Embed Size (px)
Citation preview

Patello- femoral joint instability
DR MOHIT GOELJR II, 28th Aug, 2013
The patellofemoral joint (PFJ) is a complex structure with high functional and biomechanical requirements.
The normal function of this joint is dependent on the congruent relationship of the patella with the trochlear groove.
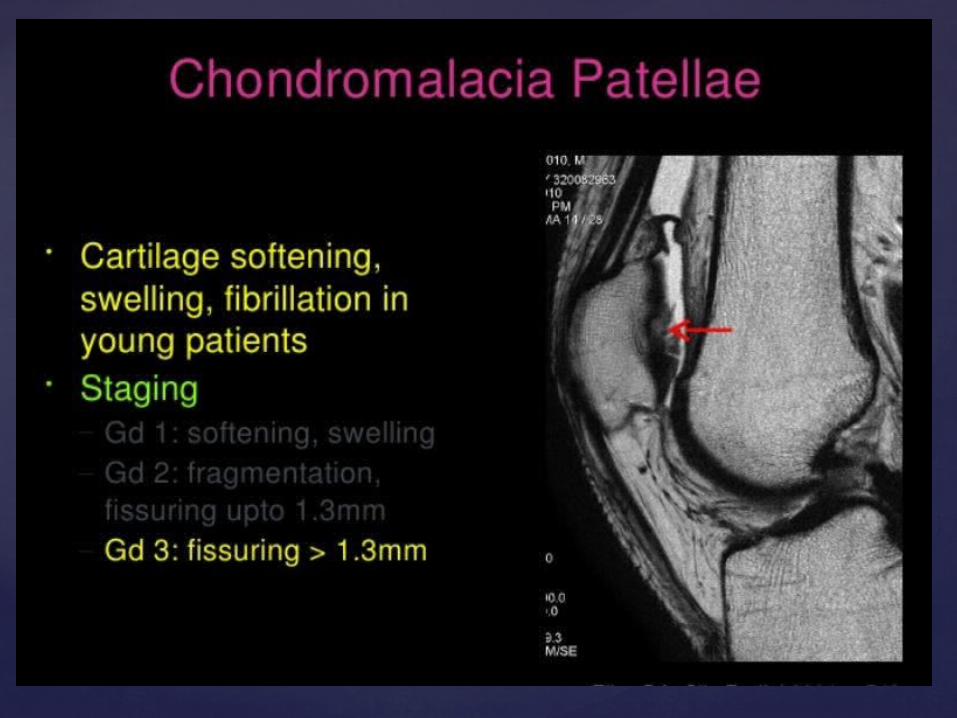
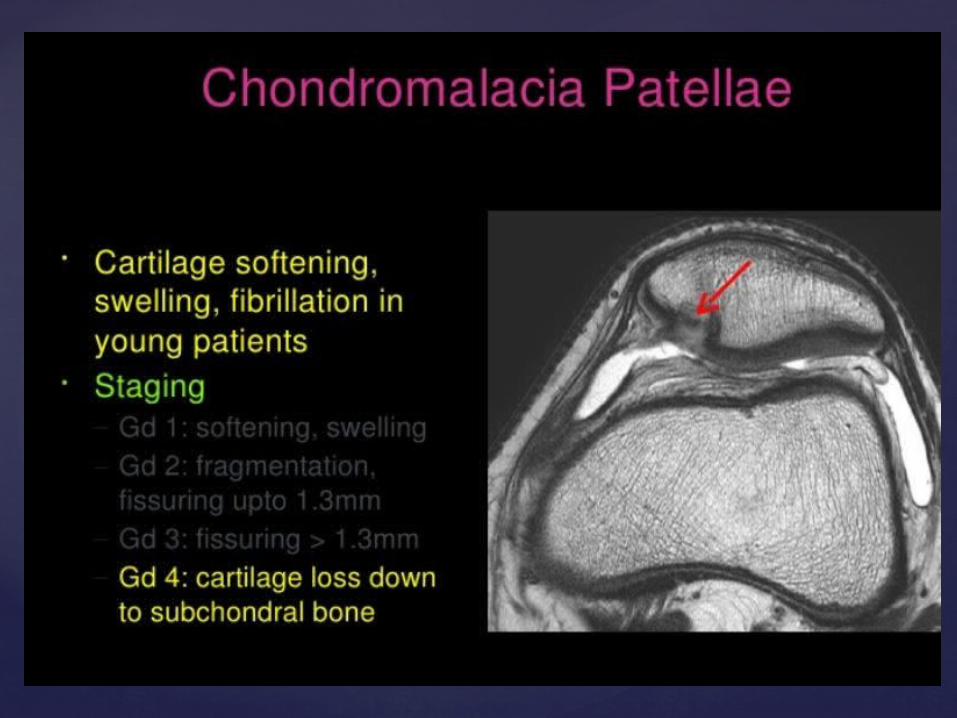
Developmental or acquired alterations in the surface geometry of the PFJ are associated with multiple clinical problems such as patellar instability; chondromalacia patella; and, consequently, anterior knee pain
Patellar Measurements
All measurements were made on the sagittal slice showing the greatest patella length.
The following measurements were obtained: patellar length, the length of the patellar tendon, the length of the patellar articular cartilage, and the length of the trochlear articular cartilage overlapping with the patellar cartilage.
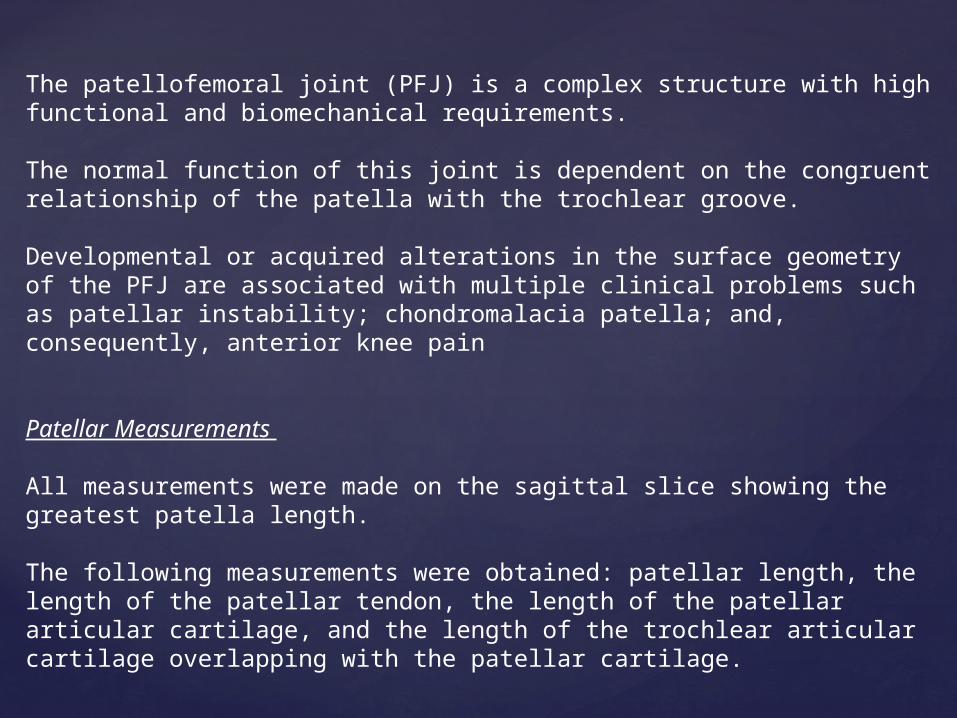
Patellar measurements in 35-year-old woman who underwent knee MRI. Patellar facet asymmetry. Medial patellar facet (MF) and lateral patellar facet (LF) were measured.
Axial slices were used to determine the patellar facet asymmetry, which is described as the ratio of the medial and lateral patellar facet lengths
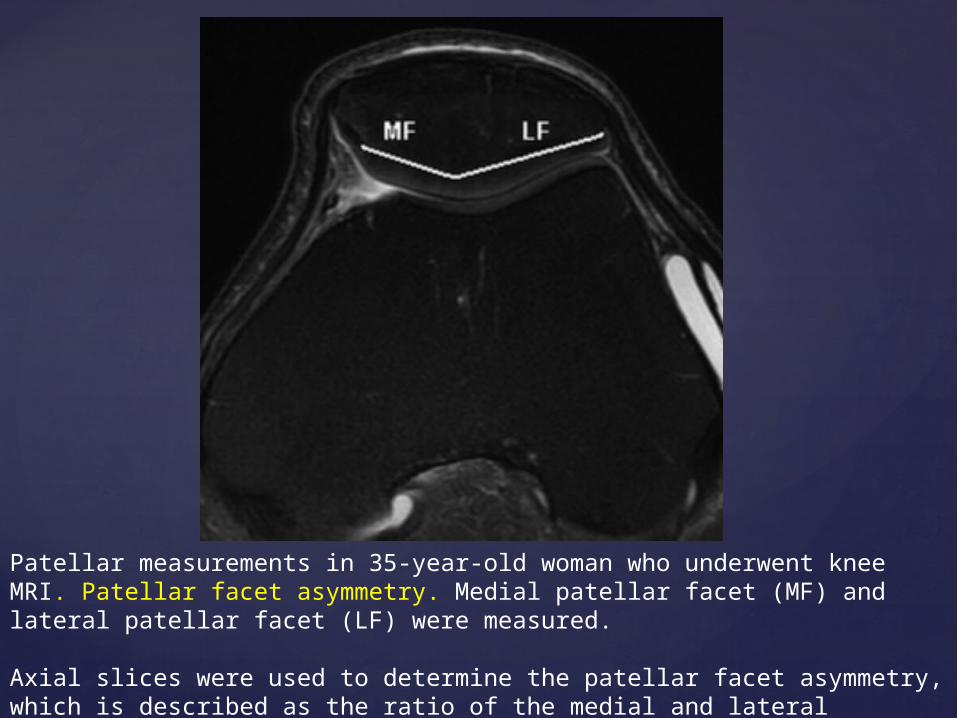
Patellotrochlear cartilage overlap. Patellar articular cartilage (PC) and trochlear articular cartilage (TC) were measured from caudal extent of patellar cartilage to cranial end of trochlear cartilage overlapping with patellar cartilage.
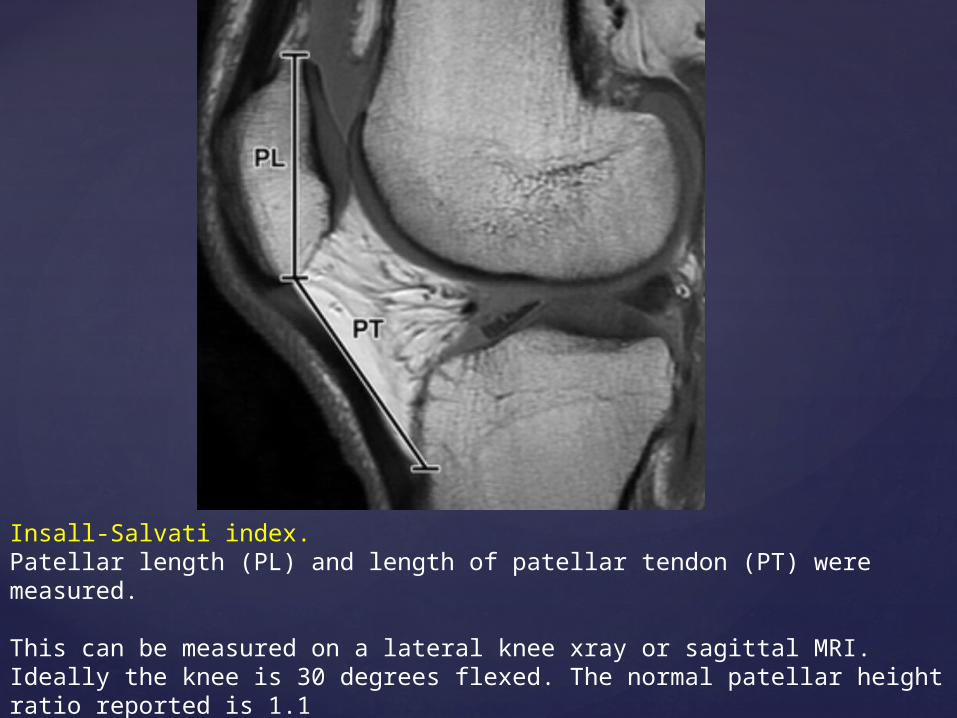
Insall-Salvati index. Patellar length (PL) and length of patellar tendon (PT) were measured.
This can be measured on a lateral knee xray or sagittal MRI. Ideally the knee is 30 degrees flexed. The normal patellar height ratio reported is 1.1patella alta : > 1.2 (>1.5) patella baja : < 0.8 (<0.74)
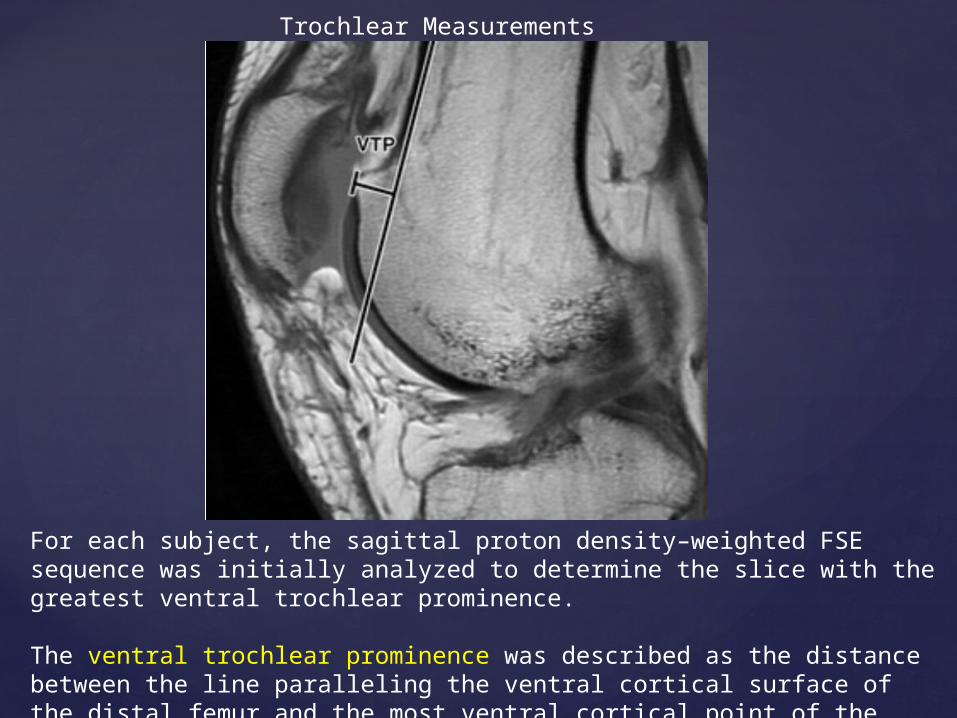
For each subject, the sagittal proton density–weighted FSE sequence was initially analyzed to determine the slice with the greatest ventral trochlear prominence.
The ventral trochlear prominence was described as the distance between the line paralleling the ventral cortical surface of the distal femur and the most ventral cortical point of the femoral trochlear floor.
Trochlear Measurements
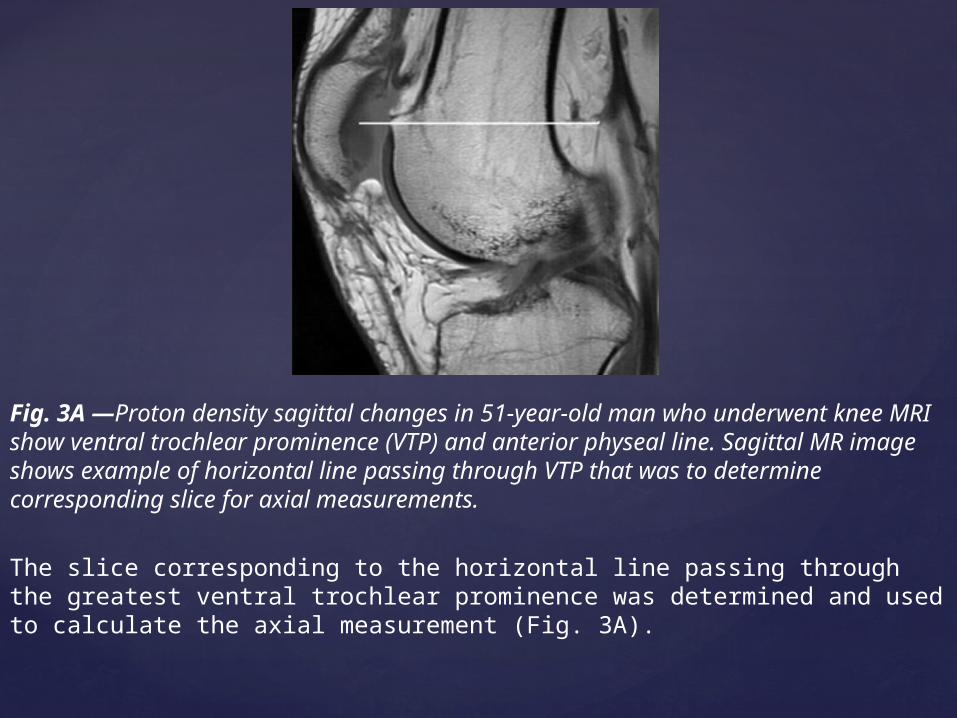
The slice corresponding to the horizontal line passing through the greatest ventral trochlear prominence was determined and used to calculate the axial measurement (Fig. 3A).
Fig. 3A —Proton density sagittal changes in 51-year-old man who underwent knee MRI show ventral trochlear prominence (VTP) and anterior physeal line. Sagittal MR image shows example of horizontal line passing through VTP that was to determine corresponding slice for axial measurements.

In PFJs with no trochlear prominence, the anterior physeal line was used as a reference for determining the axial slice (Fig. 3B).
Sagittal MR image shows example of anterior physeal line that was used as reference in knees with no VTP.
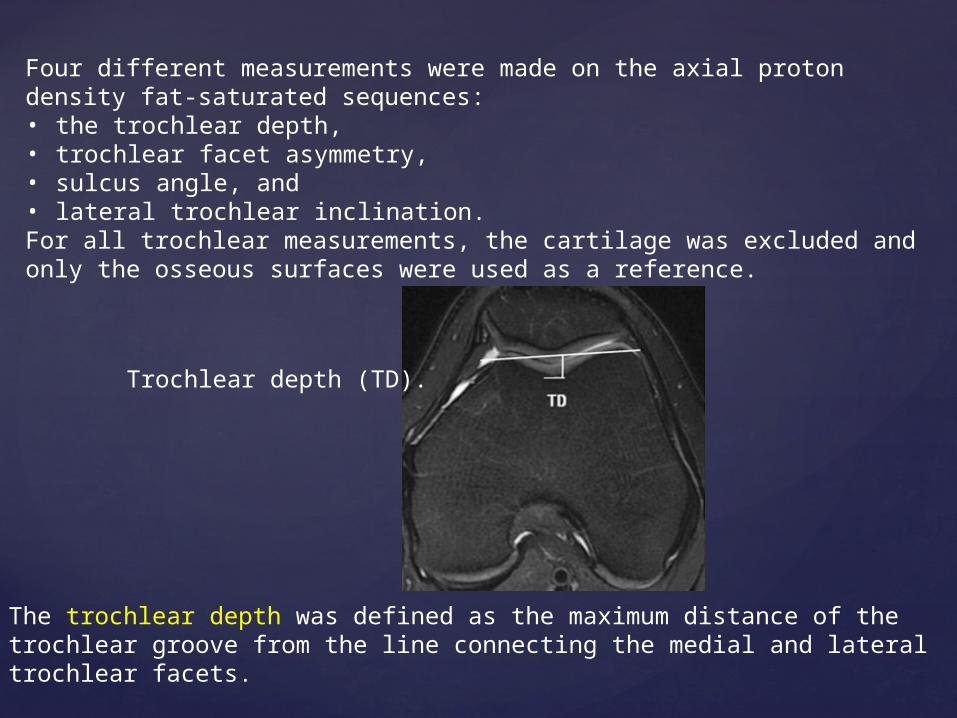
Four different measurements were made on the axial proton density fat-saturated sequences: • the trochlear depth, • trochlear facet asymmetry, • sulcus angle, and • lateral trochlear inclination. For all trochlear measurements, the cartilage was excluded and only the osseous surfaces were used as a reference.
The trochlear depth was defined as the maximum distance of the trochlear groove from the line connecting the medial and lateral trochlear facets.
A trochlear depth of less than 3mm is considered abnormal.
Trochlear depth (TD).
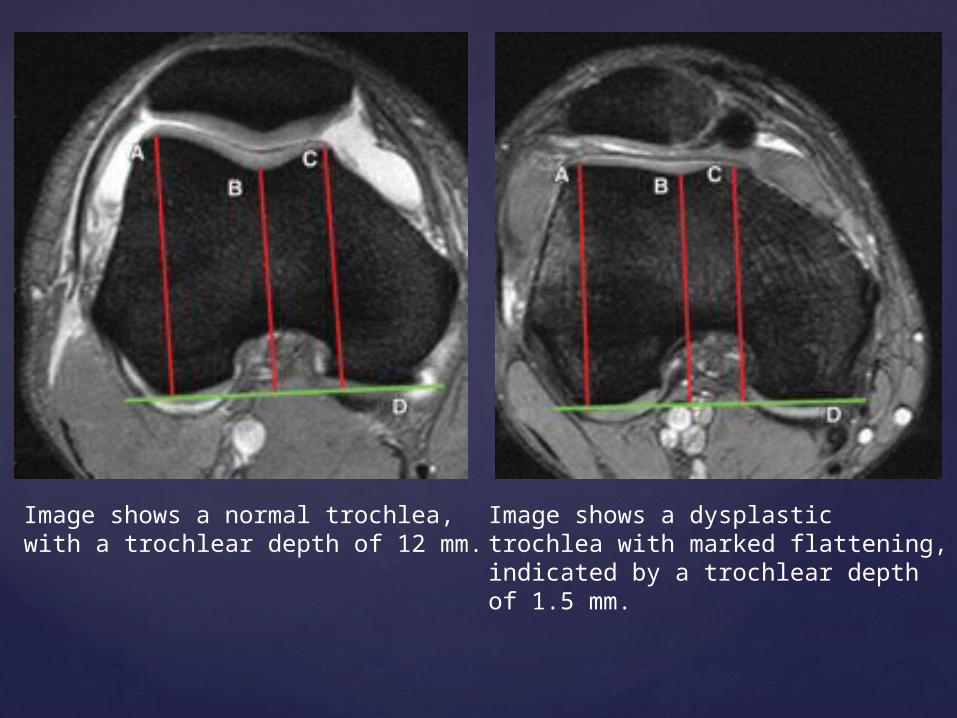
Image shows a normal trochlea, with a trochlear depth of 12 mm.
Image shows a dysplastic trochlea with marked flattening, indicated by a trochlear depth of 1.5 mm.
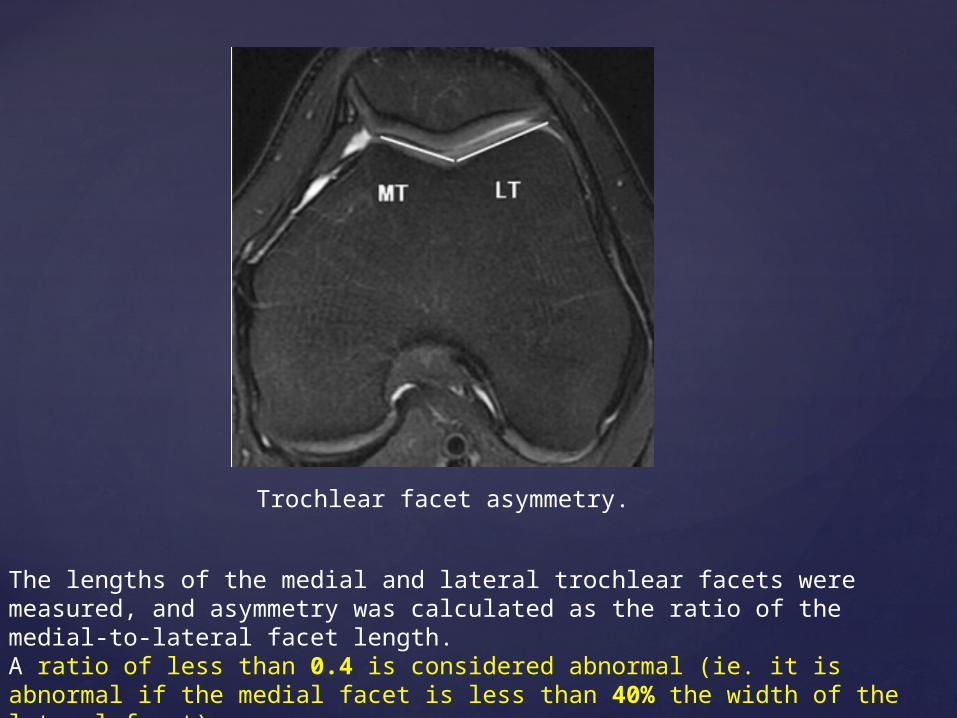
The lengths of the medial and lateral trochlear facets were measured, and asymmetry was calculated as the ratio of the medial-to-lateral facet length.A ratio of less than 0.4 is considered abnormal (ie. it is abnormal if the medial facet is less than 40% the width of the lateral facet).
Trochlear facet asymmetry.
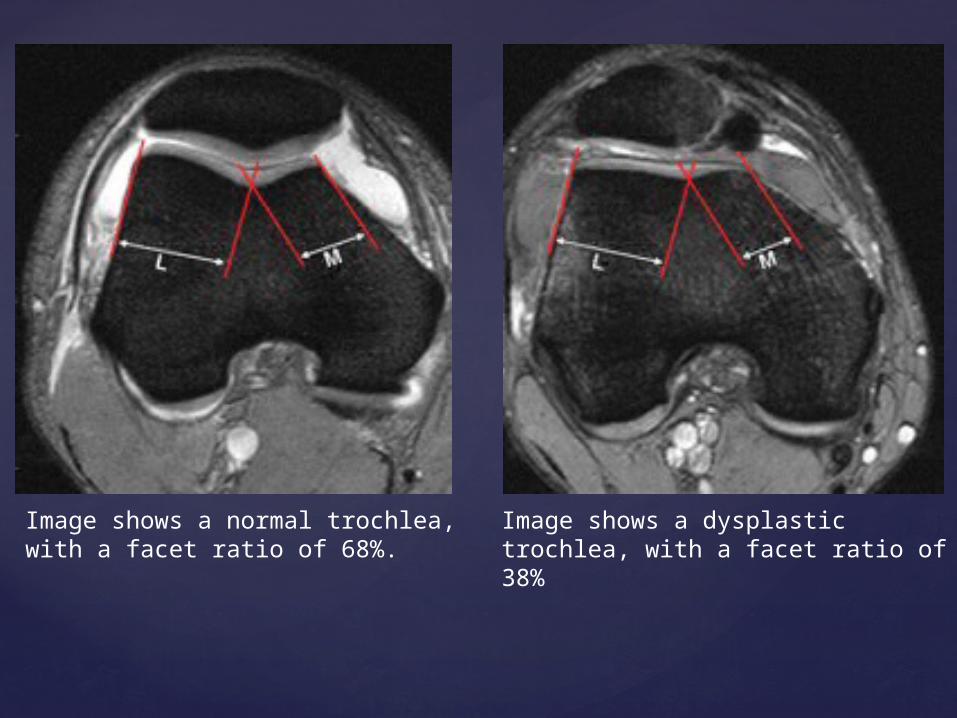
Image shows a normal trochlea, with a facet ratio of 68%.
Image shows a dysplastic trochlea, with a facet ratio of 38%
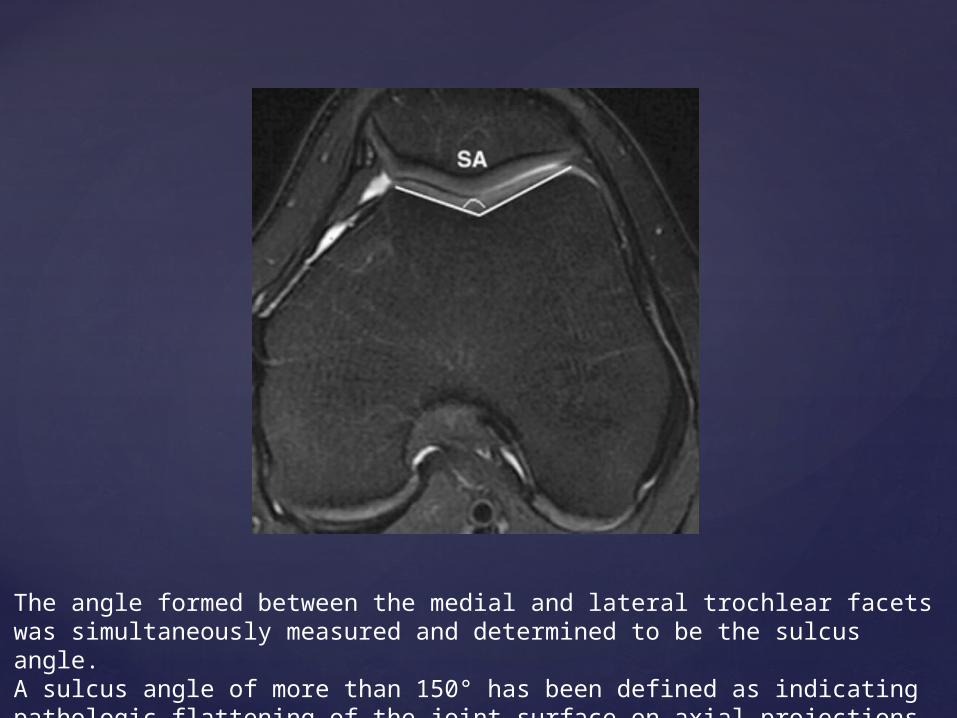
The angle formed between the medial and lateral trochlear facets was simultaneously measured and determined to be the sulcus angle.A sulcus angle of more than 150° has been defined as indicating pathologic flattening of the joint surface on axial projections.
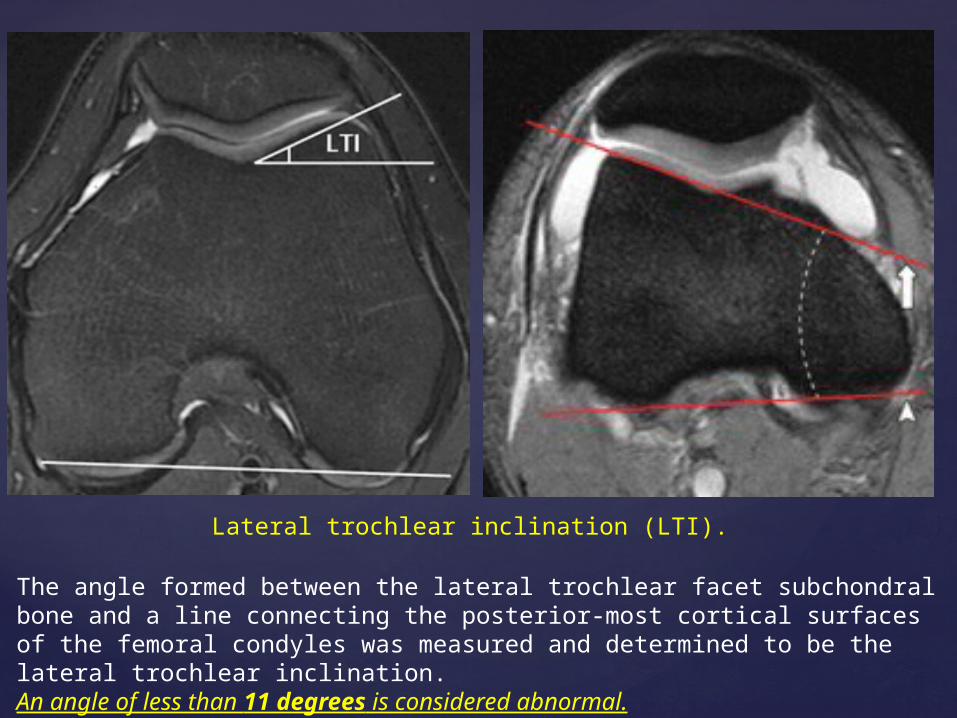
The angle formed between the lateral trochlear facet subchondral bone and a line connecting the posterior-most cortical surfaces of the femoral condyles was measured and determined to be the lateral trochlear inclination.An angle of less than 11 degrees is considered abnormal.
Lateral trochlear inclination (LTI).
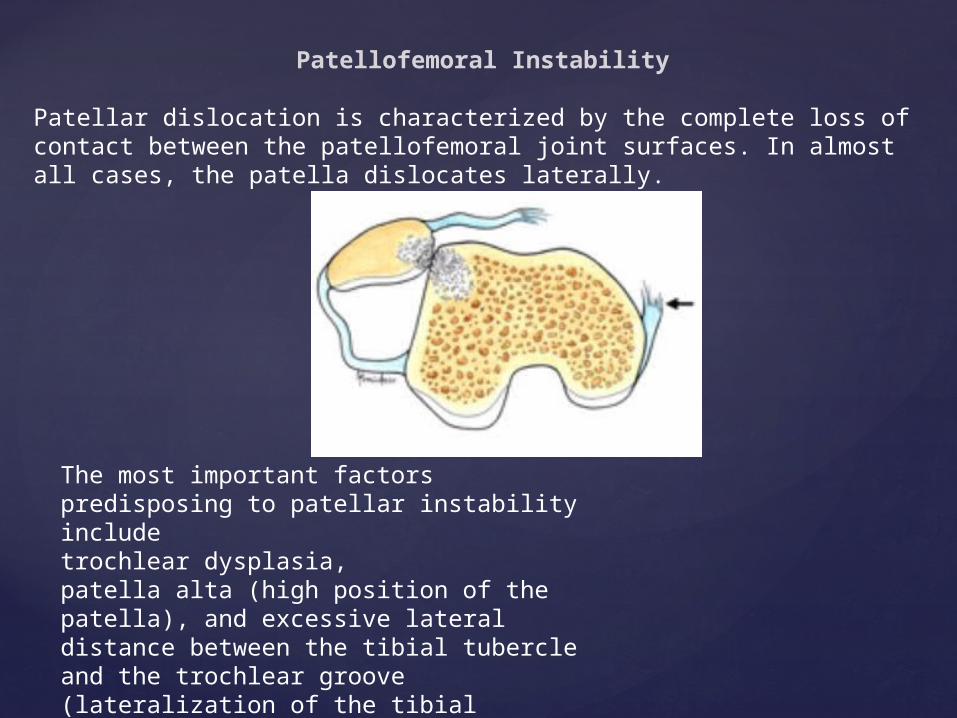
Patellofemoral Instability
Patellar dislocation is characterized by the complete loss of contact between the patellofemoral joint surfaces. In almost all cases, the patella dislocates laterally.
The most important factors predisposing to patellar instability include trochlear dysplasia, patella alta (high position of the patella), and excessive lateral distance between the tibial tubercle and the trochlear groove (lateralization of the tibial tuberosity).
Trochlear dysplasia

Trochlear dysplasia has been identified as one of the main factors contributing to chronic patellofemoral instability.
The classic criteria for diagnosing trochlear dysplasia were defined for conventional radiographs:
1] The “crossing sign” is a line represented by the deepest part of the trochlear groove crossing the anterior aspect of the condyles, assessed from lateral radiographs.
True lateral radiograph of a normal knee in a 42-year-old woman. The floor of the femoral trochlea does not cross the ventral outlines of the femoral condyles.
There is no ventral prominence of the trochlear floor.
The floor of the trochlea (arrow-heads) is always dorsal to the line paralleling the ventral cortical surface of the distal femur
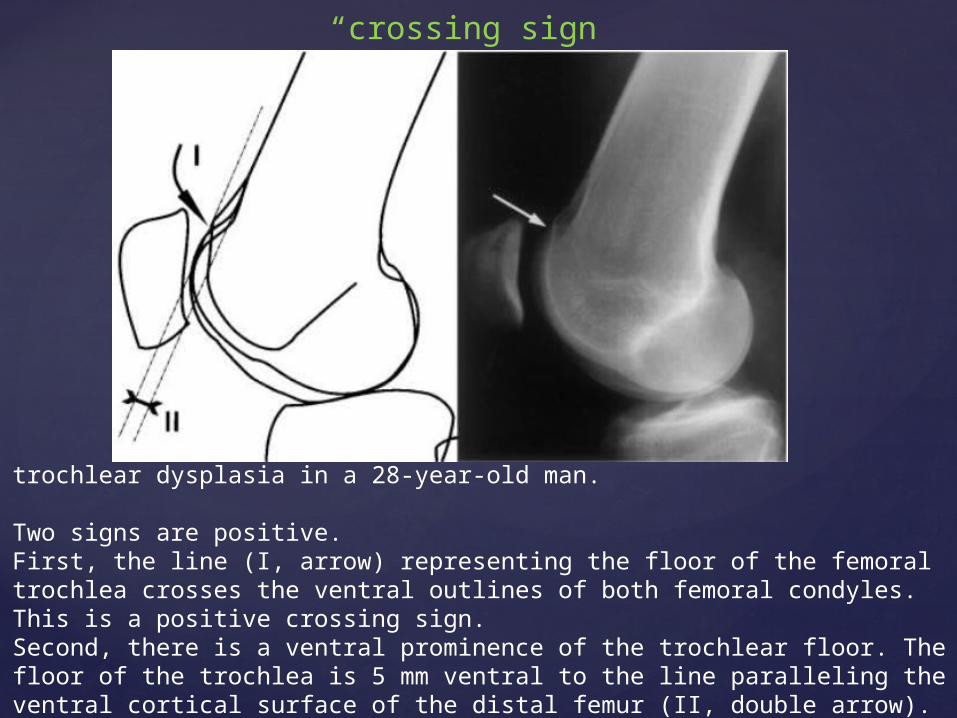
“crossing sign”
trochlear dysplasia in a 28-year-old man.
Two signs are positive.First, the line (I, arrow) representing the floor of the femoral trochlea crosses the ventral outlines of both femoral condyles. This is a positive crossing sign. Second, there is a ventral prominence of the trochlear floor. The floor of the trochlea is 5 mm ventral to the line paralleling the ventral cortical surface of the distal femur (II, double arrow).
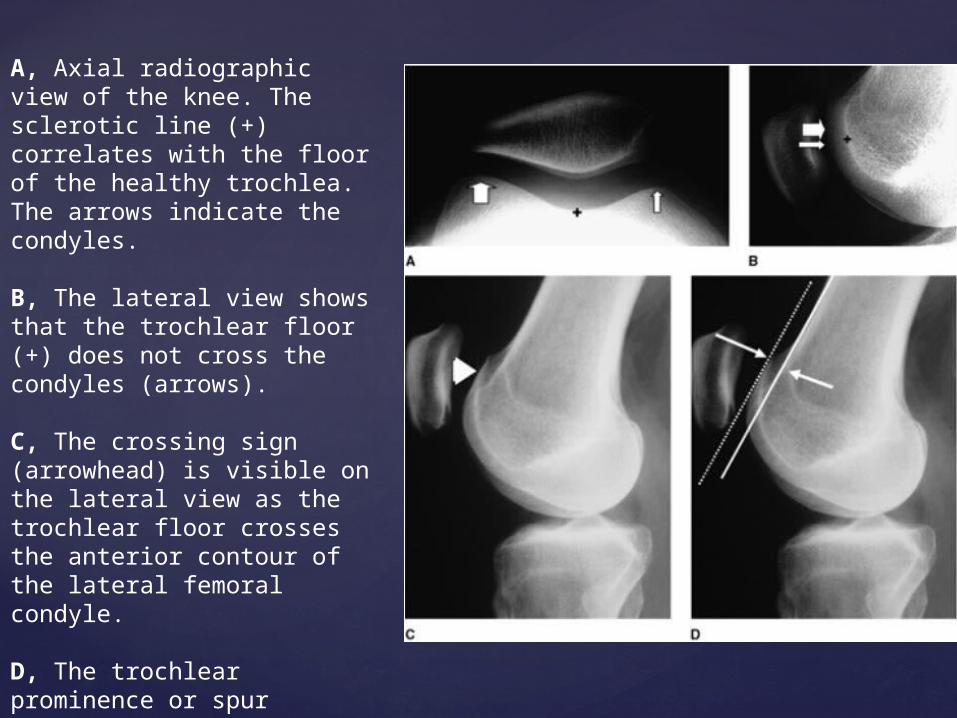
A, Axial radiographic view of the knee. The sclerotic line (+) correlates with the floor of the healthy trochlea. The arrows indicate the condyles.
B, The lateral view shows that the trochlear floor (+) does not cross the condyles (arrows).
C, The crossing sign (arrowhead) is visible on the lateral view as the trochlear floor crosses the anterior contour of the lateral femoral condyle.
D, The trochlear prominence or spur (arrows) is measured from the trochlear floor (dashed line) and a line extending from the anterior cortex of the distal femur (solid line).

2 ] The “double contour sign” is a double line at the anterior aspect of the condyles and is present if the medial condyle is hypoplastic.
3] A decreased trochlear depth and a large sulcus angle.
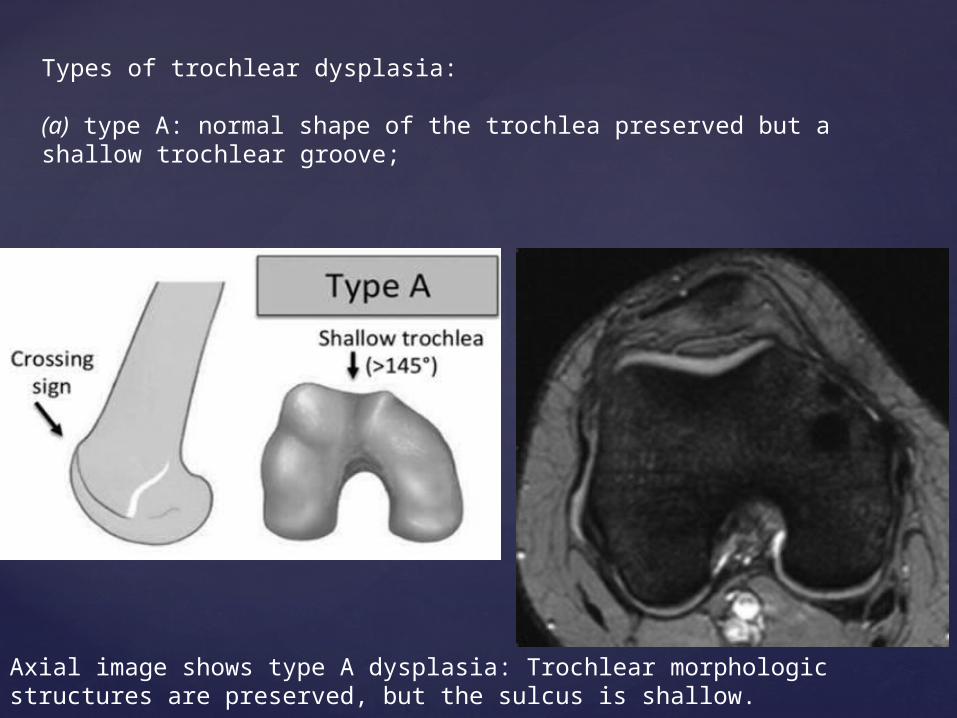
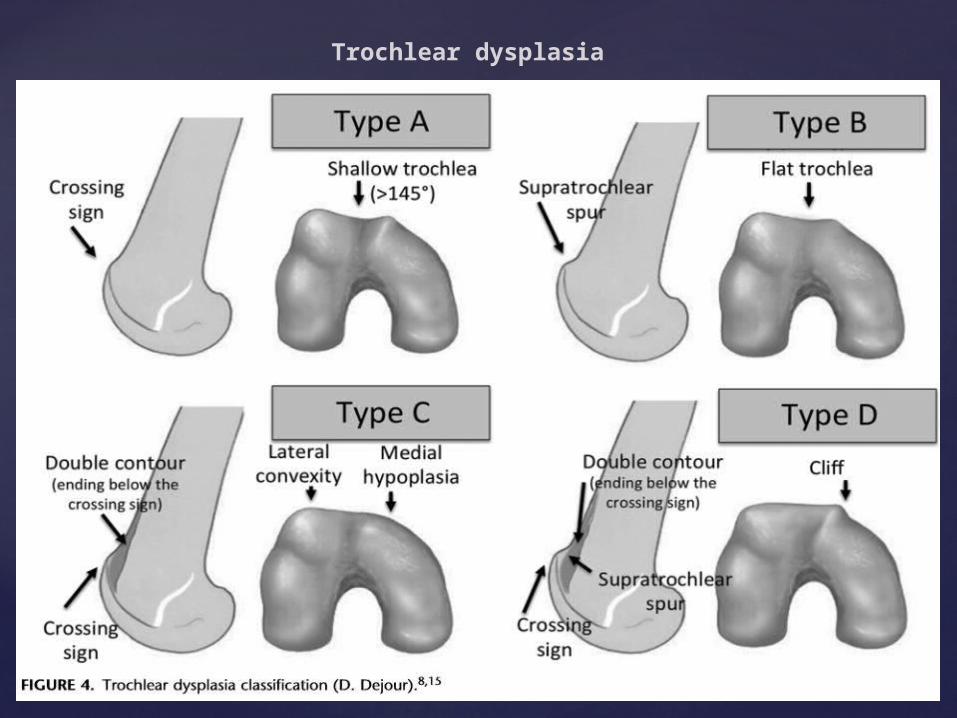
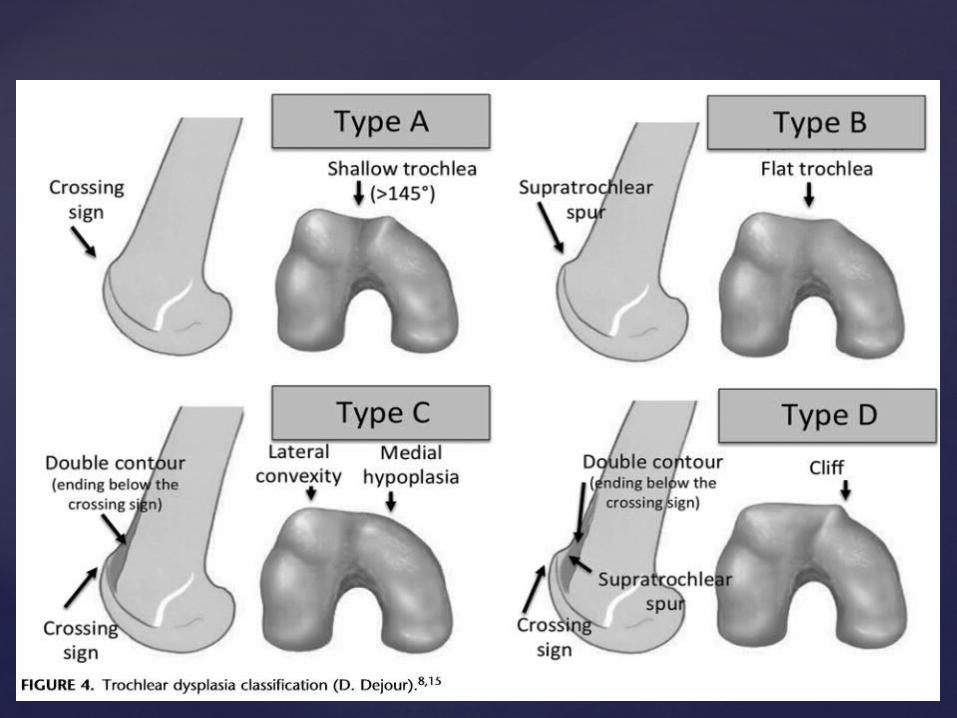
Types of trochlear dysplasia:
(a) type A: normal shape of the trochlea preserved but a shallow trochlear groove;
Axial image shows type A dysplasia: Trochlear morphologic structures are preserved, but the sulcus is shallow.
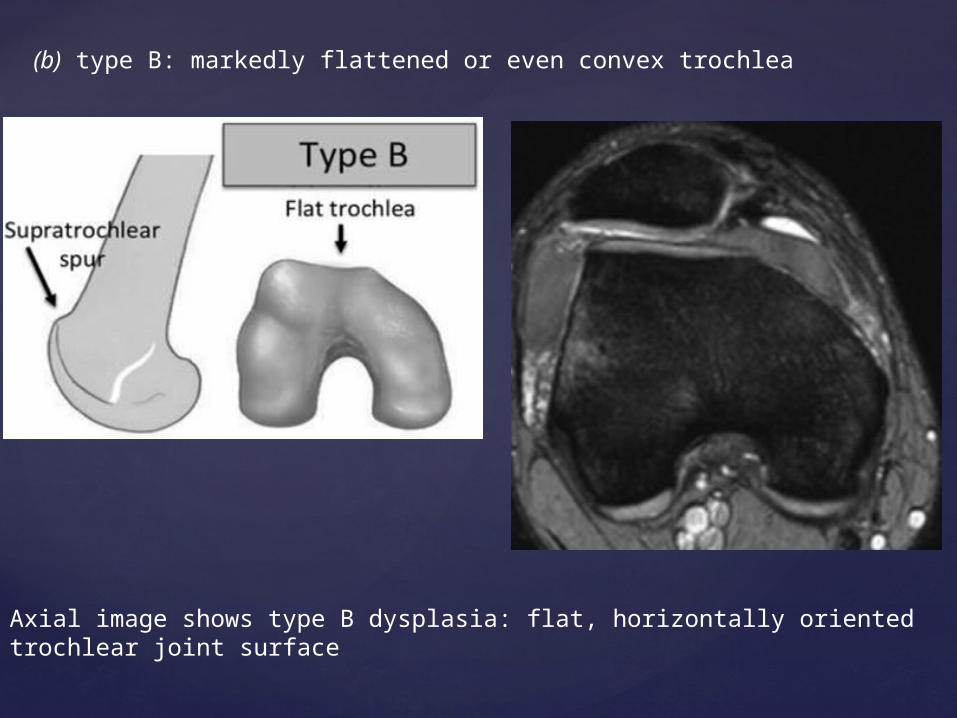
(b) type B: markedly flattened or even convex trochlea
Axial image shows type B dysplasia: flat, horizontally oriented trochlear joint surface

Image shows a normal trochlea, with an inclination angle of 24°
Image shows type B trochlear dysplasia, with an inclination angle of only 7°.

(c) type C: asymmetric trochlear facets, with the lateral facet being too high and the medial facet being hypoplastic, which results in the flattened joint surface forming an oblique plane
Axial image shows type C dysplasia: flat, obliquely oriented trochlear joint surface with facet asymmetry.

(d) type D: in addition to the features of type C, a vertical link between medial and lateral facets (cliff pattern on parasagittal images).
same as type C but with a prominent bone protrusion (arrow) on the parasagittal view (cliff pattern).

Patella Alta
A patella alta, or high-riding patella, is a patella that is too high above the trochlear fossa and occurs when the patellar tendon is too long.
Patella alta is considered a main factor in patellofemoral misalignment because with patella alta, the degree of flexion needs to be higher for the patella to engage in the trochlea, compared with a normal knee.
This problem leads to reduced patellar contact area and decreased bone stability in shallow degrees of flexion.
About 25% of the patients with acute patellar dislocation have a high-riding patella depicted on MR images, and as many as 50% of the patients have a high-riding patella depicted on projection radiographs.
Note, however, that patella alta is a normal anatomic variant that is asymptomatic in most individuals.
Nevertheless, the diagnosis of a high-riding patella is important because it increases the risk of patellar dislocation in conjunction with other factors
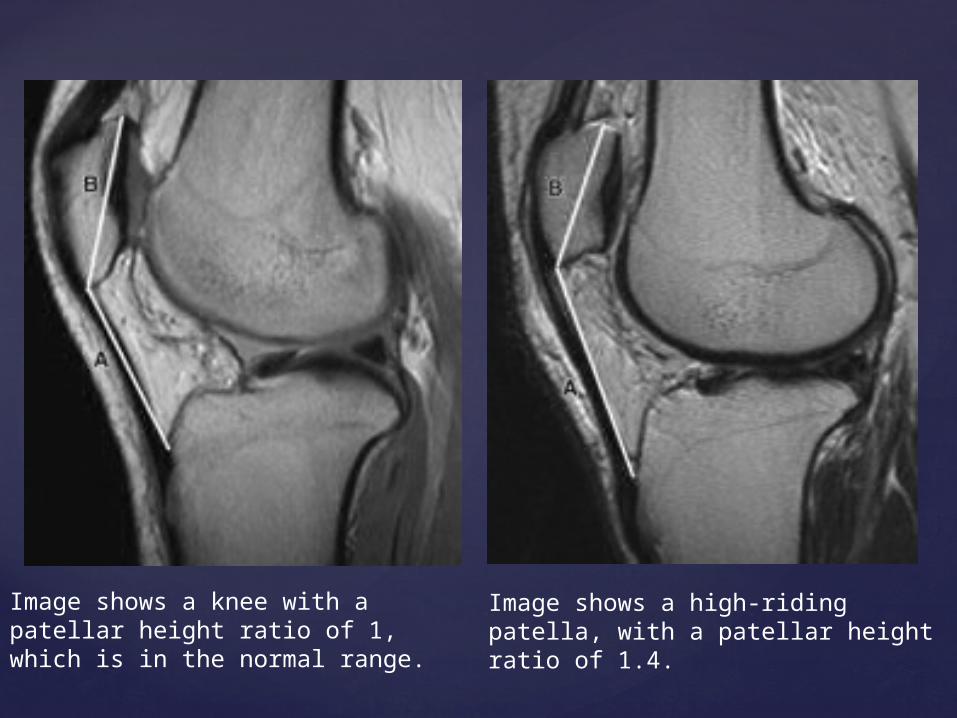
Image shows a knee with a patellar height ratio of 1, which is in the normal range.
Image shows a high-riding patella, with a patellar height ratio of 1.4.
Distance from Tibial Tubercle to Trochlear Groove
The position of the tibial tubercle is crucial for the inferolateral force vector of the patella. In a normal joint, the tibial tuberosity lies vertically under the femoral sulcus, directing the force vector inferiorly during knee bending.
However, if there is excessive lateralization of the tibial tuberosity, the patella is pulled laterally during flexion.
A tibial tubercle–trochlear groove distance of more than 20 mm is nearly always associated with patellar instability. Values of 15–20 mm are considered borderline, less than 15 mm is considered normal.
However, measurement of the lateral distance between the tibial tubercle and the trochlear groove is less accurate in individuals with severe trochlear dysplasia because no deepest point of the trochlea can be defined.
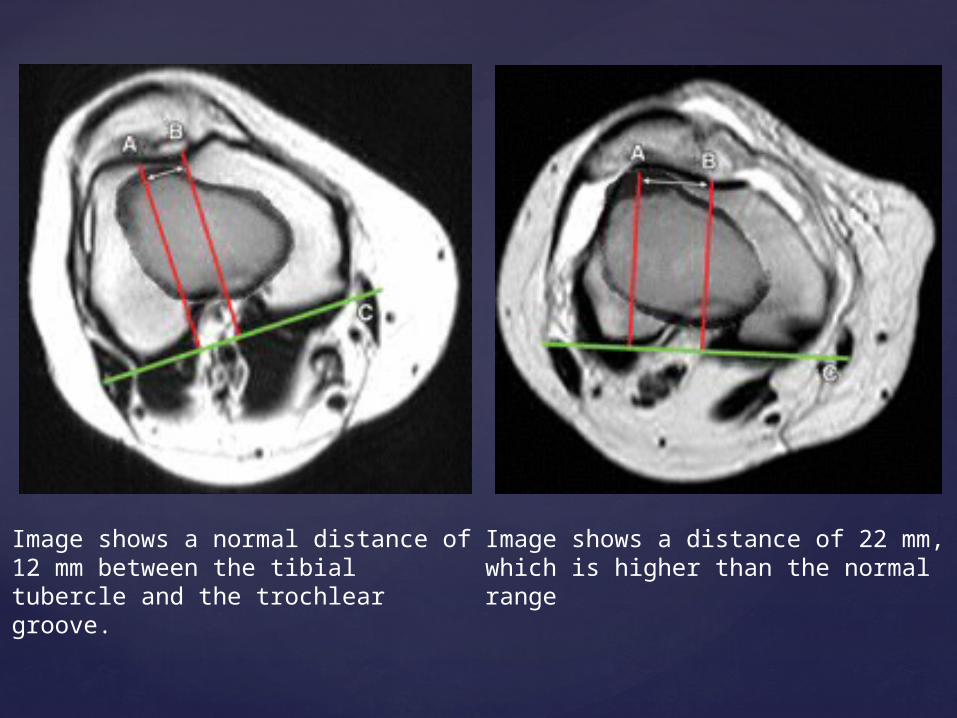
Image shows a normal distance of 12 mm between the tibial tubercle and the trochlear groove.
Image shows a distance of 22 mm, which is higher than the normal range
MR Imaging Findings after Patellar Dislocation
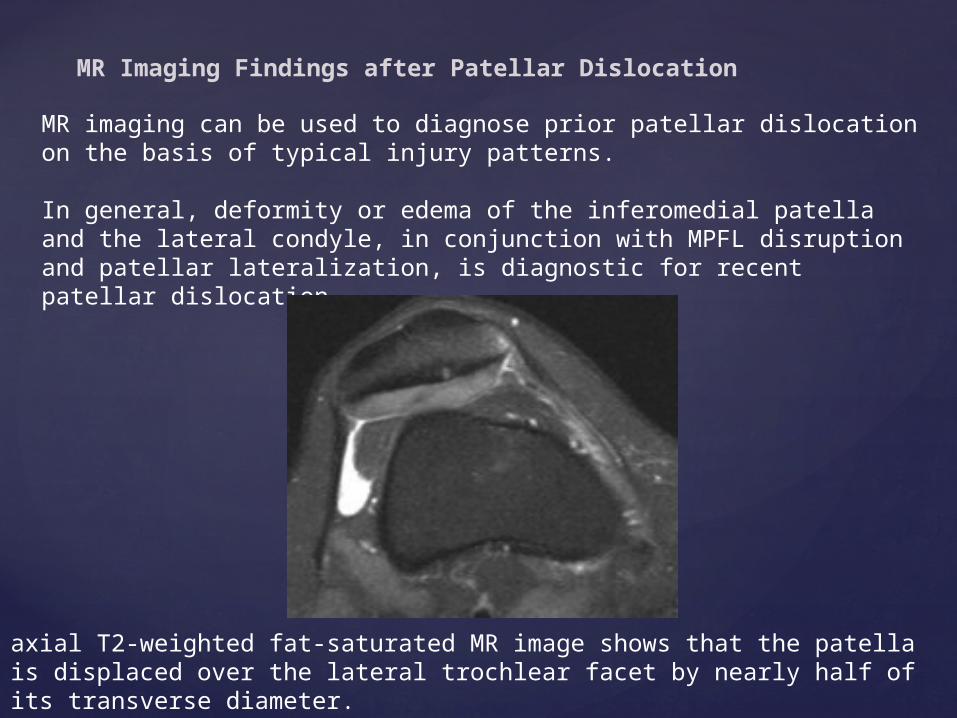
MR imaging can be used to diagnose prior patellar dislocation on the basis of typical injury patterns.
In general, deformity or edema of the inferomedial patella and the lateral condyle, in conjunction with MPFL disruption and patellar lateralization, is diagnostic for recent patellar dislocation.
axial T2-weighted fat-saturated MR image shows that the patella is displaced over the lateral trochlear facet by nearly half of its transverse diameter.
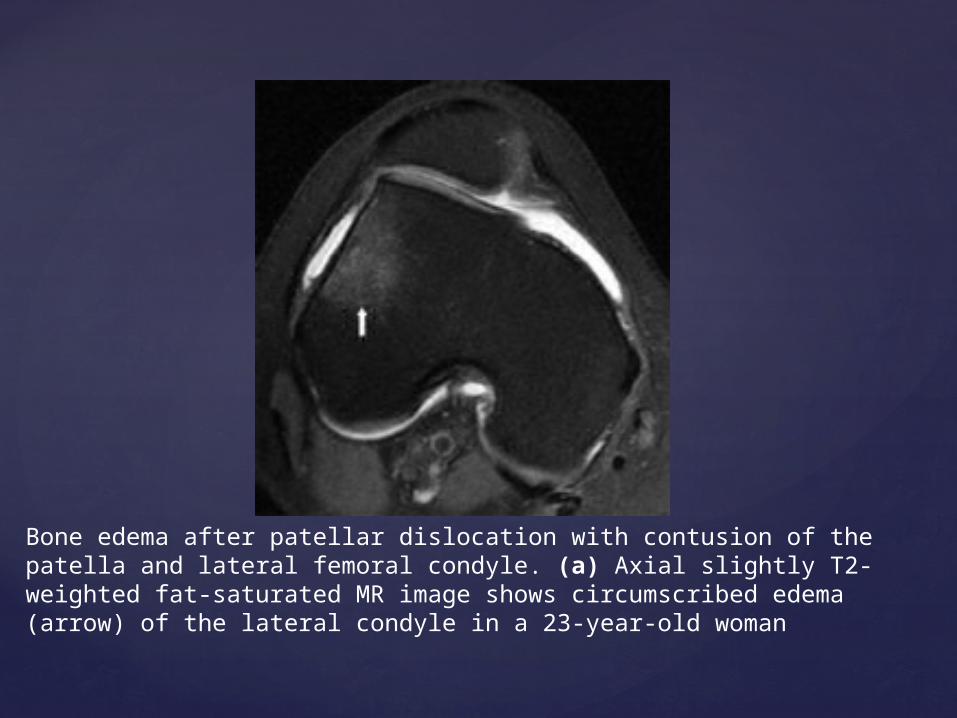
Bone edema after patellar dislocation with contusion of the patella and lateral femoral condyle. (a) Axial slightly T2-weighted fat-saturated MR image shows circumscribed edema (arrow) of the lateral condyle in a 23-year-old woman
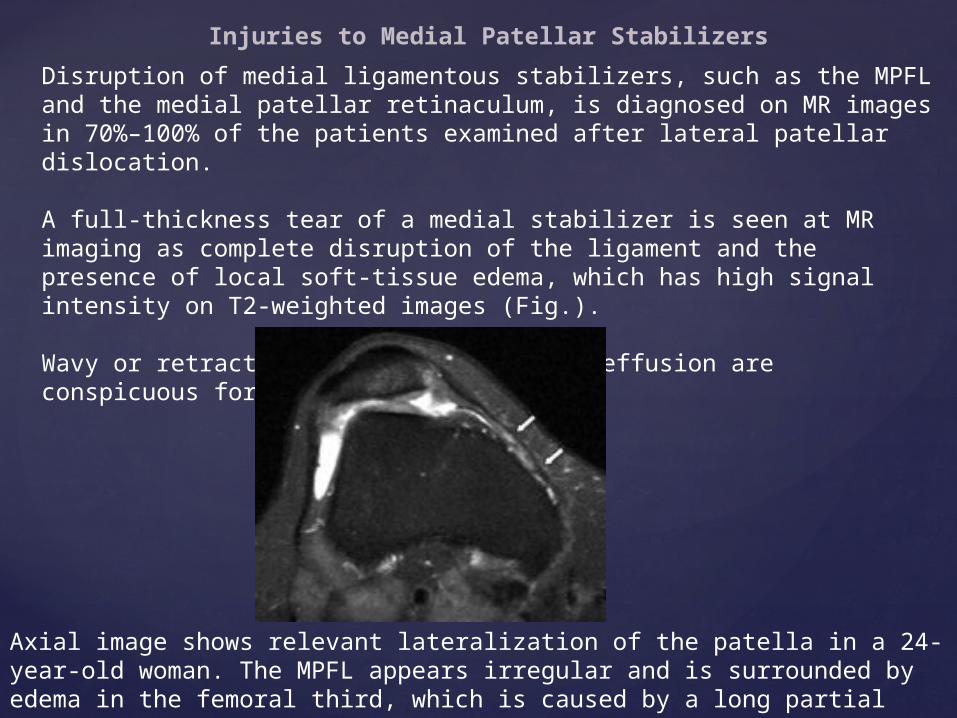
Injuries to Medial Patellar Stabilizers
Disruption of medial ligamentous stabilizers, such as the MPFL and the medial patellar retinaculum, is diagnosed on MR images in 70%–100% of the patients examined after lateral patellar dislocation.
A full-thickness tear of a medial stabilizer is seen at MR imaging as complete disruption of the ligament and the presence of local soft-tissue edema, which has high signal intensity on T2-weighted images (Fig.).
Wavy or retracted fibers surrounded by effusion are conspicuous for complete disruption.
Axial image shows relevant lateralization of the patella in a 24-year-old woman. The MPFL appears irregular and is surrounded by edema in the femoral third, which is caused by a long partial tear (arrows)
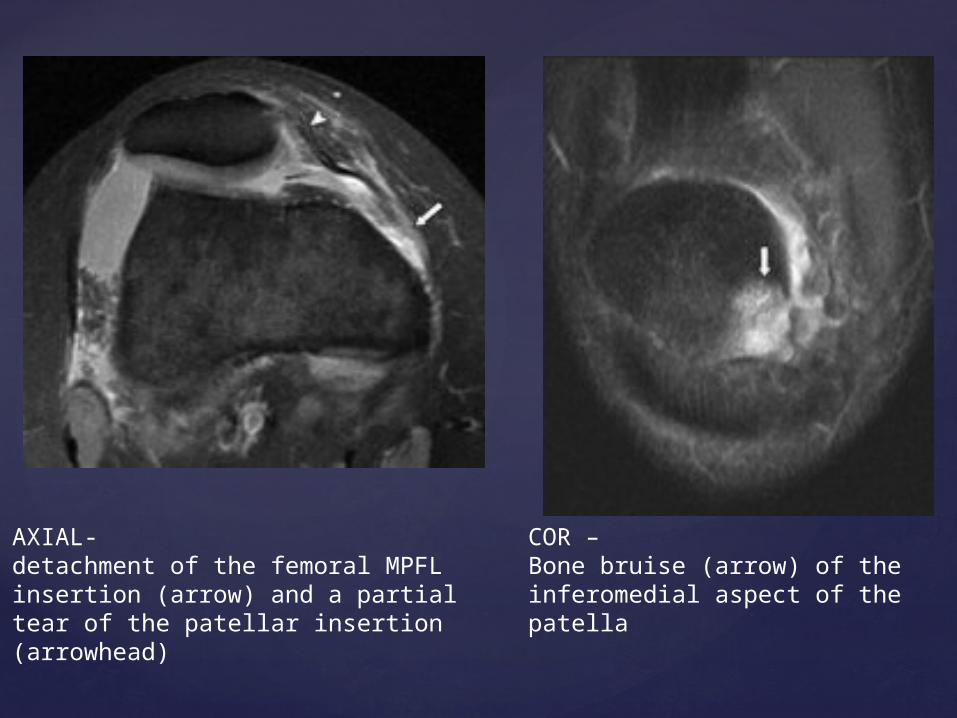
AXIAL- detachment of the femoral MPFL insertion (arrow) and a partial tear of the patellar insertion (arrowhead)
COR – Bone bruise (arrow) of the inferomedial aspect of the patella
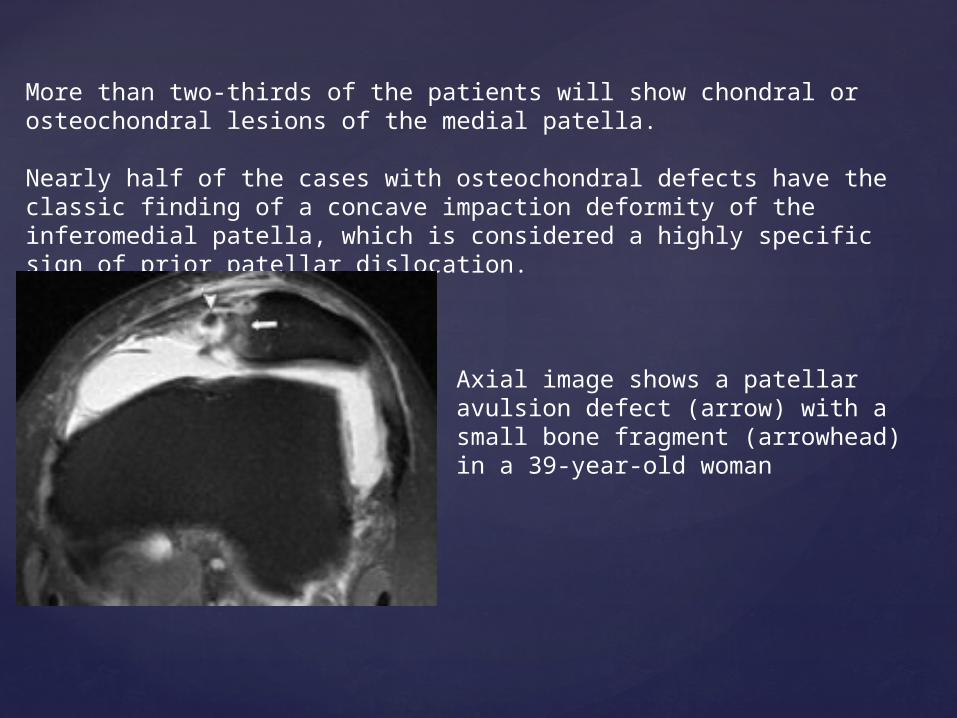
More than two-thirds of the patients will show chondral or osteochondral lesions of the medial patella.
Nearly half of the cases with osteochondral defects have the classic finding of a concave impaction deformity of the inferomedial patella, which is considered a highly specific sign of prior patellar dislocation.
Axial image shows a patellar avulsion defect (arrow) with a small bone fragment (arrowhead) in a 39-year-old woman

Axial image shows a patellar impaction deformity (arrow) resulting from contusion against the lateral condyle
Coronal image of same patient as in b depicts a concave impaction deformity (arrow), which is the severe form of bone impression on the patellar border and is considered a specific sign for prior patellar dislocation
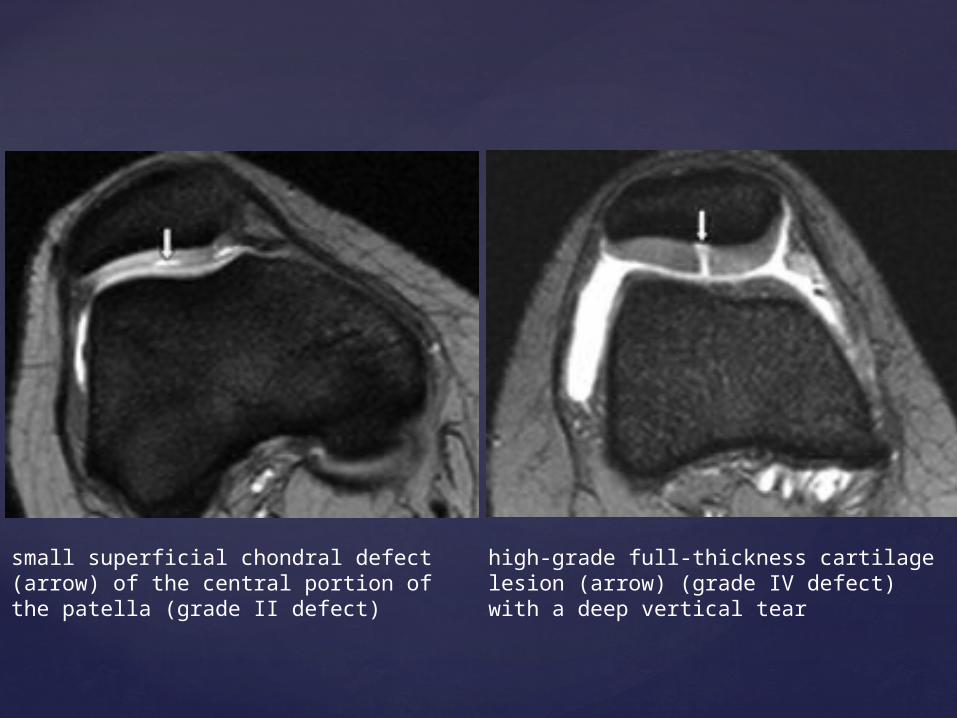
small superficial chondral defect (arrow) of the central portion of the patella (grade II defect)
high-grade full-thickness cartilage lesion (arrow) (grade IV defect) with a deep vertical tear
Thank you