Embed Size (px)
Citation preview

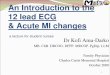
The ElectrocardiogramWhen activated, the heart is a concentrated locus of time-varying electrical potentials in the body. When a portion of the myocardium becomes depolarized from an action potential, its polarity is temporarily reversed, becoming positive on the inside and negative on the outside relative to neighboring inactivated tissue. When this reversal occurs, it temporarily creates two neighboring regions of opposite charge, or polarity, within the myocardium (Fig. 12.6). This difference in polarity between two locations is called a dipole. Electrical currents readily flow from one poll of a dipole to the other though any media between the poles that can conduct electrical current. The intracellular and extracellular fluids in the body are largely composed of electrolyte solution, which is a good conductor of electricity. For this reason, the heart can be thought of as a potential generator in a volume conductor. Consequently, any dipole formed at any time and in any direction within the myocardium between depolarized and nondepolarized regions is transmitted through the body as currents between the ends of the dipoles. These currents radiate outward through the body all the way to the surface of the skin.
An electrocardiogram, or ECG, is an amplified, timed recording of the electrical activity of the heart, as it is detected on the surface of the body. The recording gives a plot of voltage as a function of time. It results from the composite effect of all the different types of action potentials generated in the myocardium during activation and the resulting magnitude and orientation of the dipoles created. Although it is correct to say that the electrical activity in the heart is responsible for creating the ECG, the physician looks at this process in reverse; that is, the physician examines the ECG to create a picture of the electrical activity in the heart.
The electrocardiogram is one of the most useful diagnostic tools available in medicine to the physician, but it is important to understand what information can and cannot be gained from the analysis of an ECG. The ECG can be used to detect abnormalities in heart rhythm and conduction, myocardial ischemia and infarction, plasma electrolyte imbalances, and effects of numerous drugs. One can also gain information from the ECG about the anatomic orientation of the heart, the size of the atria and ventricles, and the path taken by action potentials through the heart during normal or abnormal activation (e.g., the average direction of activation of the ventricles). The ECG, however, cannot give direct information about the contractile performance of the heart, which is equally important in the evaluation of myocardial status in a clinical setting.
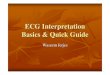
The Moment-to-Moment Orientation and Magnitude of Net Dipoles in the Heart Determine the Formation of the ElectrocardiogramThe formation of the standard wave forms within the ECG can be explained as arising from the orientation and magnitude of the net, or collective average, dipoles that are created throughout the heart during electrical activation of the myocardium. In explanation, consider the voltage changes produced in which the body serves as a volume conductor and the heart generates a collection of changing dipoles (Fig. 12.8). In this example, an electrocardiographic recorder is connected between points A and B such that when point A is positive relative to point B, the ECG is deflected upward, and when B is positive relative to A, a downward deflection results. The black arrows show (in two

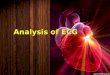
dimensions) the direction of the net dipole resulting from the many individual dipoles present at any one time. The lengths of the arrows are proportional to the magnitude (voltage) of the net dipole, which is related to the mass of myocardium generating the net dipole. The blue arrows show the magnitude of the dipole component that is parallel to the line between points A and B (the recorder electrodes); this component determines the amplitude and polarity of voltage that will be recorded on the ECG. Atrial excitation results from a wave of depolarization that originates in the SA node and spreads over the atria, as indicated in panel 1 of Figure 12.8. The net dipole generated by this excitation has a magnitude proportional to the mass of the atrial muscle involved and a direction indicated by the black arrow. The head of the arrow points toward the positive end of the dipole, where the atrial muscle is not yet depolarized. The negative end of the dipole is located at the tail of the arrow, where depolarization has already occurred. Point A, therefore, is positive relative to point B, and there will be an upward deflection of the ECG. The magnitude of this upward deflection depends on two factors: (1) it is proportional to the amount of tissue generating the dipole (the magnitude of the net dipole), and (2) it depends on the orientation of the dipole relative to a parallel line connecting points A and B. This latter relationship is demonstrated in Figure 12.9. For example, imagine a wave of depolarization traveling through the atria muscle as a sagittal plane, perpendicular to the ground, proceeding directly along the line connecting point B to point A. This wave of depolarization then is aimed directly at the positive pole A and will create a positive deflection as described above. For the sake of example only, we shall assign this deflection an amplitude of +4 mm on the ECG recorder. Should this same wave of depolarization, however, proceed from point A toward point B, the wave would be aimed directly at the negative pole, resulting in a 4-mm negative, or downward, deflection of the wave. The amplitude of the deflection will thus vary in this example between -4 mm and +4 mm, depending on the angle of the wave of depolarization relative to the line connecting A and B. Should the wave proceed toward A at a 45° angle, the deflection would be a positive 2 mm; if it proceeds at 90° (perpendicular) to the line connecting A and B, it would not be pointing at either pole and no deflection would be recorded on the ECG. The deflection will also register zero once the atria are completely depolarized, because no voltage difference will exist between A and B (i.e., no dipole exists).

Although the preceding discussion is an oversimplification, it presents the basic principles of dipole magnitude and orientation relative to two recording points that create the pattern of the common ECG. For example, after the P wave, the ECG returns to its baseline or isoelectric level. During this time, the wave of depolarization moves through the AV node, the AV bundle, the bundle branches, and the Purkinje system. The dipoles created by depolarization of these structures are too small to produce a deflection on the ECG. However, the depolarization of ventricular structures does create deflections on the ECG. The net dipole that results from the initial depolarization of the septum is shown in panel 2 of Figure 12.8. This depolarization is pointed toward point B and away from point A because the left side of the septum depolarizes before the right side. This orientation creates a small downward deflection produced on the ECG called the Q wave. The normal Q wave is often so small that it is not apparent. Next, the wave of depolarization spreads via the Purkinje system across the inside surface of the free walls of the ventricles. Depolarization of free-wall ventricular muscle proceeds from the innermost layers of muscle (subendocardium) to the outermost layers (subepicardium). Because the muscle mass of the left ventricle is much greater than that of the right ventricle, the net dipole during this phase has the direction indicated in panel 3. The deflection of the ECG is upward because the dipole is directed at point A and is large because of the great mass of tissue involved. This upward deflection is the R wave. The P.233

last portions of the ventricle to depolarize generate a net dipole with the direction shown in panel 4, and thus the deflection on the ECG is downward. This final deflection is the S wave. The ECG tracing returns to baseline when all of the ventricular muscle becomes depolarized and all dipoles associated with ventricular depolarization disappear. The S-T segment, or the period between the end of the S wave and the beginning of the T wave, is generally isoelectric. This indicates that no dipoles large enough to influence the ECG exist because all ventricular muscle is depolarized (the action potentials of all ventricular cells are in phase 2).
Repolarization, like depolarization, generates a dipole because the voltage of the depolarized area is different from that of the repolarized areas. The dipole associated with atrial repolarization does not appear as a separate deflection on the ECG because it generates a low voltage and because it is masked by the much larger QRS complex, which is present at the same time. Ventricular repolarization is not as orderly as ventricular depolarization. The duration of ventricular action potentials is longer in subendocardial myocardium than in subepicardial myocardium. The longer duration of subendocardial action potentials means that even though subendocardial cells were the first to depolarize, they are the last to repolarize. Because subepicardial cells repolarize first, the subepicardium is positive relative to the subendocardium That is, the polarity of the net dipole of repolarization is the same as the polarity of the dipole of depolarization. This results in an upward deflection because, as in depolarization, point A is positive with respect to point B. This deflection is the T wave (see panel 5, Fig. 12.8). The T wave has a longer duration than the QRS complex because repolarization does not proceed as a synchronized, propagated wave. Instead, the timing of repolarization is a function of properties of individual cells, such as numbers of particular K+ channels.