Embed Size (px)
Citation preview
Pulmonary Ventilation
DR. Sofian Awamleh
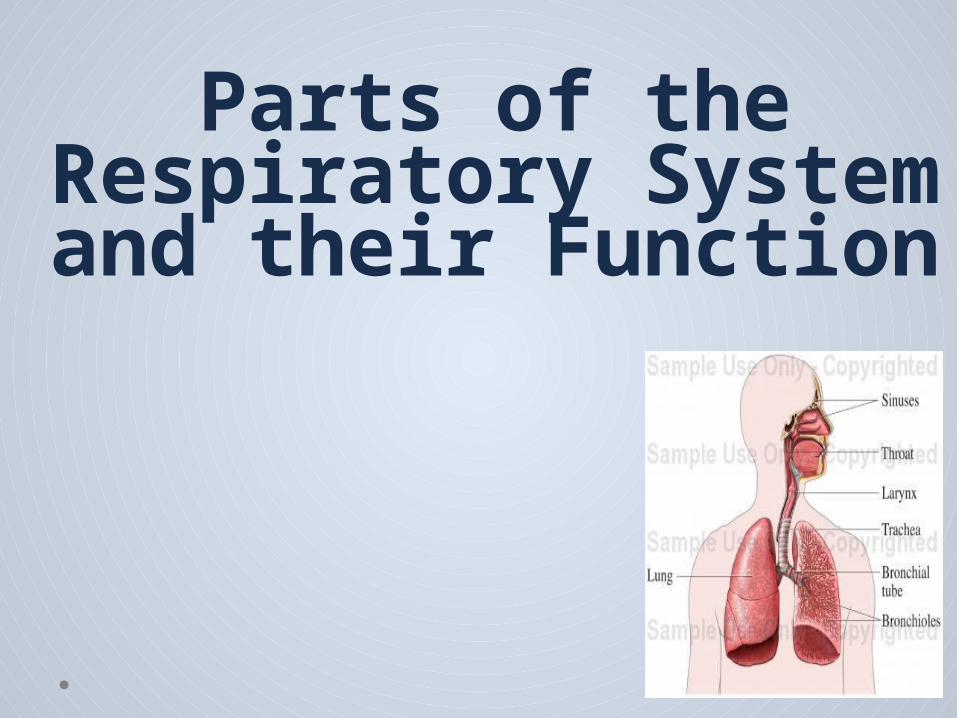
Parts of the Respiratory System and their Function

A. The upper respiratory
system
o The nose,
o Nasal o Cavity, o Paranasal
sinuses. o Pharynx
B. The lower respiratory
system
o The larynx.o trachea.o Bronchi.
bronchioleso Alveoli of the
lungs
Respiratory system consists of the organs that help to breathe .
Respiration also known as breathing : the process
which delivers oxygen from the external
atmosphere to the
body and removes the carbon dioxide from
body and expels out .
MAIN PARTS OF RESPIRATORY SYSTEM AND THEIR FUNCTIONS
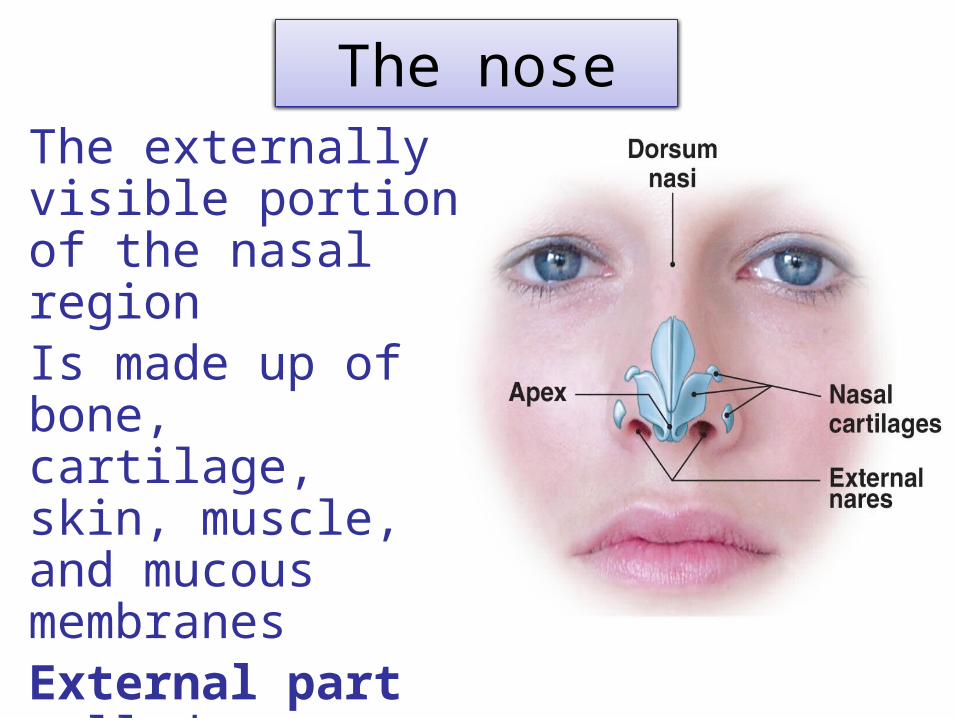
The noseThe externally visible portion of the nasal regionIs made up of bone, cartilage, skin, muscle, and mucous membranesExternal part called: Nostrils
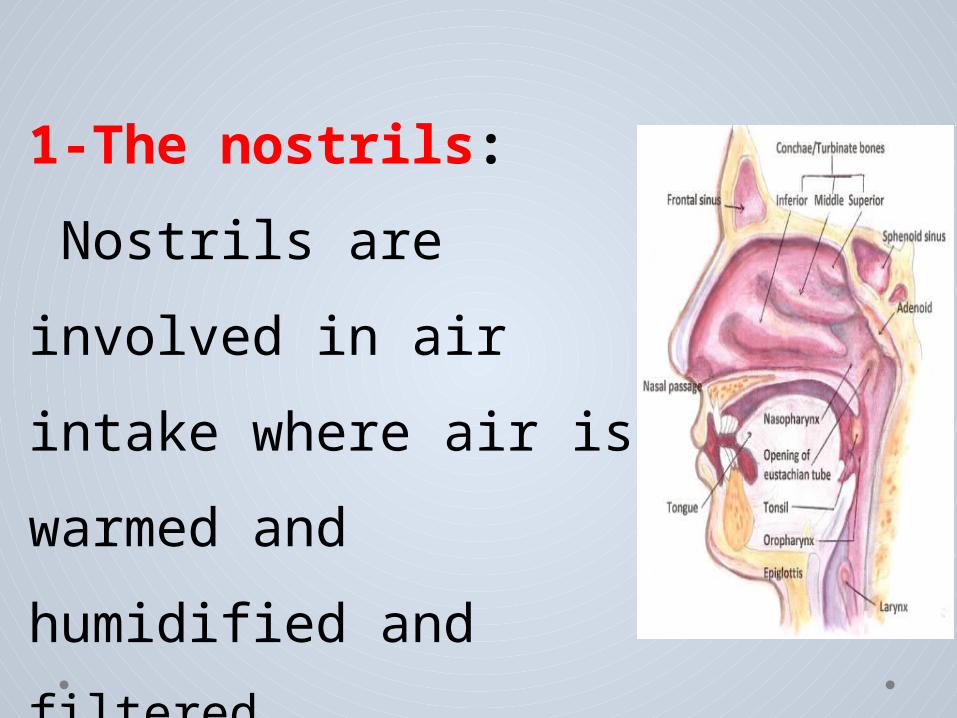
1-The nostrils: Nostrils are involved in air intake where air is warmed and humidified and filtered.
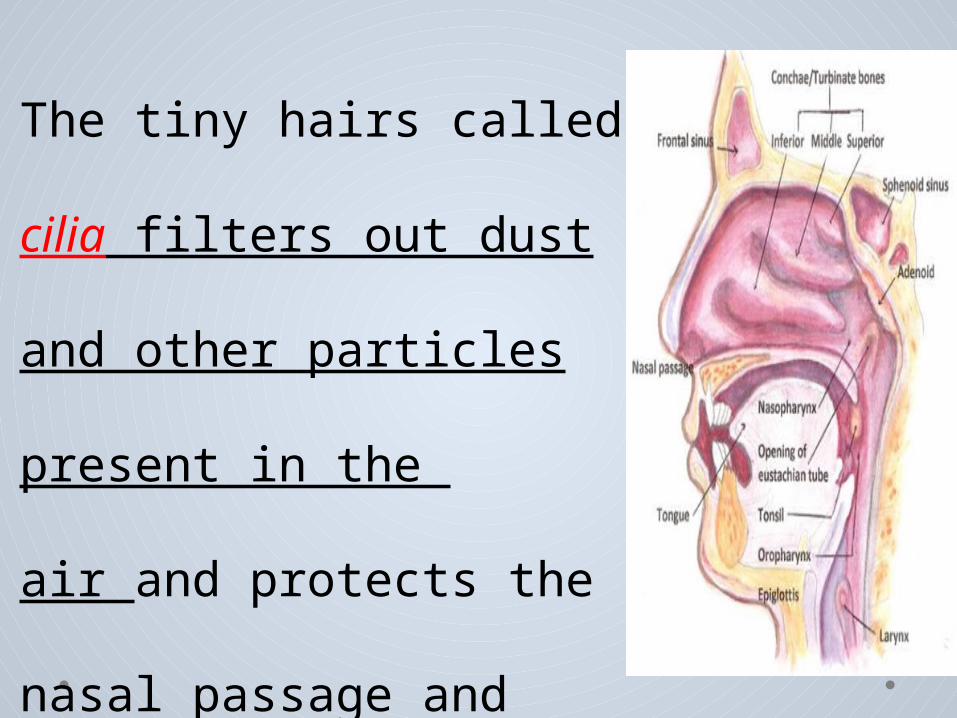
The tiny hairs called cilia
filters out dust and other
particles present in the
air and protects the
nasal passage and other
regions of the respiratory
tract.
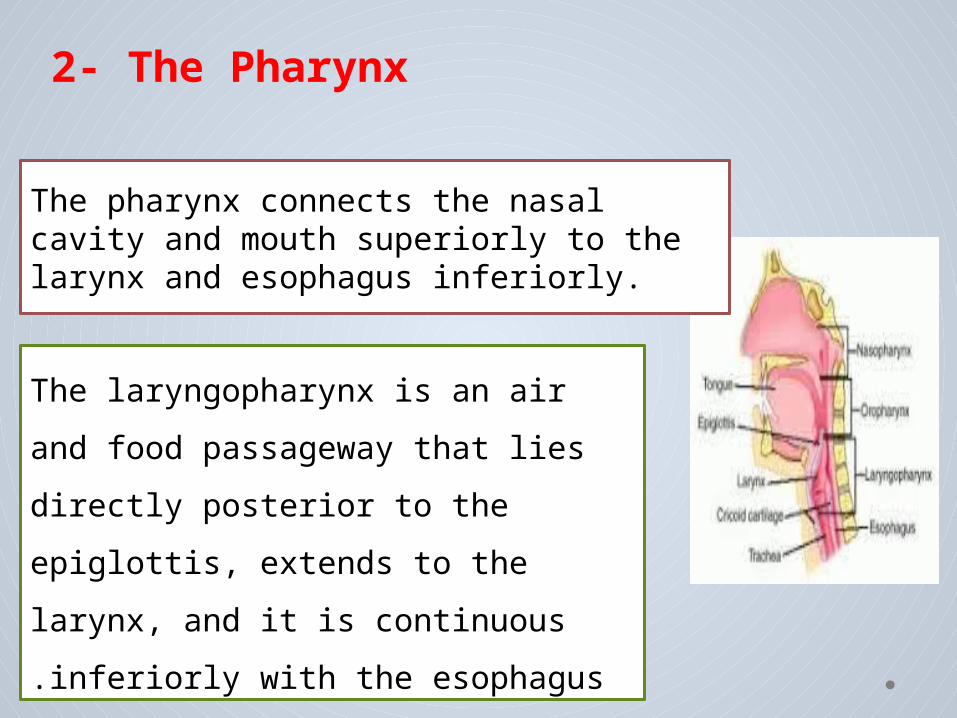
The pharynx connects the nasal cavity and mouth superiorly to the larynx and esophagus inferiorly.
The laryngopharynx is an air and food passageway that lies directly posterior to the epiglottis, extends to the larynx, and it is continuous inferiorly with the esophagus.
2- The Pharynx
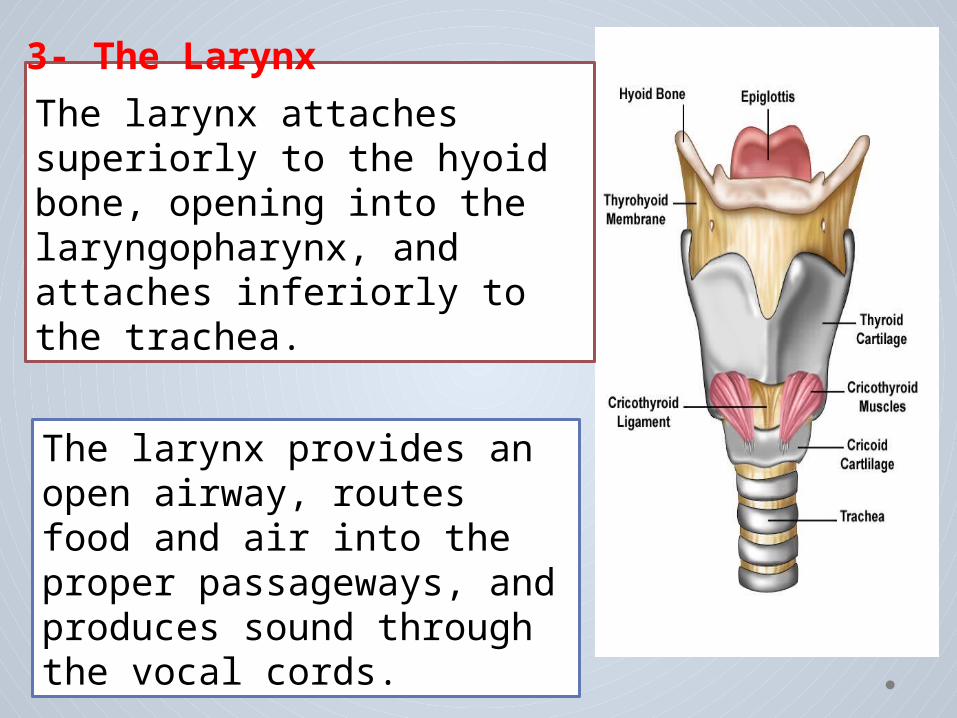
The larynx attaches superiorly to the hyoid bone, opening into the laryngopharynx, and attaches inferiorly to the trachea.
The larynx provides an open airway, routes food and air into the proper passageways, and produces sound through the vocal cords.
3- The Larynx
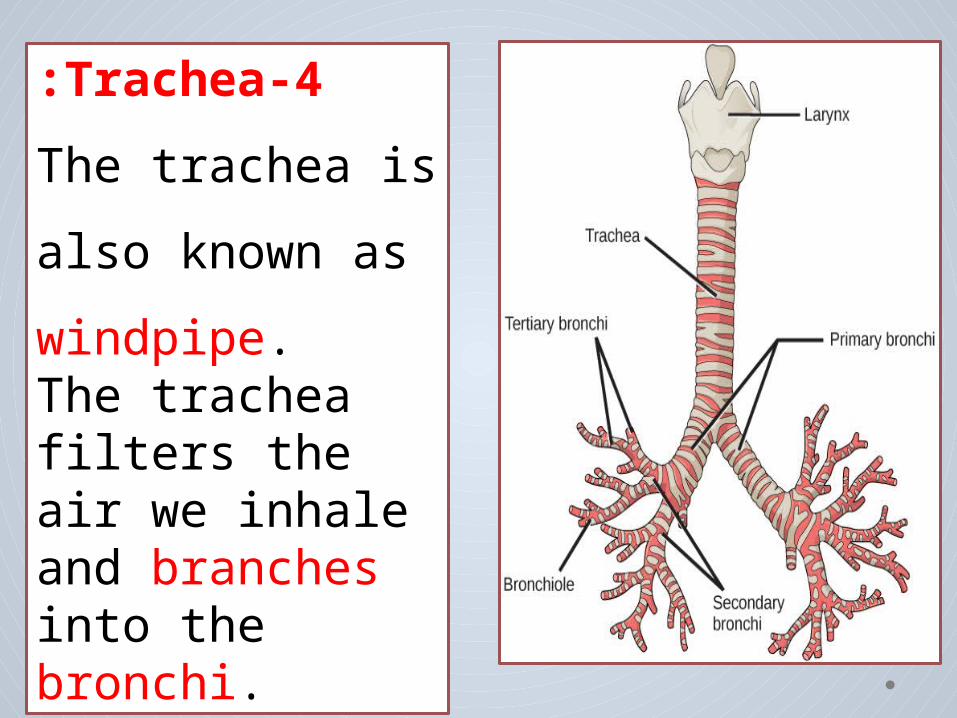
4-Trachea:The trachea is also known as windpipe. The trachea filters the air we inhale and branches into the bronchi.
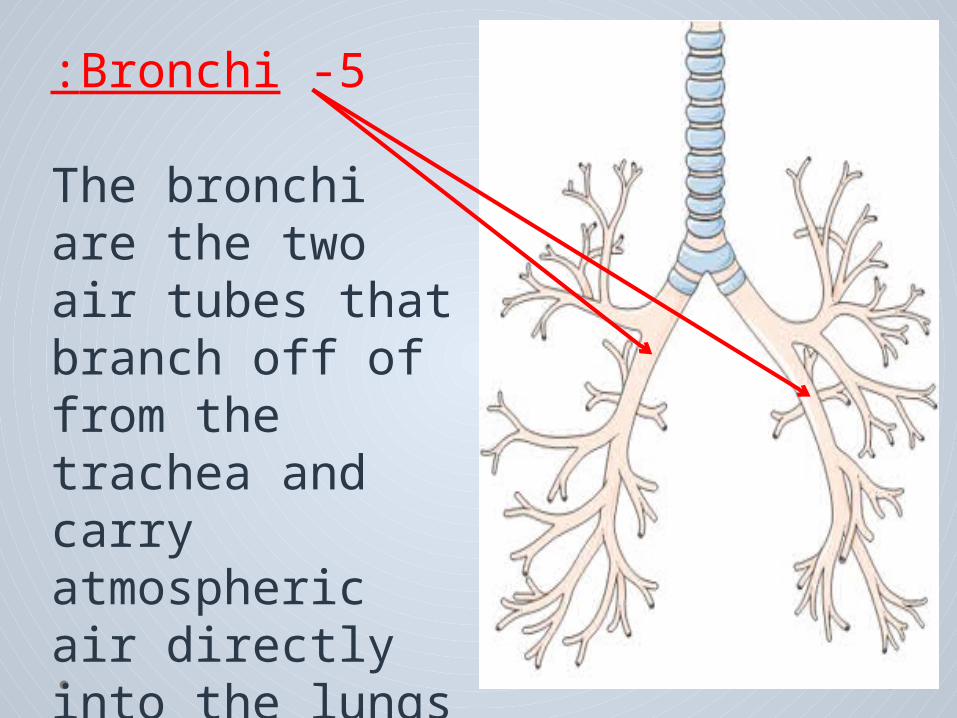
5 -Bronchi: The bronchi are the two air tubes that branch off of from the trachea and carry atmospheric air directly into the lungs
6-Lungs: The main organ of the respiratory system is lungs. Lungs are the site in body where oxygen is taken into and carbon dioxide is expelled out..
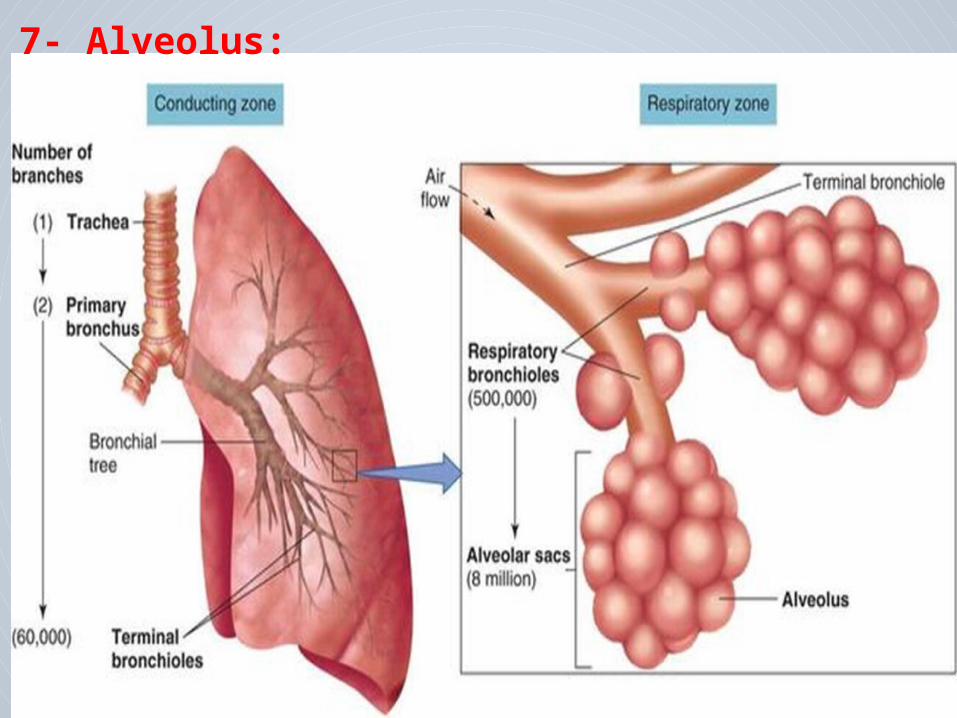
7- Alveolus:
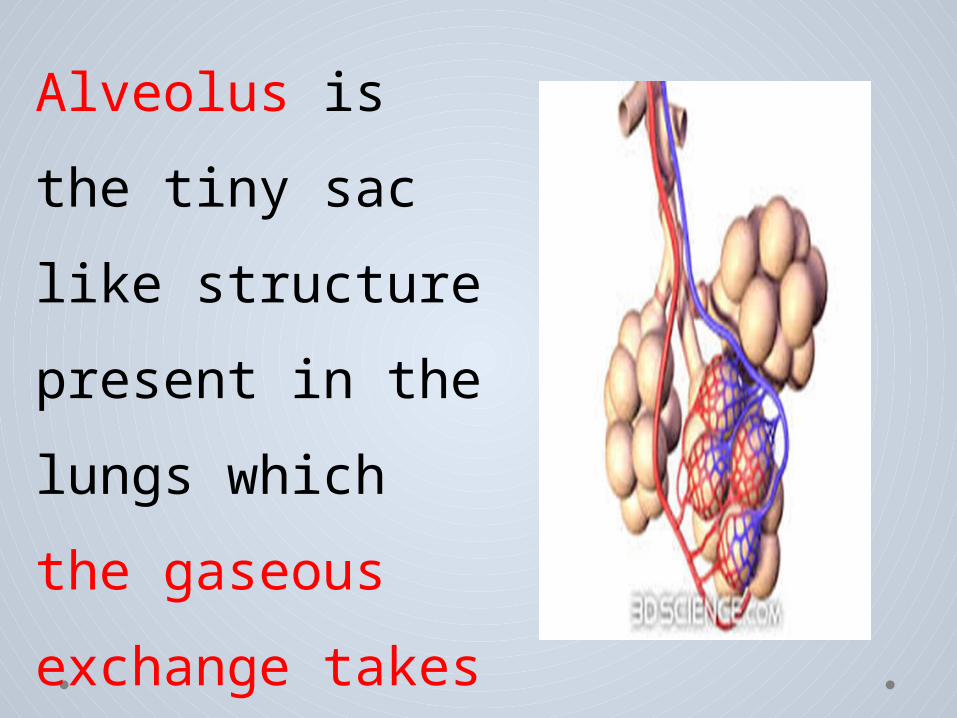
Alveolus is the tiny sac like structure present in the lungs which the gaseous exchange takes place.
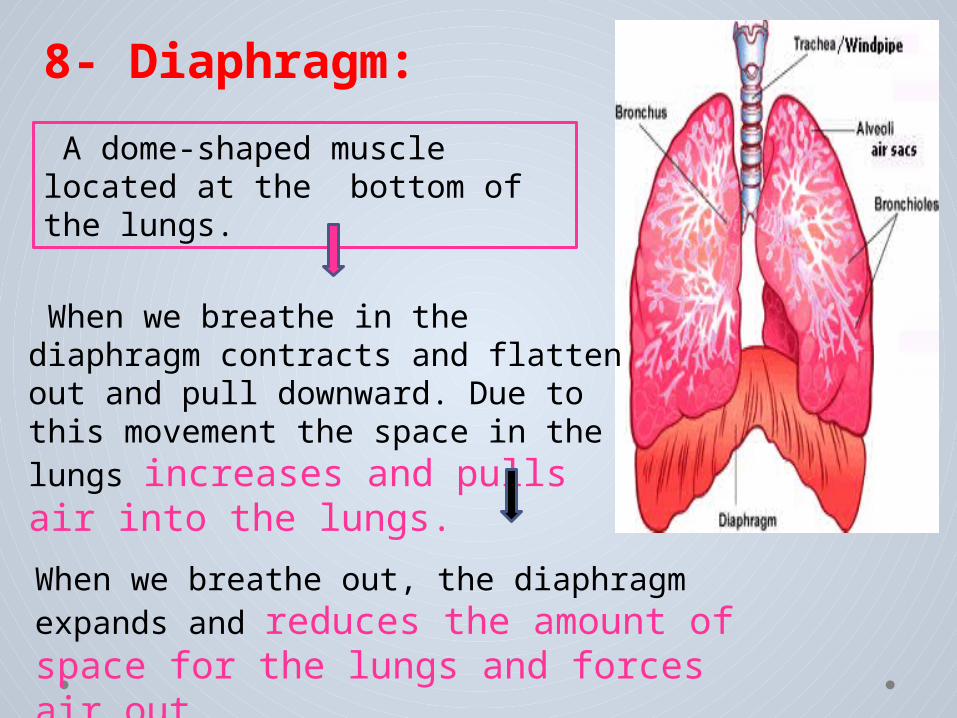
8- Diaphragm:
When we breathe in the diaphragm contracts and flatten out and pull downward. Due to this movement the space in the lungs increases and pulls air into the lungs. When we breathe out, the diaphragm expands and reduces the amount of space for the lungs and forces air out.
A dome-shaped muscle located at the bottom of the lungs.

Pulmonary Ventilation
The major four functions of respiration
1) Pulmonary ventilation: inflow and out flow of air between the atmosphere and the lung alveoli.
2 )Diffusion of oxygen and carbon dioxide between the alveoli and the blood
3) Transport of oxygen and carbon dioxide in the blood and body fluids And from the body tissues cells.
4 )Regulation of ventilation and other facts of respiration .
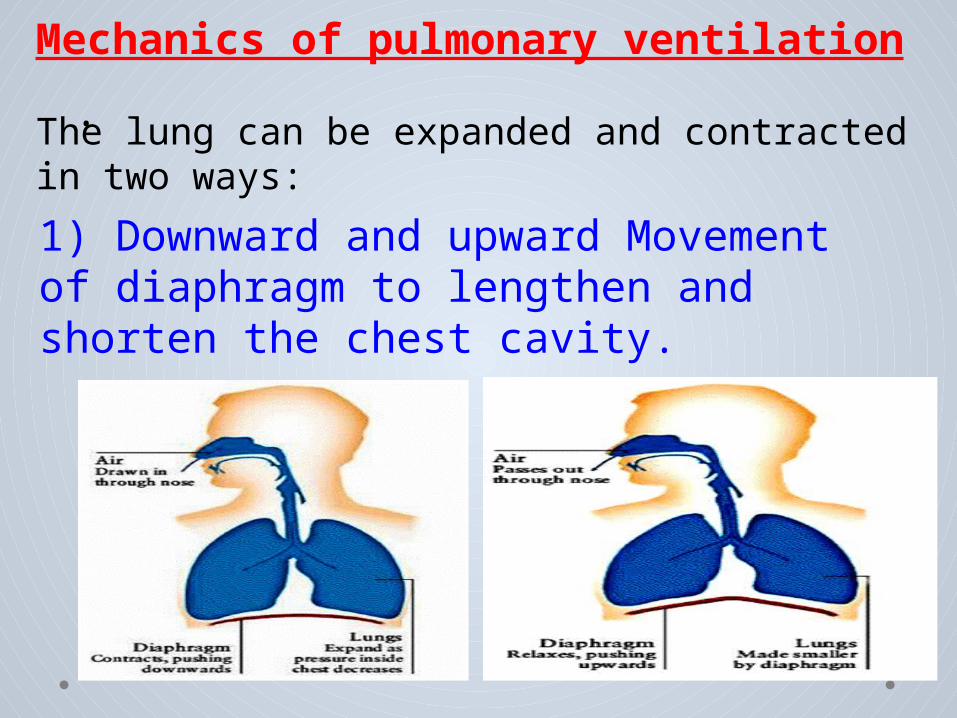
.Mechanics of pulmonary ventilation
The lung can be expanded and contracted in two ways:1) Downward and upward Movement of diaphragm to lengthen and shorten the chest cavity.
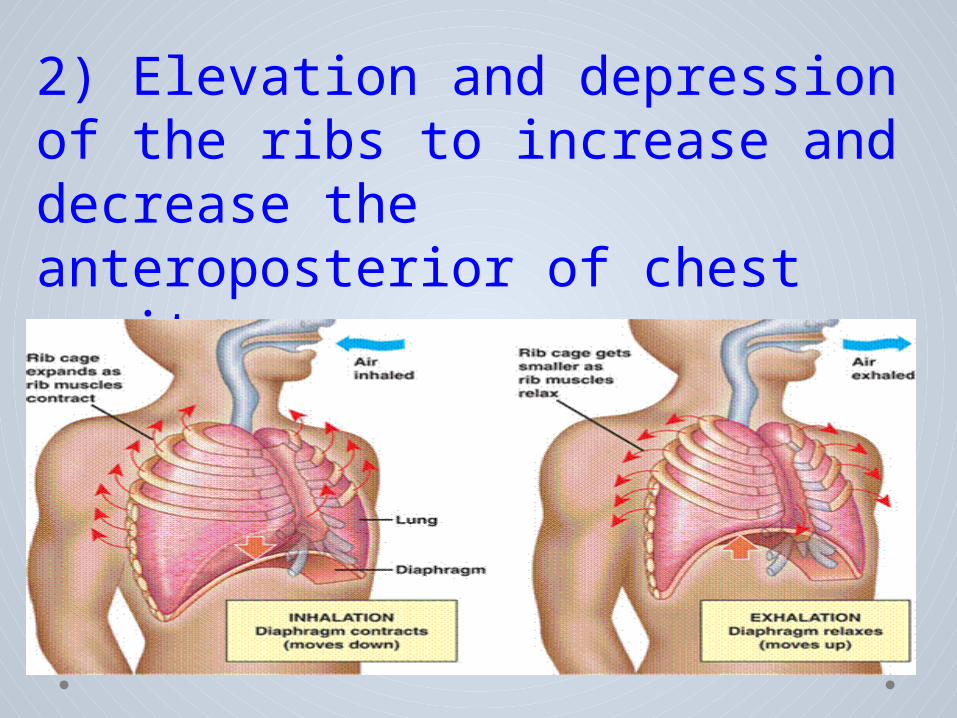
2) Elevation and depression of the ribs to increase and decrease the anteroposterior of chest cavity.
Normal quiet breathing is accomplished almost entirely by movement of the diaphragm
a. During inspiration, contraction of the diaphragm pulls the lungs downward.
b. During expiration, the diaphragm simply relaxes, and the elastic recoil compresses the lungs and expels the air.

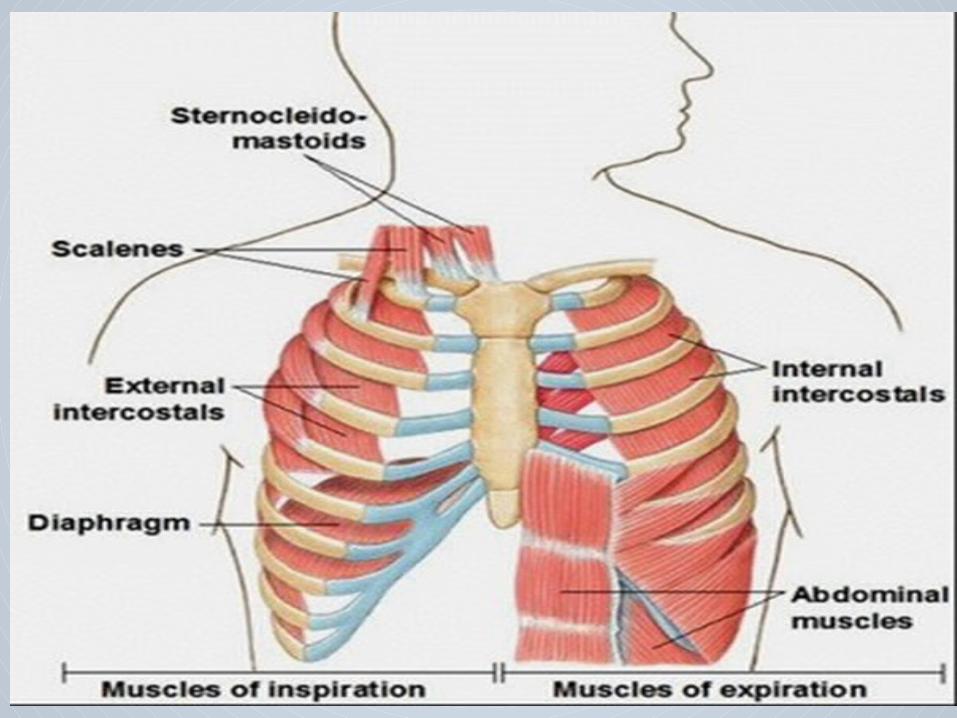
Respiratory muscles and their role in respiration :
,1)Muscles that elevate the chest cage are classified as muscles of inspiration. 2) Muscles that depress the chest cage are classified as muscles of expiration.
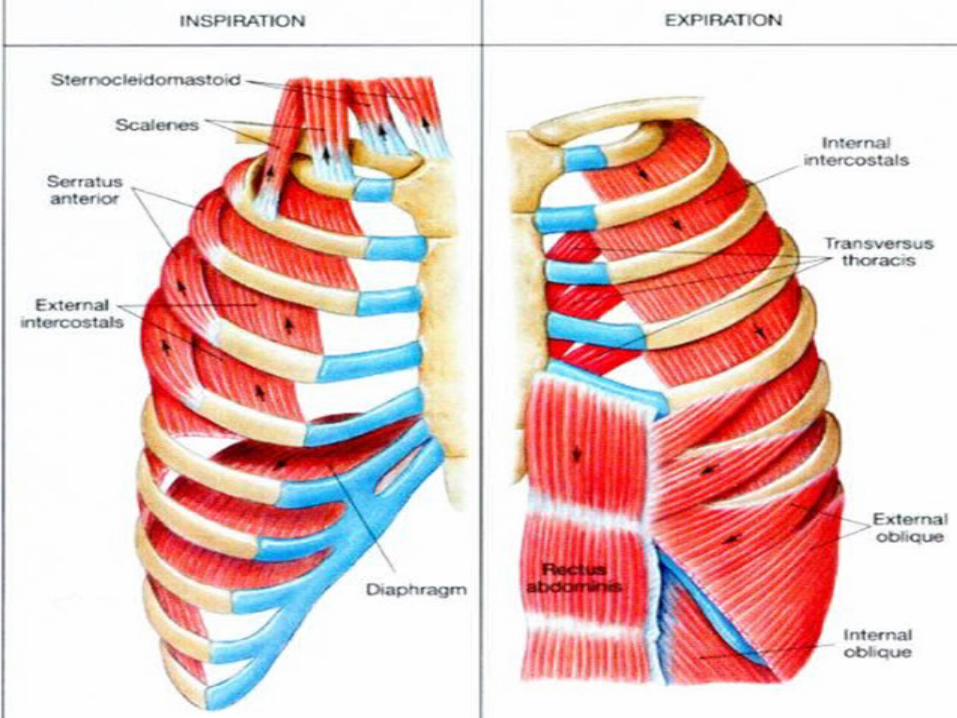
(1) sternocleidomastoid muscles, which lift
upward on the sternum.
(2) anterior serrati, which lift many of the Ribs.
(3 )Scaleni , which lift the first two ribs.
The most important muscles that raise the rib cage are the external intercostal , in addition these muscles support the previous process :
The muscles that pull the rib cage downward during expiration are:
(1) abdominal muscles : compress the abdominal cavity upward against the diaphragm up , and push air out of lungs. (2) internal intercostal muscles: pull the ribs downward and inward.
Inspiration Expiration
1.Diaphragm contracts pushing downward.
2.Lungs expand as pressure inside chest decreases.
3.Air drawn in through nose and mouth.
1. Diaphragm relaxes pushing upward.
2. Lungs made smaller and more pressurized by relaxing diaphragm.
3. Air passes out through nose and mouth.
Pleural pressure: pressure of the fluid in the thinspace between the lung pleura and the chest pleura; there is a slight suction so the pressure is negative.
Alveolar pressure: pressure of the air inside the lung alveoli
Transpulmonary pressure: difference between the pleural and alveolar pressures (recoil pressure).
Movement of Air In and Out of the Lungs and the Pressures That Cause the Movement
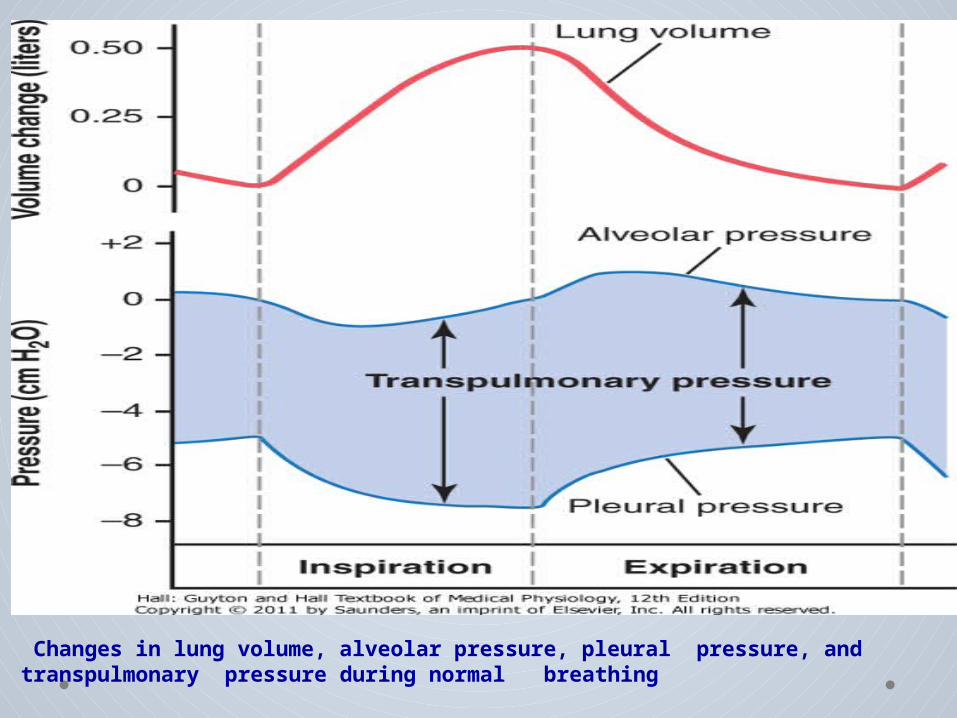
Changes in lung volume, alveolar pressure, pleural pressure, and transpulmonary pressure during normal breathing
Compliance of the Lungs The extent to which the lungs will expand for each unit increase in transpulmonary pressure.
Compliance Diagram of the Lungs
1. Inspiratory compliance curve.2. Expiratory compliance curve.3. Characteristics of the diagrams are depends
on:
The characteristics of the compliance diagram
(1) elastic forces of the lung tissue itself.
(2) elastic forces caused by surface tension of the fluid that lines the inside walls of the alveoli and other lung air spaces.

Compliance diagram in a healthy person
Comparison of the compliance of saline and air-filled lungs when the alveolar pressure is maintained at atmospheric pressure and pleural pressure is changed
Surfactant, Surface Tension, and Collapse of the Alveoli.
Principle of Surface Tension.
When water forms a surface with air, the water molecules on the surface of the water have an especially strong attraction for one another. As a result, the water surface is always attempting to contract. This is what holds raindrops together: a tight contractile membrane of water molecules around the entire surface of the raindrop.
an elastic contractile force of the entire lungs
the alveoli trays to collapse.
the water attempts to force the air out of the alveoli through the bronchi
Surface tension elastic force
Secreted by special surfactant-secreting epithelial
cells called type II alveolar epithelial cells.
Surfactant: is surface active agent in
water, which reduces the surface
tension of water.
Surfactant and Its Effect on Surface Tension
Surfactant is a complex mixture of several
phospholipids, proteins, and ions. The most
important
components are the phospholipid
Type II alveolar epithelial cells
These cells are granular, containing lipid inclusions
that are secreted in the surfactant into the alveoli.
If the air passages leading from the alveoli of the lungs are blocked, the surface tension in the alveoli tends to collapse the alveoli. This creates positive pressure in the alveoli, attempting to push the air out.
Pressure in Occluded Alveoli Caused by Surface Tension.
Effect of the Thoracic Cage on Lung Expansibility
• Compliance of the thorax and the lungs
• Work of breathing :
1.Compliance or elastic work2.Tissue resistance work3.Airway resistance work
“Work” of Breathing
Expiration
Respiratory muscle contraction
Elastic recoil of the lungs and chest cage
Inspiration
The work of inspiration can be divided into three fractions:
(1) that required to expand the lungs against the lung and chest elastic forces, called compliance work or elastic work; (2) that required to overcome the viscosity of the lung and chest wall structures, called tissue resistance work;
(3) that required to overcome airway resistance to movement of air into the lungs, called airway resistance work.
Energy Required for Respiration.
During normal quiet respiration, only 3 to 5 %of the total energy expended by the body is required for pulmonary ventilation. But during heavy exercise, the amount of energy required can increase as much as 50-fold, especially if the person has any degree of increased airway resistance or decreased pulmonary compliance.
Pulmonary Volumes and Capacities
• Pulmonary Volumes
1. Tidal Volume : volume of air inspired or expired with each normal breath; usually about 500 ml.
2. Inspiratory Reserve Volume : extra volume that can be inspired over and above the tidal volume usually about 3000 ml.
3. Expiratory Reserve Volume : maximum extra volume that can be expired at the end of a normal tidal expiration usually about 1100 ml.
4. Residual Volume : volume of air remaining in the lungs after the most forceful expiration; usually about 1200 ml.
Pulmonary Capacities
1. Inspiratory Capacity = tidal volume + inspiratory reserve volume about 3500 ml
2.Functional Residual Capacity = expiratory reverse volume + residual volume about 2300 ml3. Vital Capacity= inspiratory reserve volume + expiratory reverse volume = (4600) ml
4. Total Lung Capacity= Vital Capacity+ residual volume = (5800) ml
Mucus Lining the Respiratory Passageways.
The mucus is secreted partly by individual mucous goblet cells in the epithelial lining of the passages and partly by small submucosal glands.
Function: keeping the surfaces moist, and traps small particles out of the inspired air and keeps most of these from ever reaching the alveoli.
Nervous and Local Control of the Bronchiolar Muscles
1. Sympathetic ( dilation of the bronchi )
• Direct control of the bronchioles by sympathetic nerve fibers is relatively weak because few of these fibers penetrate to the central portions of the lung.
• The bronchial tree is very much exposed to norepinephrine and epinephrine released into the blood by sympathetic stimulation of the adrenal gland medullae.
2. Parasympathetic( Constriction of the Bronchioles) few parasympathetic nerve fibers derived from
the vagus nerves penetrate the lung . These nerves secrete acetylcholine , when activated, cause mildto moderate constriction of the bronchioles. When a disease process such as asthma has already caused some bronchiolar constriction.When this occurs, administration of drugs that block the effects of acetylcholine, such as atropine, can sometimes relax the respiratory passages enough to relieve the obstruction.
Local Factors Often Cause Bronchiolar Constriction.
1. Histamine 2. Slow reactive substance of anaphylaxis.
Both of these are released in the lung tissues by mast cells during allergic reactions.They play key roles in causing the airway obstruction that occurs in allergic asthma; this is especially true of the slow reactive substance of anaphylaxis.
Disorders of the respiratory system
1. Chronic infection : caused by inhaling smoke or other substances that irritate the bronchi and bronchioles
2. The infection, excess mucus, and inflammatory edema of the bronchiolar epithelium.
3. The obstruction of the airways causing difficulty to expire .

THANK YOU





























