Embed Size (px)
Citation preview
ANATOMY AND EXAMINATIONOF HIP JOINT
MODERATORS : Dr. CH.ADITYA (D-ortho)
DR.C. RAGHURAM(PROF&HOD)
DR.B.RAMESH (PROF & HOD)
DR.CH. RAMU (ASSO.PROF)
DR.VENU (ASST.PROF)
DR.VAMSHIDHAR REDDY (ASST.PROF)
DR.K. RAVIKANTH (ASST.PROF)
DR.SURESH (ASST.PROF)
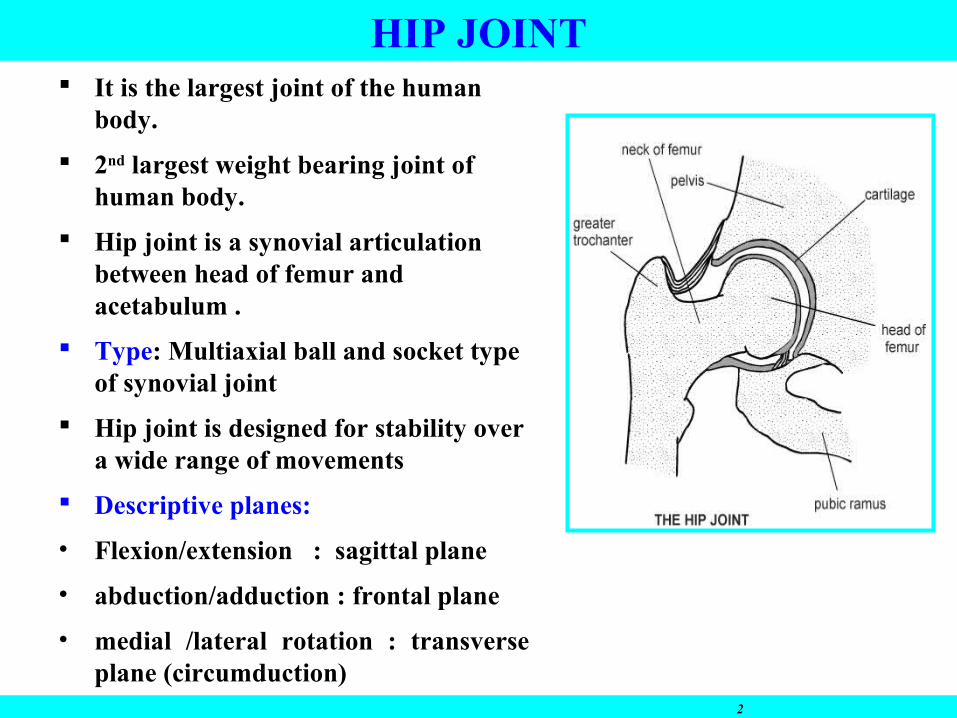
It is the largest joint of the human body.
2nd largest weight bearing joint of human body.
Hip joint is a synovial articulation between head of femur and acetabulum .
Type: Multiaxial ball and socket type of synovial joint
Hip joint is designed for stability over a wide range of movements
Descriptive planes:
• Flexion/extension : sagittal plane
• abduction/adduction : frontal plane
• medial /lateral rotation : transverse plane (circumduction)
2
HIP JOINT
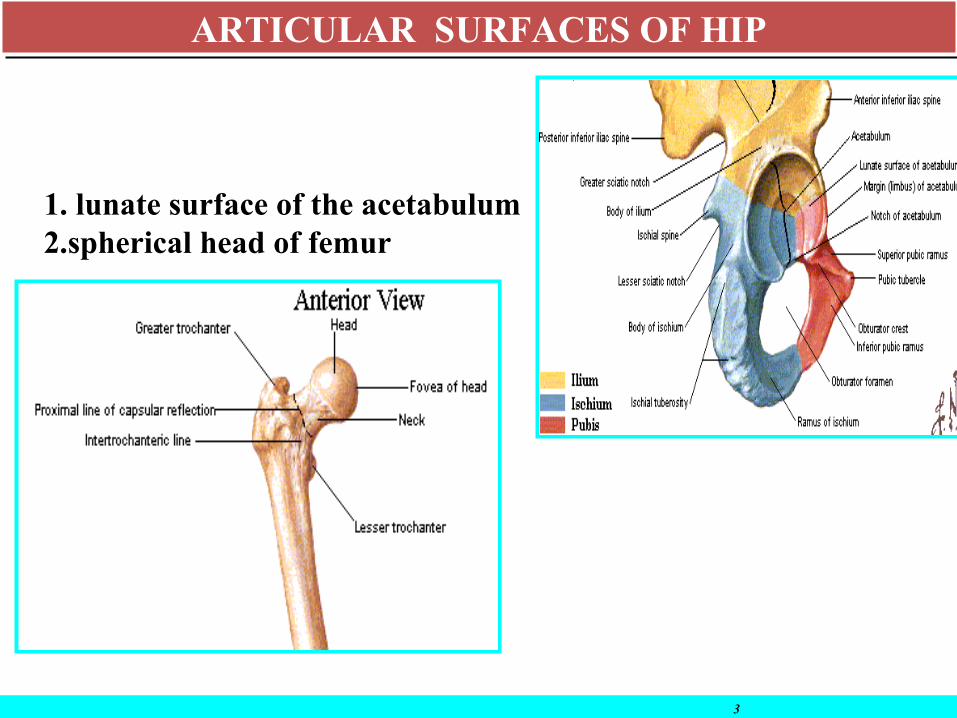
1. lunate surface of the acetabulum 2.spherical head of femur
3
ARTICULAR SURFACES OF HIPARTICULAR SURFACES OF HIP
Acetabulum
04/25/15 Dept of Sports Medicine, AFMC 4
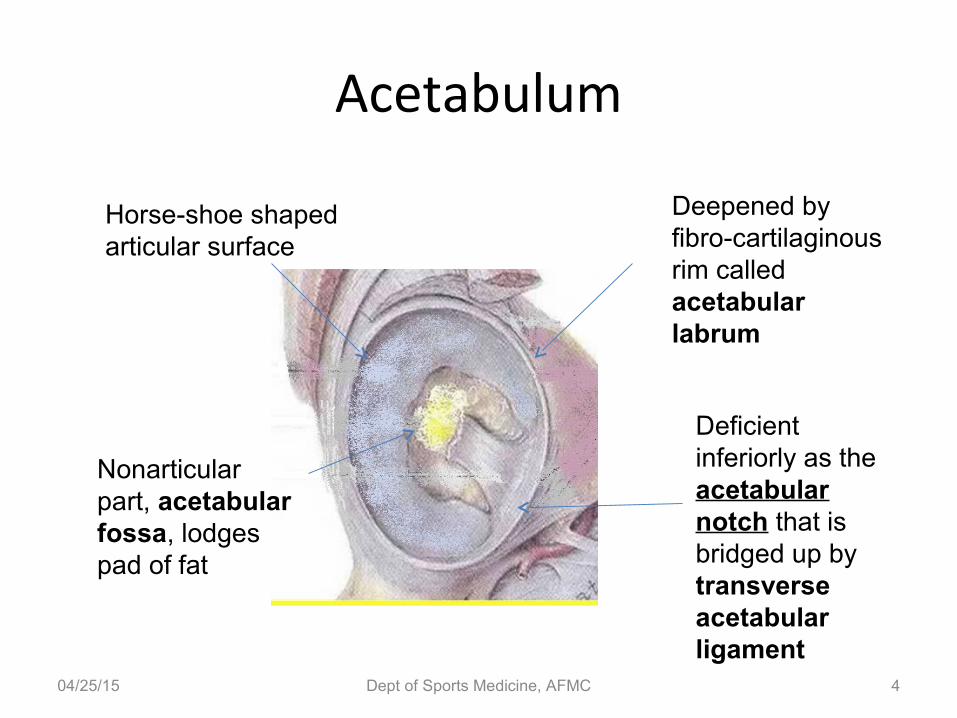
Horse-shoe shaped articular surface
Deepened by fibro-cartilaginous rim called acetabular labrum
Nonarticular part, acetabular fossa, lodges pad of fat
Deficient inferiorly as the acetabular notch that is bridged up by transverse acetabular ligament
• Acetabulum is the depression or fossa where the femoral head articulates .
It is positioned in downward and outward direction
• The rim of acetabulum is raised slightly by a fibro cartilaginous collar
known as acetabular labrum. Inferiorly the labrum bridges across the
acetabular notch as the transverse acetabular ligament and converts the
notch into foramen
• The lunate surface of the acetabulum is covered by hyaline cartilage except
for fovea
• Acetabular fossa is non articular . Formed mainly by ischium and contains
loose connective tissue.
ACETABULUM
6
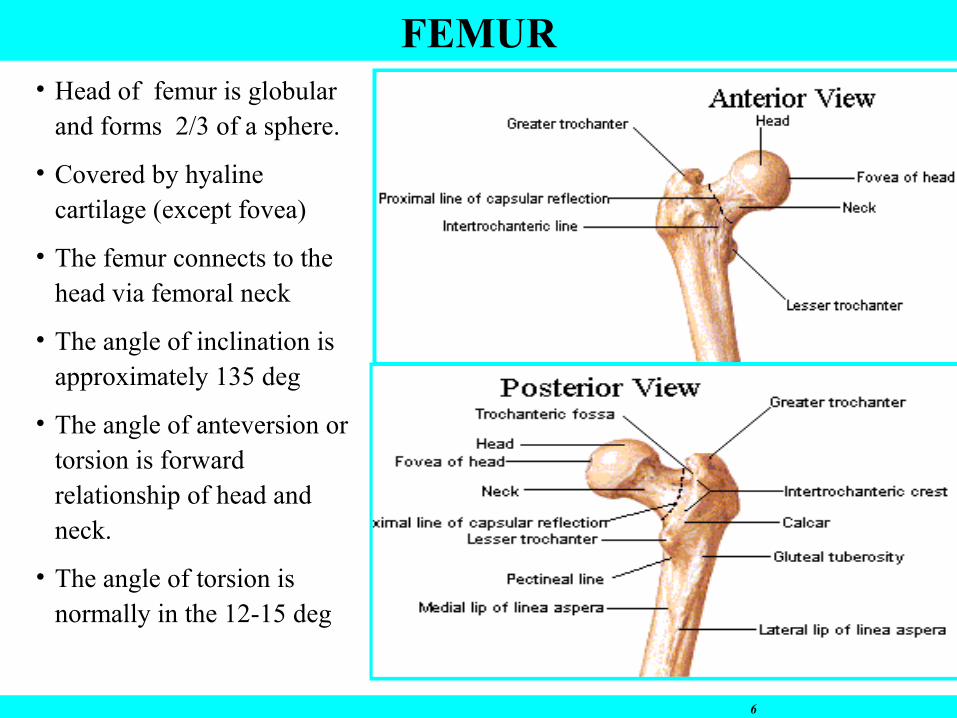
FEMUR• Head of femur is globular
and forms 2/3 of a sphere.
• Covered by hyaline cartilage (except fovea)
• The femur connects to the head via femoral neck
• The angle of inclination is approximately 135 deg
• The angle of anteversion or torsion is forward relationship of head and neck.
• The angle of torsion is normally in the 12-15 deg
Wide variation in anteversion of femoral neckTherefore during THA orientation of femoral
neck osteotomy in correct anteversion should be assessed after hip dislocation with reference to shaft of femur with knee flexed at 90 degrees.
If femoral neck osteotomy is made with reference to femoral neck anteversion inaccurate cut may result and subsequent malposition of prosthesis may occur.
FEMUR
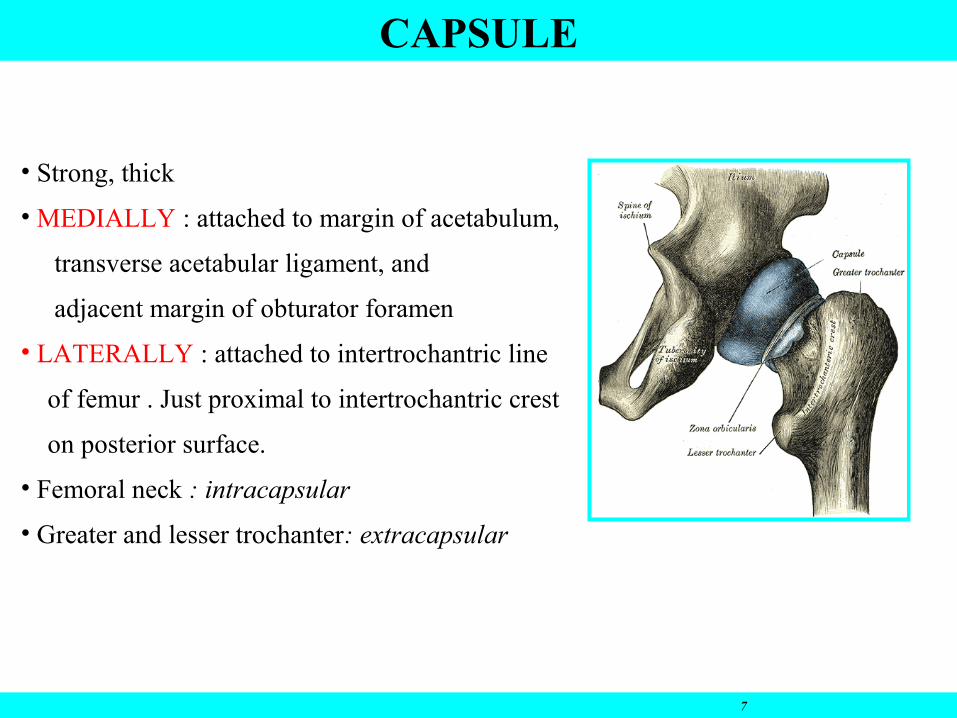
• Strong, thick
• MEDIALLY : attached to margin of acetabulum,
transverse acetabular ligament, and
adjacent margin of obturator foramen
• LATERALLY : attached to intertrochantric line
of femur . Just proximal to intertrochantric crest
on posterior surface.
• Femoral neck : intracapsular
• Greater and lesser trochanter: extracapsular
7
CAPSULE
8
SYNOVIAL MEMBRANE
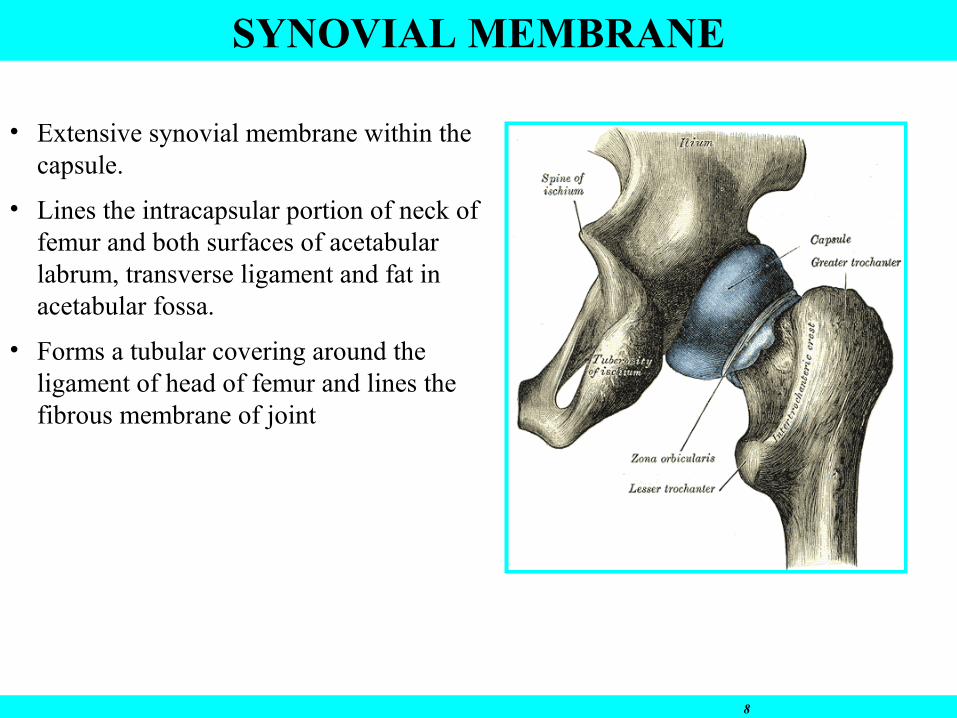
• Extensive synovial membrane within the capsule.
• Lines the intracapsular portion of neck of femur and both surfaces of acetabular labrum, transverse ligament and fat in acetabular fossa.
• Forms a tubular covering around the ligament of head of femur and lines the fibrous membrane of joint
LIGAMENTS• 3 ligaments reinforce the external surface of fibrous membrane and
stabilize the joint they are
• 1) iliofemoral ligament
• 2) pubofemoral ligament• 3) ischiofemoral ligament• Fibers of all three ligaments are oriented in a spiral fashion around the hip
joint so that the become taught when joint is extended.• This stabilizes the joint and reduces the amount of muscle energy required
to maintain a standing position.
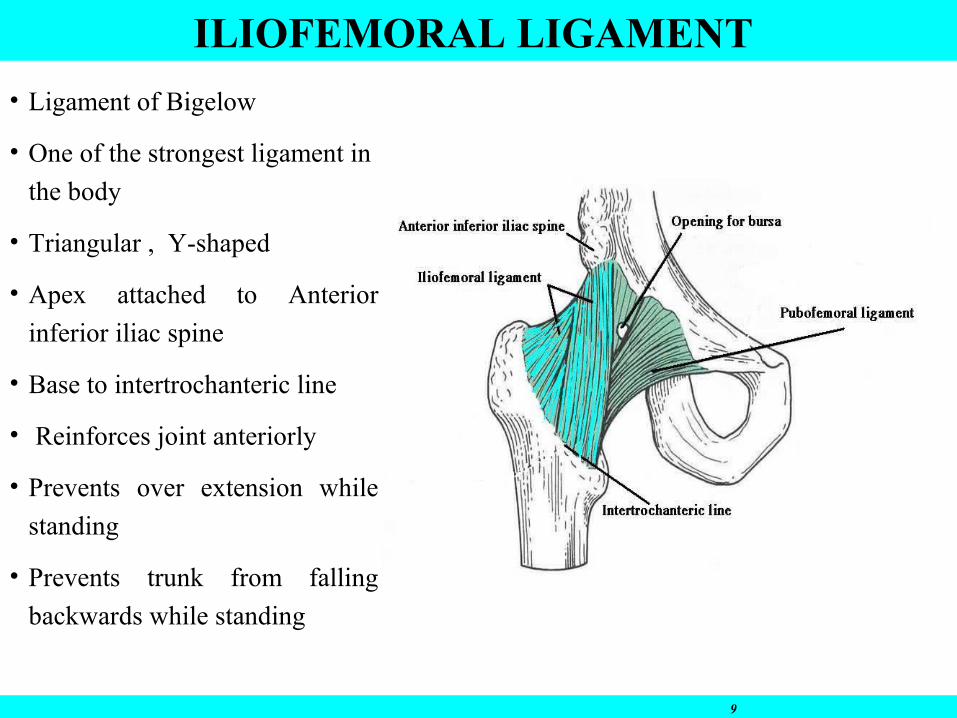
• Ligament of Bigelow
• One of the strongest ligament in
the body
• Triangular , Y-shaped
• Apex attached to Anterior
inferior iliac spine
• Base to intertrochanteric line
• Reinforces joint anteriorly
• Prevents over extension while
standing
• Prevents trunk from falling
backwards while standing
9
ILIOFEMORAL LIGAMENT
PUBOFEMORAL LIGAMENT
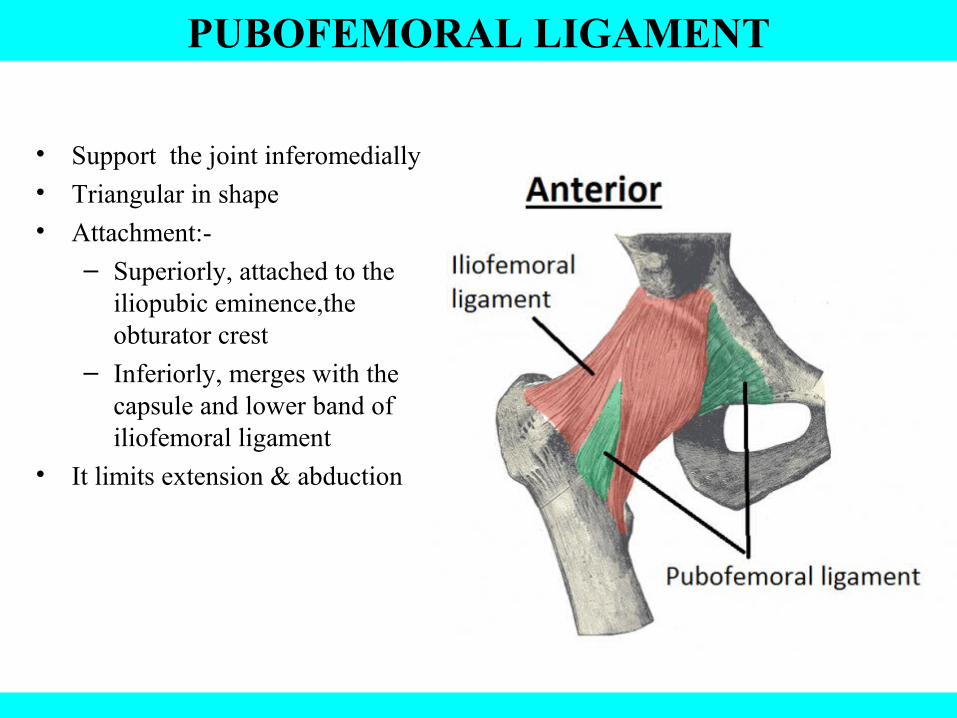
• Support the joint inferomedially
• Triangular in shape
• Attachment:-
– Superiorly, attached to the iliopubic eminence,the obturator crest
– Inferiorly, merges with the capsule and lower band of iliofemoral ligament
• It limits extension & abduction
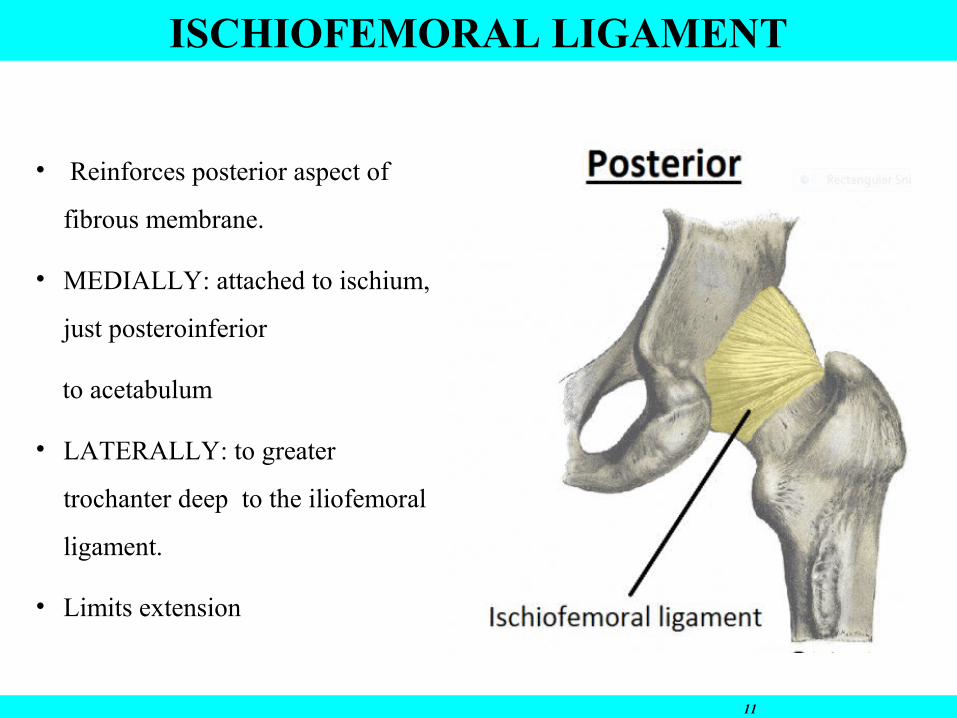
• Reinforces posterior aspect of
fibrous membrane.
• MEDIALLY: attached to ischium,
just posteroinferior
to acetabulum
• LATERALLY: to greater
trochanter deep to the iliofemoral
ligament.
• Limits extension
11
ISCHIOFEMORAL LIGAMENT
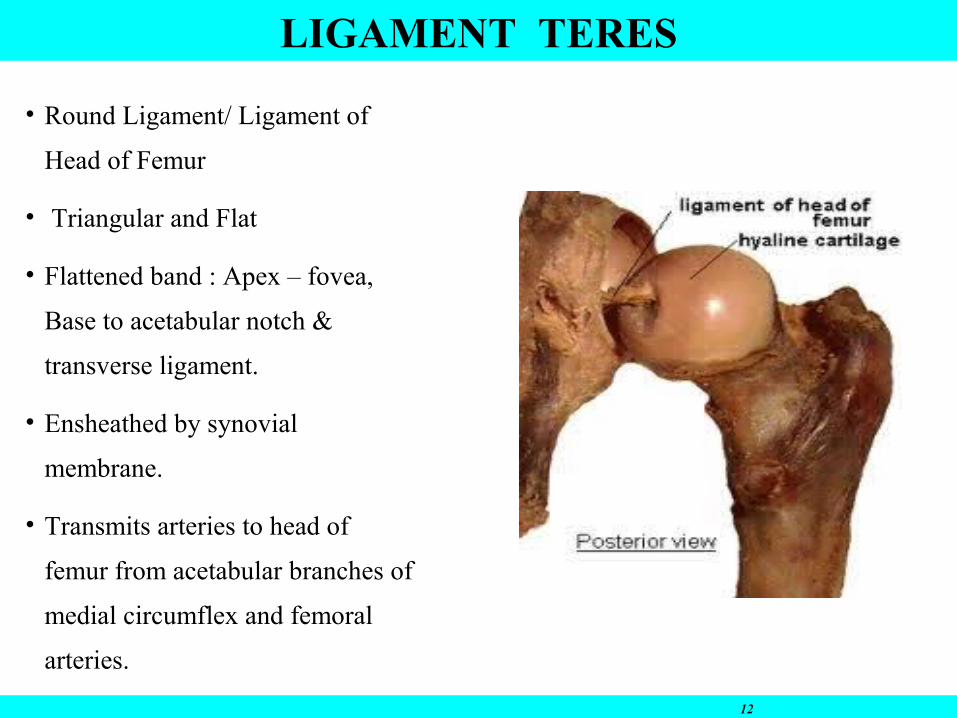
• Round Ligament/ Ligament of
Head of Femur
• Triangular and Flat
• Flattened band : Apex – fovea,
Base to acetabular notch &
transverse ligament.
• Ensheathed by synovial
membrane.
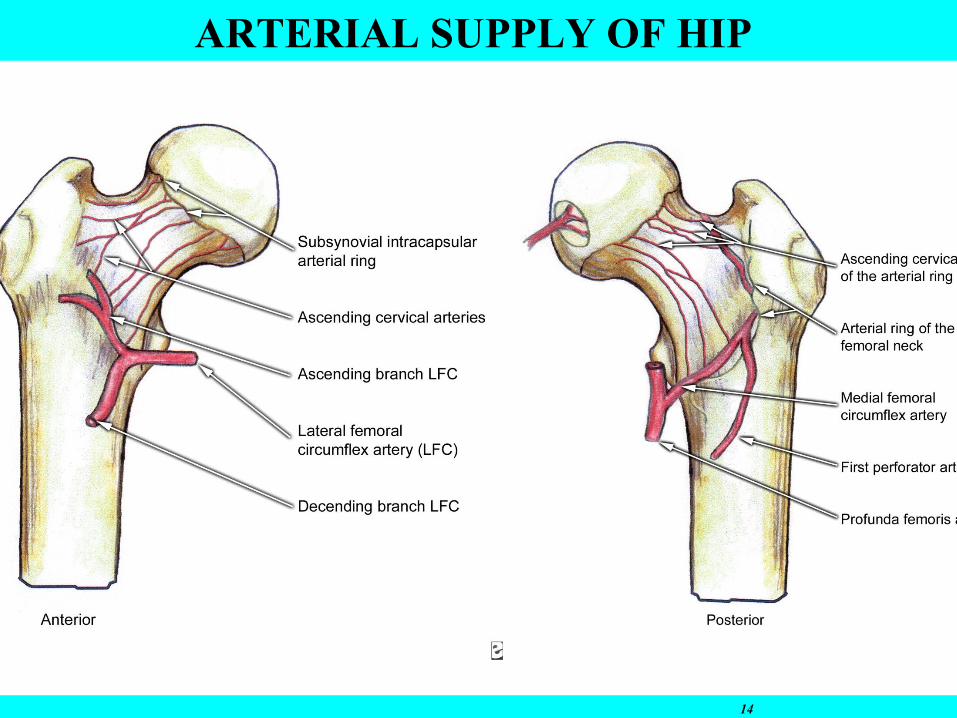
• Transmits arteries to head of
femur from acetabular branches of
medial circumflex and femoral
arteries.
12
LIGAMENT TERES
Relations• Anteriorly: Iliopsoas, pectineus, and rectus
femoris
• Posteriorly: The obturator internus, the gamelli, and the quadratus femoris muscle separate the joint from sciatic nerve
• Superiorly: Piriformis and gluteus minimus
• Inferiorly: Obturator externus tendon
13
HIP JOINT: NERVE SUPPLY
• Femoral nerve
• Anterior division of Obturator nerve
• Nerve to Rectus femoris
• Nerve to Quadratus femoris
• Sciatic nerve
• Superior gluteal nerve
Hilton’s law: “the nerve supplying the joint also supply the muscles moving the joint & the skin
covering the insertion of these muscles”
• Femoral nerve not only supplies hip joint via intermediate and cutaneous nerve of thigh, also supplies skin of front and medial side of thigh• Posterior division of obturator nerve supplies both hip and knee joint. Therefore sometimes there is referred pain to knee joint.
14
ARTERIAL SUPPLY OF HIP
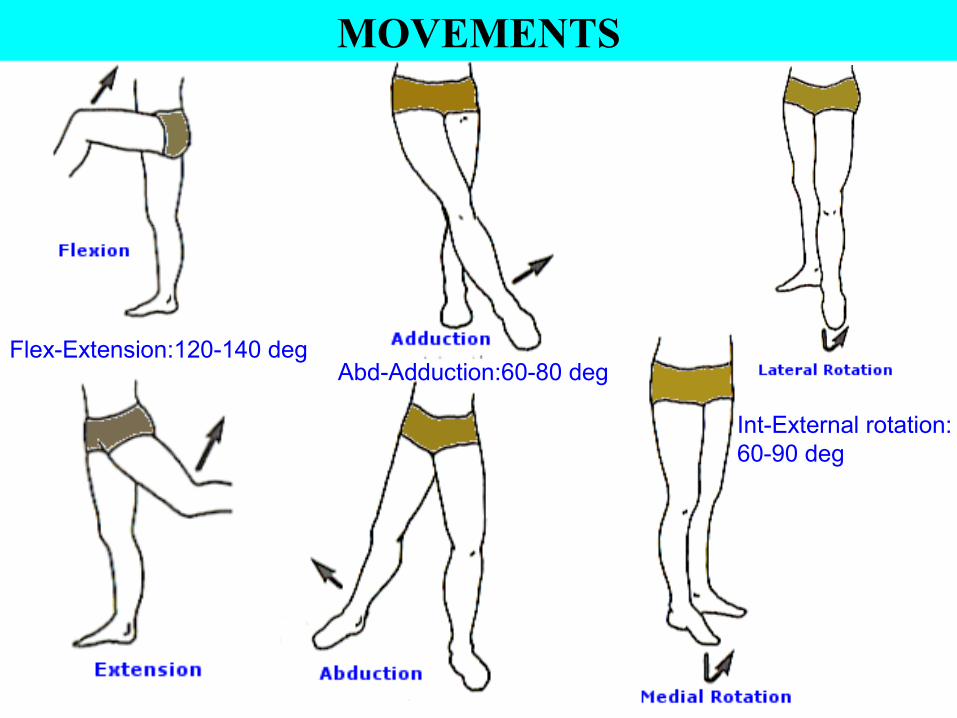
MOVEMENTS
Flex-Extension:120-140 degAbd-Adduction:60-80 deg
Int-External rotation: 60-90 deg
18
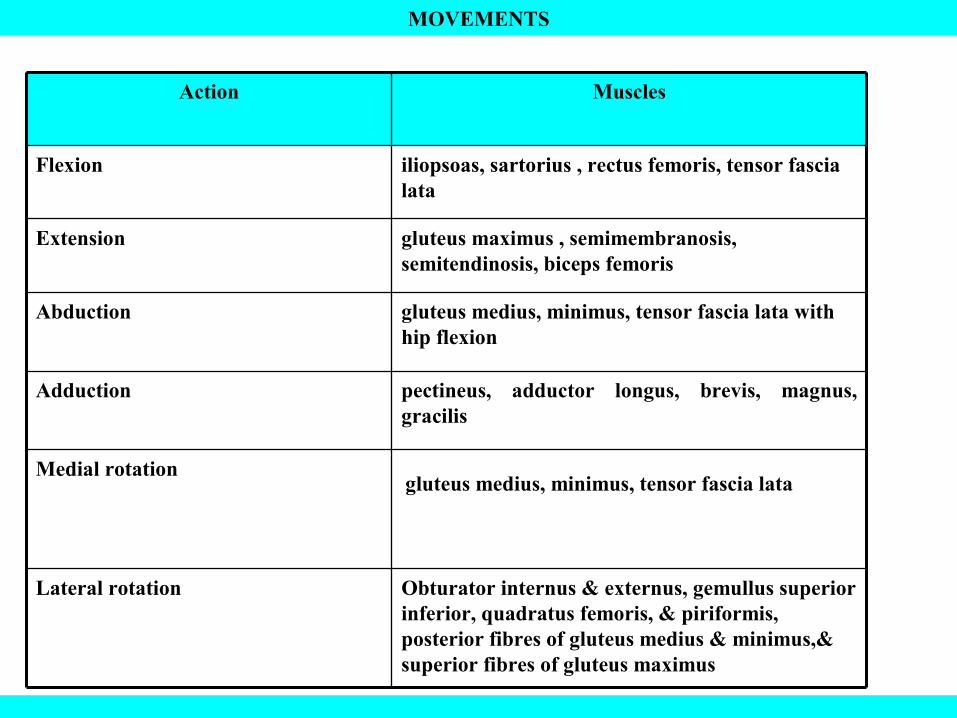
MOVEMENTS
Obturator internus & externus, gemullus superior inferior, quadratus femoris, & piriformis, posterior fibres of gluteus medius & minimus,& superior fibres of gluteus maximus
Lateral rotation
Medial rotation
pectineus, adductor longus, brevis, magnus, gracilis
Adduction
gluteus medius, minimus, tensor fascia lata with hip flexion
Abduction
gluteus maximus , semimembranosis, semitendinosis, biceps femoris
Extension
iliopsoas, sartorius , rectus femoris, tensor fascia lata
Flexion
MusclesAction
gluteus medius, minimus, tensor fascia lata
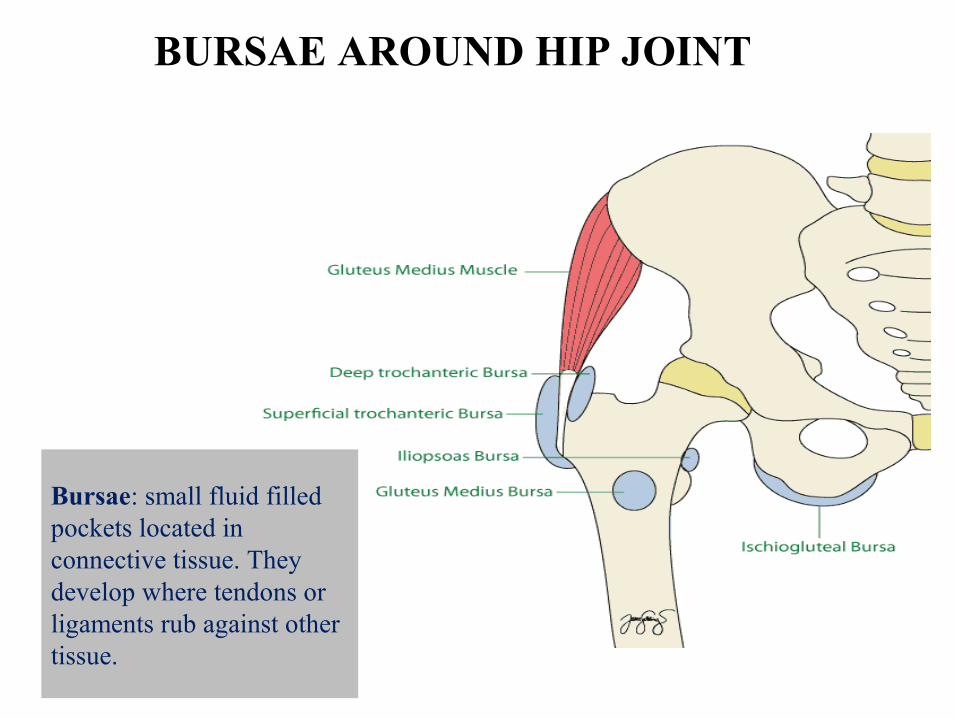
BURSAE AROUND HIP JOINT
Bursae: small fluid filled pockets located in connective tissue. They develop where tendons or ligaments rub against other tissue.
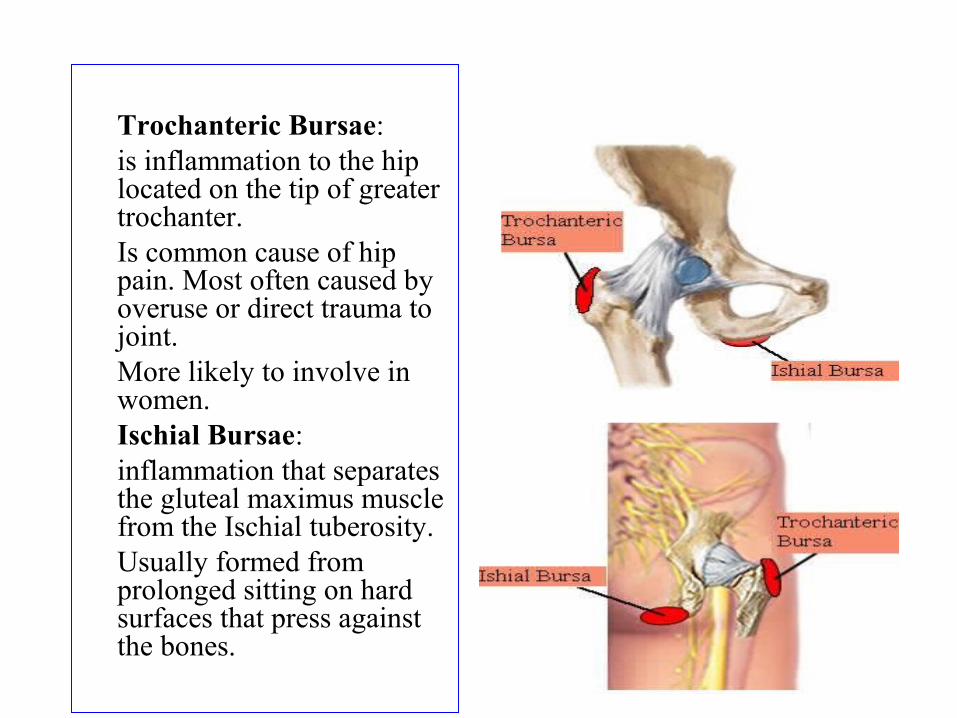
1) Trochanteric Bursae: 2) is inflammation to the hip
located on the tip of greater trochanter.
3) Is common cause of hip pain. Most often caused by overuse or direct trauma to joint.
4) More likely to involve in women.
5) Ischial Bursae: 6) inflammation that separates
the gluteal maximus muscle from the Ischial tuberosity.
7) Usually formed from prolonged sitting on hard surfaces that press against the bones.
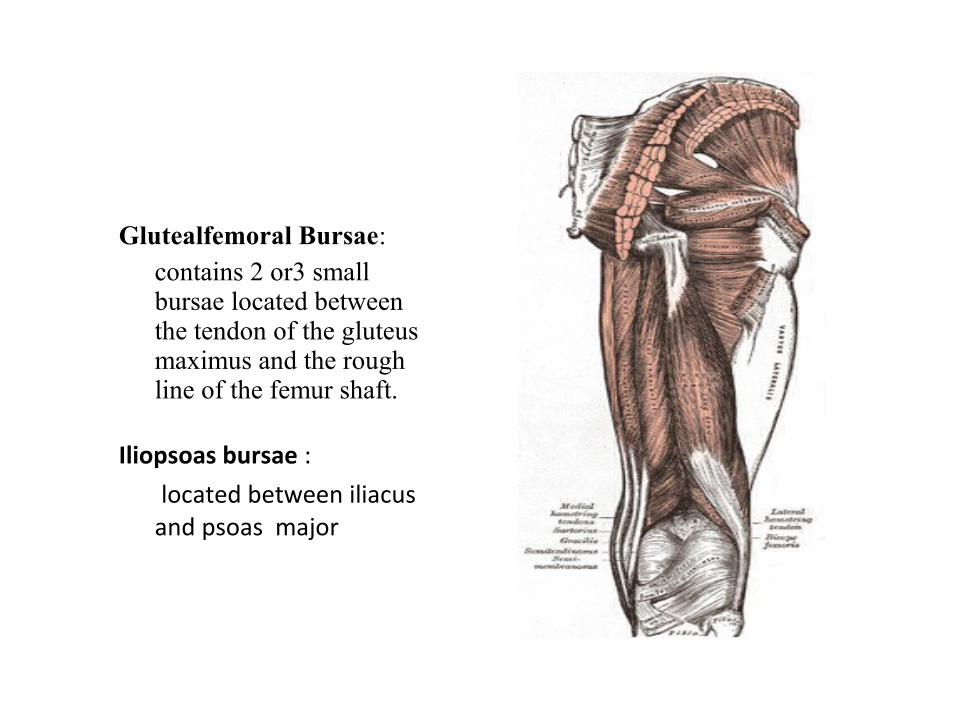
Glutealfemoral Bursae: 1) contains 2 or3 small
bursae located between the tendon of the gluteus maximus and the rough line of the femur shaft.
Iliopsoas bursae :
located between iliacus and psoas major
OSSIFICATION OF HIP BONE• the hip bone ossifies in cartilage from 3 primary centres and 5 secondary
centres
Primary centres :
• One for ilium appears at 2nd month of IUL
• One for ischium appears during 4 th month of IUL
• One for pubis appears during 5th month of IUL
at birth hip bone is ossified except for 3 cartilaginous parts .these are
1) the iliac crest
2) A y shaped cartilage separating the ilium, ischium and pubis
3) a strip along the inferior margin of bone including Ischial tuberosity.
Secondary centres are
• 2 for iliac crest
• 2 for y- shaped cartilage of acetabulum
• One for Ischial tuberosity
• All fuses at 20-25 years
• The ischiopubic rami fuse with each other at 7-8 yrs of age





























