Embed Size (px)
Citation preview

CHAPTER 37
ALTERATIONS IN FUNCTION OF THE GALLBLADDER AND
EXOCRINE PANCREAS

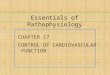
STRUCTURE AND FUNCTION OF THE PANCREATICOBILIARY SYSTEMPancreaticobiliary System• Gallbladder and cystic duct
• Forms a controlled system to deliver bile to intestinal tract
• Gallbladder: distensible sack about 30-50 ml capacity
• Cystic duct: connects with hepatic duct to form common bile duct

STRUCTURE AND FUNCTION OF THE PANCREATICOBILIARY SYSTEM
(CONT.)Pancreaticobiliary System • Intrahepatic, hepatic, and common bile
duct• Common bile duct forms major aqueduct for
digestive secretions to enter intestinal tract• Ampulla of Vater
• 3 inches long• Runs along duodenum; terminates at ampulla of
Vater• Forms terminating point of main pancreatic duct

STRUCTURE AND FUNCTION OF THE PANCREATICOBILIARY SYSTEM
(CONT.)Pancreaticobiliary System • Endocrine and exocrine pancreas
• Pancreatic duct• Runs proximally in pancreas• Branches off dorsally to drain tail of pancreas

STRUCTURE AND FUNCTION OF THE PANCREATICOBILIARY SYSTEM
(CONT.)

EMBRYOLOGY OF THE PANCREATICOBILIARY SYSTEM
3-4 Weeks’ Gestation• Hepatic diverticulum forms from the
primitive foregut• Composed of specialized progenitor liver cells• Eventually forms entire liver, biliary tree, ventral
pancreas• Dorsal pancreas forms from separate outcropping
of cells lying on the opposite side

EMBRYOLOGY OF THE PANCREATICOBILIARY SYSTEM
(CONT.)5 Weeks’ Gestation• Three buds seen in hepatic diverticulum
• Cranial contains hepatoblasts to form liver• Liver sinusoids develops and feed into developing
bile canaliculi• Caudal bud develops into gallbladder

EMBRYOLOGY OF THE PANCREATICOBILIARY SYSTEM
(CONT.)

EMBRYOLOGY OF THE PANCREATICOBILIARY SYSTEM
(CONT.)Second Trimester• Fetus produces bile: gives coloring to the
fetal meconium• Basal bud transforms into the ventral
pancreas

PHYSIOLOGY AND FUNCTION OF BILE FLOW
• Bile produced by hepatocytes in liver; stored in gallbladder• Primary bile acids: choli, chenodeoxycholic acid• Secondary bile acids: deoxycholic acid,
ursodeoxycholic acid, lithocholic acid• Composed primarily of H2O, electrolytes, organic
solute; low protein content• Additional components include pigment
cholesterol phospholipids

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)
Bile Composition• Primarily H2O, electrolytes, organic
solute• Low protein content• Additional components: pigment,
cholesterol, phospholipids

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)
Bile Functions• Aids in digestion of lipids• Transports waste products
• Bilirubin• Immunoglobulins (IgA)• Toxins• Cholesterol

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)
Gallbladder• Concentrates and stores bile• Fasting state
• Muscular sphincter at ampulla of Vater is contracted; promotes flow of bile into gallbladder
• Half of bile stored; half flows into duodenum• Absorption: 90% of H2O in bile absorbed from bile
in 4 hours

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)
• Bile flow (in sequence): 1st morning meal• Hormonally and neurally regulated contraction of
gallbladder releases concentrated bile into duodenum
• Bile acids • Eventually absorbed again in terminal ileum
(2-3 times)• Travel by portal circulation to be secreted again into
the bile• Small amount of pool enters colon (5%); undergo
bacterial transformation into secondary bile salts

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)
Bile Salts• Dual properties
• Digestion• Absorption of fats from small bowel
• Molecules aggregate into clusters• Micelles surround lipids and allow them to go into
solution• Hydrophilic/hydrophobic

PHYSIOLOGY AND FUNCTION OF BILE FLOW (CONT.)

FUNCTIONAL ANATOMY OF THE PANCREAS (CONT.)
• Endocrine pancreas• Insulin• Glucagon• Somatostatin into blood
• Exocrine pancreas• Secretes >1 L of digestive juice into duodenum
every 24 hr

FUNCTIONAL ANATOMY OF THE PANCREAS (CONT.)
Pancreas Components• Lobular; composed of two fused organs
• Dorsal• Ventral
• Pancreatic juices• Active digestive enzymes: amylase, lipase• Precursor or proenzymes: trypsinogen• Release stimulated by cholecystokinin and
secretin

FUNCTIONAL ANATOMY OF THE PANCREAS (CONT.)

DISORDERS OF THE GALLBLADDER
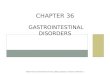
• Cholesterol gallstone formation (cholelithiasis)• Etiology
• 20 million (U.S.)• Incidence
• Native Americans > American Caucasians• Women > men (2:1)
• Risk factors• Age• Sex• Obesity (also rapid weight loss in obese)• Variety of medical factors

DISORDERS OF THE GALLBLADDER (CONT.)
• Cholesterol gallstone formation (cholelithiasis)• Pathophysiology
• Three phases• Supersaturation of bile with cholesterol• Nucleation of crystals• Hypomotility allowing stone growth
• Cholecystitis• Inflammation of the gallbladder wall• Related to continued presence of gallstones

DISORDERS OF THE GALLBLADDER (CONT.)
Signs and Symptoms: ChronicCholelithiasis• Biliary colic
• Precipitated by a meal (infrequent schedule)• Persistent epigastric (right upper abdominal pain)• Often radiates to back• Increases steadily for >15 minutes, lasts several
hours, then slowly decreases• Related to intermittent obstruction of cystic duct
• Nausea, vomiting, sweating, flatus

DISORDERS OF THE GALLBLADDER (CONT.)
Chronic Cholelithiasis• Diagnosis: ultrasound• Treatment
• Watchful waiting• Patients with significant recurrences of biliary colic
• Cholecystectomy• Chemical dissolution of gallstones• Lithotripsy

Disorders of the Gallbladder Disorders of the Gallbladder (Cont.)(Cont.)

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis: Acute Inflammationof the Gallbladder Wall• Etiology
• Cholelithiasis present in 90% of patients• Obstruction of cystic duct present in almost all
patients: related to stasis of bile• Bacterial infection may be present

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • If untreated, escalates; gangrene may occur
• Peritonitis• Septic shock• Localized abscess• Cholecystoenteric fistula (fistula between
gallbladder and GI tract)

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis• Signs and symptoms
• Severe right upper abdominal pain: radiates to back
• Abdominal tenderness• Fever

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • Acalculous cholecystitis
• Occurs in patients without preexisting gallstones• Males >50 years• Rapid development of gangrene, perforation,
emphysematous cholecystitis, and empyema develops rapidly

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • Risks
• Major surgery • Critical illness• Trauma• Burn-related injury

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • Diagnosis
• Abdominal ultrasound• Presence of stones• Thickened gallbladder wall
• HIDA scan• CT• MRCA• ERCP

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • Treatment
• Chemodissolution (nonsurgical): use of bile acids/organic solvents to dissolve gallstone
• Lithotripsy (nonsurgical)• Breaking up of gallstones using shockwaves• Stones <2 cm

DISORDERS OF THE GALLBLADDER (CONT.)
Acute Cholecystitis • Treatment
• Cholecystectomy: mainstay of therapy• Antibiotics (if bacterial infection)• Advanced acute cholecystitis complicated by
gangrene, empyema, or emphysematous changes is a surgical emergency

DISORDERS OF THE GALLBLADDER (CONT.)
Chronic Cholecystitis: ChronicInflammation of Gallbladder Wall • Related to persistent low-grade irritation
from gallstones• Related to recurrent attacks of acute
cholecystitis• Predisposing factors
• Diabetes mellitus• Obesity

DISORDERS OF THE GALLBLADDER (CONT.)
Chronic Cholecystitis • Signs and symptoms
• Asymptomatic• Leads to complications
• Biliary sepsis• Scarring (porcelain gallbladder)

DISORDERS OF THE PANCREAS (CONT.)
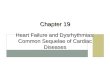
Acute Pancreatitis• Etiology: 1-5:10,000 in U.S. annually• Predisposing factors• Biliary tract disease
• Hypertriglyceridemia• Ethanol-associated (66%)
• Secretion of protein-rich pancreatic fluid• Deposition of inspissated protein plugs• Obstruction of small pancreatic ducts

DISORDERS OF THE PANCREAS (CONT.)

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Signs and Symptoms• Steady, boring pain in epigastrium or LUQ
• Increases in intensity• Severe tenderness on palpation• Radiates or penetrates to back• Accompanied by nausea and vomiting
• Abdominal distention• Hypoactive or absent bowel tones
• Low-grade fever

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Diagnosis• Laboratory
• Increase in amylase and lipase during first 12 hr• Remain elevated for several days• Lipase preferred test
• Elevated aminotransferases• Elevated alkaline phosphatase and
bilirubin• Leukocytosis• Hyperlipidemia• Hypocalcemia

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Diagnosis • Abdominal x-ray
• Ileus pattern• “Sentinel loop”: distended loop of small bowel in
area of pancreas• Abdominal ultrasound

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Diagnosis • CT of abdomen
• Gold standard and allows remarkable detail: edema, abscess, cyst formation
• Prognostic assessment: Ranson’s criteria

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Differential Diagnosis
• Perforated peptic ulcer• Acute cholecystitis• Mesenteric vascular disease

DISORDERS OF THE PANCREAS (CONT.)

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Treatment• Mild to moderate
• Conservative management• Withhold oral feedings• Nasogastric suction for adynamic ileus• IV fluid replacement• Analgesics

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Treatment • Severe
• Nutritional replacement: prevents tissue breakdown
• Calcium and magnesium administration• Control of hyperglycemia• Prevent respiratory, ARF, intraabdominal sepsis• Bacterial infection

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Treatment • Surgical intervention (abscess or
hemorrhage)• Necrosectomy: debridement of devitalized tissue• Pancreatectomy: major pancreatic resection

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Complications• Pseudocyst: collection of fluid within or
adjacent to pancreas• Signs and symptoms
• Fever• Tachycardia• Abdominal mass and tenderness
• Management: endoscopic or surgical drainage

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Complications • Pancreatic ascites: persistent leak in
pancreatic duct into pleural space and mediastinum• Signs and symptoms: painless and massive• Treatment
• Ultrasound• CT• Fluid analysis obtained by aspiration

DISORDERS OF THE PANCREAS (CONT.)
Acute Pancreatitis: Complications • Pancreatic ascites: management
• Prolonged parenteral nutrition• Endoscopic placement of a stent into main pancreatic
duct• Common bile duct obstruction• Portal or splenic vein thrombosis• Peptic ulcer disease• Chronic fistula formation

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Etiology• Mortality (3%-4% yearly)• Predisposing factors
• ETOH consumption• Idiopathic• Hereditary• Hyperparathyroidism (hypercalcemia)• Trauma

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Pathophysiology • Presence of chronic inflammatory lesions in
pancreas• Key element: necrosis followed by fibrosis• Persistence of symptoms secondary to
pancreatic dysfunction over weeks and months

DISORDERS OF THE PANCREAS (CONT.)
• Destruction of exocrine parenchyma and fibrosis• Precedes destruction of endocrine parenchyma• Leads to calcification

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Pathophysiology • Increase in protein concentration in
pancreatic juice with reduction in “pancreatic stone protein” (inhibits formation of pancreatic protein plugs)• Leads to calcification—obstruction in flow of
pancreatic juice

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Signs andSymptoms• Bouts of acute pancreatitis with progressive
signs of persistent pancreatic dysfunction• Insidious onset of epigastric pain radiating
to back (first symptom)• No pain but sequelae of chronic
pancreatitis(10%-15%)

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Signs andSymptoms • Endocrine and exocrine pancreatic
insufficiency• Diabetes: progressive loss of endocrine cells in
pancreatic islets• Malabsorption
• Pancreatic enzyme output <10% of normal• Impairment of vitamins A, D, E, and K
• Weight loss: poor intake related to pain

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Complications• Pseudocyst• Pancreatic ascites• Obstruction of common bile duct: surgical
or endoscopic intervention• Thrombosis of portal and splenic veins may
lead to GI hemorrhage related to gastric varices
• Peptic ulcer disease

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Diagnosis• History• Physical examination• Laboratory: elevated LFTs, alkaline
phosphatase, and bilirubin levels• Abdominal x-ray• CT• ERCP: suspicious cases unconfirmed with
other tests

DISORDERS OF THE PANCREAS (CONT.)

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Treatment• Pain control
• Absolute abstention from alcohol• Analgesics• Surgical intervention• Celiac plexus block
• Pancreatic sphincterotomy: management of single or multiple stones

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Treatment • Pseudocysts (adjacent to stomach or
duodenum): endoscopic drains• Obstruction of bile duct or main pancreatic
duct: biliary/pancreatic stents• Whipple procedure
(pancreaticoduodenectomy)

DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Treatment• Management of endocrine/exocrine
insufficiency• Low-fat diet• Pancreatic enzyme supplementation• Oral hypoglycemic agents/insulin

Elsevier items and derived items © 2010, 2005 by Saunders, an imprint of Elsevier Inc.
DISORDERS OF THE PANCREAS (CONT.)
Chronic Pancreatitis: Treatment• Pancreatic enzyme replacement
• Steatorrhea control• Chronic pain management• 20%-30% ETOH-induced disease respond to therapy• Medications
• H2 blocker• Proton pump inhibitor