Embed Size (px)
DESCRIPTION
It is specially for nursing & allied health science.. hope it will be useful... Jaita
Citation preview

1
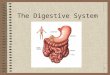
The Digestive System

• At the end of the class students will be able to:
- explain about the structure of alimentary tract
& it’s accessory organs of digestion
- explain about various alteration in diseases
- apply & implicate the knowledge in day to
day practice
Objective

• Digestive system = alimentary canal +
accessory organs + variety of digestive
processes.

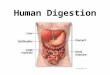
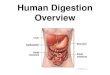
• Mouth
• Pharynx
• Oesophagus
• Stomach
• Small intestine
• Large intestine
• Rectum & Anal canal
Alimentary canal or Gastrointestinal (GI) tract

The Components of the Digestive System

• Glands situated out side of the tract; secretions pass through ducts to enter the tract:
- 3 pairs of salivary glands • Parotid in front of ear• Submandibular below lower jaw• Sublingual below tongue
- The pancreas- The liver & biliary tract
Accessory organs

7
The Major Salivary Glands

Duct System

• Ingestion:
• Propulsion:
• Digestion:
• Absorption:
• Elimination:
Digestive processes

General structures/ Layers of Digestive System

• Modified in different levels according to process
• Inner Epithelial layer/ Mucosa– Soft and pink in colour– 3 layers
Mucous membrane (innermost; columnar epithelium with goblet cells; protection, secretion, absorption)
Lamina propria (loose connective tissue; supports blood vessels & lymphoid tissue)
Muscularis mucosa (thin outer layer; smooth muscle)
– Secretion of enzyme and mucus

• Mucous membrane secrets digestive juices: saliva from the salivary glandsGastric juice from gastric glandsIntestinal juice from intestinal glandsPancreatic juice from pancreasBile from liver
• Also secrets mucus from goblet cells.
12

• Sub- mucosa
– Connective tissue (binds muscle layer to mucosa)
• Muscular layer
– Outer layer (Longitudinal muscles)
– Inner layer (Circular muscle)
Between these two layers: blood vessels, lymph vessels
& a plexus (network) of sympathetic&
parasympathetic nerves (myenteric plexus or
Auerbach’s plexus)
– Peristalsis (Segmental contraction)13

• Outer Serous layer or Adventitia
– Protective function
– In abdomen organs are covered by a serous membrane
(peritoneum)
Parietal peritoneum: lines the abdominal wall
Visceral peritoneum: covers the organs (viscera)
within the abdominal & pelvic cavities.
Home work: explain about peritoneum in detail.
14

15
Anatomy of the Mouth and Throat

Mouth or oral cavity
• Is bounded by muscles & bones:Anteriorly: by the lipsPosteriorly: continuous with oropharynxLaterally: by the muscles of the cheeksSuperiorly: by bony hard palate &
muscular soft palateInferiorly: by the muscular tongue &
soft tissues of the floor of the mouth
16

• Vestibule: part of mouth between gums & cheeks.
• Remainder of the cavity: oral cavity
• Palate: forms the roof of mouth; has 2 partsAnterior hard palate: formed by maxilla
& palatine bonePosterior soft palate: muscular curves
from back of hard palate & blends with the wall of pharynx at side.
17

• Uvula: curved fold of muscle covered with
mucous membrane, hanging down from
middle of free border of soft palate.
• Palatine tonsil: collection of lymphoid
tissue on each side between the arches.
18

19
Tongue

• Voluntary muscle structure
• Attached to hyoid bone at base
• Attached to floor of the mouth by a fold of its mucous membrane covering: frenulum
• Superior surface: numerous papillae (small projections); many of these contain sensory receptors (test buds)
20

Blood supply: lingual branch of external carotid
artery; venous drainage by lingual vein
Nerve supply: hypoglossal nerves (12th cranial
nerve)- supply voluntary muscles; lingual branch
of mandibular nerves (arises from 5th cranial
nerve)- pain, temperature & touch; facial &
glossopharyngeal nerves (7th & 9th cranial nerves)-
nerves of taste
21

Functions of tongue
• Chewing (mastication)
• Swallowing (deglutition)
• Speech
• Taste
22

23
Teeth

• Embedded in the alveoli or sockets of the
alveolar ridges of the mandible & the maxilla.
• Temporary or deciduous teeth: babies born
with two sets (dentitions)
• 20 temporary teeth (10 in each jaw); erupt at about 6 months; should be present by 24 months
• Permanent teeth begin to replace deciduous teeth in 6th year; 32 teeth; usually complete by 21st year
24

Functions of the teeth
• Incisors & canine teeth: cutting teeth; used for biting pieces of food
• Premolar & molar teeth: broad, flat surface; used for grinding or chewing food
25

Structure of tooth• Crown: part that protrudes from gum• Root: part embedded in bone• Neck: narrowed region between crown
& root.• Blood supply: maxillary artery;
jugular veins• Nerve supply: upper teeth maxillary
nerves; lower teeth mandibular nerves. Both are branches of trigeminal nerves (5th cranial nerve)
26

Salivary glands
27

Parotid glands
• Each side of the face just below the external acoustic meatus.
• Each gland has a parotid duct opening in mouth at the level of 2nd upper molar tooth.
28

Sub- mandibular glands
• One on each side of face under angle of jaw.
• 2 submandibular ducts open on the floor of the mouth (each side of the frenulum of tongue)
29

Sublingual glands
• Lie under the mucus membrane of the floor of mouth in front of submandibular glands
• Have numerous small ducts that open into the floor of mouth
30

Salivary Glands
• Produce and secrete saliva that: – Cleanses the mouth– Moistens and dissolves food chemicals – Aids in bolus formation– Chemical digestion of Food

Saliva
• 1-1.5 litre/day; pH slightly acidic (6.8)
Composition• Mostly water 97 to 99.5% • Mucus• Mineral salts• A digestive enzyme: salivary amylase• Lysozyme• Immunoglobulin• Blood clotting factors

Secretion of saliva
• Secretion is under autonomic nervous system
• Parasympathetic stimulation causes: profuse
secretion of watery saliva with a relatively low content
of enzymes & other organic substances
• Sympathetic stimulation causes: secretion in small
amount of saliva rich in organic materials specially
from sub mandibular glands
33

Functions of saliva
• Chemical digestion of polysaccharidesSaliva contains enzyme amylase: break down
of complex sugars (starch to disaccharide maltose)
• Lubrication of food made a bolus ready for swallowing
• Cleaning & lubricating the mouth prevents damage to mucous membrane by
rough & abrasive food
34

• Non- specific defence lysozyme, immunoglobulin & clotting factors
combat invading microbes
• Taste test buds are stimulated only by chemical
substances; thus dry foods only stimulate the sense of taste after thorough mixing with saliva
35

Pharynx
• Connects nasal and oral cavities with larynx & oesophagus
• force food down during swallowing• DivisionsNasopharynx (important in respiration) Oropharynx & Laryngopharynx
(both are common passage to both respiratory & digestive system)

37

• Blood supply: several branches of facial arteries; venous drainage: into facial veins & internal jugular veins
• Nerve supply: sympathetic from cervical ganglia; parasympathetic by glossopharyngeal & vagus nerves
38

Oesophagus

40
Esophagus
– 25cm long muscular tube; 2cm diameter– From pharynx to stomach– Behind trachea and in front of vertebral
column– Food passes to stomach by active muscular
action– As it passed through diaphragm it curves
upward: prevents regurgitation (backflow) of gastric content

Oesophagus contd.– Closed with two sphincters
(upper: cricopharyngeal or upper oesophageal sphincter;
lower: cardiac or lower oesophageal sphincter)– Solid food reaches stomach in 7 to 8 seconds– Liquids reaches stomach in 2 to 3 seconds
• Functions– Secrete mucous– Transport food
41

• Blood supply:
- Thoracic region- paired oesophageal arteries; venous drainage: azygous & hemizygous veins
- Abdominal region- branches from inferior phrenic arteries & left gastric branch of coeliac artery; Venous drainage in left gastric vein
42

43
Anatomy of the Stomach

44
Stomach• Usually “J” shaped; 1.5lt or more in adult• 2 sphincters: cardiac & pyloric

Organs associated with stomach• Anteriorly: left lobe of liver &
abdominal wall
• Posteriorly: abdominal aorta, pancreas, spleen, left kidney & adrenal gland
• Superiorly: diaphragm, oesophagus & left lobe of liver
• Inferiorly: transverse colon & small intestine
• To the left: diaphragm & spleen
• To the right: liver & duodenum
45

Walls of stomach• Consists of 3 layers instead of 2.
Outer: longitudinal fibresMiddle: circular fibresInner: oblique fibres
• This arrangement allows churning motion as well as peristaltic movement.
• Circular muscle is strongest in the pylorus & pyloric sphincter
46

• Mucosa of stomach: When empty: thrown into longitudinal folds
or rugaeWhen full: rugae are ironed out & surface has
a smooth, velvety appearance.Numerous gastric glands situated below
mucous membrane & open on to it: secrets gastric juice
47

• Mucous membrane– G cells – secret gastrin– Goblet cells – secret mucous– Gastric pit has Oxyntic gland – Parietal
cells – secret HCl– Chief cells or Zymogenic cells
• Pepsin• Gastric lipase
48

Histology of Stomach

• Blood supply: Arterial supply: left gastric artery, a branch
of coeliac artery, right gastric artery & gastroepiploic arteries.
Venous drainage: through veins of corresponding names into the portal vein
50

Gastric juice
• About 2 lt of gastric juice/ day• Consist of:
Water (by gastric glands)Mineral salts (by gastric glands)Mucus (mucous cells)HCL (parietal cells)Intrinsic factor (parietal cells)Inactive enzyme precursors: pepsinogen by chief
cells
51

Functions of gastric juice
• Water further liquefies the food swallowed
• HCL:Acidifies the food & stops action of salivary
amylaseKills ingested microbesProvides acid environment needed for
effective digestion by pepsins
52

• Pepsinogens: are activated to pepsins by HCL acid &
pepsins already present in the stomachThese enzymes begin the digestion of
proteins.Pepsins are more effective at a very low pH
(1.5-3.5)
53

• Intrinsic factor (a protein): needed for absorption of vit B12 from ileum
• Mucus: prevents mechanical injury to the stomach
wall by lubricating the contentsPrevents chemical injury by acting as a barrier
between stomach wall & corrosive gastric juice
54

Secretion of gastric juice
• Always a small quantity of gastric juice present in the stomach (even if no food) = “fasting juice”
• Max. level: about 1 hr after a meal• Declines to fasting level after about 4 hrs.• 3 phases of secretion of gastric juice
Cephalic phaseGastric phaseIntestinal phase
55

Cephalic Phase

Cephalic phase
• This flow of juice occurs before food reaches the stomach
• Due to reflex stimulation of vagus (parasympathetic) nerves initiated by the sight, smell or test of food.
57

Gastric phase
58
stimulated by the presence of food the in the pyloric antrum
duodenum secret gastrin (circulating in blood)
blood which supplies the stomach
stimulates the gastric glands to produce more gastric juice
Gastric phase secretion is suppressed when the pH in the pyloric antrum falls to about 1.5

Gastric Phase

Gastric Phase
• Distention of the stomach activates a parasympathetic reflex. Action potentials are carried by the vagus nerves to the medulla oblongata.
• Medulla oblongata stimulates further secretions of the stomach.
• Distention also stimulates local reflexes that amplify stomach secretions.

Intestinal Phase
• Chyme in the duodenum with a pH less than 2 or containing lipids inhibits gastric secretions by 3 mechanisms
1. Sensory input to the medulla from the duodenum inhibits the motor input from the medulla to the stomach. Stops secretion of pepsin and HCl.
2. Local reflexes inhibit gastric secretion
3. Secretin, gastric inhibitory polypeptide, and cholecystokinin produced by the duodenum inhibit gastric secretions in the stomach. (Enterogastrone)

Intestinal Phase

Intestinal phase
• When the partially digested contents of the stomach reach the small intestine, a hormone complex enterogastrone is produced which slows down the secretion of gastric juice & reduces gastric motility.
• Two hormones forming this complex are secretin & cholecystokinin (CCK)
• Enterogastrone (any hormone or combination of hormones released by the intestine that inhibits gastric secretion.)
63

• By slowing the emptying rate of the stomach, the contents of the duodenum become more thoroughly mixed with bile & pancreatic juice.
• This phase of gastric secretion is most marked when the meal has had a high fat content
64

65

66
Functions of Stomach
– Mix food– Reservoir– Mechanical digestion– Chemical digestion of
• Protein• Nucleic acids• Fats
– Activates some enzymes– Destroy some bacteria– Dissolving out iron from
food
– Limited absortion of• Alcohol
• Water
• B 12
– Storage of food for 3 hours
– Partial digestion of proteins and fats
– Outward movement of content of pyloric end of the stomach

67
Small Intestine• Extends from pyloric
sphincter ileocecal valve– 6 to 7 meter long, 2.5cm
diameter– Lies in center of
abdomen– Divided into 3 parts
• First part – Duodenum
• Second part – Jejunum
• Third part – ileum

68
Small Intestine• Alkaline Secretions
– Protects from acid contents of stomach
• Small intestine– Mucosa
• Deeply folded to increase the surface area (villi)
• Helps in absorption of food.
• Movements– Segmentation
– Peristalsis

Segmentation & Peristalsis
• Peristalsis: is a radially symmetrical contraction and relaxation of muscles which propagates in a wave down the muscular tube, in an anterograde fashion. In humans, peristalsis is found in the contraction of smooth muscles to propel contents through the digestive tract.
• Segmentation: Most areas of the small intestine and some portions of the large intestine undergo cycles of contraction that churn and fragment the bolus, mixing the contents with intestinal secretions

70
Peristalsis and Segmentation

71

Small Intestine cont.
• Structural modifications of the small intestine wall increase surface area– Plicae circulares: deep circular folds of the
mucosa and submucosa– Villi – fingerlike extensions of the mucosa– Microvilli – tiny projections of absorptive
mucosal cells’ plasma membranes

Small Intestine

74
Structure of the Villi in the Small Intestine

75
Small Intestine
• Requires pancreatic enzymes & bile to complete digestion
• Blood supply: Superior mesenteric artery; superior mesenteric vein

76
Large Intestine• Extends from ileocecal valve to anus
– 1.5meter long, 5 to 6cm diameter• Regions
– Cecum
– Colon: Divided into 3 parts• Right ascending colon
• Transverse colon
• Left descending colon
– Appendix (Epiploic appendages)
– Rectum
– Anal canal

Large Intestine• Cecum
– 1st part of large intestine, Blind sac, appendix attached
• Colon– Ascending, transverse, descending, sigmoid
• Rectum– Straight muscular tube, 13cm long, between
sigmoid colon & anal canal• Anal canal: 3.8cm long
– Internal anal sphincter (smooth muscle) – External anal sphincter (skeletal muscle)


79
Large Intestine
– No villi– No permanent circular folds– Longitudinal muscle is modified: collected
into 3 bands• Taeniae coli (Haustra)
– Otherwise like rest of Gl tract

Large intestine
• Blood supply:
- Inferior mesenteric artery, middle & inferior rectal arteries;
- Superior & inferior mesenteric vein
80

Functions of Large Intestine
• Absorption
• Microbial activity (large no. of microbes synthesize vitamin K & folic acid):E. coli, Streptococcus faecalis etc.
• Mass movement
• Defecation
81

82
Feces Formation and Defecation
• Sigmoid Colon & Rectum– Temporary storage of
faeces • Chyme dehydrated to
form feces• Feces composition
– Water– Inorganic salts– Epithelial cells– Bacteria– Byproducts of digestion
• Defecation– Peristalsis pushes feces
into rectum– Rectal walls stretch
• Control– Parasympathetic
– Voluntary

The Liver
• The largest gland in the body• Performs metabolic and hematological
regulation and produces bile• Location
– R. Hypochondrium– Epigastric region

Organs associated with liver
• Superiorly & anteriorly: diaphragm & anterior abdominal wall
• Inferiorly: stomach, bile ducts, duodenum, hepatic flexure of the colon, right kidney & adrenal gland
• Posteriorly: oesophagus, inferior vena cava, aorta, gall bladder, vertebral column, diaphragm
• Laterally: lower ribs & diaphragm
84

85
Liver• 4 Lobes
– Left – Quadrate– Caudate– Right

The Liver

• Each lobe has lobules (tiny functional units) – hexagonal in shape;
• Lobules contains hepatocytes: arranged in pairs of column
• Between 2 pairs of column of cells are sinusoids (blood vessels with incomplete walls – Feed into central vein (mix blood from portal vein & hepatic artery)
• Kupffer cells (Hepatic macrophages): within sinusoids; ingest & destroy worn out blood cells & any foreign particles present in blood
87



90
Liver
• Dual blood supply– Hepatic portal vein
– Hepatic artery/vein

Blood and Bile Flow

92
LiverFunctions•Carbohydrate, fat, protein metabolism•Synthesis of bile•Formation of urea•Detoxification of drugs, alcohol•Destruction of RBC•Storage of excess glucose in form of glycogen•Storage of Vitamin A & D•Storage of Hemoglobin•Activates vitamin D•Fetal RBC production•Phagocytosis•Manufacturing of prothrombin & fibrinogen

• Pale gray gland; (Both exocrine & endocrine gland)• In epigastric & left hypochondriac regions; posterior
to stomach• Weighing 60 gm; 12-15cm long• Parts of pancreas
– Broad Head (lies in curve of duodenum)– Body (behind the stomach)– Narrow Tail (infront of left kidney just reaches the
spleen)• Abdominal aorta & inferior vena cava lie behind
The Pancreas

Pancreas
94
Head
Body
Tail

• Endocrine functions– Groups of specialized cells (pancreatic islets of
Langerhans): have no ducts; hormones diffuse directly into blood.
– Secrets Insulin, Glucagon (controls blood glucose)
The Pancreas

• Exocrine functions
– Majority of pancreatic secretions– Consists of a large number of lobules made up
of small alveoli (walls consists of secretory cells)
– Each lobules is drained by tiny duct (unite to form pancreatic duct): joins with common bile duct (forms hepatopancreatic ampulla) & opens into duodenum
– Duodenal opening of ampulla is controlled by hepatopancreatic sphincter (sphincter of Oddi)
96

The Pancreas
– Produces pancreatic juice containing enzymes
– Pancreatic juice digests• Carbohydrate• Proteins• Fats


Pancreas
• Blood supply:
Arterial supply: splenic & mesenteric arteries;
Venous drainage: splenic & mesenteric veins joins to form portal vein
99

Biliary tract
• Consists of bile duct & gall bladder
100

Bile ducts
• Right & Left Hepatic ducts merge Common hepatic duct (7.5 cm long, 6mm diameter)
• Common hepatic duct joins Cystic duct from gallbladder Common Bile duct
• Bile duct joins Pancreatic duct at Hepatopancreatic ampulla and enters duodenum
• Hepatopancreatic sphincter regulates passage of bile and pancreatic juices into duodenum

102

• Hollow, pear-shaped sac; attached to posterior surface of liver
• Has a fundus (expanded end) & body (main part) & neck (continuous with cystic duct)
• Stores, modifies and concentrates bile• Releases bile via the cystic duct, which flows into the
bile duct• Blood supply:- Cystic artery (branch of hepatic artery)- Cystic vein (joins portal vein)
The Gallbladder

Functions of gall bladder
• Reservoir for bile
• Secretion of mucus into the bile
• Absorption of water so that it is 10-15 times more concentrated than liver bile
• Release of stored bile
104

Metabolism
• Carbohydrate
• Protein
• Fat
105

• Ingestion: taking food in GI tract (eating,
drinking)
• Propulsion: mixes & moves the contents
along GI tract.
Digestive processes

• Digestion: Mechanical breakdown of food
(mastication) & chemical digestion (by
enzymes of secretion produced by glands
& accessory organs.
Digestive processes cont.

• Absorption: digested food substances pass
through the walls of some organs of GI
tract into blood & lymph capillaries for
circulation &use by body cell
Digestive processes cont.

• Elimination: food substances which can
not be digested & absorbed excreted as
faeces by the process of defaecation.
Digestive processes cont.

The path of food:
oral cavity/teeth/salivary glands
oropharynx/epiglottis
oesophagus
stomach
small intestine: duodenum
small intestine: ileum
small intestine: jejunum
large intestine: ascending colon
large intestine: transverse colon
large intestine: descending colon
sigmoid colon rectum anus

Diseases of mouth
• Inflammation: thrush, angular cheilitis, gingivitis, stomatitis,
• Viral infection
• Tumors of mouth: squamous cell carcinoma
• Developmental defects: cleft palate & cleft lip
111

Diseases of pharynx
• Tonsillitis
• Diphtheria
112

Diseases of salivary glands
• Mumps
• Calculus formation
• tumors
113

Diseases of oesophagus
• Esophageal varices
• Inflammatory conditions
• Spontaneous rupture of oesophagus
• Tumors
• Congenital malformation
114

Diseases of the stomach
• Gastritis
• Peptic ulceration
• Tumors of stomach
• Congenital pyloric stenosis
115

Diseases of the intestine
• Appendicitis
• Microbial disease: typhoid fever, paratyphoid fever, infection, food poisoning, cholera, dysentery
• Inflammatory bowel disease: crohn’s disease, ulcerative colitis, tumors, hernias, intestinal obstruction etc
116

Diseases of pancreas
• Acute pancreatitis
• Chronic pancreatitis
• Tumors
117

Disease of liver
• Acute hepatitis
• Chronic hepatitis
• Non- viral inflammation of liver: liver abscess, cirrhosis of liver, liver faliure, hepatic encephalopathy, blood coagulation defect, ascites etc.
• Tumors of the liver
118

Disease of gall bladder & bile duct
• Gall stones (cholelithiasis)
• Tumors
• Jaundice
• Cholecystitis
119