Embed Size (px)
DESCRIPTION
embryology
Citation preview

Development
of the
Stomach

• Stomach develops from distal part of foregut. • It is initially a simple tubular midline structure. • Around the middle of the fourth week, a slight
dilation indicates the site of the future stomach. It first appears as a fusiform enlargement of the caudal part of the foregut.
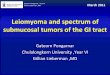
• This primordium soon enlarges and broadens dorsally. This is due to differential growth on dorsal side. During the next 2 weeks the dorsal border of the primitive stomach grows faster than its ventral border; this demarcates the greater curvature of the stomach.

Lateral view of developing stomach in successive stages showing differential growth dorsally.

Rotation of the developing stomach
• During development the developing stomach rotates along two axes.
• These rotations determine the final position of stomach in left hypochondrium.

First rotation
• 90 degrees clockwise Differential growth
• original left side becomes ventral surface • original right side becomes dorsal surface.

Second rotation anterior-posterior axis
• Before rotation, the cranial and caudal ends of the stomach are in the median plane.
• After rotation, the stomach assumes its final position with its long axis almost transverse to the long axis of the body.

Mesenteries of the stomach
• The stomach is suspended from the dorsal wall of the abdominal cavity by a dorsal mesentery called dorsal mesogastrium. This mesentery is originally very thick and lies in the median plane. Later on it is shifted to left side due to rotation of stomach.
• A ventral mesentery called ventral mesogastrium attaches the stomach with anterior abdominal wall. It is in fact septum transversum.

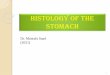
Transverse section of abdominal cavity of a developing embryo in 4th week at the level of stomach.

• Isolated clefts or spaces develop in the mesenchyme forming the thick dorsal mesogastrium during fourth week of embryonic period. The clefts soon coalesce to form a single cavity called omental bursa or lesser sac.

• Later on as the stomach rotates along longitudinal axis, dorsal mesogastrium is carried to the left thereby enlarging the bursa. Now there is a large recess of the peritoneal cavity behind stomach. The omental bursa expands transversely and cranially and soon lies between the stomach and the posterior abdominal wall. This pouch like bursa (L., purse) facilitates movements of the stomach).
• At this stage, omental bursa is related anteriorly to stomach and posteriorly to posterior abdominal wall. Its left lateral boundary is dorsal mesogastrium. It is wide open on to the right side.

• Development of lesser sac or omental bursa. Successive stages

• The primordium of spleen appears in 5th week of development as a mesodermal proliferation between the two leaves of dorsal mesogastrium.
• As the omental bursa expands and swings to the left side, a portion of dorsal mesogastrium behind spleen fuses with the peritoneum of posterior abdominal wall.
• The fused layers are absorbed and disappear.

• Thus the tail of pancreas becomes retroperitoneal.
• Remember that pancreas develops in dorsal mesoduodenum, but later on its tail expands into dorsal mesogastrium.


• Spleen maintains its intraperitoneal position.
• It is connected with dorsal body wall in the region of left kidney by lienorenal ligament (Lien L., spleen) and to stomach by gastrosplenic ligament.
• These two ligaments are nothing but parts of dorsal mesogastrium.

• Later on as stomach enlarges and rotates around anterio-posterior axis the dorsal mesogastrium forming the left wall of omental bursa is thrown downward.
• It grows enormously downward forming anterior and posterior layers of dorsal mesogastrium in front of transverse colon and small intestinal loops like an apron. Anterior layer is hanging down from greater curvature of stomach and posterior layer from posterior abdominal wall.
• The space between the two layers is called inferior recess of omental bursa.


• Later on these anterior and posterior layers fuse to form a single sheet hanging downward from greater curvature of stomach.
• The posterior layer also fuses with the mesentery of transverse colon.
• The fused apron of dorsal mesogastrium hanging downward from greater curvature of stomach is now called greater omentum (L., fat skin).

• This is a four-layered membrane. It overhangs the developing intestines.
• The inferior recess of omental bursa disappears as the anterior and posterior layers of greater omentum fuse.

• Ventral mesogastrium is actually septum transversum. It is between foregut and anterior abdominal wall. Later on the liver bud enters in septum transversum and the liver grows within septum transversum. As a result of the enormous growth of liver, the mesenchyme of septum transversum becomes stretched and membranous thus forming 1. falciform ligament, between anterior
abdominal wall and liver2. the peritoneal coving forming the false capsule of
liver 3. and lesser omentum between liver and
stomach/upper part of duodenum.


• The free margin of falciform ligament contains umbilical vein, which after birth is obliterated to form ligamentum teres hepatic.
• Lesser omentum between liver and stomach is called hepato-gastric ligament, while the part of lesser omentum between liver and duodenum is hepato-duodenal ligament.

• The free margin of lesser omentum between liver and duodenum contains bile duct, portal vein and hepatic artery. In adults the right border of lesser omentum forms the anterior boundary of epiploic foramen. Epiploic foramen is the connection between lesser sac and greater sac.

• Liver is completely covered by peritoneum forming the false capsule of liver. It is derived from the mesenchyme of septum transversum.
• Superiorly a triangular portion of liver is not covered by peritoneum. This triangular area is called the bare area of liver. It is covered by diaphragm. Here liver is attached to diaphragm by areolar tissue.
• Remember that diaphragm also develops from septum transversum.


• Stomach is supplied by
1. left gastric artery – a branch of celiac artery
2. right gastric artery – a branch of common hepatic artery – a branch of celiac artery
3. right gastro-epiploic – a branch of gastro-duodenal artery – a branch of common hepatic artery – a branch of celiac artery
4. left gastro-epiploic – a branch of splenic artery – a branch of celiac artery

Development of the
Duodenum

• Duodenum begins to develop in the early part of fourth week.
• It (epithelium) develops from caudal part of foregut and cranial part of midgut.
• All the other layers of duodenum are derived from surrounding splanchnic mesenchyme.
• The junction of the two parts of the duodenum is just distal to the origin of the liver diverticulum and in adult it is common bile duct.
• At this junction the ventral and dorsal pancreatic buds are also developing.

• Duodenum grows rapidly, forming a C-shaped loop ventrally.

• As stomach rotates 90 degrees in clockwise direction around its longitudinal axis to the left, duodenal loop rotates to the right.
• This rotation together with rapid growth of pancreas swings duodenum from its initial midline position to the right.

• Duodenum and pancreas are pressed against posterior abdominal wall. The right leaf of dorsal meso-duodenum fuses with parietal layer of peritoneum. The two layers subsequently disappear. Duodenum and pancreas become retroperitoneal structures.
• Mesoduodenum disappears entirely except in the region of pylorus of stomach, where a small portion of duodenum (duodenal cap) retains its mesentery and remains intraperitoneal.

• Transverse sections 5th and 7th week embryo

• During the fifth and sixth weeks, the lumen of duodenum becomes progressively smaller and is temporarily obliterated because of the proliferation of its epithelial cells. Normally vacuolization occurs because of degeneration of the epithelial cells. As a result, the duodenum normally becomes re-canalized by the end of the embryonic period. But sometimes the occlusion persists leading to duodenal stenosis.

• Because duodenum is developing from foregut and midgut, it is supplied by branches of celiac and superior mesenteric arteries. 1.right gastric - a branch of hepatic artery - a
branch of celiac trunk.
2.supra-duodenal – arises from either gastro-duodenal, hepatic artery, or right gastric artery. Gastro-duodenal and right gastric are branches of hepatic artery. Hepatic artery is branch of celiac trunk.

1. right gastro-epiploic - a branch of hepatic artery - a branch of celiac trunk.
2. superior pancreatico-duodenal - a branch of hepatic artery - a branch of celiac trunk.
3. inferior pancreatico-duodenal – a branch of superior mesenteric artery.