Embed Size (px)
Citation preview
PrednisonePrepared by: Abdulaziz Thaer Aziz, RN
Email: [email protected]
Directed by: Dr. Heba Khader, Ph.D., Pharmacist
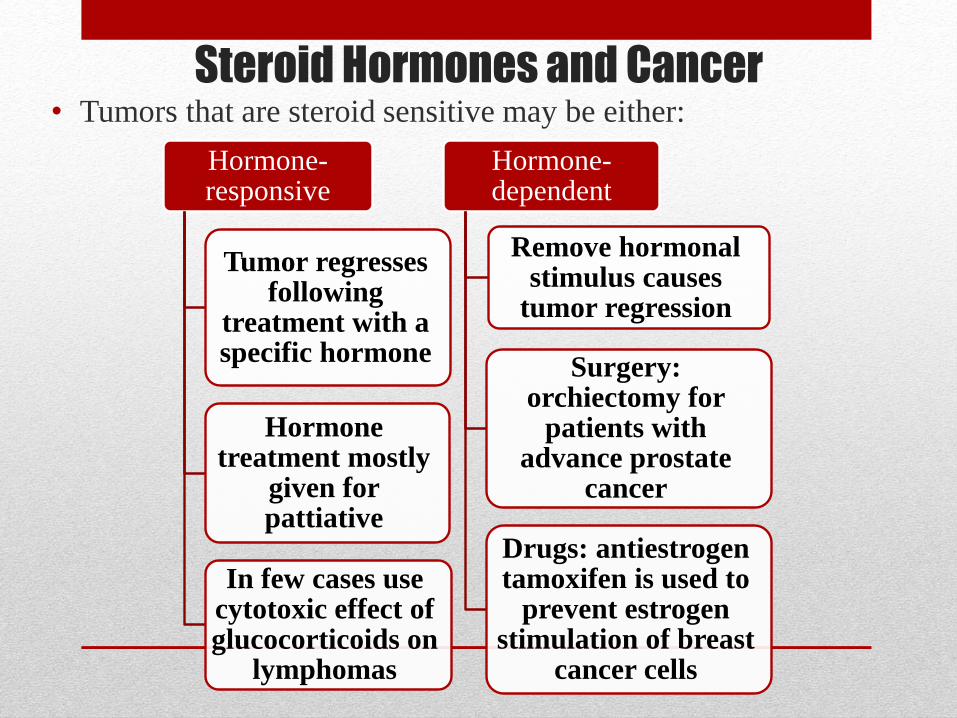
Steroid Hormones and Cancer• Tumors that are steroid sensitive may be either:
Hormone-responsive
Tumor regresses following
treatment with a specific hormone
Hormone treatment mostly
given for pattiative
In few cases use cytotoxic effect of glucocorticoids on
lymphomas
Hormone-dependent
Remove hormonal stimulus causes
tumor regression
Surgery: orchiectomy for
patients with advance prostate
cancer
Drugs: antiestrogentamoxifen is used to
prevent estrogen stimulation of breast
cancer cells

• Prednisone is an oral, naturally-occurring corticosteroid
produced in the body by the cortex of adrenal glands. It
mimics the action of cortisol (hydrocortisone) with less
mineralocorticoid activity than cortisol.
• Corticosteroids have many effects on the body, but the
most common are used for their potent anti-
inflammatory effects on immune system (arthritis,
colitis and asthma).
• It was observed that patients with cushing syndrome
have lymphocytopenia and decreased lymphoid mass.
This result from corticosteroid action on lymphocyte
formation and distribution, that is, movement of these
cells from the circulation to lymphoid tissue.
Mechanism of Action
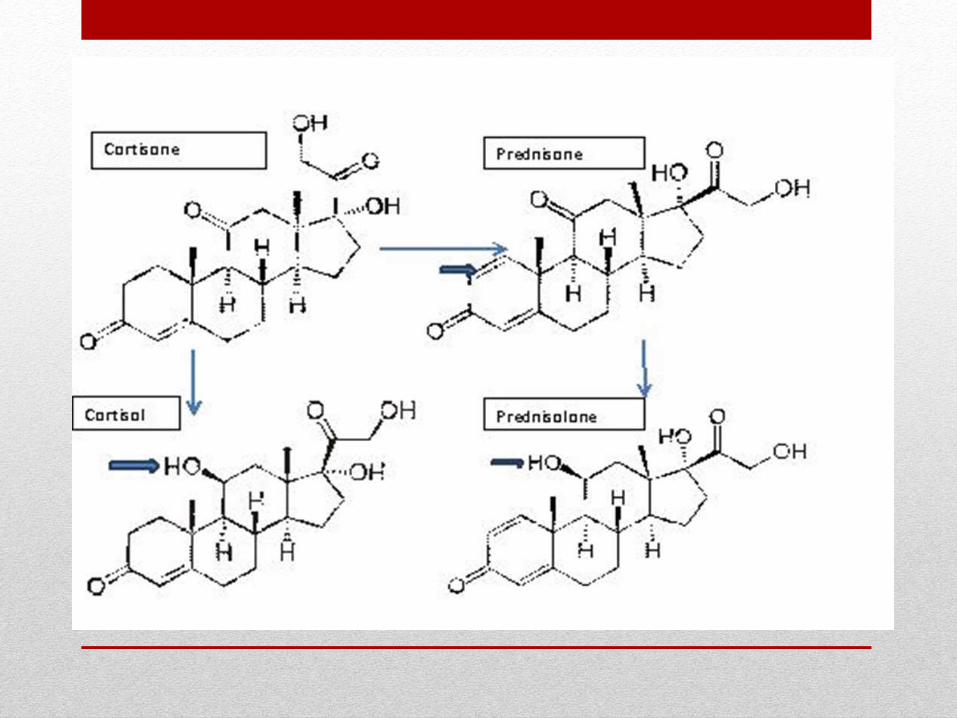
• Prednisone itself is inactive and must first be preduced to
predinsolone by 11-β-hydroxysteroid dehydrogenase. The
steroid binds to a receptor that triggers the production of specific
protein.
• Glucocorticoids are naturally occurring hormones that prevent
or suppress inflammation and immune responses when
administered at pharmacological doses. At a molecular level,
unbound glucocorticoids readily cross cell membranes and bind
with high affinity to specific cytoplasmic receptors. This binding
induces a response by modifying transcription and, ultimately
protein synthesis to achieve the steroid's intended action.

Mechanism of Action• Such actions may include: inhibition of leukocyte infiltration at the site
of inflammation, interference in the function of mediators of
inflammatory response, and suppression of humeral immune
responses. Some of the net effects include reduction in edema or scar
tissue, as well as a general suppression in immune response. The
degree of clinical effect is normally related to the dose administered.
• The anti-inflammatory actions of corticosteroids are thought to involve
phospholipase A2 inhibitory proteins, collectively called lipocortins.
Lipocortins, in turn, control the biosynthesis of potent mediators of
inflammation such as prostaglandins and leukotrienes by inhibiting the
release of the precursor molecule arachidonic acid. Likewise, the
numerous adverse effects related to corticosteroid use are usually
related to the dose administered and the duration of therapy.
• Resistance is associated with an absence of
the receptor protein or a mutation that
lowers receptor affinity for the hormone.
However, some resistant cells appear to
have functional receptors, but some
subsequent step(s) is affected.
Pharmacokinetics• Prednisone is rapidly absorbed across the GI membrane
following oral administration. Peak effects can be observed after
1-2 hours. The circulating drug binds extensively to the plasma
proteins albumin and transcortin, with only the unbound portion
of a dose active.
• Systemic prednisone is quickly distributed into the kidneys,
intestines, skin, liver and muscle. Corticosteroids distribute into
the breast milk and cross the placenta. Prednisone is metabolized
by the liver by microsomal oxidizing enzymes to the active
metabolite prednisolone (caution with hepatic dysfunction ),
which is then further metabolized to inactive compounds.
• These inactive metabolites, as well as a small portion of
unchanged drug, are excreted in the urine.
Indications• Remission of acute lymphocytic leukemia
• Chronic lymphocytic leukemia
• Hodgkin's and non-Hodgkin's lymphomas
• Mycosis fungoides
• Congenital adrenal hyperplasia
• Replacement therapy for primary adrenocortical insufficiency (Addison's disease)
• Replacement therapy for secondary or tertiary adrenocortical insufficiency (defect either in CRF production by hypothalamus or corticotropinproduction by pituitary)
• Relief of inflammatory symptoms
• Treatment of allergies
• thrombocytopenia
• Nervous system: acute exacerbations of multiple sclerosis
• Edematous state: to induce a diuresis or remission of proteinuria in the nephrotic syndrome
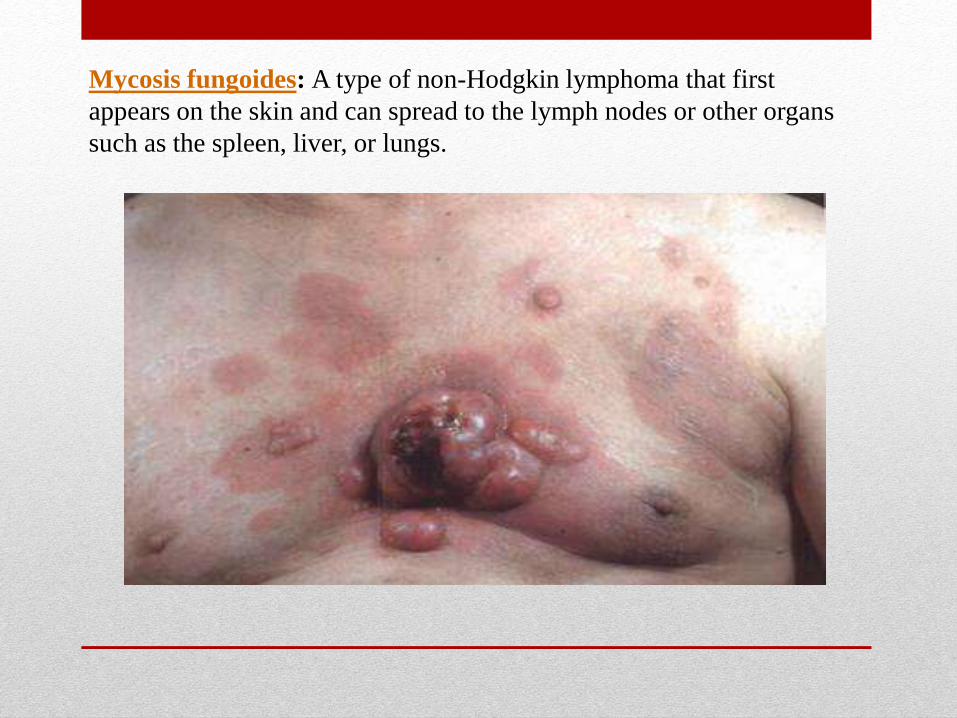
Mycosis fungoides: A type of non-Hodgkin lymphoma that first
appears on the skin and can spread to the lymph nodes or other organs
such as the spleen, liver, or lungs.

Withdrawal• Withdrawal from the drugs can be a serous problem, because if
the patient Withdrawal from these drugs can be a serious
problem because, if the patient has experienced hypothalamic-
pituitary-adrenal-suppression, abrupt removal of the
corticosteroids causes an acute adrenal insufficiency syndrome
that can be lethal.
• This risk, coupled with the possibility of psychological
dependence on the drug and the fact that withdrawal might
cause an exacerbation of the disease, means the dose must be
tapered according to the individual, possibly through trial and
error. The patient must be monitored carefully.

Prednisone: Nursing Diagnoses and Outcomes
• Excess Fluid Volume related to sodium and water retention secondary to corticosteroid therapy• Desired outcome: The patient will
relate causative factors and methods of preventing edema and exhibit decreased peripheral and sacral edema.
• Risk for Infection or Risk for Injury related to anti-inflammatory, immunosuppressive, dermatologic, and metabolic effects of chronic corticosteroid therapy• Desired outcome: The patient
will demonstrate knowledge of risk factors associated with potential for infection or injury and will practice appropriate precautions for prevention.
• Imbalanced nutrition: More than Body Requirements related to increased appetite secondary to corticosteroid medications• Desired outcome: The
patient will maintain a healthy weight, discuss current nutritional needs, and discuss the effects of exercise on weight control.
• Altered Body Image related
to cushingoid characteristics
or physical changes
secondary to glucocorticoid
therapy
• Desired outcome: The
patient will verbalize and
demonstrate acceptance
of appearance, verbalize
and demonstrate healthy
adaptation and coping
skills.
Prednisone: Planning and Interventions
• Maximizing therapeutic effects
• The most opportune time for administration of daily doses or
alternate-day doses of glucocorticoids is early in the morning.
• Minimizing adverse effects
• Monitor the patient, especially the surgical patient, carefully for
signs of infection.
• Administration can lead to peptic ulcer disease.
Prednisone: Teaching, Assessment, and Evaluations
• Patient and family education
• Discuss taking the drug exactly as prescribed.
• Discuss not stopping the drug abruptly.
• Emphasize the importance of patients’ notifying all health care
providers about glucocorticoid therapy.
• Ongoing assessment and evaluation
• Monitor for therapeutic drug response, adverse drug reactions, and
indications of drug toxicity.





























