Embed Size (px)
Citation preview
Research biopsies and
translational research
protocol participation
Jennifer A. Wargo, MD, MMSc
Departments of
Surgical Oncology & Genomic Medicine
Melanoma Research Foundation
Understanding Melanoma:
From Prevention to Cure
Houston, TX
January 31, 2015
Targeted therapy
Immunotherapy
• Cancer is a disease of the DNA
• Genetic mutations may result in the development of cancer
• These genetic mutations can lead to increased growth and spread of tumors
• Targeting these mutations may allow us to stop the cancer cells from growing and spreading and may kill the tumor cells (BRAF gene)
Targeted Therapy for Melanoma
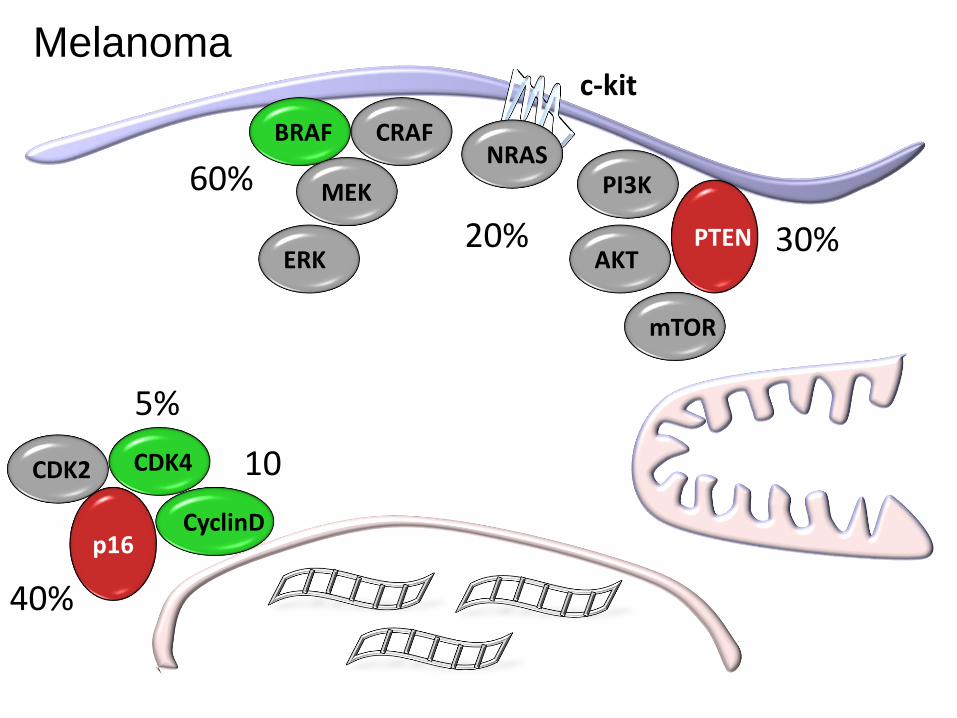
CRAFBRAF
PI3KMEK
AKT
mTOR
CDK2 CDK4
PTEN
p16CyclinD
60%
c-kit
30% 20%
5%
40%
10%
NRAS
ERK
Melanoma
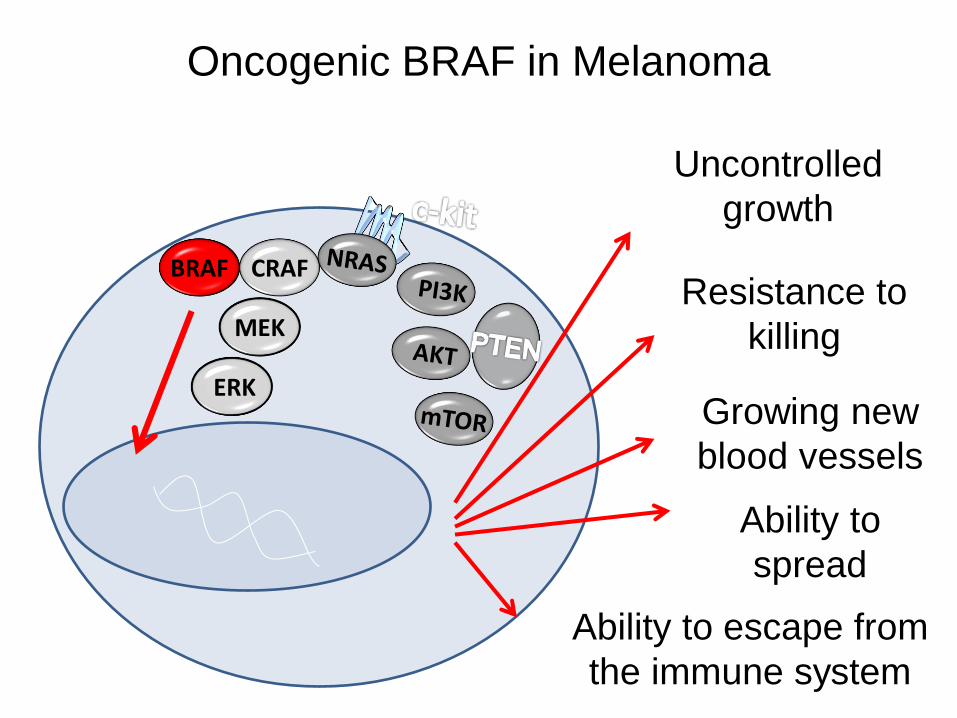
Oncogenic BRAF in Melanoma
CRAFBRAF
MEK
ERK
BRAF
Uncontrolled
growth
Resistance to
killing
Growing new
blood vessels
Ability to
spread
Ability to escape from
the immune system
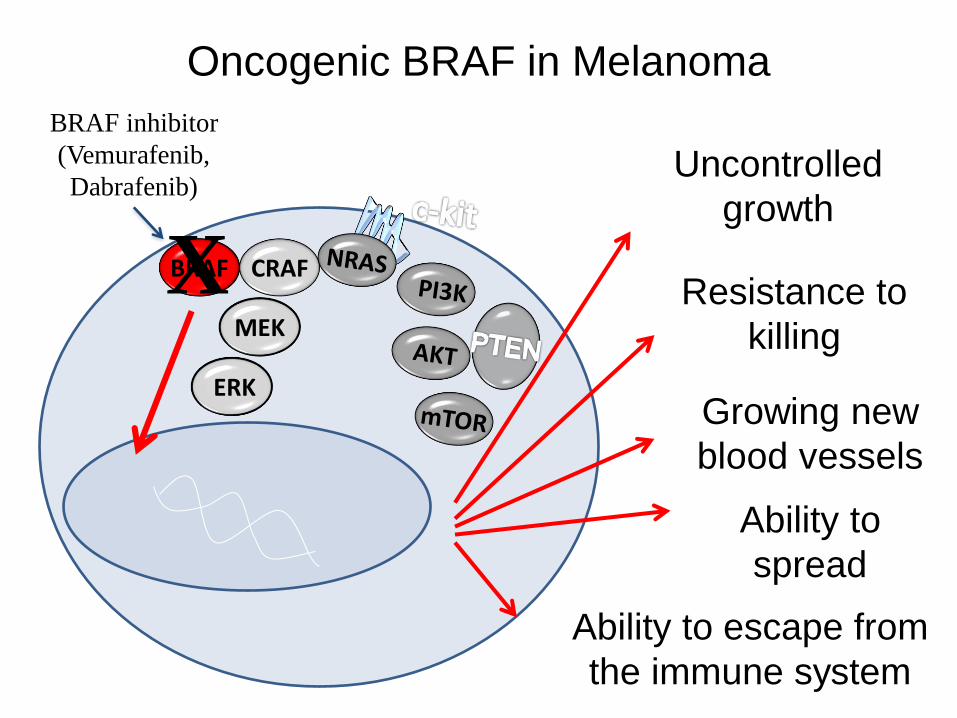
Oncogenic BRAF in Melanoma
CRAFBRAF
MEK
ERK
BRAF
Uncontrolled
growth
Resistance to
killing
Growing new
blood vessels
Ability to
spread
Ability to escape from
the immune system
X
BRAF inhibitor
(Vemurafenib,
Dabrafenib)
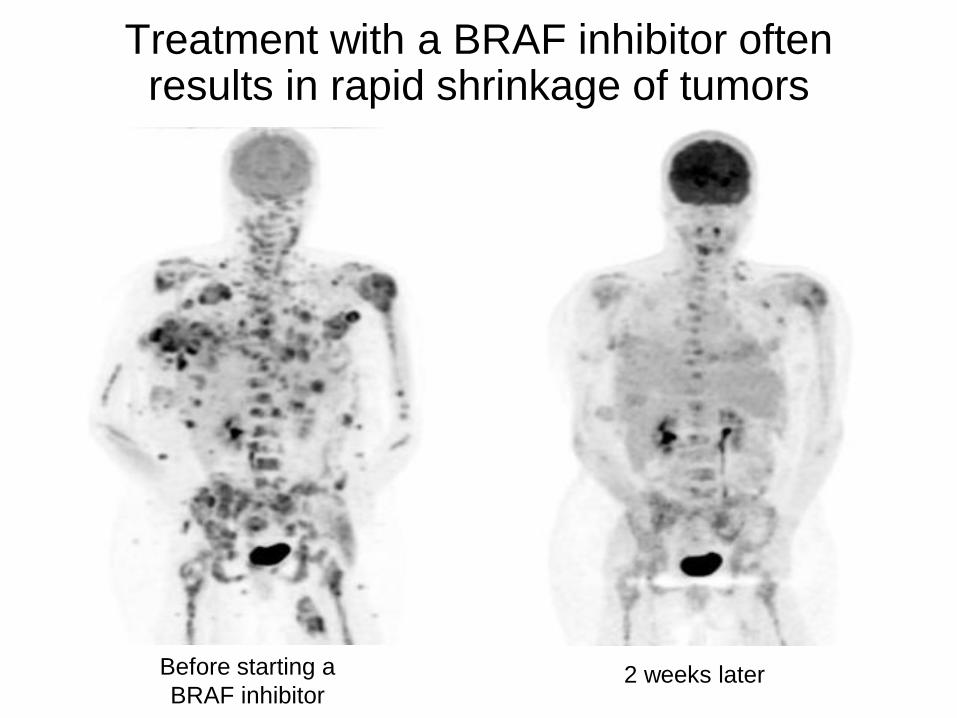
Treatment with a BRAF inhibitor often results in rapid shrinkage of tumors
Before starting a
BRAF inhibitor 2 weeks later
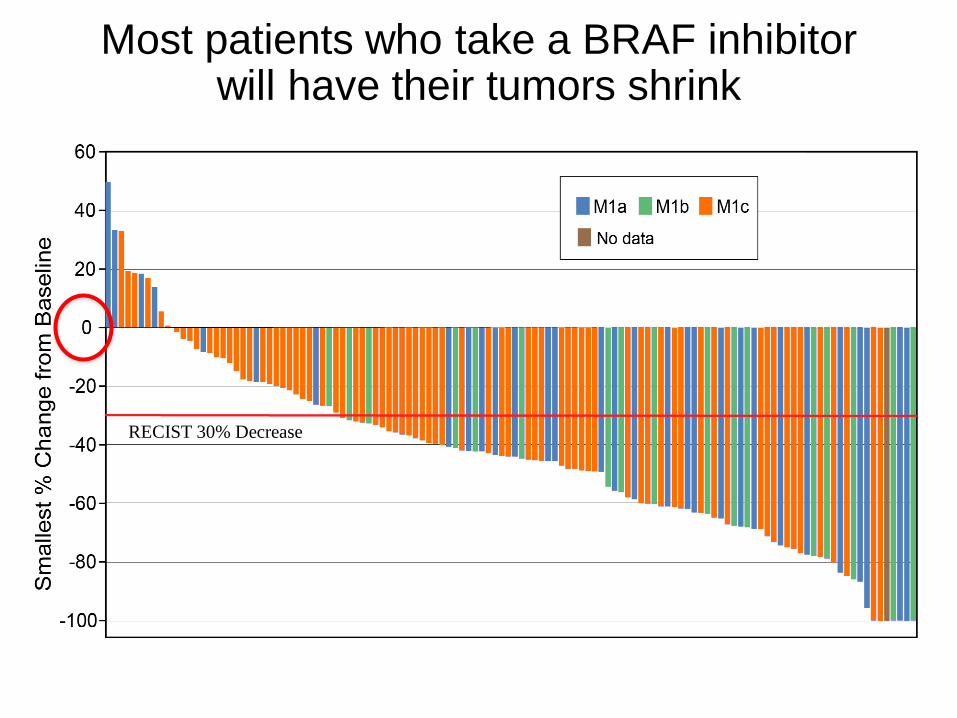
RECIST 30% Decrease
Most patients who take a BRAF inhibitor will have their tumors shrink
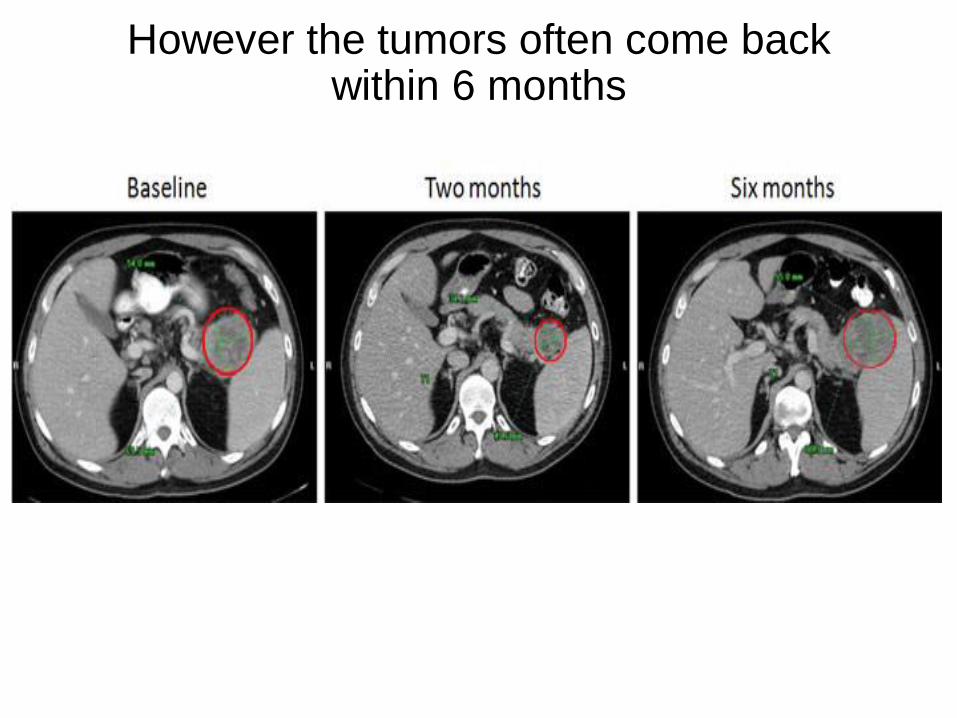
However the tumors often come back within 6 months
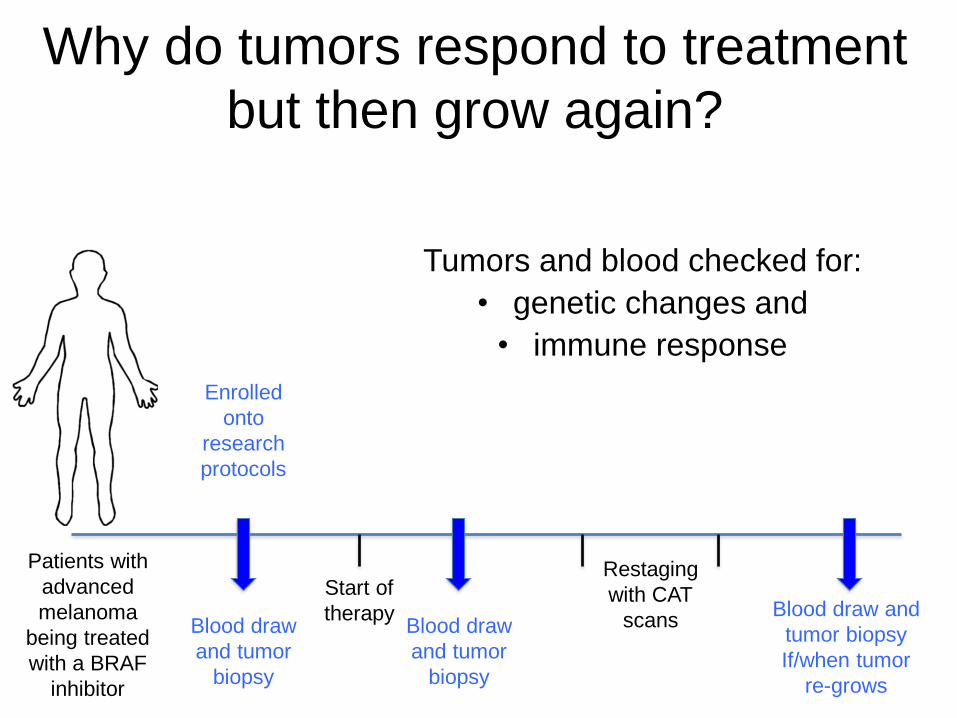
Why do tumors respond to treatment
but then grow again?
Patients with
advanced
melanoma
being treated
with a BRAF
inhibitor
Enrolled
onto
research
protocols
Blood draw
and tumor
biopsy
Start of
therapy Blood draw
and tumor
biopsy
Restaging
with CAT
scansBlood draw and
tumor biopsy
If/when tumor
re-grows
Tumors and blood checked for:
• genetic changes and
• immune response
CRAFBRAF
PI3KMEK
AKT
mTOR
CDK2 CDK4
PTEN
p16CyclinD
NRAS
ERK
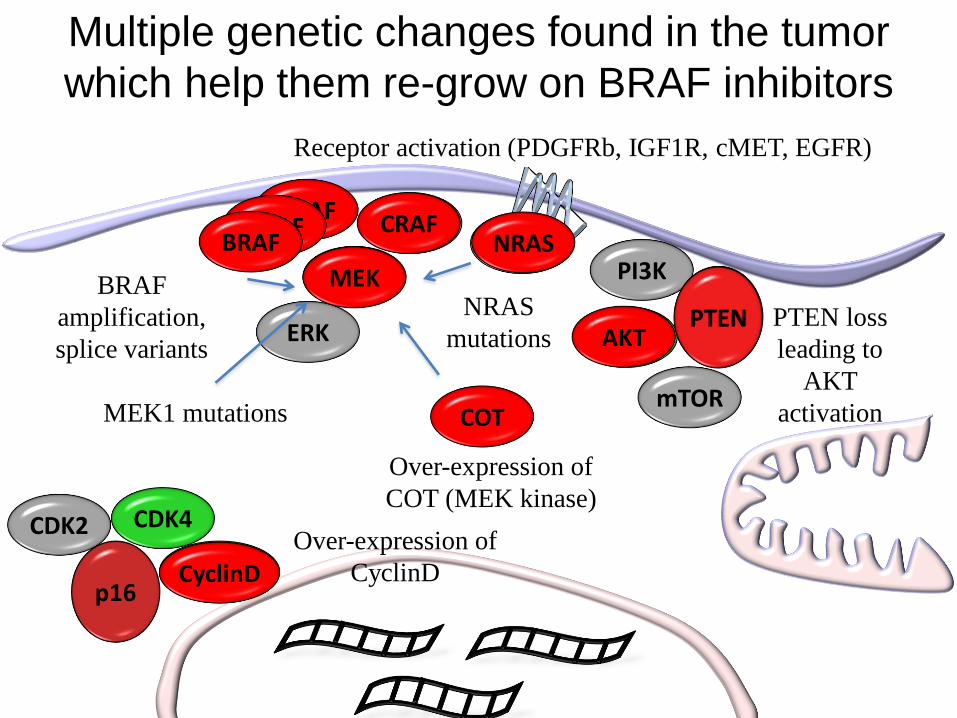
Multiple genetic changes found in the tumor
which help them re-grow on BRAF inhibitors
BRAFBRAF
BRAF
amplification,
splice variants
NRAS
NRAS
mutations
COT
CRAF
Over-expression of
COT (MEK kinase)
Receptor activation (PDGFRb, IGF1R, cMET, EGFR)
MEK1 mutations
CyclinDOver-expression of
CyclinD
PTENAKT
PTEN loss
leading to
AKT
activation
MEK
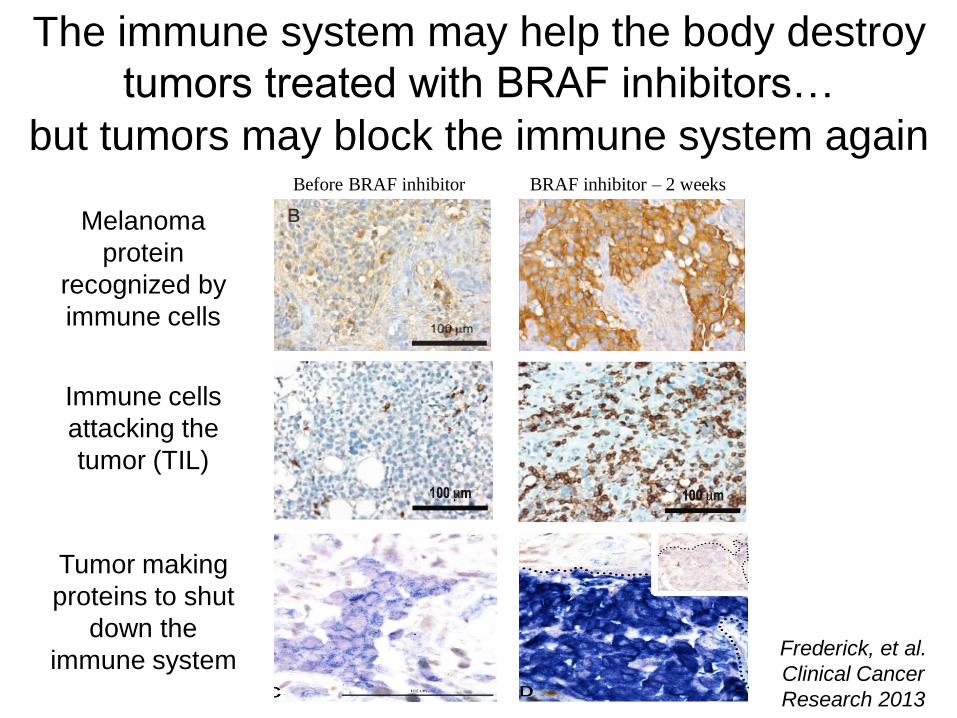
Frederick, et al.
Clinical Cancer
Research 2013
Melanoma
protein
recognized by
immune cells
The immune system may help the body destroy
tumors treated with BRAF inhibitors…
Immune cells
attacking the
tumor (TIL)
Tumor making
proteins to shut
down the
immune system
Before BRAF inhibitor BRAF inhibitor – 2 weeks
but tumors may block the immune system again
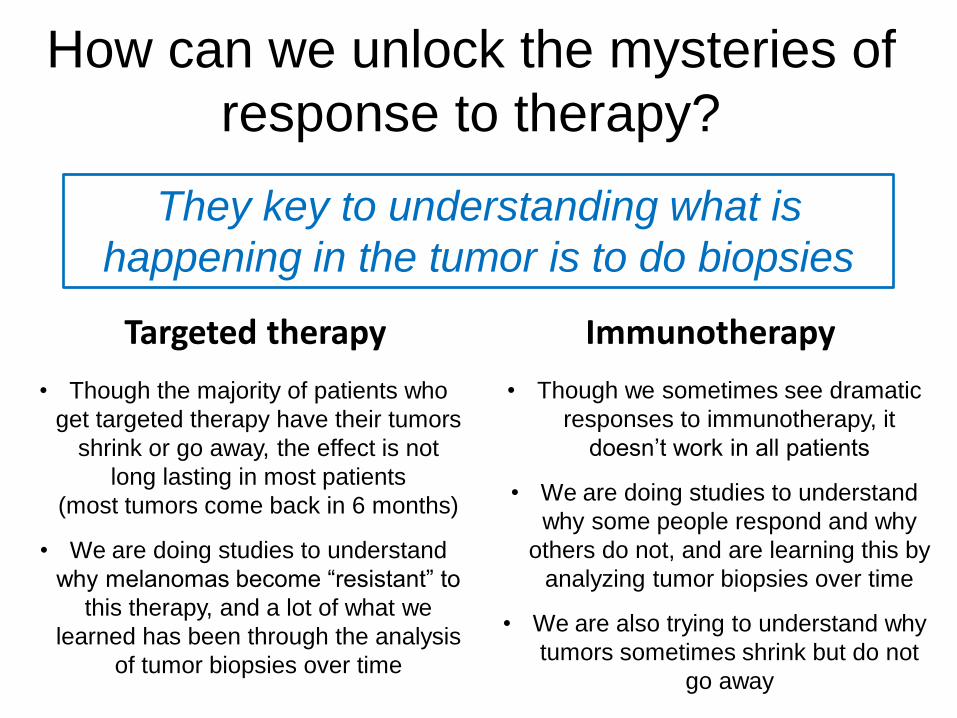
Targeted therapy
• Though the majority of patients who
get targeted therapy have their tumors
shrink or go away, the effect is not
long lasting in most patients
(most tumors come back in 6 months)
• We are doing studies to understand
why melanomas become “resistant” to
this therapy, and a lot of what we
learned has been through the analysis
of tumor biopsies over time
Immunotherapy
• Though we sometimes see dramatic
responses to immunotherapy, it
doesn’t work in all patients
• We are doing studies to understand
why some people respond and why
others do not, and are learning this by
analyzing tumor biopsies over time
• We are also trying to understand why
tumors sometimes shrink but do not
go away
How can we unlock the mysteries of
response to therapy?
They key to understanding what is
happening in the tumor is to do biopsies
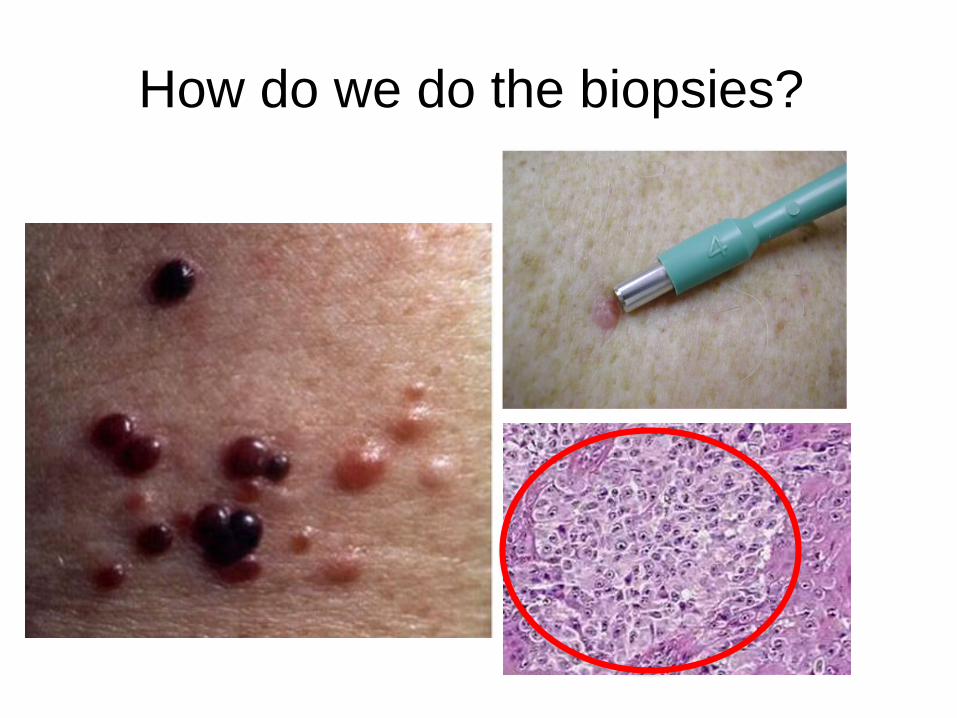
How do we do the biopsies?
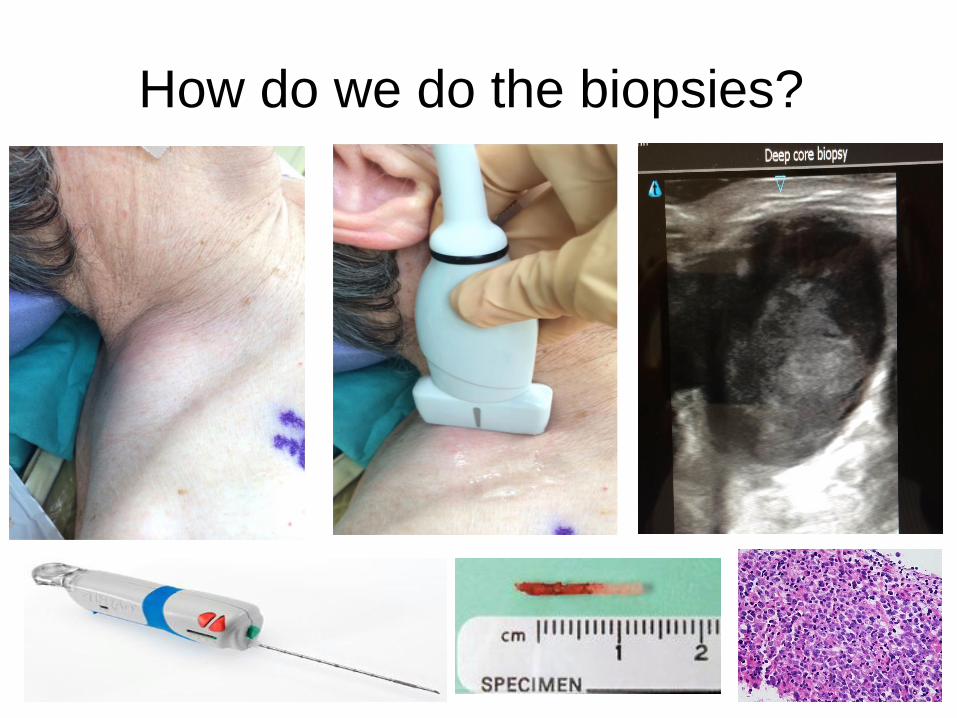
How do we do the biopsies?
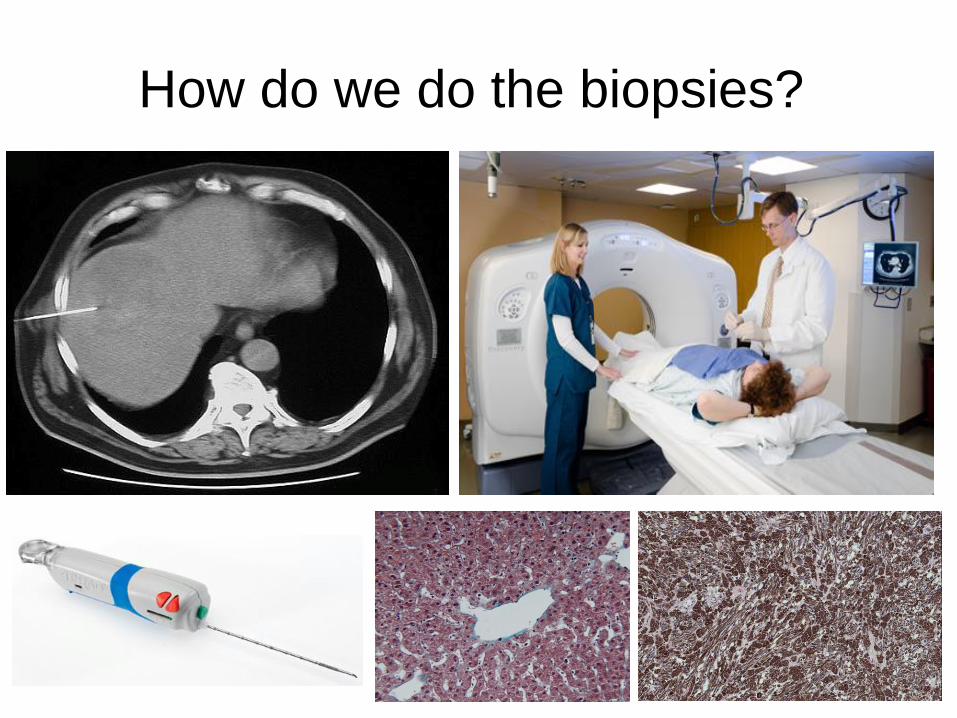
How do we do the biopsies?
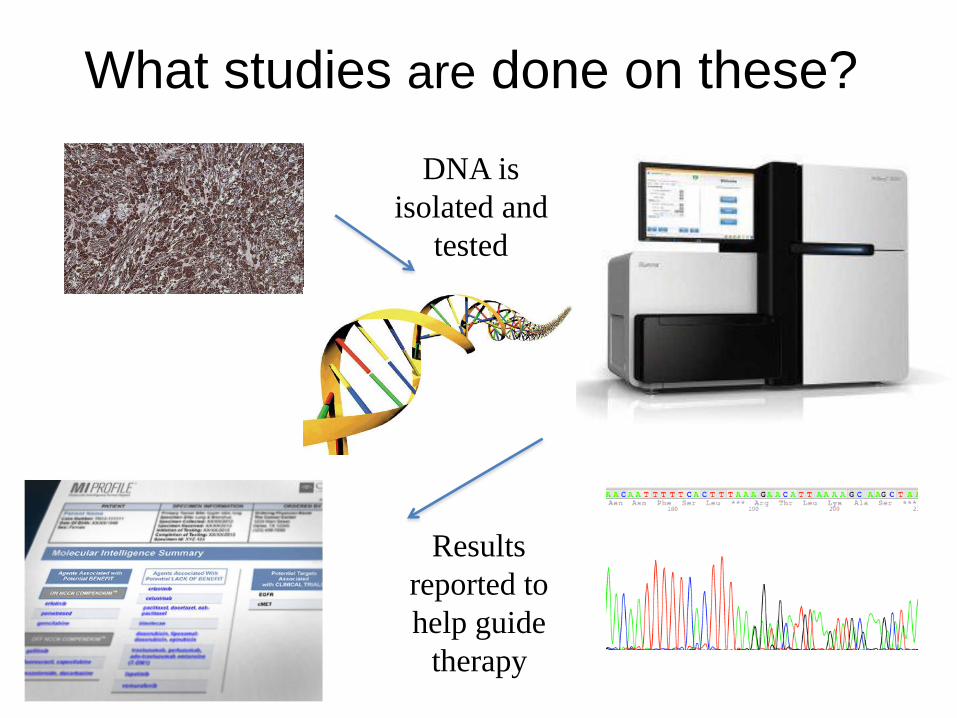
What studies are done on these?
DNA is
isolated and
tested
Results
reported to
help guide
therapy
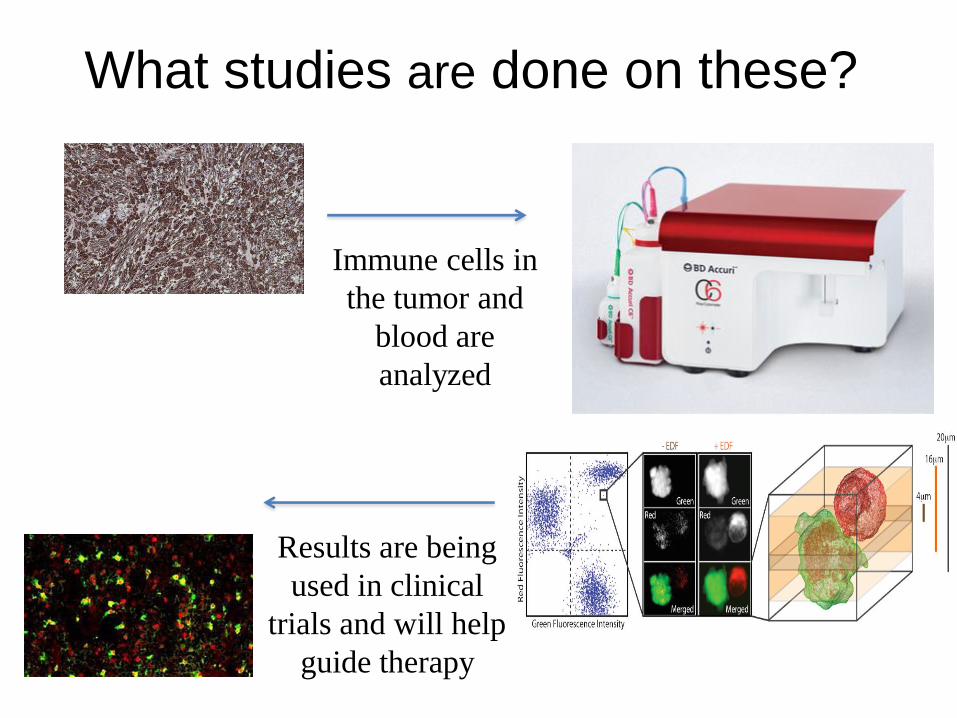
What studies are done on these?
Immune cells in
the tumor and
blood are
analyzed
Results are being
used in clinical
trials and will help
guide therapy
Can these studies help patients with
melanoma?
They already have!
Research into genetic
changes and immune changes
in tumors have already led to
advances in treatment
CRAFBRAF
MEK
ERK
BRAF
Uncontrolled
growth
Resistance to
killing
Growing new
blood vessels
Ability to
spread
Ability to escape from
the immune system
X
BRAF inhibitor
(Vemurafenib,
Dabrafenib)
MEK
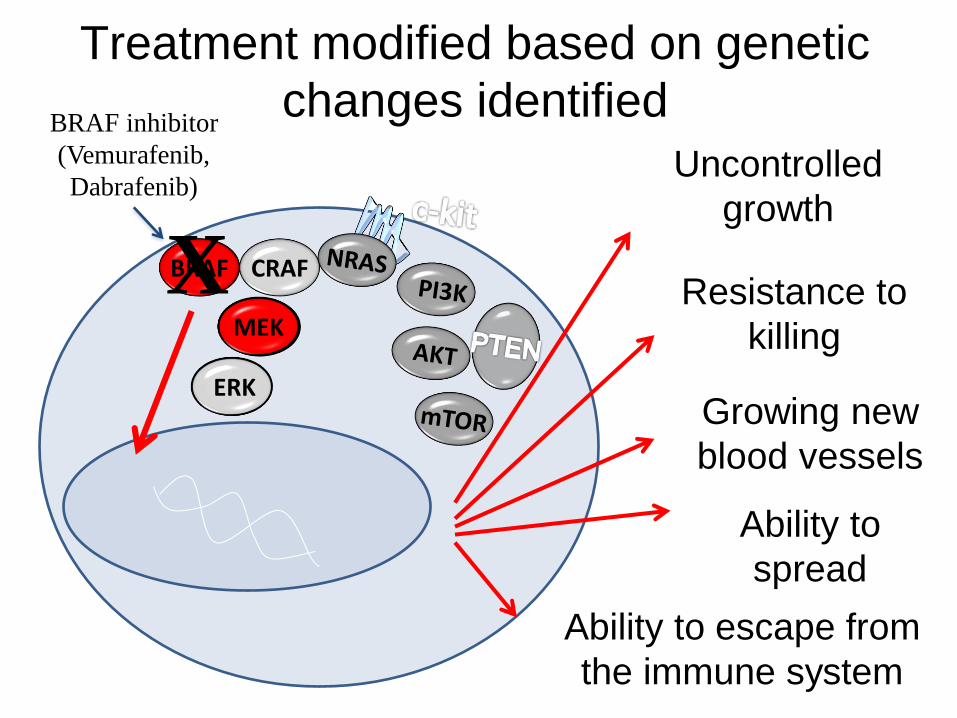
Treatment modified based on genetic
changes identified
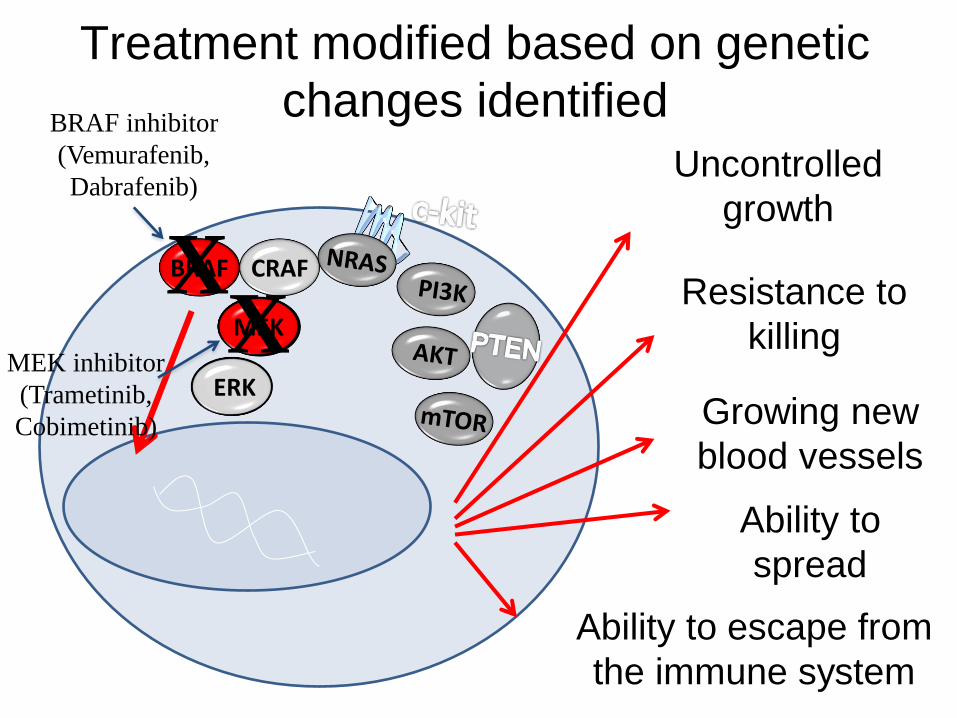
CRAFBRAF
MEK
ERK
BRAF
Uncontrolled
growth
Resistance to
killing
Growing new
blood vessels
Ability to
spread
Ability to escape from
the immune system
X
BRAF inhibitor
(Vemurafenib,
Dabrafenib)
MEK
Treatment modified based on genetic
changes identified
MEK inhibitor
(Trametinib,
Cobimetinib)
X

Combinations of a BRAF
inhibitor and a MEK inhibitor
are now being used in the
treatment of advanced
melanoma
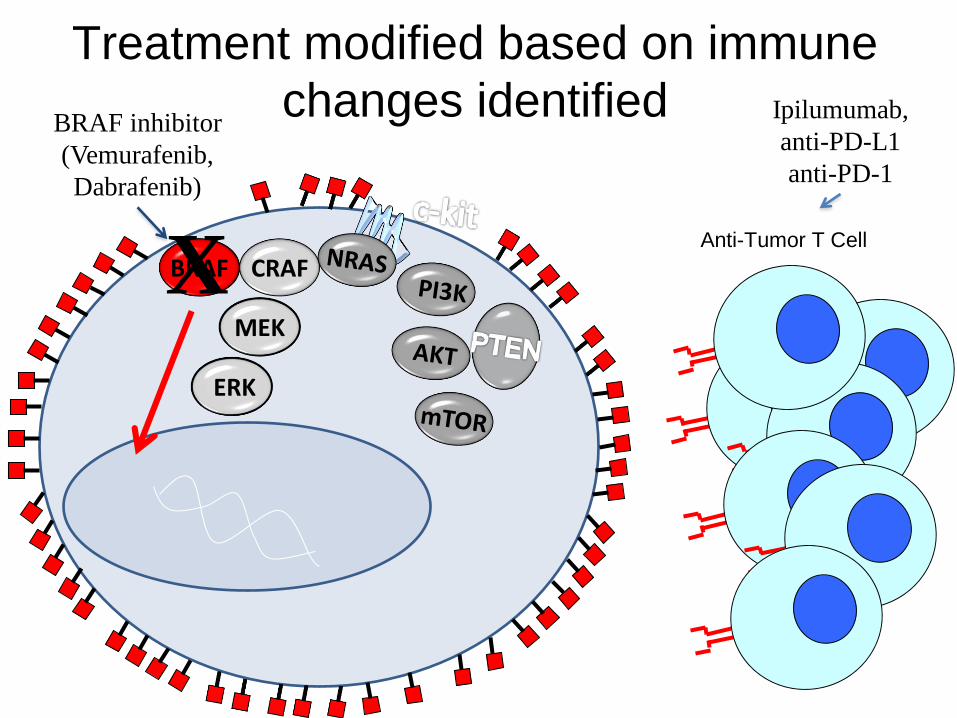
Treatment modified based on immune
changes identified
CRAFBRAF
MEK
ERK
BRAFX
BRAF inhibitor
(Vemurafenib,
Dabrafenib)
Ipilumumab,
anti-PD-L1
anti-PD-1
Anti-Tumor T Cell
Combination of BRAF
inhibitors and immunotherapy
are now in clinical trials and
show promise for patients with
advanced melanoma
BRAF inhibitor + Ipilimumab
BRAF inhibitor + PD-L1
BRAF inhibitor + TIL
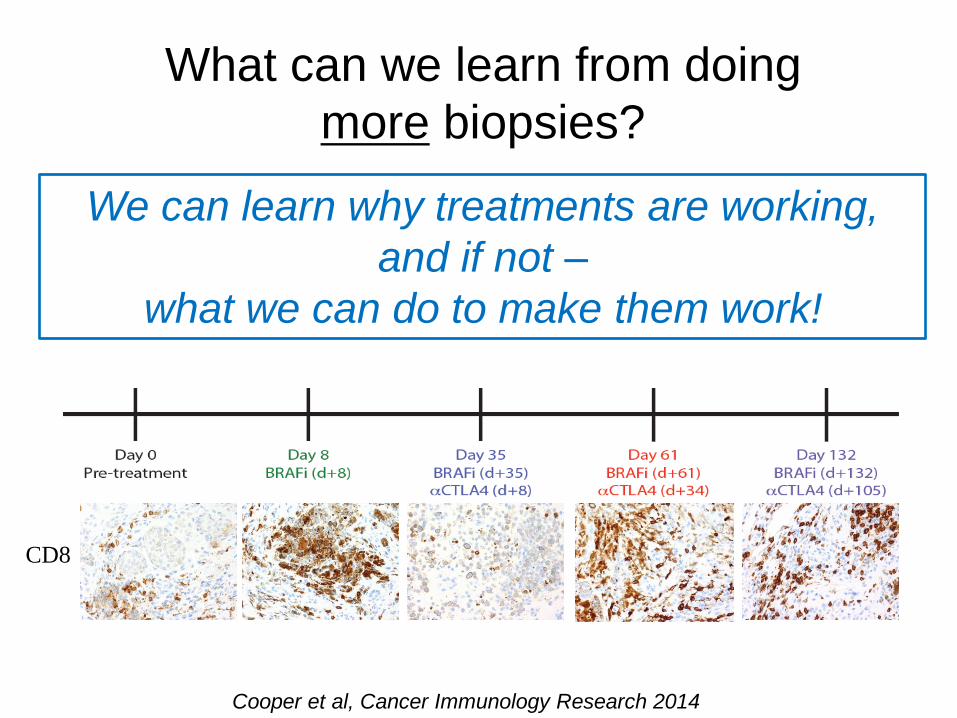
Cooper et al, Cancer Immunology Research 2014
What can we learn from doing
more biopsies?
CD8
We can learn why treatments are working,
and if not –
what we can do to make them work!
When may my doctor ask me if I am
willing to have a biopsy?
Clinical indications:
• Diagnosis of an abnormal area (from exam
or from CT scans)
• As indicated for a clinical trial (for
enrollment or during treatment)
Research:
•Ultimate goal is to cure ALL patients with
melanoma – research is critical to this
•You can help others beat this disease!
The Melanoma
Moon Shot ProgramThese efforts are going on worldwide
through outstanding research studies

We are all
working together
to cure melanoma
AcknowledgementsMelanoma Research Foundation
Patients, families, participants
Other speakers
Laboratory InvestigationZachary Cooper, PhD
Alexandre Reuben, PhD
Jacob Austin-Breneman, BS
Hong Jiang, MS
Dennie T. Frederick, MS
Devarati Mitra, MD PhD
Vikram Juneja
MGH / Harvard CollaboratorsDavid Fisher, MD PhD
Keith Flaherty, MD
Arlene Sharpe, MD PhD
Lyn Duncan, MD
Adriano Piris, MD
Don Lawrence, MD
Ryan Sullivan, MD
MDACC CollaboratorsPatrick Hwu MD, Mike Davies MD PhD
Roda Amaria MD, other melanoma med onc
Merrick Ross MD, Jeff Gershenwald MD
Jeff Lee MD (other surg onc colleagues)
Many other MDACC past, present, and future
collaborators
Other Mentors / CollaboratorsAntoni Ribas, MD
Steven A. Rosenberg, MD PhD
Philanthropic / Grant SupportK08 and TMEN Grant support
Industry Sponsors for TrialsGenentech, GSK, BMS
Merck, MedImmune
Patients treated on trial (& families)
Questions?





























