Embed Size (px)
Citation preview
1616Nutrition in
Metabolic andRespiratory
Stress
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Introduction
• Metabolic stress– Disruption in the body’s chemical environment
due to the effects of disease or injury• Respiratory stress
– Characterized by inadequate oxygen and excessive carbon dioxide in the blood and tissues
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
The Body’s Responses to Stress and Injury
• Stress response– Body’s nonspecific response to a variety of
stressors• Energy nutrients mobilized from storage• Heart rate and respiration (breathing rate) increase• Blood pressure rises• Energy diverted from processes that are not life
sustaining
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
The Body’s Responses to Stress and Injury (cont’d.)
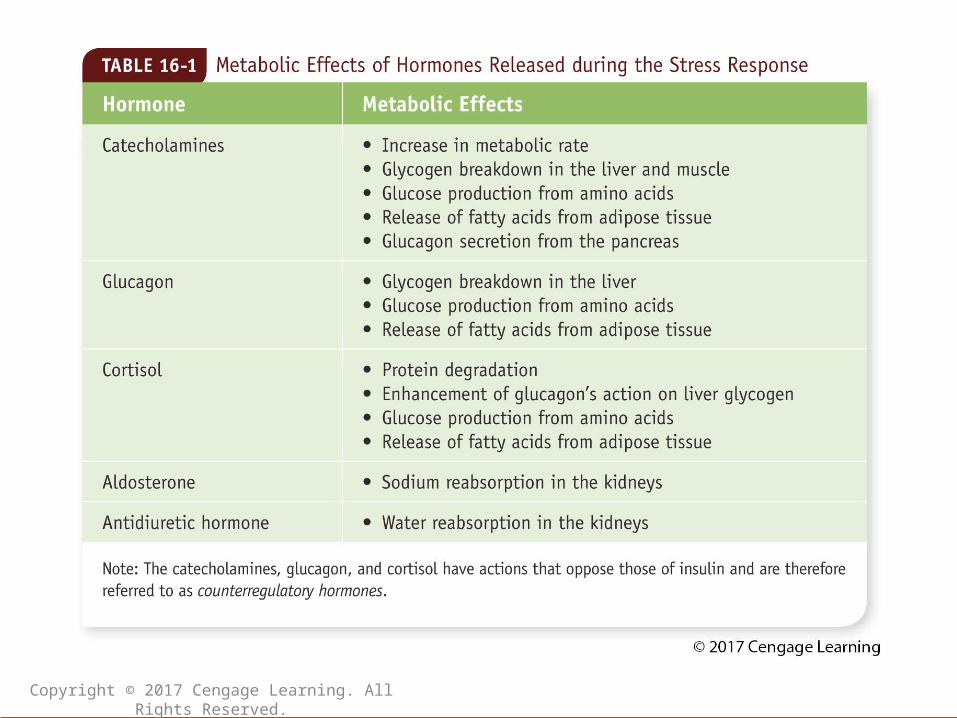
• Hormonal responses to stress– Hormones released into the blood soon after
an injury occurs– Catecholamines
• Fight-or-flight hormones: epinephrine and norepinephrine
– Glucagon• Causes release of nutrients from storage
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
The Body’s Responses to Stress and Injury (cont’d.)
• Hormonal responses to stress– Cortisol
• Enhances muscle protein degradation• Prolonged exposure impairs wound healing,
promotes insulin resistance– Aldosterone
• Stimulates kidneys to reabsorb more sodium– Antidiuretic hormone
• Stimulates kidneys to reabsorb more water
Copyright © 2017 Cengage Learning. All Rights Reserved.
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
The Body’s Responses to Stress and Injury (cont’d.)
• The inflammatory response– Immune system’s nonspecific response to
infection or tissue injury– Functions
• Contains and destroys infectious agents (and their products)
• Prevents further tissue damage– What are classic signs of inflammation?
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
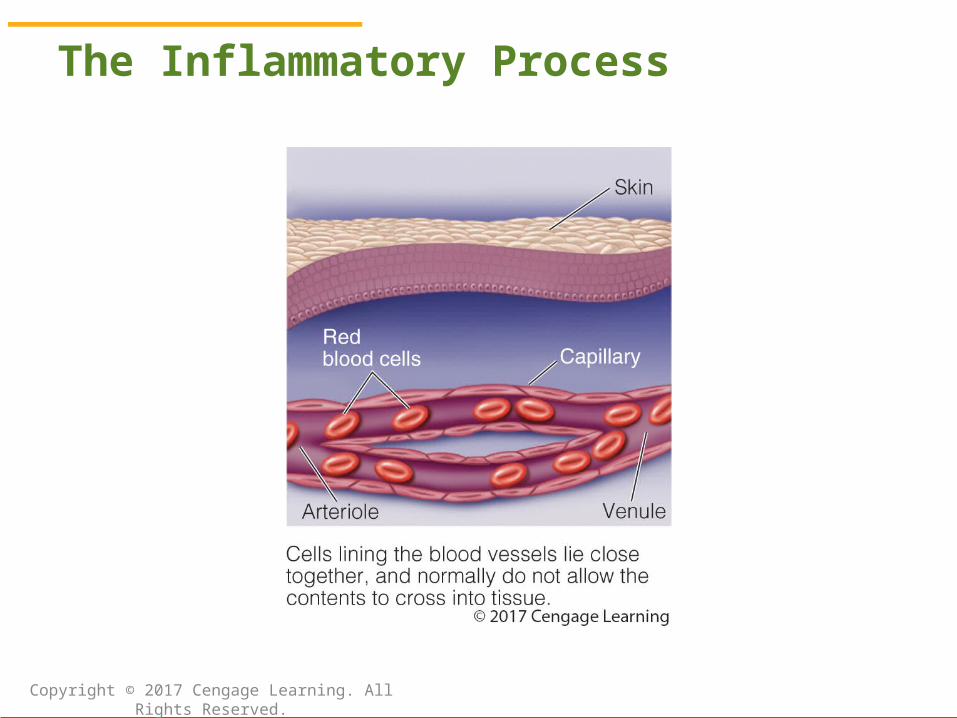
The Inflammatory Process
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
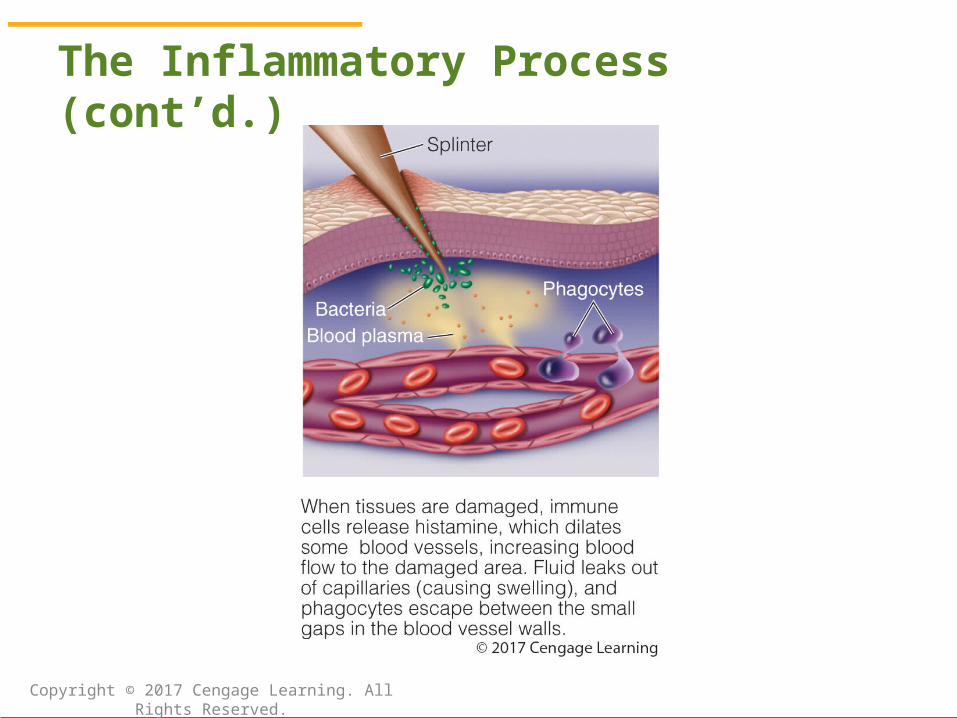
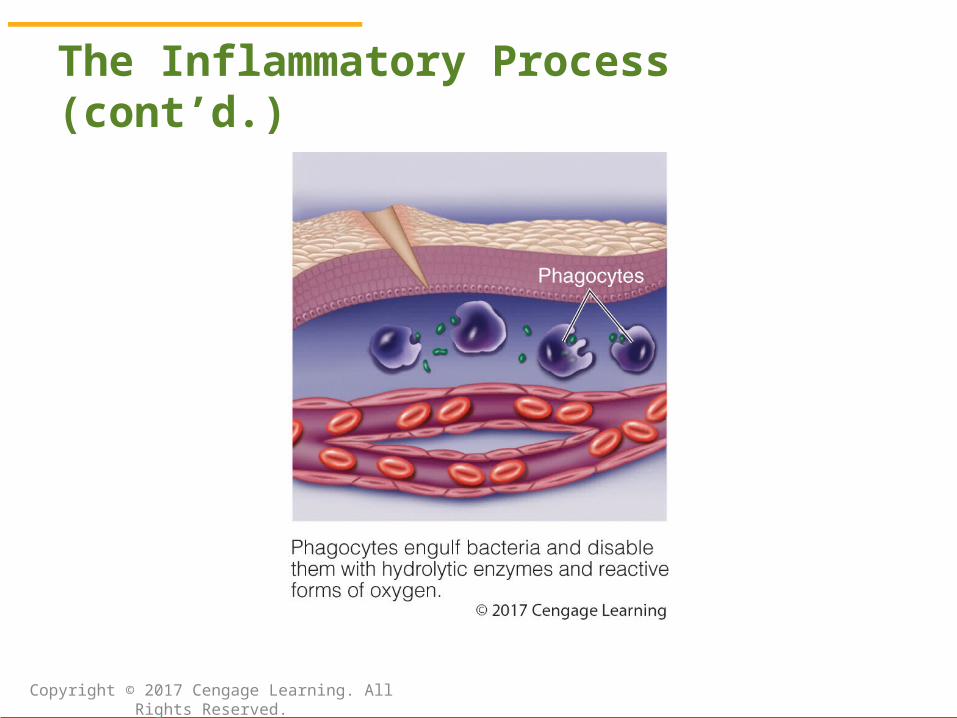
The Inflammatory Process (cont’d.)
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
The Inflammatory Process (cont’d.)
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Responses to Stress and Injury: The Inflammatory Response (cont’d.)
• Mediators of inflammation: regulate the inflammatory process– Histamine: released from granules within mast
cells, causing vasodilation and capillary permeability
– Cytokines: produced by white blood cells (and some other types of cells)
– Eicosanoids: derived from dietary fatty acids
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Responses to Stress and Injury: The Inflammatory Response (cont’d.)
• Systemic effects of inflammation: acute-phase response– Liver increases production of acute-phase
proteins (C-reactive protein, complement, hepcidin, fibrinogen, prothrombin, etc.)
– Plasma concentrations of albumin, iron, and zinc levels fall
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Responses to Stress and Injury: The Inflammatory Response (cont’d.)
• Systemic effects of inflammation– Muscle catabolism makes amino acids
available for glucose production, tissue repair, immune protein synthesis
– Systemic inflammatory response syndrome (SIRS): raised heart and respiratory rates, abnormal white blood cell counts, and fever
– What is the condition known as shock?
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress
• Initial treatments– Administer intravenous solutions– Treat infections, repair wounds, drain
abscesses, and remove dead tissue (debridement)
• Following stabilization– Provide nutrition assessment and therapy
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress (cont’d.)
• Determining nutritional requirements– Principle goals of nutrition therapy
• Preserve lean (muscle) tissue• Maintain immune defenses• Promote healing
– What are complicating factors in assessing the nutritional needs of an acutely stressed patient?
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress: Determining Nutritional Requirements (cont’d.)• Estimating energy needs in acute stress
– Indirect calorimetry (critically ill patients)– Multiply estimated resting metabolic rate
(RMR) by a stress factor (Box 16-6)– Equations with built-in stress factors (Table
16-2)– Multiply body weight by appropriate factor
• Critical care: 25-30 kcal/kg• Hypocaloric feedings (obese pt.): 11-14 kcal/kg
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress: Determining Nutritional Requirements (cont’d.)• Protein requirements in acute stress
– Nonobese critically ill patients: 1.2 to 2.0 grams per kilogram body weight per day
– Obese patients given hypocaloric feedings: 2.0 to 2.5 grams per kilogram ideal body weight per day
– Glutamine and/or arginine supplementation may benefit some patient populations
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress: Determining Nutritional Requirements (cont’d.)• Carbohydrate and fat intakes in acute
stress– Carbohydrates: generally 50% to 60% of total
energy requirements– Patients with severe hyperglycemia: fat may
supply up to 50% of kcalories• Micronutrient needs in acute stress
– Specific requirements remain unknown but thought to be increased
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition Treatment of Acute Stress (cont’d.)
• Approaches to nutrition care in acute stress– Initial care: simple intravenous solutions– Enteral feedings or parenteral feedings may
be required– Transition to oral feedings
• High-kcal, high-protein diet often prescribed• Take care to avoid overfeeding• Oral supplements often provided
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
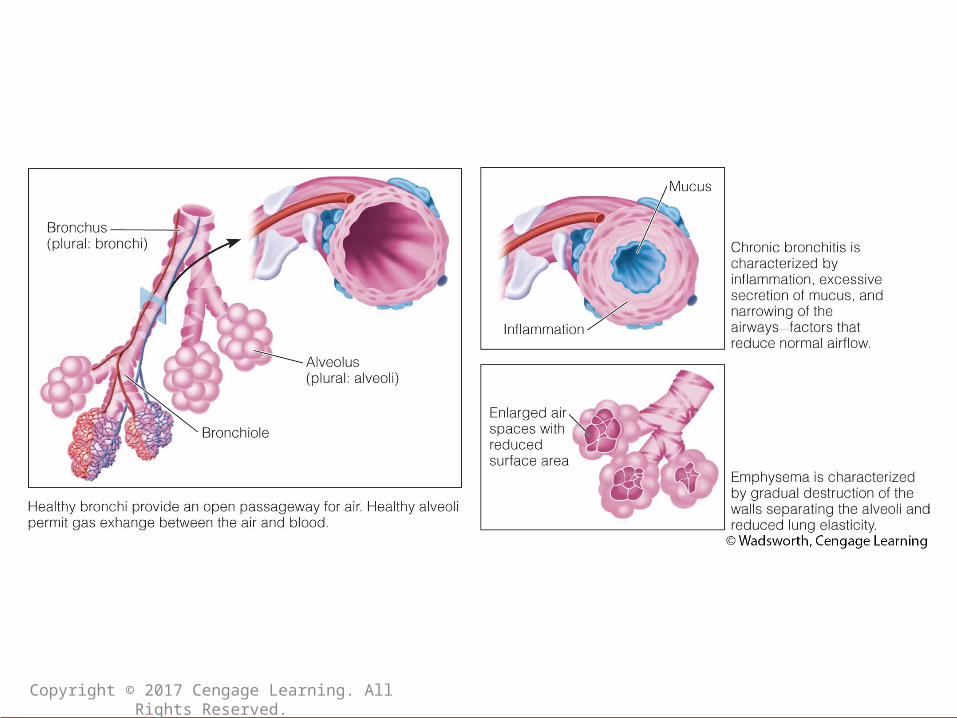
Nutrition and Respiratory Stress
• Chronic obstructive pulmonary disease (COPD)– Conditions characterized by the persistent
obstruction of airflow through the lungs– Main categories:
• Chronic bronchitis: persistent inflammation and excessive mucus secretions in airways
• Emphysema: breakdown of elastic structure and destruction of walls of bronchioles and alveoli
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
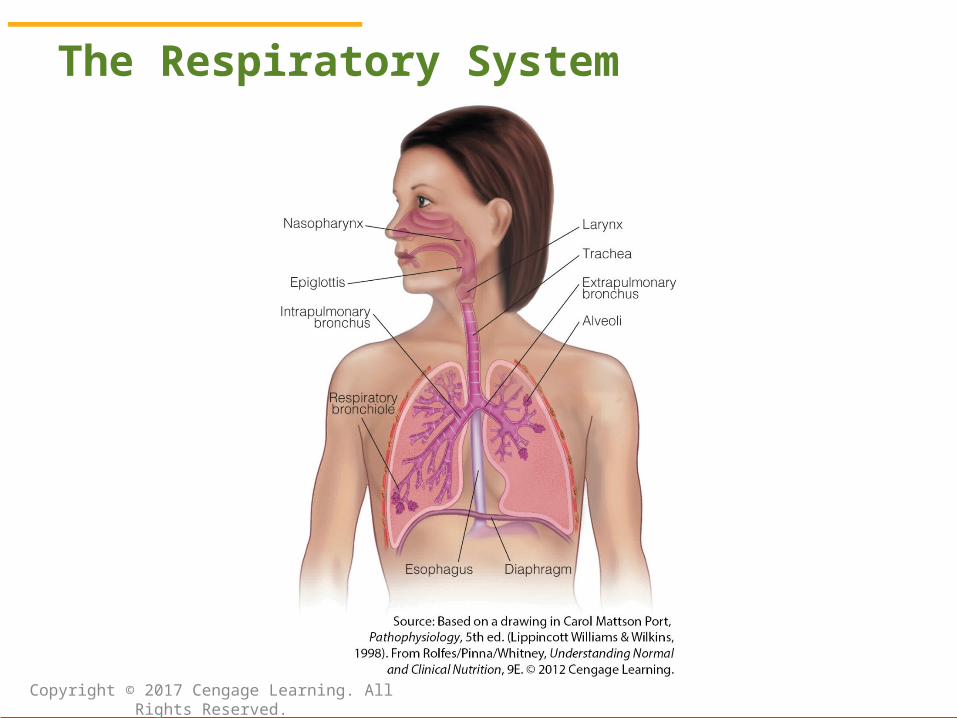
The Respiratory System
Copyright © 2017 Cengage Learning. All Rights Reserved.
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: COPD (cont’d.)
• Associated with abnormal levels of oxygen and carbon dioxide in the blood
• Shortness of breath (dyspnea)• May lead to respiratory or heart failure• Causes of COPD
– Primary risk factor: smoking– Exposure to pollutants– Genetic factors
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: COPD (cont’d.)
• Treatment of COPD– Primary objectives
• Prevent the disease from progressing• Relieve major symptoms (dyspnea and coughing)
– Recommendations• Quit smoking• Obtain flu and pneumonia vaccinations
– Bronchodilators, corticosteroids; supplemental oxygen therapy in severe cases
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: COPD (cont’d.)
• Nutrition therapy for COPD– Main goals
• Correct malnutrition• Promote the maintenance of a healthy body weight• Prevent muscle wasting
– Main focus of the nutrition care plan: usually, encouraging adequate food intake
• Small, frequent meals; adequate fluids in between• Excessive energy intakes increase CO2 production
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: COPD (cont’d.)
• Pulmonary formulas– More kcalories from fat and fewer from
carbohydrate• Incorporating an exercise program
– Prevent or reverse muscle loss– Aerobic training and resistance exercise– May need to increase activity gradually over 4
to 6 weeks
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress (cont’d.)
• Respiratory failure– Potentially life-threatening condition
• Impaired gas exchange between the air and circulating blood
• Abnormal levels of tissue gases– What are possible causes of respiratory
failure?– Acute respiratory distress syndrome (ARDS)
• Requires emergency care
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: Respiratory Failure (cont’d.)
• Consequences of respiratory failure– Severe hypoxemia: low O2 in blood
– Hypercapnia: excessive CO2 in blood
– Hypoxia: low O2 in tissues– Acidosis: acid accumulation in tissues– Cyanosis: bluish cast in the skin– Headache, confusion, and drowsiness– Heart arrhythmias and, ultimately, coma
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: Respiratory Failure (cont’d.)
• Treatment of respiratory failure– Focuses on supporting lung function and
correcting underlying disorder– Treatment plans vary considerably
• Oxygen therapy via face mask or nasal tubing• Mechanical ventilation• Diuretics• Other medications
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: Respiratory Failure (cont’d.)
• Nutrition therapy for respiratory failure– Energy needs
• Indirect calorimetry or predictive equations• Avoid overfeeding (can increase CO2)
– Protein needs• Mild or moderate lung injury: 1.0 to 1.5 g/kg/day• ARDS patients: 1.5 to 2 g/kg/day
– Fluids: monitored to prevent imbalances
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition and Respiratory Stress: Respiratory Failure (cont’d.)
• Nutrition support in respiratory failure– Indication: patient unable to eat meals– Enteral feedings
• Intestinal feedings may be preferred over gastric feedings to reduce aspiration risk
– Parenteral nutrition support• May be considered when aspiration risk is high
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition in Practice: Multiple Organ Dysfunction Syndrome (MODS)
• MODS: progressive dysfunction of 2 or more organ systems– Results when shock causes organ failure– Typically first lungs, then heart, liver, kidneys,
and GI tract• Risk factors: age, severe SIRS, infection,
blood transfusions
Copyright © 2017 Cengage Learning. All Rights Reserved.
© Cengage Learning 2017
Nutrition in Practice: Multiple Organ Dysfunction Syndrome (MODS)
• Treatment– Lung support– Fluid resuscitation– Support of heart and blood vessel function– Kidney support– Protection against infection– Nutrition support
• Prevention: mitigate organ stress
Copyright © 2017 Cengage Learning. All Rights Reserved.