Embed Size (px)
Citation preview
Paul Tobin-O'Brien 2013
Dementia Awareness and
EducationInforming on Dementia and Person
Centred Care Practice
Paul Tobin-O'Brien 2013
Created and presented by
Paul Tobin-O’Brien BSoc.Sc. Dip HE (nursing studies),
RGN Associate Tutor Comfort Keepers
(training) Ireland
Paul Tobin-OBrien 2013
“ME”There are still many things I can do like, walking, smiling, crying, laughing, speaking my way. I am here and I hear you speak, I have not yet gone
My mind might be slowly ebbing away but deep down I know I am still Mary. You see the changes in me I do not. I have not yet gone
I know the time will come when I will not remember your name but please remind me even if only for a few seconds I can say it back to you. I have not yet gone
When words fail me I strike out. I do not mean to hurt you. I still have feelings but these feelings I cannot put into words. I have not yet gone
Actions speak louder than words. Your help keeps me going. I have not yet gone
Where have you gone? I know not where. When I call you, you do not answer Where am I? I am not sure but in my world I feel secure. I have not yet gone
I love your smile, your name is gone. I know your face and feel at peace. I have not yet gone(Margaret Mackinlay)
Paul Tobin-OBrien 2013
Dementia is an umbrella term used to describe diseases that cause the loss of nerve cells in the human brain. These impact on the ability of a Person with dementia to function as they would normally do in their daily lives.
What is Dementia?
Paul Tobin-OBrien 2013
“Dementia is the decline in memory and other cognitive functions in comparison with the patient’s previous level of function as determined by a history of decline in performance and by abnormalities noted from clinical examination and neuropsychological tests. A diagnosis of dementia cannot be made when consciousness is impaired or when other clinical abnormalities prevent adequate evaluation of mental state. Dementia is a diagnosis based on behaviour and cannot be determined by brain scan, EEG or other laboratory instruments, although specific causes of dementia may be identified by these means”(McKhann in Kitwood (2002) p21)
Paul Tobin-OBrien 2013
5% of all persons over 65 years of age have some form of dementia
85years and older age group this rises to 20%
conservative estimate suggests that over 30,000 people in Ireland have dementia.
2020 this figure could be as high as 50,000.
How common is Dementia:
Paul Tobin-OBrien 2013
“The basic cause of dementia is damage to the nerve cells in the brain” (Graham. N., Warner. J. Alzheimer’s Disease and other Dementias, BMA)
Cause of Dementia
Paul Tobin-OBrien 2013
Alzheimer’s disease Vascular Dementia Lewy body dementia Frontotemporal Dementia These are the most common of hundreds of
forms/types of Dementia
Types of Dementia
Paul Tobin-OBrien 2013
Memory loss (short term ) Behaviour changes Depression Confusion Complex thinking (decision making) Ability to care for themselves Uninhibited behaviour
Common Symptoms
Paul Tobin-OBrien 2013
Most common of the dementias Slightly more common in women that in men Affects over 26 million people worldwide Over 90% of people with Alzheimer’s are
over 70 years of age Slow start with very mild symptoms initially Memory often affected first Smooth progression often over many years People often live 10 years or more after
diagnosis
Alzheimer’s Disease
Paul Tobin-OBrien 2013
Second most common cause of dementia Slightly more common in men that in
women Poor blood supply to the brain Often has a sudden start and gets worse in
steps
Vascular Dementia
Paul Tobin-OBrien 2013
Third most common cause of dementia More common in men Fluctuating confusion(often with spells
where they seem normal especially early on)
Features include symptoms of Parkinson’s disease and visual hallucinations
Risk of falls and poor mobility
Lewy body dementia
Paul Tobin-OBrien 2013
About 1 in 50 people with dementia have Frontotemporal dementia
tend to be younger usually around 50 years behaviour includes aggression, lack of
concentration, and loss of speech (finding right words).
Memory is affected late in the progress of the disease, and may appear normal in the early stages.
Some forms of this dementia are genetically inherited.
Frontotemporal Lobe
Paul Tobin-OBrien 2013
Depression Underactive thyroid gland Parkinson’s disease Acute confusion (delirium) Some vitamin deficiencies (e.g. vitamin
B12) Some infections (e.g. Syphilis) Rarely brain tumour
(Graham. N. p30)
Pseudo dementia

Paul Tobin-OBrien 2013
no known cure for Dementia
Paul Tobin-OBrien 2013
Group of drugs known as cholinesterase inhibitors, there are three drugs in this group currently in use
Donepezil (Aricept) Rivastigmine (Exelon) Galantamine (Reminyl)
Medical interventions
Paul Tobin-OBrien 2013
These drugs do not stop the disease from progressing or make people completely better.
Paul Tobin-OBrien 2013
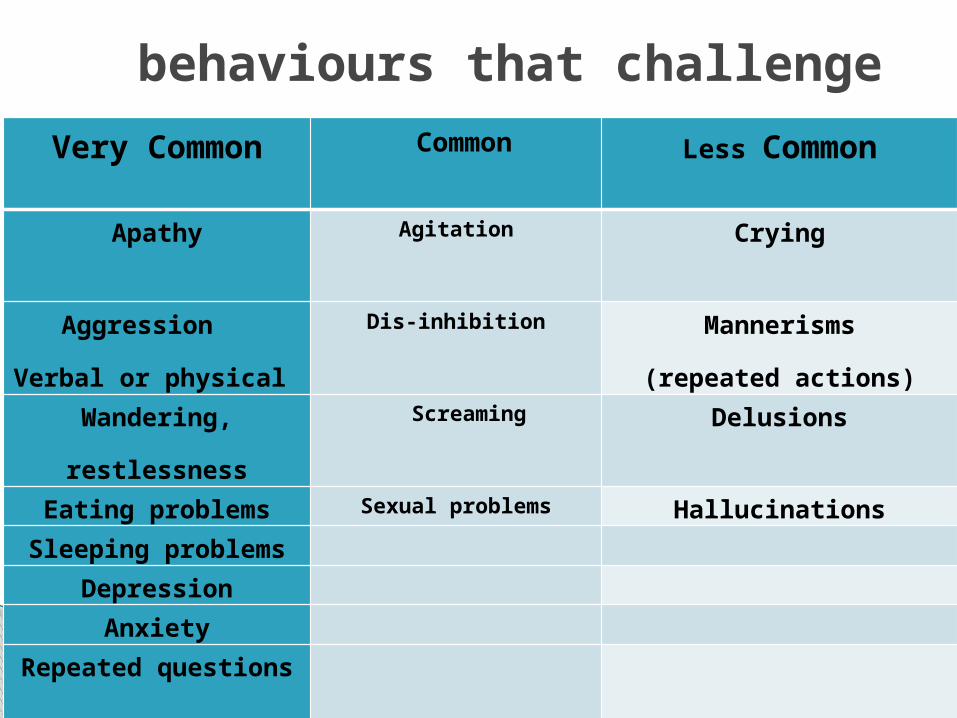
behaviours that challenge Very Common Common Less Common
Apathy Agitation Crying
Aggression
Verbal or physical
Dis-inhibition Mannerisms
(repeated actions)
Wandering,
restlessness
Screaming Delusions
Eating problems Sexual problems HallucinationsSleeping problems
Depression
Anxiety
Repeated questions
Paul Tobin-O'Brien 2013
Validation: A communication therapy. Reality orientation Reminiscence: Music therapy Aromatherapy: Diversion
Interventions/Therapies
Paul Tobin-O'Brien 2013
Assess, Plan Implement Evaluate Record all changes that occur in the condition of
the Person with dementia.
Carer’s role
Paul Tobin-O'Brien 2013
PersonWith
DementiaIs at the centre of the care you are
providing.
Learn about the Person
Remember
Paul Tobin-O'Brien 2013
Environment Safety Forgetfulness Interpersonal Communications Avoid confrontation
Be Aware of
Paul Tobin-O'Brien 2013
Take deep breaths before reacting to an episode, stepping back to allow the patient or family member space. If the patient is extremely agitated, you may need to exit the room for a few minutes until he/she has calmed down.
Remain calm and do not argue with the patient. Try to reassure him/her or distract her from the issue at hand.
Offer aid to the patient without appearing to take over the situation. Direct him in small steps, using simple words and allowing them plenty of time to perform the needed action. Offer praise and encouragement.
Guidelines Behaviour that Challenges
Paul Tobin-O'Brien 2013
Reduce any demands that are unnecessarily placed upon the patient, rearranging his/her day into a more stress-free routine that he/she will be better able to cope with.
If the patient becomes physically violent, move away from him/her and leave the area; do not attempt to restrain him/her unless it is absolutely necessary for his own safety. Seek the aid of an additional helper, if possible.
Analyse, with the patient, what triggers the episodes and try to minimise these types of situations in the future.
Paul Tobin-O'Brien 2013
Mrs A was a very well respected lady in her local community. She was a founder member of meals on wheels and supported other services for older people in her area. She was regarded as a refined and well-spoken person, well dressed and mannerly. She had been living alone for a number of years since her husband had passed on. She had no children and no known relatives in the area. In her late 70’s she developed Dementia and as it progressed she began to lose her independence. Neighbours and friends began to notice that she was becoming dishevelled and had been seen wandering outside her house at odd times of the night and very early in the morning. Previous colleagues decided that some sort of intervention was required and put in place an informal system of care for her. These interventions included some of her friends visiting her and helping to take care of her appearance by providing personal care such as bathing, dressing and grooming. As her condition progressed it was found that she began to swear at anyone who was trying to help her and became very aggressive. This behaviour led to fewer and fewer friends and former colleagues becoming available to attend to her. They decided to get in some professional help and arranged for a home care company to provide care for Mrs A in her
Case Study
Paul Tobin-O'Brien 2013
1. Dementia is a normal consequence of ageing2. If you get dementia, nothing can be done about it3. Alzheimer’s disease is a common cause of dementia4. Memory problems are just part of getting old5. Most people with dementia live in the developing
world6. Alzheimer’s disease usually runs in families7. There are Drugs available to treat dementia8. The best way to treat dementia is the bio-medical
method9. The person is lost who has dementia10. Dementia is curable
Dementia Quiz
Paul Tobin-O'Brien 2013
Questions ?Thank You
Paul Tobin-O'Brien 2013
Dementia is not part of the Ageing Process
Who is the behaviour challenging to?
Without a comprehensive history to create a personal care profile an intervention to alleviate behaviours that challenge may never be found
Treat each person with dementia as unique.
Remember
Paul Tobin-O'Brien 2013
There is no one treatment or intervention that works for everyone
Effective communication is essential to ensure that all care that is given to the Person is continuous and effective. This includes communication with the person, with colleagues, family members and other members of the multidisciplinary team.