood, or a combination of the two. The margins of the lesion are usually indistinct and the increased density may have a stippled appearance. The differential diagnosis on CT includes low-grade calcified neoplasms, hemorrhage, and vascular malformations. MR imaging is required to make a more definitive diagnosis. The characteristic MR imaging appearance is a well-defined, lobulated lesion with a reticulated core of heterogenous signal intensity on both T1 and T2 weighted sequences resulting from thrombosis, fibrosis, calcification, and hemorrhage. Extracellular and intracellular methemoglobin and thrombosis are responsible for the high intensity signal within the lesion, while calcifications, fibrosis, and acute and subacute blood are responsible for the low signal areas. On T2 weighted or gradient echo images, there is a peripheral ring of hypointensity that corresponds to the deposition of hemosiderin and iron in the surrounding brain parenchyma [7-11,14,16,19,22]. The hemosiderin ring may not be evident in intraventricular cavernous malformations. Intraventricular CMs can exhibit rapid growth and be quite voluminous, leading to a diagnosis of a tumor instead of a vascular malformation [10,21] (Fig. 9).
Table 4. Neuroimaging characteristics of cavernomas
Cavernous malformations are angiographically occult lesions. They are by far the most common type of angiographically occult vascular malformation [13,43]. Earlier reports on angiography in CMs described venous pooling or a capillary blush in some lesions [9,11]. Presently, angiography has no role in the diagnosis. CT scan is a relatively sensitive test to detect cavernous malformations, but it is not specific. Vaquero stated that in their series, CT scanning was only able to diagnose CMs in 44% of patients [45]. Marraire et al in a later study reiterated the high sensitivity (70-100%) and low specificity ({50%) of this modality in the diagnosis of CMs [9]. On CT the presence of thrombosis and hemorrhage in various stages of evolution cannot be accurately characterized.
On noncontrast CT, CMs frequently appear as focal areas of increased density within the brain often without mass effect. The increased density either represents calcium, blood, or a combination of the two. The margins of the lesion are usually indistinct and the increased density may have a stippled appearance.
The characteristic MR imaging appearance is a well-defined, lobulated lesion with a reticulated core of heterogenous signal intensity on both T1 and T2 weighted sequences resulting from thrombosis, fibrosis, calcification, and hemorrhage. Extracellular and intracellular methemoglobin and thrombosis are responsible for the high intensity signal within the lesion, while calcifications, fibrosis, and acute and subacute blood are responsible for the low signal areas.
On T2 weighted or gradient echo images, there is a peripheral ring of hypointensity that corresponds to the deposition of hemosiderin and iron in the surrounding brain parenchyma

Zabramski et al classified CMs into four types (I- IV) based on the MR imaging appearance [22]. Type I is a subacute bleed dominated by methemoglobin and therefore homogeneously hyperintense on TI weighted images (Fig. 10). Type II lesions have the classic "popcorn" appearance, heterogeneous on both TI and T2 weighted sequences (Fig. 4). Type III lesions are isointense to hypointense on both TI and T2 weighted images because of the predominance of chronic blood products (Fig. 11). Type IV lesions are tiny, punctate, foci hypointense on both TI and T2 weighted sequences. These type IV lesions are often multiple and best seen on gradient echo sequences [11,22,46] (Fig. 8). In contrast with telangiectasias, type IV lesions rarely enhance [6]. Gradient echo sequences best identify these lesions because of the susceptibility artifact from microscopic deposits of hemosiderin [6]. Several authors have noted that patients with type I and type 11 lesions were more commonly symptomatic compared with the other types [22,27,32].Willinsky et al [16] in 1996 reviewed their own series (156 patients) and on serial MR imaging studies found no significant correlation between the type of CM (according to Zabramski's classification) and the natural history of the lesion. None of the four morphological appearances were immune from change, and the evolution of the lesions was not predictable based on the original morphology (Fig. 12).
Table 2. Cavernomas types
Type Neuroimaging characteristics Type I Is a subacute bleed dominated by methemoglobin and therefore homogeneously hyperintense on TI
weighted images (Fig. 10) Type II The lesions have the classic "popcorn" appearance, heterogeneous on both TI and T2 weighted sequences
(Fig. 4, the current case) Type III The lesions are isointense to hypointense on both TI and T2 weighted images because of the predominance
of chronic blood products (Fig. 11) Type IV The lesions are tiny, punctate, foci hypointense on both TI and T2 weighted sequences. These type IV
lesions are often multiple and best seen on gradient echo sequences (Fig. 8). In contrast with telangiectasias, type IV lesions rarely enhance
Figure 8. Multiple CMs. (A) Noncontrast CT shows two areas of hyperdensity with no mass effect and no edema. (B,C) T2 weighted MR imaging shows two left frontal lobe lesions. Both have central areas of mixed signal intensity and a surrounding rim of hemosiderin. (D) Gradient echo MR imaging shows multiple foci of hypointensity. Only the largest lesions were evident on the spin-echo images. The small foci that are seen only with the gradient echo technique have been referred to as type TV CMs.

Figure 9. Intraventricular CM. (A) Sagittal TI weighted MR imaging shows a heterogeneous hyperintense lesion in the third ventricle (arrow). (B) Axial T2 weighted MR imaging shows a hemosiderin rim surrounding the hyperintense lesion (arrow).
In cases where a CM is suspected but the radiologic image is not pathognomonic, serial imaging is of value if immediate surgical intervention is not warranted. Differential diagnoses include neoplasms, infectious and inflammatory masses, hemorrhagic emboli, and hematomas. If there is a recent bleed or thrombosis in a CM, the typical features of a CM are not evident (Figs. I0 and 11). The hemosiderin ring may be obscured by a recent bleed and therefore follow-up MR imaging is important to establish CM as the cause for the bleed. Peri-lesional and extralesional hemorrhage may be evident outside the hemosiderin ring [16]. Repeat MR imaging is also needed in patients who report a worsening of symptoms or when new deficits are detected by the clinician. The presence of edema and mass effect on MR imaging may correlate with new signs and symptoms that the patient has developed [16] (Figs. 10-12). Hemorrhage outside the hemosiderin ring may be evident in patients with new clinical findings or worsening of an existing deficit [16]. A fluid/fluid level may be evident in some active CMs (Fig. 14). On serial MR imaging, a change in the signal intensity within the lesion may or may not correspond with recent clinical events. Clinical deterioration can, however, also occur without any significant change in the MR imaging [19]. On MR imaging, there may be changes in the size of the CM or the signal intensity within the lesion without a corresponding clinical event in the patient.
Figure 10. Type I CM. (A) TI weighted MR imaging shows a homogeneous hyperintense lesion. (B) T2 weighted MR Imaging shows a lesion with a well-defined hemosiderin rim and no surrounding edema.

Figure 11. Type 3 CM. (A,B) Tl and T2 weighted MR imaging shows a homogeneous hypointense lesion on both sequences (arrows).
There are pitfalls in the interpretation of post- operative MR imaging of CM. The postoperative MR imaging often appears similar to the preoperative image. This occurs despite the impression at surgery that there was a complete resection. The most plausible explanation for this is that the excision cavity is filled with organizing blood products. The natural history of such postoperative findings is unknown, so ongoing serial imaging and clinical follow-up is prudent.
NATURAL HISTORY
There has been much controversy regarding the natural history of CMs. Several factors have lead to this confusion: the variability of the periods at risk identified by different authors, different definitions of hemorrhage, patterns of referral, MR imaging versus clinical/radiographic studies, and the timing of the MR imaging follow-up. Because CMs were originally considered to be congenital, early reports defined the period at risk as beginning from birth. These studies assumed that the CMs were present at birth and the risk of bleeding was the same throughout life [7]. These retrospective studies had lower hemorrhage rates compared with studies that based their calculations on the time from the initial diagnosis to the final follow-up. The evidence is clear that CMs can be acquired [6,9,22,27-29,32,35,40].
In the literature, the definition of hemorrhage in relation to CMs has varied. This inconsistency has lead to significant variation in the estimated hemorrhage rate. It is better to use a radiologic definition of hemorrhage to eliminate any ambiguity "acute or subacute blood located outside the hemosiderin ring or an increase in lesion size by 20% or more in diameter on serial imaging with associated mass effect and/or edema" (Fig. 15) [16]. Because of the observation that several patients being followed had clinical deterioration without radiologic evidence of hemorrhage, as defined above, Porter et al used the term clinical/neurologic events to study the natural history of CMs. A clinical/neurologic event was defined as deterioration in symptoms as noted by the patient and worsening or new onset of neurologic signs as detected by the clinician [19]. New symptoms alone (eg, increased headache only) were not sufficient to qualify. Clinical/neurologic events are independent of hemorrhages and therefore may or may not be accompanied by radiologic proof of hemorrhage (Fig. 14) [19]. As symptoms and deficits are more important to the patient than results of MR imaging, it is preferable to report event rates, as these are more encompassing in terms of clinical deterioration (with or without hemorrhage) as opposed to hemorrhage rates that may or may not have clinical significance.

Figure 12. Morphological changes on serial imaging in a patient with CMs. (A) Initially the proton density weighted MR imaging shows that the occipital pole lesion is hyperintense (arrow). (B) Later, it has a heterogeneous appearance (arrow). (C) Finally, it is homogeneously hypointense (arrow).
In defining the natural history of CMs, it would be beneficial if patient or lesional factors could be identified that predict a poor prognosis. Throughout the years, several authors have reported on patient and lesional characteristics that may predict the natural history of these lesions. Lesion presentation, location, size, number, MR imaging appearance, presence of DVAS, familial occurrence, timing from initial event, and patient age, sex, and pregnancy have all been studied [6-9,12-17,19,21-23,26,27,32, 42,43,47-49].
Figure 13. Symptomatic hemorrhage in a cerebellar cavernoma (confirmed surgically)
The most significant predictor of clinical events is lesion location [19]. When lesions were classified as supratentorial versus infratentorial, the infratentorial lesions had a higher event rate (10.61/o/year vs. 0.41/o/year). In a recent review of the same database with a longer follow-up and more patients, there was still a statistically significant difference in the annual event rates between these two locations (6.5% for infratentorial vs. 0.7% supratentorial) (Peter Rivera, MD, University of Toronto Vascular Malformation Study Group, February 2002). The significance of location assumes an even stronger power when the lesion location is classified as superficial versus deep. The annual event rate reported by Porter et al is 10.6% for the deep lesions and 0% for the superficial lesions. A more recent study shows the same trend, with deep lesions having a statistically significant difference in annual event rates when compared with superficial lesions [19]. When a Cox proportional hazards modeling was used to verify the relative importance of these various factors, lesion location when classified as deep versus superficial was the most important predictor of subsequent events. There are several hypotheses as to why deep CMs have more clinical events than superficial CMs. Intuitively, the most plausible explanation is that the eloquence of deep structures will lead to clinical signs and symptoms even with a small change in the lesion., either growth or hemorrhage. The same small change would probably not manifest any signs in a superficial lesion. There may also be an inherent physiologic and structural difference between superficial and deep structures that may predispose to lesion activity. Differences in venous pressures between deep and superficial neural tissue might be another reason r the higher event rate in deep

lesions [19]. Studies to validate these hypotheses have not been done.
The growth of CMs is related to repeated intralesional hemorrhage, thrombosis, and subsequent organization and recanalization [21,43,50]. Enlargement of hemorrhagic cysts, deposition of hemosiderin, recanalization of thrombi with formation of new vascular channels, and reactive gliosis may all add to the bulk of the lesion [21]. Repeated intralesional microhemorrhages and their breakdown products can also initiate a series of responses such as cellular proliferation, fibrosis, calcification, and gliosis that promote new vessel formation and coalescence (hemorrhagic angiogenic proliferation) [9,21]. The leaky vessels produced by this reactive angiogenesis and the neovascularization of hemorrhagic cysts lead to further microscopic or gross hemorrhages that perpetuate the cycle and result in growth of the lesion. These changes in the lesion may or may not have clinical manifestations.
Figure 14. CM: fluid/fluid level. (A,B) Tl and T2 weighted NM imaging shows a cerebellar mass compressing the fourth ventricle and surrounded by edema. The T I hyperintensity, T2 hypointensity, and fluid/fluid levels all indicate subacute blood products.
Figure 15. CM: growth secondary to hemorrhage. (A,B)'I'2 weighted MR imaging shows a small hypointense lesion on the initial scan (eirroA,) that increased in size (curved arrow) on the follow-up scan I year later. The interval change in size and the development of surrounding edema indicates a hemorrhage. The patient had seizures only.
Recovery from events
Several authors have studied recovery from neurologic events secondary to lesion activity. Tung et al reported that an initial bleed caused only a transient deficit in 80% of patients [42]. They observed, however, that with each

subsequent hemorrhage, there is an increased chance of the patient ending up with a deficit, noting that all patients with more than two bleeds had persistent neurologic deficits. In one study Porter et al reported that only one third of patients experiencing an event will recover fully. One third of patients with events will have no significant recovery, and one third will have, partial recovery [19]. This study reports that there is no difference in the degree of recovery when comparing hemorrhagic versus nonhemorrhagic events, supratentorial versus infratentorial lesions, and deep versus superficial locations. In an updated review of this same patient population, with more patients and a longer follow-up, Porter et al [19] still found no difference in the recovery of patients from hemorrhagic versus nonhemorrhagic events and between supratentorial versus infratentorial lesions. No difference was found in the degree of recovery between superficial and deep lesions; 50% of patients with clinical events related to superficial lesions completely recovered compared with only 33% of patients with deep lesions (P = 0.024).
Figure 16. Intraventricular cavernoma
MANAGEMENT
The recommendations for the management of patients with cavernous malformations have varied throughout the years. In general surgery is hardly advised for superficial lesions because of the benign nature and course of superficial lesions. Surgery is probably only indicated for seizure control in superficial lesions.
Deep lesions have a greater propensity to produce symptoms and deficits compared with superficial lesions. Intuitively, therefore, management of these patients should be more aggressive, as the postoperative functional status largely depends on the preoperative neurologic function. Logically, it would be beneficial to the patient to be treated before any deficits arise from these deep lesions. Approaching lesions in the deep areas of the neuraxis, however, particularly the brainstem, carries significant risk. Although several authors have reported good results with surgery in terms of neurologic function, these results should be interpreted with caution, as these are highly selected series [14,15,20,42,51]. In addition, lesions that do reach the pial or ependymal surface carry an even higher risk at surgery, because eloquent tissue must be traversed to reach the lesion.
Radiosurgery of CMs has been considered to be an appealing alternative to surgery, particularly in the deep lesions. The literature on radiosurgery of CMs is inconclusive. In 1995, Kondziolka et al reported on their series of 47 patients [17]. They quoted an annual hemorrhage rate of 56.5% (including the first bleed) and a subsequent hemorrhage rate of 320/o/year. This high hemorrhage rate reflects the fact that this population was a highly selected group, and hemorrhage was defined as any clinical or radiologic event. After treatment with radiosurgery, they reported hemorrhage rates of 8.8% for the first two years, then 1. I %/year from two to six years. They concluded that there is a latency of 2-3 years for the maximal effects of radiosurgery to take place, with the most benefit experienced after 3.5 years [52]. Karisson et al [53], based on their experience at the Karolinska Institute, reported that 9 out of 22 patients developed a hemorrhage after radiosurgery with the gamma knife, and 6 developed radiation-induced complications, with 2 patients experiencing both. They quoted an 8.8% hemorrhage rate after radiosurgery. They noted a trend for the hemorrhage rate to decrease four years after treatment. They reported that there is a sevenfold increase in the occurrence of complications in the treatment of CMs when compared with treating arteriovenous malformations with the same dose distribution. They concluded that the high incidence of complications does not justify the limited protection the treatment provides in only exceptional cases [53]. Results presented by Pollock et al [54] agree with those from the Karolinska group. They noted a 59% morbidity rate (transient and permanent) after treatment and a 41% permanent radiation-related morbidity for CMs. Pollock et al

agree with Karlsson that whatever protection radiosurgery provides for these patients may not be worth the significant occurrence of radiation-induced complications [54].
Present literature supports the fact that the hemorrhage rates after radiosurgery decrease after a latency of about two to four years. This statement has to be qualified, however, as only a select group of patients benefit and a significant number of patients experience permanent morbidity, either from hemorrhage after the treatment or from radiation-induced necrosis. Also, the reduction in hemorrhage rates after treatment may actually reflect the natural course of a CM after a bleed (caused by clustering of events), and not actual protection provided by the irradiation [48,54]. Barker et al reported a monthly rehemorrhage rate of 2.0% during the first 2.5 years after an initial symptomatic hemorrhage. This was followed by a decrease in the hemorrhage risk to less than 1% per month without any treatment [48].
Patients with superficial CMs are advised of the benign course of their disease and are usually asked to come for follow-up every one to two years, unless surgery is required for medically refractory seizures. Patients with deep CMs are informed that clinical events are not uncommon, up to 10% per year. The risks, benefits, and possible complications of surgery are discussed with patients who have deep lesions with pial or ependymal representation. Symptomatic patients with lesions that have no pial nor ependymal representation are also considered for surgery. For deep, symptomatic lesions that do not reach the pial or ependymal surfaces, we consider stereotactic radiosurgery as a potential treatment modality, still of unproven value, and would encourage its use only in the setting of a randomized, controlled trial that allows direct comparison to the natural history over time.
SUMMARY
Cavernous malformations are commonly being recognized on CT and MR imaging in both asymptomatic and symptomatic patients. The diagnosis of CMs can often be made on MR imaging based on the characteristic morphology of the subacute and chronic blood products. An atypical appearance of a CM in the setting of a recent hemorrhage requires follow-up imaging to confirm the diagnosis. Deep CMs have a significant clinical event rate that justifies close follow up or surgical treatment if possible.
Addendum
A new version of this PDF file (with a new case) is uploaded in my web site every week (every Saturday and remains available till Friday.)
To download the current version follow the link "http://pdf.yassermetwally.com/case.pdf". You can also download the current version from my web site at "http://yassermetwally.com". To download the software version of the publication (crow.exe) follow the link:
http://neurology.yassermetwally.com/crow.zip The case is also presented as a short case in PDF format, to download the short case follow the link:
http://pdf.yassermetwally.com/short.pdf At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to
know more details. Screen resolution is better set at 1024*768 pixel screen area for optimum display. For an archive of the previously reported cases go to www.yassermetwally.net, then under pages in the right
panel, scroll down and click on the text entry "downloadable case records in PDF format"
SUMMARY

References
[1] McCormick WF. The pathology of vascular ("arteriovenous") malformations. J Neurosurg 1966;24: 807-16.
[2] Lobato RD, Perez C, Rivas JJ, et al. Clinical, radiological, and pathological spectrum of angiographically occult intracranial vascular malformations. Analysis of 21 cases and review of the literature. J Neurosurg 1988; 68:518-31.
[3] Ogilvy CS, Heros RC, Ojemann RG, et al. Angiographically occult arteriovenous malformations. J Neurosurg 1988;69:350-5.
[4] Bruner JM, Tien RD, McLendon RE. Tumors of vascular origin. In: Bigner DD, McLendon RE, Bruner JM, editors. Russell and Rubenstein's pathology of tumors of the nervous system. 6th edition. London: Arnold; 1998. p. 260-4.
[5] Tomlinson F, Houser OW, Scheithauer BW, et al. Angiographically occult vascular malformations: a correlative study of features on magnetic resonance imaging and histological examination. Neurosurgery 1994;34: 792 - 9.
[6] Clatterbuck R, Mofty JL, Elmaci 1, et al. Dynamic nature of cavernous malformations: a prospective magnetic resonance imaging study with volumetric analysis. J Neurosurg 2000;93:981-6.
[7] Del Curling Jr 0, Kelly DL, Elster AD, et al. An analysis of the natural history of cavernous angiomas. J Neurosurg 1991;75:702-8.
[8] Dubovsky J, Zabramski J, Kurth J, et al. A gene responsible for cavernous malformations of the brain maps to chromosome 7q. Hum Mol Genet 1995;4(3):453 - 8.
[9] Maraire JN, Awad IA. Intracranial cavernous malformations: lesion behavior and management strategies. Neurosurgery 1995;37:591-605.
[10] Reyns N, Assaker R, Louis E, et al. Intraventricular cavernomas: three cases and a review of the literature. Neurosurgery 1999;44:648-53.
[11] Rigamonti D, Drayer BP, Johnson PC, et al. The MRI appearance of cavernous malformations (angiomas). J Neurosurg 1987;67:518-24.
[12] Robinson J, Awad IA, Magdinec M, et al. Factors predisposing to clinical disability in patients with cavernous malformations of the brain. Neurosurgery 1993; 32:730-5.
[13] Robinson J, Awad IA, Masaryk TJ, et al. Pathological heterogeneity of angiographically occult vascular malformations of the brain. Neurosurgery 1993;33: 547-54.
[14] Steinberg G, Chang S, Gewirtz R, et al. Microsurgical resection of brainstem, thalamic, and basal ganglia angiographically occult vascular malformations. Neurosurgery 2000;46:260-70.
[15] Sinson G, Zager E, Grossman R, et al. Cavernous malformations of the third ventricle. Neurosurgery 1995; 37:37-41.
[16] Willinsky R, Harper W, Wallace MC, et al. Follow-up MR of intracranial cavernoma: the relationship between haemorrhagic events and morphology. interventional Neuroradiology 1996;2:127-35.
[17] Kondziolka D, Lunsford LD, Kestle JR. The natural history of cerebral cavernous malformations. J Neurosurg 1995;83:820-4.
[18] Moiiarity JL, Wetzel M, Clatterbuck RE, et al. The natural history of cavernous malformations: a prospective study of 68 patients. J Neurosurg 1999;44:1166-73.
[19] Porter P, Willinsky R, Harper W, et al. Cerebral cavernous malformations: natural history and prognosis after
REFERENCES

clinical deterioration with or without hemorrhage. J Neurosurg 1997;87:190-7.
[20] Porter R, Detwiler P, Spetzler R, et al. Cavernous malformations of the brainstem: experience with 100 patients. J Neurosurg 1999;90:50-8.
[21] Pozzati E, Acciarri N, Tognetti F, et al. Growth, subsequent bleeding, and de novo appearance of cerebral cavernous angiomas. Neurosurgery 1996;38: 662-9.
[22] Zabramski JM, Wascher TM, Spetzler RF, et al. The natural history of familial cavernous malformations: results of an ongoing study. J Neurosurg 1994;80: 422-32.
[23] Abduirauf S, Kaynar MY, Awad IA. A comparison of the clinical profile of cavernous malformations with and without associated venous malformations. Neurosurgery 1999;44:41-5.
[24] Amin-Hanjani S, Ogilvy CS, Candia GJ, et al. Stereotactic radiosurgery for cavernous malformations: Kjellberg's experience with proton beam therapy in 98 cases at the Harvard cyclotron. Neurosurgery 1998;42: 1229-38.
[25] Giombini S, Morello G. Cavernous angiomas of the brain. Account of fourteen personal cases and review of literature. Acta Neurochir 1978;40:61-82.
[26] Kim DS, Park YG, Choi JU, et al. An analysis of the natural history of cavernous malformations. Surg Neurol 1997;53:30-40.
[27] Labauge P, Brunereau L, Levy C, et al. The natural history of familial cerebral cavernomas: a retrospective MRI study of 40 patients. Neuroradiology 2000;42: 327-32.
[28] Detwiler P, Porter RW, Zabramski JM, et al. De novo formation of a central nervous system cavernous malformation: implications for predicting risk of hemorrhage. J Neurosurg 1997;87:629-32.
[29] Larson J, Ball WS, Bove KE, et al. Formation of intracerebral cavernous malformations after radiation treatment for central nervous system neoplasia in children. J Neurosurg 1998;88:51-6.
[30] Ogilvy CS, Moayeri N, Golden JN. Appearance of a cavernous hemangioma in the cerebral cortex after biopsy of a deeper lesion. Neurosurgery 1993;33: 307-9.
[31] Pozzati E, Giangaspero F, Marliani F, et al. Occult cerebrovascular malformations after irradiation. Neurosurgery 1996;39:677-84.
[32] Labauge P, Brunereau L, Laberge S, et al. Prospective follow-up of 33 asymptomatic patients with familial cerebral cavernous malformations. Neurology 2001; 57(10):1825-8.
[33] Craig H, Gunel M, Cepeda 0, et al. Multilocus linkage identifies two new loci for a Mendelian form of stroke, cerebral cavernous malformation, at 7pl5-13 and 3q25.2-27. Hum Mol Genet 1998;7(12):1851-8.
[34] Zhang J, Clatterbuck R, Rigamonti D, et al. Mutations in KRITI in familial cerebral cavernous malformations. Neurosurgery 2000;46:1272-9.
[35] Maeder P, Gudinchet F, Meuli R, et al. Development of a cavernous malformation of the brain. AJNR 1998; 19:1141-5.
[36] Gamer TB, Del Curling Jr 0, Kelly Jr DL, et al. The natural history of intracranial venous angiomas. J Neurosurg 1991;75:715-22.
[37] Truwift CL. Venous angioma of the brain: history, significance and imaging findings. AJR Am J Roentgenol 1992;159:1299-307.
[38] Sazaki 0, Tanaka R, Koike T, et al. Excision of cavernous malformation with preservation of coexisting venous angioma. J Neurosurg 1991;75:461-4.

[39] Dillon WP. Cryptic vascular malformations: controversies in terminology, diagnosis, pathophysiology, and treatment. Am J Neuroradiol 1997;18:1839-46.
[40] Sure U, Butz N, Schlegel J, et al. Endothelial proliferation, neoangiogenesis, and potential de novo generation of cerebrovascular malformations. J Neurosurg 2001;94:972-7.
[41] Wong J, Awad IA, Kim JH. Ultrastructural pathological features of cerebrovascular malformations: a preliminary report. Neurosurgery 2000;46:1454-9.
[42] Tung H, Giannotta SL, Chandrasoma PT, et al. Recurrent intraparenchymal hemorrhages from angiographically occult vascular malformations. J Nearosurg 1990; 73:174-80.
[43] Tomlinson F, Houser OW, Scheithauer BW, et al. Angiographically occult vascular malformations: a correlative study of features on magnetic resonance imaging and histological examination. Neurosurgery 1994;34: 792-9.
[44] Cammta PJ, Heros RC. Arteriovenous malformations of the Brain. In: Youmans JR, editor. Neurological surgery: a comprehensive reference guide to diagnosis and management of neurosurgical problems. 4th edition. Philadelphia: N" Saunders; 1996. p. 1372 - 404.
[45] Vaquero J, Salazar J, Martinez R, et al. Cavernomas of the central nervous system: clinical syndromes, CT scan diagnosis, and prognosis after surgical treatment. Acta Neurochir 1987;85:29-33.
[46] Rigamonti D, Johnson PC, Spetzier RF, et al. Cavernous malformations and capillary telangiectasia: a spectrum within a single pathological entity. Neurosurgery 1991;28:60-4.
[47] Aiba T, Tanaka R, Koike T, et al. Natural history of intracranial cavernous malformations. J Neurosurg 1995;83:56-9.
[48] Barker II FG, Amin-Hanjani S, Buttler WE, et al. Temporal clustering of hemorrhages from untreated cavernous malformations of the central nervous system. Neurosurgery 2001;49:15 23.
[49] Kupersmifli MJ, Kalish H, Epstein F, et al. Natural history of brainstem cavernous malformations. Neurosurgery 2001;48:47-52.
[50] Scott RM, Bames P, Kupsky W, et al. Cavernous angiomas of the central nervous system in children. J Neurosurg 1992;76:38-46.
[51] Amin-Hanjani S, Ogilvy C, Ojemann R, et al. Risks of surgical management for cavernous malformations of the nervous system. Neurosurgery 1998;42:1220-6.
[52] Kondziolka D, Lunsford D, Flickinger J, et al. Reduction of hemorrhage risk after stereotactic radiosurgery for cavernous malformations. J Neurosurg 1995;83: 825-31.
[53] Karlsson B, Kiblstrom L, Lindquist C, et al. Radiosurgery for cavernous malformations. J Neurosurg 1998;88:293-7.
[54] Pollock B, Garces Y, Stafford S, et al. Stereotactic radiosurgery for cavernous malformations. J Neurosurg 2000;93:987-91.
[55] Requena I, Arias M, Lopez Ibor L, et al. Cavernomas of the central nervous system: clinical and neuroimaging manifestations in 47 patients. J Neurol Neurosurg Psychiatry 1991;54:590-594
[56] Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency for electronic publication, version 9.2a April 2008